
Abstract
The hydraulic calcium silicate-based (HCSB) or often called “bioceramic” sealers-fillers are rapidly gaining popularity among clinicians due to their superior biological, physicochemical properties and simplified clinical application. In addition, these materials can be successfully used with different root canal obturation techniques. This article will shortly introduce and discuss the most popular fourth and fifth type of HCSB sealers-fillers for root canal obturation, focusing on their clinical properties, applicability, and advantages.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Quick reference/description
Conventional techniques of root canal obturation have been successfully used by clinicians with a favorable prognosis of the endodontically treated teeth. A basic principle of traditional root canal obturation techniques, such as cold or warm (thermoplastic) compaction, is increasing the gutta-percha volume and minimizing the sealer film thickness to prevent seal deterioration. Development of HCSB sealers has significantly changed these principles of root canal obturation. There are five types of HCSB materials currently available. The first type includes materials based on Portland cement with or without radio-pacifier, with no additives and which are mixed with water. The second type has various additives (calcium oxide, calcium carbonate, hydroxyapatite), whereas in the third type, the water is replaced by alternative vehicles. The fourth- and fifth-type materials are tri-calcium silicate-based; however, the type 4 materials are mixed with water while type 5 are premixed and ready-to-use formulations. The specific physicochemical and biological properties of HCSB materials have made them suitable for use along with all obturation techniques, particularly with the single-cone obturation technique in modern endodontics.
Overview
Bioceramic materials | Indications | Rationale for use |
|---|---|---|
Flowable hydraulic calcium silicate-based materials | ||
iRoot®SP, EndoSequence® BC Sealer™ and TotalFill® BC Sealer™ | - For root canal sealing and permanent filling using cold and warm compaction or single-cone obturation techniques | - Its properties of bioactivity, biocompatibility and antibacterial activity are well-known - During setting, the sealers slightly expand to facilitate a good seal between the filling material and the dentin |
EndoSequence BC Sealer HiFlow and TotalFill® BC Sealer HiFlow™ | - For root canal sealing and permanent filling using warm compaction obturation techniques | - These sealers possess higher viscosity and have enhanced heat resistance for use with warm obturation techniques |
Bio-C Sealer and Bio-C Sealer ION + | - For root canal sealing and permanent filling using cold and warm compaction or single-cone obturation techniques | - Sealers possess all main biological and physicochemical properties of the flowable HCSB materials - Bio-C Sealer ION + is more viscous and more suitable with warm obturation techniques |
Well-Root ST | - For root canal sealing and permanent filling using cold and warm compaction or single-cone obturation techniques | - Well-Root ST has enhanced angiogenetic properties and low cytotoxicity, while other biological effects and physicochemical properties are comparable to other HCSB sealers |
CeraSeal | - For root canal sealing and permanent filling using cold and warm compaction or single-cone obturation techniques | - It has a shorter setting time and is highly resistant to washout - Biological, physicochemical properties and clinical applicability are comparable to other HCSB sealers |
BioRoot™ RCS | - For root canal sealing and permanent filling using cold compaction or single-cone obturation techniques | - BioRoot™ RCS is based on the Active Biosilicate Technology that allows the conversion of raw material to pure tri-calcium silicate - It is the fourth-type water-based bioceramic sealer, which is sensitive to the heat and desiccation, therefore should not be used with the warm obturation techniques |
Bioceramic-Coated (BC) Gutta- Percha Points | - For three-dimensional (3D) bonded root canal obturation at body temperature along with bioceramic sealers using cold obturation methods - Use of 150 series BC GP points and Pellets for 3D root canal obturation along with bioceramic sealers using warm obturation | - BC gutta-percha points are coated and impregnated with bioceramic nanoparticles, which results in a uniform monoblock with BC Sealer within the root canal |
Materials/Instruments
-
Fifth type premixed injectable HCSB sealer (iRoot®SP, EndoSequence® BC Sealer™, TotalFill® BC Sealer™, Bio-C sealer, Bio-C Sealer ION + , Well-Root ST, CeraSeal)
-
Heat-resistant premixed hydraulic calcium silicate-based sealer (EndoSequence BC Sealer HiFlow, TotalFill® BC Sealer HiFlow™)
-
Fourth type, water-based Active Biosilicate technology-based sealer or filler (BioRoot™ RCS)
-
BC gutta-percha points
-
Hand file
-
Special rotary instruments
-
Syringe
-
Disposable tips
Procedure
Conventional techniques of root canal obturation have been successfully used by clinicians with a favorable prognosis of the endodontically treated teeth. A basic principle of root canal obturation was increasing the gutta-percha volume and minimizing the sealer film thickness to prevent seal deterioration. Development of novel HCSB sealers-fillers has significantly changed these principles of root canal obturation. The various biological and physicochemical properties of these materials have made them favorable for use not only with cold or warm compaction techniques but also along with the single-cone obturation technique in modern endodontic.
Flowable hydraulic calcium silicate-based obturation materials
Currently, flowable HCSB materials are available in the form of premixed pastes (fifth type) or powder/liquid formulations (fourth type). The premixed formulations are not water-based like powder/liquid sealers and have different properties and applications; therefore, the clinical uses should be strictly selected following the manufacturer’s recommendations, recent knowledge and scientific evidence. These flowable HCSB materials can be utilized as biologic fillers or sealers along with regular or BC gutta-percha points and several obturation techniques.
iRoot®SP, EndoSequence® BC Sealer™ and TotalFill® BC Sealer™
A Canadian company, Innovative BioCeramix Inc., Vancouver, introduced the first premixed and ready-to-use HCSB material, iRoot SP injectable root canal sealer (iRoot®SP). The material is available as EndoSequence® BC Sealer™ in North America from Brasseler, USA since 2008 and as TotalFill® BC Sealer™ in Europe from FKG Dentaire, Switzerland. The sealers are marketed as pre-loaded syringes with disposable tips (Fig. 1). All three products are chemically identical and are composed of calcium silicates, calcium phosphate monobasic, zirconium oxide and fillers, possesses similar biological and physicochemical characteristics, and handling properties. They are also equally clinically effective.

Commercially available flowable HCSB sealers: a iRoot®SP, bEndoSequence® BC Sealer™, c TotalFill® BC Sealer™
TotalFill® BC Sealer™, EndoSequence® BC Sealer™ and iRoot®SP are convenient, premixed and ready-to-use injectable white hydraulic pastes that are used for sealing and permanent root canal filling applications in both vital and necrotic pulp cases. The physiochemical and biological properties of these materials like bioactivity, biocompatibility and antibacterial activity are widely evaluated and well-known. During setting, the sealers tend to expand slightly, thus facilitating a reliable seal between the paste, core filling material and the dentin. Furthermore, these materials are highly flowable and ensure superior penetrability into root canal irregularities and dentinal tubules.
The use of these sealers is clinically appealing due to premixed and ready-to-use formulas, simple and fast, time-saving delivery of the materials. Direct delivery and immediate application of the sealers from the syringe into the root canal are possible with disposable tips or via traditional placement techniques.
The moisture in the dentinal tubules induces the setting reaction of HCSB sealers. The sealers use the residual root canal moisture to form hydroxyapatite and ensure optimal adhesion between the paste and the dentin via mineral infiltration layer and chemical bonding. The major advantages of these sealers are:
-
High pH during setting
-
Antimicrobial activity
-
Biocompatibility
-
Bioactivity
-
Prolonged dimensional stability after setting
-
Easy manipulation and application
-
Economic packaging
-
Bond between cement and dentin
-
Limited microorganism growth
-
Conservative canal preparation for obturation
These materials have a working time of more than 4 h at room temperature and a setting time of 4 h. The setting time depends on the presence of moisture in radicular dentin and can go up to 10 h in over-dried root canals. Increase in body temperature decreases setting time and increases flowability. These materials are designed to be utilized with all cold and warm root canal obturation techniques. Endodontic retreatment is not more complicated or difficult when these sealers are used along with gutta-percha points. The fillings can be removed using traditional techniques.
EndoSequence BC Sealer HiFlow and TotalFill® BC Sealer HiFlow™
Some manufacturers have proposed that warm root canal obturation techniques cannot be performed using conventional HCSB sealers as heat application can significantly alter material properties. Therefore, the manufacturers developed and introduced two new formulations and modifications of premixed injectable HCSB sealers. The novel HiFlow formula of the EndoSequence® BC Sealer™ and TotalFill® BC Sealer enhances heat resistance (up to 220° C), has lower viscosity heating and is more radiopaque. These properties optimize it for use with warm obturation techniques (Fig. 2). However, the necessity of these novel materials is still questionable as it is not confirmed that temperatures within root canals reach such high values. Moreover, the existing scientific evidence demonstrates little to no impact of the heat on the properties of the premixed/fifth generation pastes. The negative impact of the heat on the properties of the HCSB materials was confirmed just for fourth-type water-based formulations.

a BC and b TotalFill formulations for warm root canal obturation techniques
Bio-C Sealer and Bio-C Sealer ION +
A novel premixed, ready-to-use, injectable HCSB material, Bio-C Sealer (Angelus, Londrína, PR, Brazil), has been developed for root canal sealing and permanent filling during endodontic therapy. It is composed of calcium silicates, calcium oxide, calcium aluminate, iron oxide, zirconium oxide, silicon dioxide and dispersing agents packed in a single syringe (Fig. 3a). Bioceramic particles account for almost 65% of the material, while polyethylene glycol establishes the material’s viscosity and allows its removal and cleaning following obturation. The manufacturers claim that its bioactivity is due to the release of calcium ions that stimulate hard tissue formation. Bio-C Sealer ION + (Angelus, Londrína, PR, Brazil) is the latest modification of Bio-C Sealer with a slightly changed microstructural and chemical composition. The material possesses all the main biological properties of the previous formulation; however, it is slightly more viscous, release more Ca2+, MG2+ and Si2+ ions, and is suitable to be used for both cold and warm vertical obturation techniques, according to the manufacturer (Fig. 3b).

a Bio-C Sealer (a) and (b) more viscous Bio-C Sealer ION + sealer are ready-to-use HCSB pastes suitable with cold and warm obturation techniques
Both material’s working time is 60 min. They have a setting time of 120–240 min after insertion into the root canal, which depends on the moisture content in the root canal. The pH of materials is 12.0–12.5 and both are highly radiopaque (≈ 7 mm of aluminum scale). The sealers are partially absorbable, possess low solubility and do not shrink after setting. According to the manufacturer, all root canal obturation techniques can be performed using these sealers. The more viscous ION + formula can be more advantageous for thermoplastic obturation than its original version; however, there is no solid scientific evidence to confirm this hypothesis. The sealers should not be stored in a refrigerator. As the presence of moisture in the root canal initiates the setting reaction of the sealers, it is crucial to not over-dry the canal using paper points. Conventional gutta-percha removal approaches can aid in removing the materials from the canals.
Well-Root ST
Well-Root ST (Vericom, Gangwon-Do, Korea) is a HCSB root canal sealer (Fig. 4). It is a premixed, injectable, ready-to-use bioactive material. It is a hydrophilic paste that needs the presence of water for setting. Well-Root ST is indicated for permanent obturation of root canals along with gutta-percha points and different obturation techniques. It is composed of calcium silicate, zirconium oxide, thickening agents and fillers. As per ISO 6876:2012, Well-Root ST has a setting time of 25 min at 100% humidity conditions. However, the setting time can be more than 2.5 h in normal root canals as mentioned by the manufacturer. It has good angiogenetic properties and low cytotoxicity, and similar biological effects as Biodentine, ProRoot MTA or other HCSB materials.

Well-Root ST sealer in pre-loaded ready-to-use syringe
CeraSeal
Another novel premixed endodontic sealer that contains zirconium oxide, calcium silicates and a thickening agent is known as CeraSeal (Meta Biomed Co., Cheongju, Korea). It is a HCSB sealer that has enhanced flowability and sealing ability according to the manufacturer. Presence of moisture within the dentinal tubules and chemical reaction of calcium silicate cause crystallization of calcium hydroxide, which aids in achieving a hermetic seal of the root canal and prevents bacterial influx and propagation. As other similar products, CeraSeal is dimensionally stable, does not shrink or expand in the root canal and prevents from fractures or root infractions by maintaining volumetric stability. It can be used along with all root canal filling techniques, including the single-cone obturation technique.
CeraSeal has a shorter initial setting time making it highly resistant to washout. It induces extensive calcium ion release, gradually hardens by absorbing the moisture within the root canal. CeraSeal is white in color and esthetic. It has a setting time of about 3.5 h. It has an alkaline pH (12.73), a flowability of 23 mm and a high radiopacity (≈ 8 mm of aluminum). It is marketed as a 2 g premixed syringe with intra-canal cannulas or tips (Fig. 5). CeraSeal is similar to iRoot®SP in composition and properties and the only difference is that calcium hydroxide and calcium monobasic from iRoot®SP are replaced by 1,3-propanediol in CeraSeal.

Premixed CeraSeal sealer is suitable to be used with all conventional root canal obturation techniques
BioRoot™ RCS
Septodont (Saint-Maur-des-Fosses, France) introduced a new generation of hydraulic root canal sealer or filler based on the Active Biosilicate Technology known as BioRoot™ RCS. The technology facilitates conversion of raw material to pure tri-calcium silicate without the presence of calcium sulfate and aluminate in the final product. BioRoot™ RCS was marketed in 2015. It is available as a powder containing tri-calcium silicate and zirconium oxide, and a water-based liquid containing calcium chloride and a water-soluble polymer. It demonstrates antimicrobial activity, can induce deposition of hard tissues and has a lower cytotoxicity than other traditional resin-based root canal sealers.
BioRoot™ RCS is extremely biocompatible and is free of monomers. It decreases the risk of any adverse tissue reactions. Clinical failures due to potential bacterial growth can be prevented by its antimicrobial properties. Additionally, the crystallization of BioRoot™ RCS results in a hermetic seal for improved resistance to micro-leakage. It is bioactive and induces bone physiological processes and mineralization of dentinal structure, which generates a suitable environment for periapical healing. Its bioactive properties include biocompatibility, alkaline pH, hydroxyapatite formation, sealing properties and mineralization.
BioRoot™ RCS is used by manual mixing of the powder (1 spoon) and the liquid (5 drops) in a simple spatulation motion. It has a working time of about 15 min and a setting time of less than 4 h in the root canal. Additionally, it also shows a tight seal with the gutta-percha and the dentin (Fig. 6) along with a proper radiopacity (≈5 mm of aluminum). The mixed cement has a smooth consistency with good flow that increases following placement in the root canal due to the body temperature. BioRoot™ RCS has a film thickness of 45 µm and a flow rate of 26 mm.

BioRoot™ RCS sealer available as a powder/liquid system, requiring manual mixing before application
BioRoot™ RCS is the fourth-type water-based sealer, which is not suitable to be used with warm gutta-percha obturation techniques. It is recommended for use only with cold lateral compaction or single-cone obturation techniques because heat production during thermoplastic obturation can lead to the desiccation of the material, adversely affect its film thickness and flowability. Currently, the single-cone technique is highly reccomended while using HCSB sealers/fillers.
Bioceramic-coated (BC) gutta-percha points for root canal obturation
Despite the lack of solid evidence that BC gutta-percha points when used with HCSB sealers offer better root canal sealing than conventional gutta-percha points, some manufacturers still recommend using BC points along with TotalFill or BC Sealer for a tight, hermetic seal. BC gutta-percha points are coated and impregnated with bioceramic nanoparticles that permits its bonding with BC Sealer resulting in a uniform monoblock within the root canal (Fig. 7a). The use of BC points and BC sealer facilitates 3D bonded root canal obturation at body temperature. The combined use of EndoSequence BC Points/TotalFill BC Points and EndoSequence® BC Sealer™/TotalFill® BC Sealer™ as a “monoblock” can reinforce the root and markedly enhance its fracture resistance following therapy (Fig. 7b).

a EndoSequence and b TotalFill BC points, 150 Series BC points and BC Pellets (left to right)
It has been proposed that while using warm obturation techniques, extreme heat can ‘dry’ the HCSB sealers and alter the material properties, which can compromise the quality of obturation. Hence, when a clinician prefers a warm obturation approach, the use of 150 series BC GP and Pellets was recommended. The 150 gutta-percha series containing bioceramic nanoparticles melt at 150 °C and are usually compatible with most thermoplastic heat ‘guns’ for backfilling of root canals. These gutta-percha points and backfilling pellets with lower melting temperatures aids in avoiding the application of excessive heat. However, it should be highlighted that these precautions should be applied just only for fourth-type water-based HCSB sealers, like BioRoot™ RCS, as the premixed formulations are not sensitive to heat and desiccation.
Sealer delivery methods
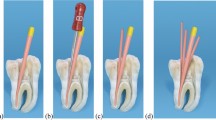
Several approaches can be used to deliver flowable HCSB sealers or fillers to cleaned, shaped and dried root canals. The popular methods of sealer delivery are injection of the material, use of special rotary endodontic instruments and coating of a hand file or master gutta-percha point with a sealer for application to the canal space and walls (Fig. 8). The sealing ability and sealer penetration into dentinal tubules are significantly governed by the sealer placement approaches. When root canals are obturated with the single-cone obturation technique, the sealer placement method is crucial, while the quality of obturation is not affected with the lateral or vertical compaction of the filling materials.

Delivery of flowable hydraulic calcium silicate materials using injection via tip syringe, lentulo spiral, endodontic instruments or master gutta-percha point (left to right)
A ‘tip delivery’ approach is commonly used to deliver premixed sealers or fillers. After removal of the cap from the material’s syringe, a plastic tip or cannula is connected to the syringe hub with a clockwise twist. Plastic cannulas are flexible and can be bent to provide access to the root canal. The syringe tip should be placed in the canal at the level of the apical and middle third.
According to the size of the prepared root canal, a small amount of the product (usually about 1–2 reference markings) should be smoothly injected into the root canal by gently pressing the plunger of the syringe and withdrawing the tip till the sealer is visible at the root canal orifice. The walls of the root canal can additionally be coated and the sealer better distributed inside the root canal space using a gutta-percha point, small hand file (size #15 or #20) or special rotary endodontic instrument like a Lentulo spiral. The plastic cannula should be disconnected from the syringe with a counterclockwise twist and disposed after every application. The syringe should be cleaned on the outside by removing the excess paste. It should be tightly capped and placed in a foil pouch for storage in a dry place at the appropriate temperature.
When the powder/liquid form of HCSB sealers (BioRoot™ RCS) is used, it should be manipulated following the manufacturer’s instructions and placed in the root canal using a pre-fitted gutta-percha point. Alternatively, a small plastic syringe and tip can be used to deliver the freshly mixed sealer. After inserting the mixed sealer in the back of a disposable syringe, the plunger is replaced, and the plastic tip is attached (Fig. 9). The sealer is injected in the root canal about 2 mm short of the established working length by gently compressing the syringe plunger and withdrawing the tip till the sealer is visible at the root canal orifice. The use of small syringes for delivering freshly mixed sealer can be clinically favorable to ensure better sealer distribution within the root canal.

a Freshly mixed BioRoot™ RCS placed into the syringe, b the plunger reinserted and c adjusted flexible cannula capillary tip
Pitfalls & Complications
-
Warm root canal obturation techniques cannot be performed using fourth-type water-based HCSB sealers as heat application can adversely affect properties, film thickness and paste flowability.
-
The residual dentinal tubules moisture is needed to initiate the setting of premixed fifth-type HCSB sealers; therefore, intra-canal dentin desiccation should be avoided, leading to gently dry the root canal before obturation.
Further Reading
Sfeir G, Zogheib C, Patel S, Giraud T, Nagendrababu V, Bukiet F (2021) Calcium silicate-based root canal sealers: a narrative review and clinical perspectives. Materials 14:3965. https://doi.org/10.3390/ma14143965
Aksel H, Makowka S, Bosaid F, Guardian MG, Sarkar D, Azim AA (2021) Effect of heat application on the physical properties and chemical structure of calcium silicate-based sealers. Clin Oral Investig 25:2717–2725
Donnermeyer D, Ibing M, Bürklein S, Weber I, Reitze MP, Schäfer E (2021) Physico-chemical investigation of endodontic sealers exposed to simulated intracanal heat application: hydraulic calcium silicate-based sealers. Materials 14:728
Atmeh AR, Hadis M, Camilleri J (2020) Real-time chemical analysis of root filling materials with heating: guidelines for safe temperature levels. Int Endod J 53:698–708
Donnermeyer D, Bürklein S, Dammaschke T, Schäfer E (2019) Endodontic sealers based on calcium silicates: a systematic review. Odontology 107:421–436
Duarte MAH, Marciano MA, Vivan RR, Tanomaru Filho M, Tanomaru JMG, Camilleri J (2018) Tricalcium silicate-based cements: properties and modifications. Braz Oral Res 32:111–118
Komabayashi T, Colmenar D, Cvach N, Bhat A, Primus C, Imai Y (2020) Comprehensive review of current endodontic sealers. Dent Mater J. https://doi.org/10.4012/dmj.2019-288
Primus CM, Tay FR, Niu LN (2019) Bioactive tri/dicalcium silicate cements for treatment of pulpal and periapical tissues. Acta Biomater 96:35–54. https://doi.org/10.1016/j.actbio.2019.05.050
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Drukteinis, S. Hydraulic calcium silicate-based materials for root canal obturation. Clin Dent Rev 6, 1 (2022). https://doi.org/10.1007/s41894-022-00115-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41894-022-00115-8