
Abstract
Power has been demonstrated to be an early and potent marker of frailty. The measurements currently available are tied to locality. Usually, measurements include single joint movements or movements of only the legs and the resistance is not adjusted for body weight. In this study, a portable method to measure power in the sit-to-stand transfer was developed and tested. Mean power was calculated from the vertical ground reaction force of body weight, the difference between height in a sitting and in an upright position and the time taken to stand up. The results of this power measurement were compared with an isokinetic force measurement, the "Nottingham power rig", and measurement of physical performance in a five-repetition chair rise (five-chair rise). A convenience sample of 33 healthy elderly subjects [mean (SD) age: 67.8 (6.7) years; 17 men, 16 women] was included. Measurement of power during the sit-to-stand transfer showed good correlation to isokinetic force measurement (r=0.68) and to the "Nottingham power rig" (r=0.6). Correlation to five-chair rise was poor (r=−0.08). In conclusion, the study shows that the method presented is able to measure power during performance of a daily task. The poor correlation between the introduced measurement and the five-chair rise suggests that it might be able to detect decline in muscle function earlier by the introduced measurement than by measurement of the functional status. As it is inexpensive and portable, its use in clinical practice and research contexts, including home-bound individuals, is feasible.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With advancing age and loss of functional capacity, power as the product of force and speed is more important than strength for performing daily activities like rising from a chair, walking or stair climbing (Bassey et al. 1992; Harridge and Young 2000). Thus, during recent years new strategies to improve power output (Skelton et al. 1995; Jozsi et al. 1999) have been given high priority (Evans 2000).
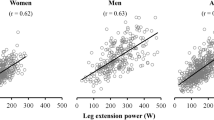
Power is frequently calculated from isokinetic strength measurements, where dynamic force is measured at a constant velocity. Single-joint extension and/or flexion is performed in this measurement. Rahmani et al. (1999) developed a method using knee extension, including a ballistic movement, which seems to be more related to daily activities (Kostka et al. 2000). Power output was calculated from the speed of the load displacement resulting from the leg extension.
The "gold standard" to measure power is the "Nottingham power rig" (Bassey and Short 1990). Here, the average leg extensor power is inferred from the angular velocity and inertia of a flywheel, which is driven by a single thrust with one leg, including hip and knee extension and ankle plantar flexion. The assessment of power by cycling provides data calculated by the mass and angular velocity of a flywheel (Martin et al. 2000), which reflects the power of a cyclic guided motion and the concentric work of the muscles. All these measurement devices are relatively expensive and locally tied.
Power measurements can also be conducted in more physiological manoeuvres like jumping (Davies et al. 1983). These measurements automatically overcome the problem of the resistance and its adaptation to body weight as they include body weight in the measurement. In elderly subjects jumping measurements are not recommended because of safety considerations.
The sit-to-stand (STS) transfer can be divided into different phases. In the preparation phase the trunk is accelerated forward (Roebroeck et al. 1994) until hip flexion reaches its maximum and the buttocks lose contact to the seat. Simultaneously vertical ground force at the feet peaks (Kralj et al. 1990; Hirschfeld et al. 1999). The extension phase begins with seat-off and lasts until the velocity of the centre of mass decreases to zero (Hirschfeld et al. 1999) which is concurrent with an extension of the hip and knee joint (Kralj et al. 1990). In the following stabilization phase postural control is achieved by contractions of calf muscles (Roebroek et al. 1994).
Fleming et al. (1991) tried to develop a simple method to measure power while standing up from a chair. Using a force plate, a curve of force related to time was provided. Peak power was defined as the slope of the curve. The same shape of this curve was shown by Hirschfeld et al. (1999) adding the concurrent kinetic data. Rising from a chair was described with the help of force plates under each buttock and foot as well as a two-camera optoelectronic system to provide data of calculated centre of mass kinematics. Further kinetic data of knee, hip and ankle joint angles were presented by Kralj et al. (1990), who defined different phases of the STS transfer.
Based on the aforementioned investigations, this study attempts to introduce a safe and portable method to measure power output in the STS transfer, representing a functional task. Furthermore, it attempts to compare the results with other commonly used methods.
A good correlation of the introduced method to isokinetic measurement and to results provided by the Nottingham power rig is hypothesized, because all these investigations aim to measure the power output of a lower extremity movement. Very high correlations might not be observed because of the diversity of the movements, representing a single-joint movement, a ballistic movement and a more complex movement in the STS transfer.
Methods
Subjects and design
For a cross-sectional evaluation a convenience sample of 33 healthy elderly [mean (SD): 67.8 (6.7) years; 17 men, 16 women] were recruited. Subjects had no known neurological or orthopaedic problems and were successively enrolled. All subjects gave written informed consent. The study was conducted in September and October 2001.
Measurement of power during STS
Subjects sat on a chair of standard height (46 cm) with their arms crossed over their chest, each foot resting non-constrained on a force plate (Soehnle, Germany) and their trunk touching the backrest of the chair. They were instructed to stand up as fast as possible. The force plates (two calibrated commercially available scales) provided a curve of vertical force as a function of time by a two-channel acquisition of the analogous signals which were digitized at 142 Hz. Storage of files and calculation of data was done on a PC. In this investigation we focused on the general validity of the method and used only the sum values of ground reaction force of both legs.
According to the work of Hirschfeld et al. (1999) and Kralj et al. (1990) we defined a preparation phase (PP, T1–T2) during the STS transfer, beginning with the decrease of vertical force by more than 2.5% of feet weight (T1). The preparation phase lasts until the peak of vertical force (T2) was reached, which indicates seat-off. The rising phase (RP, T2–T3) starts with the peak vertical force (T2). The end of RP was defined as the point when the vertical force reaches body weight (T3) after decreasing and increasing again. In a following stabilization phase (SP, T3–T4) the vertical force oscillates around body weight. The end of SP (T4) was defined as the point when the vertical force oscillates inside a corridor of 2.5% plus/minus body weight. A typical curve of vertical force as function of time is shown in Fig. 1.

The complete sit-to-stand transfer is divided into preparation phase (T1–T2), rising phase (T2–T3) and stabilization phase (T3–T4). BW Body weight, MGRF maximum ground reaction force, OS overshoot, IC incline, WFL weight of feet/legs at rest, T1 start of movement, T2 seat-off, T3 extension of body, T4 end of movement
The movement to determine power during the STS transfer was defined as raising body weight from sitting to an upright position as fast as possible. Thus, mean power was calculated from the vertical force of body weight, the difference between height in a sitting and in an upright position and the time needed for rising (T2–T3). It was calculated from the following equation:
where the constant factors body weight (f) and distance (s) represent the ground reaction force of body weight and the difference between body height in a sitting and in an upright position, respectively. The time interval of the RP (T2–T3) was expressed as time (t).
The body weight as well as the peak force were measured as the sum of the ground reaction forces of both feet. As the STS manoeuvre is a daily task, the effect of extensive motor learning can be neglected and the better of two trials, according to the power result, was taken for the analysis.
As characteristic features of the force–time curve, the maximum ground reaction force at T2, the overshoot as the difference between the maximum ground reaction force and body weight and the incline of the curve between 20% and 90% of the maximum ground reaction force were evaluated.
Reliability of repeated measurement was assessed in 31 healthy young hospital employees [37.9 (7.6) years]. Two sets on the same day, taking the better of two trials, according to the power results, were compared to describe test-retest reliability (r icc=0.95). A break of 4 min between sets was given. Inter-rater reliability was assessed by comparing the first set with the same protocol on the following day, as assessed by a different investigator (r icc=0.96).
Other measurements
Power of the lower limb was assessed by the Nottingham power rig (Bassey and Short 1990). Subjects were seated with just their pelvis supported at their back. They were instructed to push with a single leg against a plate over a distance of 16.5 cm. At the end of the movement the leg was extended. Power was inferred from angular velocity and inertia of a flywheel, which was driven by a chain connected to the foot plate by a lever. Out of five successive trials in total, the trial with the largest calculated power of each leg was taken. For the analysis the results of the right and left leg were added.
Isokinetic force of the knee extensors and flexors was measured by a Cybex Norm dynamometer (Lumex, New York, USA) at a speed of 60°/s. Subjects were instructed to extend and flex their knee as hard as possible. The better of two trials, according to the force results of each leg, was taken. For the analysis the maximum force of extension as well as flexion of the right and left leg were added.
In order to assess the performance to stand up from a chair subjects were told to stand up from a chair and to sit down five times in a row as fast as they could (five-chair rise, Guralnik 1994). The time needed to do so was included for the analysis.
Before each measurement the subjects familiarized themselves with the equipment and had a short warm-up. The order of measurements was randomly assigned for each subject.
Statistical analysis
The results are reported as mean (SD). Pearson's coefficient of correlation (r) was used to show an association between various measurements. Absolute value of the correlation coefficient was classified as poor (0.00–0.40), fair to good (0.41–0.75) and excellent (>0.75) based on criteria established by Fleiss (1986). Intraclass correlation coefficient (r icc) was used to describe the test retest as well as the inter-rater reliability in the younger population. The data were analysed using SAS 8.0 (SAS Institute, Cary, USA).
Results
There was no occurrence of negative side effects. The characteristics of the group are shown in Table 1.
The mean time of the total STS transfer (T1–T4) was 1.2 (0.07) s for the healthy elderly subjects. According to the different phases during the transfer described above, time from seat-off to extended legs (RP, T2–T3) took 37.5% [0.45 (0.07) s] of the total movement. PP (T1–T2) and SP (T3–T4) represented 52.5% [0.63 (0.11) s] and 10% [0.12 (0.08) s], respectively, of the total movement.
Maximum ground reaction force, overshoot and incline were strongly associated with power during the RP transfer with correlations all above 0.67 ranging from good (overshoot) to excellent (maximum ground reaction force, incline).
Measurement of power during the RP transfer showed good correlation to the isokinetic force and to measurement of power by the Nottingham power rig. Correlation to the five-chair rise was poor. The mean results of all different measurements, of the characteristics of the power measurement and all coefficients of correlation are shown in Table 2.
Discussion
Phases of the STS transfer related to force
The decrease of the ground reaction force during the initiation of the STS transfer might indicate hip flexion with relief of strain on the feet while the upper body is shifted forward from the back rest of the seat. After this, ground reaction force increases up to peak force. Although ground reaction force increases above body weight, the test subject still has contact with the seat. This was shown by Kralj et al. (1990) and by Hirschfeld et al. (1999). Peak force is primarily generated by the quadriceps contributing to the redirection of the forward shift of the upper body. This forward shift leads to an increased loading of the feet. When ground reaction force increases above body weight, centre of mass is accelerated upward, but its position is lowered (Roebroek et al. 1994), indicating isometric and eccentric force generation. The lowering of the centre of mass is caused by the forward and downward shift of the upper body during the preparation phase. At peak force (T2) the body looses contact with the seat (Kralj et al. 1990; Hirschfeld et al. 1999). Although ground reaction force decreases now, the body is extended; thus, the centre of mass is lifted. It is accelerated as long as force is greater than the level of body weight. Then centre of mass is decelerated until ground reaction force again reaches the level of body weight (T3). This point is concurrent with the extension of the hip and knee joint (Kralj et al. 1990). Thus, it represents the moment when the body is standing upright. In a last phase of stabilization (T3–T4) the ground reaction force oscillates around body weight. As balance plays a role in the performance of the chair rise, the duration of this phase might be related to balance capacity (Schenkman et al. 1996). The oscillating ground reaction force likely is generated by the activity of the calf muscles in order to stabilize stance (Manchester et al. 1989; Roebroeck et al. 1994).
All these explanations show that the calculation of power during the STS transfer, concerning our definition to raise body weight from a seated to an upright position, is restricted to the RP.
Measurement of power
As power includes the aspect of speed related to force, it becomes more important for elderly people than force alone (Bassey et al. 1992). Thus, measurement of power will become an indispensable necessity in clinical practice. Since many frail candidates are unwilling or not capableof being transported to a mobility laboratory we must be interested in portable devices to assess physical performance. Isokinetic power calculation, power measurement by ballistic knee extension as well as the Nottingham power rig do not meet these requirements. The results of power measurement by isokinetic equipment, by ballistic knee extension and by the Nottingham power rig have to be adjusted for body weight. Conversely, the results of our described method are automatically adjusted to body weight, as body weight is included in the calculation of power. Furthermore, the validity of the guided movement of the isokinetic measurement is questionable to represent a functional task. The speed of the movement is given and power is calculated only from the variation of force. Thus, the physiological aspect of time/speed is neglected. If a single joint movement is performed to assess power, a ballistic movement (Rahmani et al. 1999) should be preferred. Furthermore, 20–30 min are necessary when using an isokinetic dynamometer to assess power. Conversely, the described measurement of power during the STS transfer is accomplished within 10 min, including demonstration and warm-up.
Using biomechanical, isokinetic or isometric measurements it is recommended that the results be weighed of the measured muscle forces related to their function during the relevant movement (Chandler et al. 1997). Conversely, our method represents a biomechanical measurement of function, with each muscle showing the typical activity of the investigated movement.
The assessment of power by a cycling ergometer was not included in the protocol. Functional tasks like walking, stair-climbing or the STS transfer are characterized by concentric as well as eccentric forces. Cycling, however, is clearly dominated by concentric forces while the proportion of eccentric forces is unclear.
The good correlation of the results with the Nottingham power rig and the isokinetic force measurement express its concurrent validity. The fact that the correlations were not excellent is not surprising as the presented measurement of power during the STS transfer does represent a different movement. Movements such as knee extension (isokinetic force) or leg extension (Nottingham power rig) do not include an upper body movement, which is included in the presented measurement. This interpretation is supported by the fact that the mean power during STS transfer was twice as large compared to the Nottingham power rig. Another explanation for the good, but not excellent, correlation between the two measurements might be the difference in the applied load (weight-bearing versus non-weight-bearing). Concerning the Nottingham power rig there are results demonstrating that loading should be varied (Pearson et al. 2001).
The poor correlation between power during the STS transfer and the time needed in the five-chair rise might be explained by the good results of all subjects and the small standard deviation in five-chair rise indicating a ceiling effect in this particular measurement. Another explanation might be the different issues measured by the tests. The results of the five-chair rise have been shown to be associated with disability (Guralnik et al. 1994). Conversely, the introduced assessment measures on a biomechanical level. As the correlation between these measurements is poor, the biomechanical measurement of power during the STS transfer might be able to detect an early decline in muscle function, even when the functional status of performance (five-chair rise) is still sufficient. Furthermore, the five-chair-rise test is likely an insufficient measurement to detect differences in performance of standing up from a chair in a healthy population.
Our results might help to understand the misinterpreted curve of Fleming et al. (1991), who equated the incline of the curve with the power. This is not correct in terms of physics, but has a good correlation to power as we demonstrated.
The interpretation of the ground reaction-force curve is transferable to a curve derived from other force plates. If it is not possible to determine the exact time of the RP (T2–T3), which is necessary to calculate power, maximum ground-reaction force seems to be a sufficient surrogate to describe power during the STS transfer.
In conclusion, the study shows that the method presented is able to measure power during performance of a functional task. It might be able to detect decline in muscle function earlier than measurement of the functional status. As it is portable and the costs are considerably lower than those of the Nottingham power rig or isokinetic measurements, its use in clinical practice and research is sensible. Further investigation, including values of the right and left leg separately, might be useful in the assessment of pain treatment of the lower limb, and the evaluation of operative hip and knee replacement. Currently mainly subjective or observational methods (Lingard et al. 2001) are being used here to assess outcome.
References
Bassey E, Short A (1990) A new method for measuring power output in a single leg extension: feasibility, reliability and validity. Eur J Appl Physiol 60:385–390
Bassey E, Fiatarone M, O'Neill E, Kelly M, Evans W, Lipsitz L (1992) Leg extensor power and functional performance in very old men and women. Clin Sci (Colch) 82:321–327
Chandler J, Duncan P, Studenski S (1997) Choosing the best strength measure in frail older persons: Importance of task specifity. Muscle Nerve [Suppl] 5:47–51
Davies CT, White MJ, Young K (1983) Electrically evoked and voluntary maximal isometric tension in relation to dynamic muscle performance in elderly male subjects. Eur J Appl Physiol Occup Physiol 51:37–43
Evans W (2000) Exercise strategies should be designed to increase muscle power (editorial comment). J Gerontol A Biol Sci Med Sci 55: M309–310
Fleiss J (1986) The design and analysis of clinical experiments. Wiley, New York
Fleming B, Wilson D, Pendergast D (1991) A portable, easily performed muscle power test and its association with falls by elderly persons. Arch Phys Med Rehabil 72:886–889
Guralnik J, Simonsick E, Ferrucci L, et al (1994) A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 49:M85–94
Harridge S, Young A (2000) Strength and power. In: Evans J, Williams T, Beattie B, et al (eds) Oxford textbook of geriatric medicine, vol 2. Langton, Oxford
Hirschfeld H, Thorsteinsdottir M, Olsson E (1999) Coordinated ground forces exerted by buttocks and feet are adequately programmed for weight transfer during sit-to-stand. J Neurophysiol 82:3021–3029
Jozsi A, Campbell W, Joseph L, Davey S, Evans W (1999) Changes in power with resistance training in older and younger men and women. J Gerontol A Biol Sci Med Sci 54:M591–596
Kostka T, Rahmani A, Berthouze SE, Lacour JR, Bonnefoy M (2000) Quadriceps muscle function in relation to habitual physical activity and VO2max in men and women aged more than 65 years. J Gerontol A Biol Sci Med Sci 55:B481–488
Kralj A, Jaeger R, Munih M (1990) Analysis of standing up and sitting down in humans: definitions and normative data presentation. J Biomech 23:1123–1138
Lingard EA, Katz JN, Wright RJ, Wright EA, Sledge CB (2001) Validity and responsiveness of the Knee Society Clinical Rating System in comparison with the SF-36 and WOMAC. J Bone Joint Surg [Am] 83:1856–1864
Manchester D, Woollacott M, Zederbauer-Hylton N, Marin O (1989) Visual, vestibular and somatosensory contributions to balance control in the older adult. J Gerontol A Biol Sci Med Sci 44:M118–127
Martin J, Farrar R, Wagner B, Spirduso W (2000) Maximal power across the lifespan (see comments). J Gerontol A Biol Sci Med Sci 55:M311–316
Pearson SJ, Harridge SDR, Grieve DW, Young A, Woledge RC (2001) A variable inertial system for measuring the contractile properties of human muscle. Med Sci Sports Exerc 33:2072–2076
Rahmani A, Belli A, Kostka T, Dalleau G, Bonnefoy M, Lacour JR (1999) Evaluation of knee extensor muscles under non-isokinetic conditions in elderly subjects. J Appl Biomech 15:337–344
Roebroek M, Doorenbosch C, Harlaar J, Jacobs R, Lankhorst G (1994) Biomechanics and muscular activity during sit-to-stand transfer. Clin Biomech 9:235–244
Schenkman M, Hughes M, Samsa G, Studenski S (1996) The relative importance of strength and balance in chair rise by functionally impaired older individuals. J Am Geriatr Soc 44:1441–1446
Skelton D, Young A, Greig C, Malbut K (1995) Effects of resistance training on strength, power, and selected functional abilities of women aged 75 and older. J Am Geriatr Soc 43:1081–1087
Acknowledgements
We acknowledge the help of Wiebren Zijlstra, University of Groningen, who discussed our results, and Barbara Eichner, Bethesda Geriatric Hospital Ulm, who was responsible for data management. The study was supported by the Bethesda Geriatric Hospital Ulm, Academic Centre at the University of Ulm and Martin Conzelmann, Felix Platter Spital in Basel. This study complies with the current laws of Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lindemann, U., Claus, H., Stuber, M. et al. Measuring power during the sit-to-stand transfer. Eur J Appl Physiol 89, 466–470 (2003). https://doi.org/10.1007/s00421-003-0837-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-003-0837-z