
Abstract
The fourth and fifth types of hydraulic calcium silicate-based sealers are rapidly gaining popularity among clinicians due to their exceptional biological, physicochemical properties, and simplified clinical application. These materials can be used with all root canal obturation techniques, such as cold lateral or warm vertical compaction techniques, and especially a single-cone technique. Although all obturation techniques are equally effective and not superior to each other, the single-cone obturation technique is easier to apply, is more time-consuming, and clinically appealing in modern endodontics. This chapter will introduce and discuss the most popular hydraulic calcium silicate–based sealers and root canal obturation techniques used in conjunction with these materials.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Root canal obturation
- Lateral compaction
- Warm vertical condensation
- Single cone
- Hydraulic calcium silicate
1 Introduction
Clinicians have used the lateral compaction and thermoplastic root canal obturation techniques all around the world with high clinical success and acceptable long-term prognosis of the root-filled teeth [1, 2]. However, these techniques require a quite long learning curve, time-consuming, and difficult to undertake [3]. Additionally, obturation of the root canal system involves maximizing the amount of gutta-percha and decreasing the thickness of sealer. Epoxy resin, calcium hydroxide, and zinc oxide eugenol–based sealers significantly shrink and resorb over time; therefore, a thin layer of sealer has always been advocated to avoid deterioration of the seal [1].
Introduction of hydraulic calcium silicate–based cements has changed the root canal obturation standards and strategies [4, 5]. The main advantages of these materials are biocompatibility, bioactivity, and high antimicrobial activity [5]. Meanwhile, due to the no shrinkage and long-term dimensional stability, these materials can be used in larger volumes without the need to increase the amount of gutta-percha in the root canal, as it is a sealer- or filler-based obturation [6]. The hydraulic calcium silicate–based sealers are recommended to be used with a single-cone obturation technique, while the purpose of the gutta-percha cone is to increase hydraulic pressure inside the root canal and drive the sealer into isthmuses, irregularities, and dentinal tubules [6, 7]. The new obturation technique is simple to apply even for the inexperienced clinician [8].
The new materials and obturation technique have been extensively compared in vitro and in vivo studies and have shown similar or superior results in comparison to the conventional obturation materials and techniques [9,10,11,12,13,14]. Although the long-term randomized clinical trials are needed to prove the long-term efficacy of the single-cone technique, the preliminary retrospective clinical investigations demonstrated an overall success rate of 90.9% [15]. The hydrophilic nature, sealability, biocompatibility, antibacterial property, bioactivity, and ease of delivery have made hydraulic calcium silicate–based sealers promising materials to be used in conjunction with the single-cone obturation technique in modern endodontics [14, 16,17,18].
2 Flowable Hydraulic Calcium Silicate–Based Obturation Materials
A wide variety of flowable hydraulic calcium silicate–based materials are available on the market [19]. Majority of them are premixed pastes in the syringes, while few materials are produced as liquid/powder formulations [6, 18]. However, it should be mentioned that premixed materials are not water-based in comparison to liquid/powder sealers. Therefore, there are differences in the properties, applicability, and clinical use of these flowable hydraulic calcium silicate–based materials, which can be used as sealers or biologic fillers in conjunction with a regular or bioceramic coated gutta-percha point and different obturation techniques [4, 20, 21].
2.1 iRoot®SP, EndoSequence® BC Sealer™, and TotalFill® BC Sealer™
The first premixed and ready-to-use hydraulic calcium silicate–based material was developed and introduced in 2007 by a Canadian company Innovative BioCeramix, Inc., Vancouver. The material was launched as iRoot SP injectable root canal sealer (iRoot®SP). Since 2008, this premixed sealer is available in North America from Brasseler USA as EndoSequence® BC Sealer™. Recently, this material has also been marketed in Europe as TotalFill® BC Sealer™ by FKG Dentaire, Switzerland. The materials are packaged in pre-loaded syringes and are supplied with disposable tips (Fig. 1). All three materials are the same in chemical composition (calcium silicates, zirconium oxide, calcium phosphate monobasic, and fillers), possess the same physicochemical and biological properties, handling characteristics, and are equally clinically effective [6, 12, 19].

Commercially available flowable hydraulic calcium silicate–based sealers: iRoot®SP (a), EndoSequence® BC Sealer™ (b), TotalFill® BC Sealer™ (c)
iRoot®SP, EndoSequence® BC Sealer™, and TotalFill® BC Sealer™ are premixed, convenient, ready-to-use injectable white hydraulic cement pastes developed for permanent root canal filling and sealing applications. Indications for use include permanent obturation of the root canal following vital and necrotic pulp cases [12, 18].
These materials are widely tested and are recognized for their biological properties such as biocompatibility, bioactivity, and antibacterial activity, as well as for excellent physicochemical properties [13, 20,21,22]. Sealers do not shrink during setting, but tend to expand slightly and being extremely flowable provide an excellent seal between the dentin and filling material [5, 22, 23, 26].
These materials are also distinguished by its ease of use [4, 15]. Materials are launched as a premixed and ready to use. Subsequentially, it saves time and provides a perfect consistency, reproducible between applications. They can be applied immediately and delivered directly from the syringe into the root canal using the disposable tips provided or can be used with traditional placement methods [4, 6].
Unlike the majority conventional hydrophobic sealers, the setting reaction of these hydraulic calcium silicate–based sealers is induced by the moisture present in the dentinal tubules [22, 24, 25]. Using this moisture, sealers form hydroxyapatite, to ensure optimum chemical adhesion between the dentin and the cement [21]. Studies have demonstrated that TotalFill BC Sealer has a stronger bond than other commonly used cements regardless of the moisture level inside the root canal [26]. Main advantages of these three sealers are a high pH during setting, antimicrobial activity, biocompatibility, and bioactivity when set, long-term dimensional stability [25, 27, 28]. Clinically appealing properties, such us easy manipulation and deployment, economic packaging, bond between cement–dentin, limited microorganism growth, and quite conservative canal preparation, needed for obturation.
The working time for these materials can be more than 4 h at room temperature, while the setting time is 4 h. However, in overdried root canals, the setting time can increase up to 10 h. The setting time of the sealer is highly dependent on the presence of moisture in the radicular dentin. Additionally, the body temperature increases the flowability and decreases the setting time [29]. These materials are designed and can be used with all root canal obturation techniques. It has been shown that endodontic retreatment procedures are not more difficult or complicated when these materials are used in conjunction with gutta-percha points—conventional techniques can be used for the removal of the fillings [15, 30].
2.2 EndoSequence BC Sealer HiFlow and TotalFill® BC Sealer HiFlow™
It has been shown that water-based hydraulic calcium silicate sealers cannot be used with the warm root canal obturation techniques because heat dramatically changes properties of the materials [31,32,33]. However, many dental practitioners have been using warm vertical compaction technique for decades and were not ready to make the transition to the simpler single-cone obturation technique [8]. Due to the recent needs, the two distinct formulations and modifications of the same premixed hydraulic calcium silicate–based sealers were introduced [34]. According to manufacturers, the new HiFlow formula of the original BC and TotalFill Sealers was designed for higher heat resistance (up to 220 °C), exhibits a lower viscosity when heated, and is more radiopaque, making it optimized for warm obturation techniques [29] (Fig. 2). However, nowadays there is no solid scientific evidence confirming superior properties and clinical advantages of the modified high viscosity sealers [29, 35]. It is not clearly confirmed that the real temperature inside root canals during the thermoplastic obturation can reach these high values [31]. Thus, the necessity of these new formulations of the original BC and TotalFill sealers is still questionable [29].

BC (a) and TotalFill (b) formulations for warm root canal obturation techniques
2.3 Bio-C Sealer
The Bio-C Sealer (Angelus, Londrína, PR, Brazil) is a new, premixed, ready for use, injectable hydraulic calcium silicate–based material developed for permanent filling and sealing during root canal treatment [36]. Bio-C Sealer is available in a single syringe, composed of calcium silicates, calcium aluminate, calcium oxide, zirconium oxide, iron oxide, silicon dioxide, and dispersing agents (Fig. 3a) [21]. Overall, approximately 65% of the material is composed by bioceramic particles, while the polyethylene glycol is used to achieve the viscosity of the material and facilitate its removal and cleaning after obturation procedures [21]. According to the manufacturer, its bioactivity is attributed to the release of calcium ions that stimulate the formation of mineralized tissue [36]. However, to date, few studies have evaluated its effects on periapical tissues and related cells [36, 37]. The working time is 60 min; the average setting time is 120 min (maximum up to 240 min) after insertion into the root canal and highly depends on the moisture inside the root canal [36]. Material is highly alkaline—pH 12.5, has high radiopacity (equivalent to 7 mm of aluminum scale), does not shrink at the setting time, and is non-soluble or absorbable. According to the manufacturer, sealer can be used with different root canal obturation techniques, including a single-cone [36]. It is strongly recommended to not overdry root canal with paper points, as the moisture from the dentin tubules is needed to initiate the material’s setting reaction. Material can be removed from the root canal during endodontic retreatment using conventional gutta-percha removal techniques. It is recommended not to store the sealer in refrigerator.

The recently introduced hydraulic calcium silicate sealers–fillers: Bio-C Sealer (a), Well-Root ST (b), CeraSeal (c)
2.4 Well-Root ST
Another sealer based on tricalcium silicate is Well-Root ST (Vericom, Gangwon-Do, Korea) (Fig. 3b). This sealer is a premixed, ready-to-use, injectable, bioactive root canal sealer based on tricalcium silicate, which is a hydrophilic sealer that requires water presence to set and harden [27, 38]. The material is developed for permanent obturation of the root canal. The composition of Well-Root as described by the manufacturer includes zirconium oxide, calcium silicate, filler, and thickening agents [22, 38]. The material is hydrophilic and uses moisture in dentinal tubules to initiate and complete its setting reactions. The setting time is 25 min, measured according to ISO 6876:2012 (100% humidity conditions). However, in normal root canals, the setting time can be more than 2.5 h as reported by the manufacturer [38]. The Well-Root ST should be used in conjunction with gutta-percha points. It has been shown that the Well-Root ST possesses good angiogenetic properties, has a similar biological effects and low cytotoxicity as ProRoot MTA or Biodentine [39].
2.5 CeraSeal
CeraSeal (Meta Biomed Co., Cheongju, Korea) is a newly launched premixed endodontic sealer containing calcium silicates, zirconium oxide, and thickening agent. According to the manufacturer, CeraSeal is hydraulic calcium silicate–based sealer, which possesses superior sealing ability [40]. Moisture in the dentinal tubules and calcium silicate’s chemical reaction produce crystallization of calcium hydroxide. The material guarantees the hermetic seal of the root canal and prevents the influx and propagation of bacteria [41]. The material is dimensionally stable, does not shrink or expand in the root canal, and prevents from root infractions or fractures by keeping its stable volume [42]. The single-cone obturation technique can be used with this material [40]. Due to the shorter setting time, the material is highly resistant to the washout [41]. CeraSeal induce a high degree of Ca2+ release. This product characteristically cures slowly by absorbing the ambient water inside the root canal. It is white and esthetic.
CeraSeal setting time is approximately 3.5 h, material possesses high pH of 12.73, flowability—23 mm, and radiopacity (equivalent to 8 mm of Al). The material is selling as package of 2 g premixed syringe with intra canal tips cannulas (Fig. 3c). According to manufacturer, the composition and properties of CeraSeal are very similar to iRoot®SP, while 1,3-propanediol instead of calcium phosphate monobasic and calcium hydroxide is used in CeraSeal [40].
2.6 BioRoot™ RCS
BioRoot™ RCS is the new generation of root canal sealer/filler from Septodont (Saint-Maur-des-Fosses, France) which benefits from the Active Biosilicate Technology. This unique technology allows transforming the raw material to the pure tricalcium silicate, without any presence of aluminate and calcium sulfate in the final product [13, 43].
BioRoot™ RCS is a hydraulic cement, marketed on 2015 and presented as a powder composed of tricalcium silicate, zirconium oxide, and a liquid, which is mainly water-based with additions of calcium chloride and a water-soluble polymer [25, 32]. BioRoot™ RCS has been reported to induce in vitro the production of angiogenic and osteogenic growth factors by human periodontal ligament cells [44]; moreover, it has a lower cytotoxicity than other conventional root canal sealers, may induce hard tissue deposition [45, 46], and has antimicrobial activity [47].
BioRoot™ RCS is free of monomers, highly biocompatible, and reduces the risks of adverse tissue reaction [43]. The antimicrobial properties of BioRoot™ RCS prevent bacterial growth leading to clinical failures [13, 47]. In addition, BioRoot™ RCS crystallization creates a tight seal within the dentin tubules for improved resistance to microleakage. BioRoot™ RCS is bioactive by stimulating bone physiological process and mineralization of the dentinal structure. Therefore, it creates a favorable environment for periapical healing and bioactive properties including biocompatibility, hydroxyapatite formation, mineralization of dentinal structure, alkaline pH, and sealing properties.
BioRoot™ RCS was designed to be used by manually mixing powder part (1 spoon) with the liquid part (5 drops) by simple spatulation; the working time is around 15 min and the setting time is less than 4 h in the root canal [48]. In addition, BioRoot™ RCS displayed a tight seal with the dentin and the gutta-percha (Fig. 4) and an appropriate radiopacity (5 mm of aluminum). The mixed paste is of smooth consistency with good flow which even more increases after placement in the root canal (at body temperature). It has been shown that the flow rate is 26 mm and film thickness is 45 μm [43].

BioRoot™ RCS sealer available as a powder/liquid system, requiring manual mixing before application
BioRoot™ RCS was designed to simplify the obturation techniques of root canal, by ease of mixing and use, its optimized consistency, and elimination of the need for a warm gutta-percha technique [4]. It has been proposed that BioRoot™ RCS should only be used with cold root canal filling techniques, as the heat generated during thermoplastic obturation can negatively affect the flowability and film thickness of the material [32]. In recent times, the single-cone technique was suggested for use with hydraulic calcium silicate cements [7].
3 Bioceramic-Coated (BC) Gutta-Percha Points for Root Canal Obturation
There is still the lack of solid scientific evidence that BC gutta-percha points in conjunction with hydraulic calcium silicate–based cements ensure significantly better root canal sealing in comparison to conventional gutta-percha and hydraulic calcium silicate cements fillings [12, 49]. It has been claimed that standard gutta-percha points can be used with BC Sealer or TotalFill, but for a tight, gap-free seal, manufacturers recommend use BC Points [18]. BC Points are impregnated and coated with bioceramic nanoparticles to allow for bonding with BC Sealer producing the uniform monoblock inside the root canal space (Fig. 5). The benefit of using BC Sealer and BC Points is that three-dimensional bonded root canal obturation can be achieved at body temperature [12]. It has been demonstrated that combined use of TotalFill® BC Sealer™/EndoSequence® BC Sealer™ and TotalFill BC Points/EndoSequenc BC Points can reinforce the root significantly increasing the fracture resistance after treatment [29].

EndoSequence (a) and TotalFill (b) BC points, 150 Series BC points and BC Pellets (left to right)
It has been shown that the excessive heat can “dry out” the hydraulic calcium silicate–based sealers and thus change the properties of the materials, potentially compromising the quality of root canal obturation [31, 32]. Therefore, the manufacturer’s suggested if a warm vertical compaction technique with original formulations of BC or TotalFill sealers is preferred by the clinician, it is recommended to use 150 series BC GP and Pellets. This new line of lowering melting temperature gutta-percha points and backfilling pellets has been introduced to avoid applying excessive heat, thus making vertical compaction using BC/TotalFill sealers a clinically possible. The 150 series bioceramic nanoparticles containing gutta-percha melt at 150 °C and are compatible with most thermoplastic heat “guns” for the backfilling of the root canals. However, it should be highlighted that these manufacturers’ recommendations do not have any solid scientific background. In opposite, recent investigations demonstrated that BC series sealers can be heated and used with thermoplastic gutta-percha obturation techniques, as they are not water-based materials [29, 31].
4 Sealer Delivery Methods
Flowable hydraulic calcium silicate–based sealers/fillers can be delivered to the shaped, cleaned, and dried root canals using different methods. The most popular are injecting the material, using special rotary instruments and coating the master gutta-percha point or a hand file with a sealer to apply it to the canal walls and space (Fig. 6). It has been concluded that the sealer placement methods can play a significant role in the sealing ability and penetrability of the sealers into dentinal tubules [48]. However, it also has been shown that the sealer placement technique is important if root canals are obturated using single-cone obturation method, but not affect the quality of obturation when lateral compaction is used [49].

The flowable hydraulic calcium silicate materials can be delivered using (left to right) injection via tip syringe, Lentuo spiral, endodontic instruments, or master gutta-percha point
Premixed sealer/fillers usually are delivered using so-called “tip delivery method,” After the syringe cap removal from the material’s syringe, gently attach a tip (plastic cannula) with a clockwise twist to the hub of the syringe. Plastic tips are flexible and can be easily bent to facilitate access to the root canal. According to the manufacturers, the tip of the syringe should be inserted into the canal at the level of the middle-apical third [50]. The small amount (approximately 1–2 reference markings, depending on the size of the prepared root canal) of the material should be gently and smoothly injected into the root canal by compressing the plunger of the syringe. Using a small hand file (size #15 or #20) or gutta-percha point, root canal walls are lightly coated with the sealer. After each application, the plastic tip should be removed from the syringe with a counterclockwise twist and discarded. The outside of the syringe should be cleaned, excess paste removed. and the syringe cap tightly placed onto the syringe hub. After use, the syringe should be placed into the foil pouch and stored in a dry area at the room temperature.
If the powder/liquid formulation of the hydraulic calcium silicate–based sealer is used (for example, BioRoot™ RCS), the sealer should be mixed according to the manufacturer’s instructions and inserted into the root canal using pre-fitted gutta-percha point [1]. However, the freshly mixed material also can be delivered using small plastic syringes and cannulas. After that material is inserted into the back of the single-use syringe, the plunger is reinserted into the syringe, and the plastic cannula is adjusted (Fig. 7). The sealer is injected into the root canal approximately 2 mm shorter than the determined WL gently pressing the plunger of the syringe and withdrawing the cannula until the sealer was visible at the orifice of the root canal. Such an adapted use of the small syringes for freshly mixed sealer delivery can be clinically appealing and ensure the better sealer distribution in the root canal space.

Freshly mixed BioRoot™ RCS is placed into the syringe (a), the plunger reinserted (b) and flexible cannula-capillary tip is adjusted (c)
5 Root Canal Obturation Techniques
The flowable hydraulic calcium silicate–based cements can be used with all root canal obturation techniques. Root canals can be obturated using cold lateral compaction, warm vertical compaction, or “single-cone” techniques and their modifications [4, 19]. However, there is solid evidence that all techniques can be equally effective for root canal obturation if they are used following indications and recommendations [4, 6, 17].
5.1 Cold Lateral Compaction
Cold lateral condensation/compaction of gutta-percha is the most popular obturation method used throughout the world for many decades [1, 50, 51]. Root canal obturation procedure using hydraulic calcium silicate–based sealers in conjunction with gutta-percha points is not different from that when conventional sealers are used [4, 25].
After root canal preparation, the paper points corresponding to the last instrument used to shape the canal are selected and gently inserted into the root canal to the full working length to dry it. It should be mentioned that it is critically important to not overdry root canals when hydraulic calcium silicate cements are used for obturation, as some moisture is needed for the setting of these materials [13, 49, 52]. The root canal is dry enough but not overdried if the 3–4 mm of the tip of the paper point are wet after point removal. It indicates that there is some moisture which will be sufficient to initiate the hydration of the hydraulic calcium silicate–based sealer and setting [49, 53]. When the root canal is ready for obturation, the master gutta-percha point is selected (Fig. 8a). It should match the last instrument used to shape the canal in size/diameter and taper [54, 55]. The cone’s resistance to displacement or “tug back” indicates its suitability. When proper gutta-percha point is selected, the periapical radiograph should be taken, to confirm the correct placement of the cone. Subsequently, the sealer is applied to the root canal walls and space using the preferred delivery method. The tip of the master gutta-percha point is covered with a small amount of the sealer and slowly inserted into the root canal to the final working length. The selected pre-fitted spreader is used for gutta-percha compaction. Preferably, it should be inserted along with master gutta-percha point to within 1–2 mm from working length [51] (Fig. 8b). However, in the curved root canals, the penetration depth of the spreader to within 3–4 mm from the working length is acceptable [1, 44]. Meanwhile, it has been shown that there is a direct correlation between the spreader penetration depth and the quality of the root canal obturation when conventional sealers were used for root canal filling [56, 57]. Appropriate accessory points are also selected to match the size of the spreader.

(a–d) The clinical steps of lateral compaction technique using master and accessory gutta-percha points and finger spreader
It has been recommended to use NiTi spreaders instead of stainless steel, especially in the curved root canal, as they provide increased flexibility, reduce stress, and can be inserted deeper into the root canals [58, 59]. It should be mentioned that spreader penetration depth will be significantly lower if the larger taper master gutta-percha point will be used for obturation [24, 60]. After placement, the spreader is removed by constant counterclockwise rotation as it is withdrawn. The accessory point is inserted in the space made by the spreader (Fig. 8c), and the procedure is repeated until the spreader is no longer going than 3–4 mm below the root canal orifice (Fig. 8d). It should be mentioned that due to the increased flowability of sealer, the space for the accessory point, created by spreader, can spontaneously be filled by the flowable sealer. It can complicate the filling procedure because the clinician is not able to see where the auxiliary point should be inserted. To avoid this clinical inconvenience, the appropriate amount of the sealer should be used. Additionally, the excess of the material can be removed by a wet cotton pellet. The excess gutta-percha is removed using the hot instrument, and the gentle vertical condensation with the plugger is recommended to complete obturation procedure. If wide root canals are being obturated, the big amount of the accessory points can fill the access cavity, decreasing visibility and control. To facilitate obturation procedure and control, the excess gutta-percha can be removed and the lateral compaction can be continued to ensure optimal condensation and homogeneity of the filling [61]. When obturation is completed, the quality of obturation should be confirmed by radiograph, and the temporary or permanent restoration should be placed.
5.2 Warm Vertical Condensation and Its Modifications
It has been reported that the hydraulic calcium silicate–based sealers are not suitable for use with warm gutta-percha obturation techniques, as the heat negatively affects the physical properties of the sealers [31, 32, 62]. However, as it was be mentioned previously in this chapter, just water-based hydraulic calcium silicate–based sealers, such as BioRoot™ RCS, are sensitive to the heat and should be used with cold obturation techniques [52, 63]. Meanwhile, all premixed materials can be used with all cold and thermoplastic obturation techniques at the higher temperatures can be used with no restrictions [14, 29, 31]. Therefore, the clinicians have plenty of choices how to apply and use the new hydraulic calcium silicate–based sealers with thermoplastic obturation techniques.
After the canal was dried with the paper point, the master gutta-percha point is selected (Fig. 9). Preferably, it should be 0.5–2 mm shorter of the correct working length with resistance to displacement or “tug back.” If the point is too loose, it can be adjusted by removing the tip in 0.5 mm increments with sterile scalpel or scissors. Afterwards, the largest heat plugger that will go to within 5 mm of the working length without binding but no closer than 3 mm should be selected and confirmed working length should be set using a rubber stopper. The sealer should be delivered into the canal using a preferable technique described above. The apical third of the master gutta-percha point is covered with a sealer, gently placed into the canal, and the coronal portion is removed with a hot instrument, while the remaining gutta-percha will be softened. The cold plugger is used to condense the softened gutta-percha and force the plasticized material apically. The procedure is repeated until the apical third of the canal has been obturated. The middle and coronal root canal thirds are backfilled, using small pieces of gutta-percha, preferably previously introduced BC gutta-percha pellets, applying heat, and condensing the softened gutta-percha with a plugger. When root canal obturation is completed, the periapical X-ray should be taken, to confirm the quality of obturation.

The “classic” warm vertical compaction technique. A master gutta-percha point is selected and fit 0.5–2.0 mm short of the working length (a). Heat is applied, and coronal part of master gutta-percha point is removed using plugger (b). The cold plugger is used to compact the softened gutta-percha apically (c). Down-pack or apical compaction is completed (d). A gutta-percha pellet is placed in the canal, and heat is applied (e). The heated pellet is condensed apically with a cold plugger (f). The procedure is repeated in the middle and coronal thirds of the canal by delivering and heating pellets of gutta-percha (g). A cold plugger is used to compact the softened gutta-percha (h). Completely obturated root canal (i)
The recent and the most popular modification of the “classic” warm vertical compaction is the continuous wave compaction technique. The technique uses special dual wired or cordless devices combining both down-pack handpiece heat carrier and backfill handpieces using special gutta-percha cartridges (Fig. 10a). The GP cone is measured with the appropriate tip size and taper and 0.5–2 mm shorter of the WL, while the heat plugger is pre-fitted to fit approximately 5 mm from the WL (Fig. 11). The premixed or freshly prepared hydraulic calcium silicate–based sealer is delivered into the root canal, and master gutta-percha point is inserted. Activated heat plugger is used to remove coronal excess of gutta-percha. Material compaction in the canal orifice and coronal part is initiated with a cold plugger. Subsequently, the firm pressure to the plugger is applied, the heat is activated, and plugger is rapidly moved apically into the root canal to within 5 mm of the working length. Then the heat is deactivated and continued apical pressure for approximately 5–10 s is applied. When the gutta-percha has cooled, the heat is activated for a 1 s to separate filling material and plugger and it is withdrawn. Selected small hand plugger is used for gentle compaction the remaining gutta-percha apically. At this point, apical obturation should be confirmed radiographically. The backfill procedure is performed by using a backfill handpiece and thermoplastic injection technique. The heated applicator needle is inserted into the canal, allowing the tip to heat the apical plug of gutta-percha for approximately 2–5 s. The handpiece is activated, and softened gutta-percha is extruded into the root canal.

Devices for continuous wave compaction technique: wired Elements™ Obturation Unit for down-pack and backfill (a) and cordless backfill gun-handpiece for use with gutta-percha pellets (b)

The main clinical steps of the continuous wave compaction technique using Elements™ Obturation Unit: pre-fitting of the Buchanan Plugger (a); activation of the plugger and vertical compaction (b); backfill using motorized extruder (c)
In small and narrow canals, the gutta-percha can be delivered and obturation completed in one step. However, in larger canals, it is recommended to deliver the warm gutta-percha in 3–5 mm increments coronally until the canal orifice will be reached. The larger stainless steel hand plugger is used to compact extruded gutta-percha reducing the shrinkage that may occur during cooling. Depending on the size of the root canal, it can be obturated in 1–3 steps until the canal is completely filled. Moreover, for the backfill procedure, the special backfill guns, suitable with gutta-percha pellets instead special cartridges, can be used (Fig. 10b). Softened gutta-percha is injecting in the small increments and condensing the material as described below. The use of the BC gutta-percha pellets in conjunction with bioceramic sealers can be advantageous in comparison to regular gutta-percha backfills, as it should ensure more uniform root canal filling [64]. However, there is no solid scientific evidence to confirm this hypothesis [4, 65]. The quality of obturation should be verified by X-ray, endodontic access cleaned and isolated with a temporary or permanent filling material.
It should be mentioned that due to the unique properties of the highly flowable and dimensionally stable hydraulic calcium silicate–based sealers, the down-pack procedure became easier and should not be performed so precisely in comparison to cases, when conventional sealers are used. Conventional sealers shrink over the time, so precise condensation of the gutta-percha seeking to pull the sealer of root canal walls and replace it with heat softened GP was necessary, thereby thinning the sealer layer as much as possible. However, the hydraulic calcium silicate–based sealers are dimensionally stable and flows into all root canal irregularities, isthmuses, and dentinal tubules [11, 29, 49]. Therefore, the thickness of the sealer layer is not important to ensure the high-quality obturation, even if the minimal condensation to softened gutta-percha is applied [31, 64,65,66].
5.3 Single-Cone Obturation
The unique properties of the flowable hydraulic calcium silicate–based sealers have led to the introduction in clinical practice of simplified root canal filling technique known as a “single cone” obturation technique [12, 15]. The concept basically relies on the use the flowable hydraulic tricalcium silicate sealer–filler and single gutta-percha point, corresponding the size and the taper of the last instrument, used for the root canal preparation [4, 31]. The preliminary clinical results of using this simplified obturation technique in conjunction with hydraulic sealers have shown that it is equally effective as lateral compaction or thermoplastic obturation [12, 14, 17].
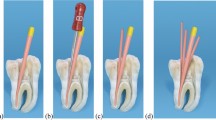
The use of cold hydraulic obturation technique with hydraulic calcium silicate–based sealers is not complicated and is clinically appealing [8, 15]. After the root canal cleaning and shaping is completed, the root canal is dried, and the master gutta-percha point is selected as described previously (Fig. 12a). It is very important to remember that root canals should not be overdried as the residual moisture is needed for setting of the hydraulic calcium silicate–based sealers [24, 25]. It is recommended to use a gutta-percha point of the same size and taper as the last endodontic instrument, used for root canal enlargement [4, 6, 67]. The sealers/fillers should be prepared according to the manufacturer’s instructions and delivered to the root canal using all the conventional methods. Due to the high flowability of the hydraulic calcium silicate materials, the injectable delivery method can be superior because a larger amount of sealer is delivered and it is better distributed in the root canal [4, 6, 68] (Fig. 12b). If premixed sealers in syringes are used, no mixing preparation is required. When the sealer has been placed, the tip of the pre-fitted gutta-percha point is covered with the sealer (Fig. 12c), and the point is inserted into the root canal by the full WL (Fig. 12d, e).

(a–e) Main clinical steps of the single-cone obturation technique, using flowable hydraulic calcium silicate–based sealer BioRoot™ RCS and a single gutta-percha point
The gutta-percha must be inserted very slowly as its rapid movement increases the possibility of the sealer being extruded into periapical tissues and the formation of the voids in the sealer/filler mass [4, 6, 69]. The master gutta-percha point generates hydraulic pressure in the root canal, resulting in a better distribution of the sealer in the root canal space, irregularities, and isthmuses as well as facilitating material penetration into dentinal tubules [13, 31, 69]. In addition, the gutta-percha point enables to retreat the root canals filled with this technique, if the failure occurs. The master gutta-percha point should be removed by a hot instrument at the level of the root canal orifices and endo access should be cleaned with a wet cotton pellet. If the root canal is very wide, accessory gutta-percha points can be added passively along with master gutta-percha point without any condensation. However, it is not necessary as the hydraulic tricalcium silicate–based sealers are used as biological fillers which do not shrink, and it is not necessary to minimize the amount of the sealer inside the root canal [8, 17].
The single-cone obturation technique is very simple, does not require a long learning curve, and is easily managed by clinicians. The preliminary microcomputer tomographic evaluation revealed that the quality of root canal obturation using a single gutta-percha point and hydraulic tricalcium silicate–based sealer BioRoot™ RCS was the same regardless of who performed the root canal filling: general practitioner, endodontist, postgraduate endodontology student, or fourth-year dental student (Fig. 13). This clearly demonstrates that the quality of the root canal obturation using this simplified technique is not depending on the clinical experience and manual skills of the operator.

The cross-sectional images of micro-CT scans of the root canals, obturated with BioRoot™ RCS and single GP point by general practitioner (a), endodontist (b), postgraduate endodontology student (c), and fourth-year dental student (d) (unpublished data)
The cold lateral compaction or warm vertical compaction techniques are much more complicated to apply clinically, are quite expensive, and time consuming [15, 51]. It has been shown that apical third of the curved canals often is filled just with a master gutta-percha point because it is complicated and unrealistic to insert spreader and accessory gutta-percha points at the desirable length in the curved roots [70, 71]. Although there is a lack of long-term clinical trials, confirming the clinical performance of cold hydraulic obturation technique, it has already been reported that the clinical success rate of the cold hydraulic obturation method using a single gutta-percha point and a flowable bioceramic sealer based on tricalcium silicate reaches 90.9% [15, 72]. Recently, it has been shown that retreatability of the cases, when hydraulic calcium silicate sealers in conjunction with the single gutta-percha cone technique were used is not more complicated or challenging in comparison to other obturation materials and techniques [30, 73, 74]. The simplified root canal obturation technique, when used with the stable, biocompatible, and bioactive sealers-fillers, seems promising and clinically appealing technique even in a difficult cases of endodontic retreatment (Fig. 14).


Apical periodontitis of 46 (a–c) and 36 (d–f) teeth with extensive periapical lesions (a, d). Endodontic retreatment performed using conventional cleaning and shaping protocol and 1-week calcium hydroxide therapy. Root canals were obturated with BioRoot™ RCS sealer (b) and TotalFill BC sealer (e) in conjunction with a big taper single gutta-percha point. Noticeable healing of the periapical tissues 8 months after endodontic retreatment (c, f)
6 Conclusions
Majority of modern commercially available flowable hydraulic calcium silicate materials have particularly the same chemical composition and possess mainly the same physical, biological, and handling characteristic. Nowadays, hydraulic calcium silicate sealers are widely researched and the clinical effectiveness of the single-cone obturation technique when these materials are used is confirmed. However, the decision for the clinician to change materials and techniques is very complicated and not an easy task in everyday clinical practice. The solid scientific background indicates that the biocompatible, bioactive, and antibacterial hydraulic calcium silicate materials that slightly expand upon setting and remain dimensionally stable in conjunction with the simplified single-cone obturation can provide much better results than lateral condensation and can replace it as the most efficient endodontic sealing method.
References
Whitworth J. Methods of filling root canals: principles and practices. Endod Top. 2005;12:2–24.
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - Part 2. Influence of clinical factors. Int Endod J. 2008;41:6–31.
Gok T, Capar ID, Akcay I, Keles A. Evaluation of different techniques for filling simulated c-shaped canals of 3-dimensional printed resin teeth. J Endod. 2017;43:1559–64.
Camilleri J. Will bioceramics be the future root canal filling materials? Curr Oral Heal Reports. 2017;4:228–38.
Al-Haddad A, Aziz ZACA. Bioceramic-based root canal sealers: a review. Int J Biomater. 2016;2016:9753210. https://doi.org/10.1155/2016/9753210.
Debelian G, Trope M. The use of premixed bioceramic materials in endodontics. G Ital Endod. 2016;30:70–80.
Jeong JW, DeGraft-Johnson A, Dorn SO, Di Fiore PM. Dentinal tubule penetration of a calcium silicate–based root canal sealer with different obturation methods. J Endod. 2017;43:633–7.
Guivarc’h M, Jeanneau C, Giraud T, Pommel L, About I, Azim AA, et al. An international survey on the use of calcium silicate-based sealers in non-surgical endodontic treatment. Clin Oral Investig. 2020;24:417–24.
Zhou HM, Du TF, Shen Y, Wang ZJ, Zheng YF, Haapasalo M. In vitro cytotoxicity of calcium silicate-containing endodontic sealers. J Endod. 2015;41:56–61.
Candeiro GTM, Moura-Netto C, D’Almeida-Couto RS, Azambuja-Júnior N, Marques MM, Cai S, et al. Cytotoxicity, genotoxicity and antibacterial effectiveness of a bioceramic endodontic sealer. Int Endod J. 2016;49:858–64.
Candeiro GTDM, Correia FC, Duarte MAH, Ribeiro-Siqueira DC, Gavini G. Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J Endod. 2012;38:842–5.
Silva Almeida LH, Moraes RR, Morgental RD, Pappen FG. Are premixed calcium silicate–based endodontic sealers comparable to conventional materials? A systematic review of in vitro studies. J Endod. 2017;43:527–35.
Khalil I, Naaman A, Camilleri J. Properties of tricalcium silicate sealers. J Endod. 2016;42:1529–35.
Zavattini A, Knight A, Foschi F, Mannocci F. Outcome of root canal treatments using a new calcium silicate root canal sealer: a non-randomized clinical trial. J Clin Med. 2020;9:782. https://doi.org/10.3390/jcm9030782.
Chybowski EA, Glickman GN, Patel Y, Fleury A, Solomon E, He J. Clinical outcome of non-surgical root canal treatment using a single-cone technique with endosequence bioceramic sealer: a retrospective analysis. J Endod. 2018;44:941–5.
Fonseca B, Coelho MS, Bueno CEDS, Fontana CE, Martin AS, Rocha DGP. Assessment of extrusion and postoperative pain of a bioceramic and resin-based root canal sealer. Eur J Dent. 2019;13:343–8.
Roizenblit RN, Soares FO, Lopes RT, dos Santos BC, Gusman H. Root canal filling quality of mandibular molars with EndoSequence BC and AH Plus sealers: a micro-CT study. Aust Endod J. 2020;46:82. https://doi.org/10.1111/aej.12373.
Jafari F, Jafari S. Composition and physicochemical properties of calcium silicate-based sealers: a review article. J Clin Exp Dent. 2017;9:1249–55.
Trope M, Bunes A, Debelian G. Root filling materials and techniques: bioceramics a new hope? Endod Top. 2015;32:86–96.
López-García S, Pecci-Lloret MR, Guerrero-Gironés J, Pecci-Lloret MP, Lozano A, Llena C, et al. Comparative cytocompatibility and mineralization potential of Bio-C Sealer and TotalFill BC Sealer. Materials (Basel). 2019;12:3087. https://doi.org/10.3390/ma12193087.
Zordan-Bronzel CL, Esteves Torres FF, Tanomaru-Filho M, Chávez-Andrade GM, Bosso-Martelo R, Guerreiro-Tanomaru JM. Evaluation of physicochemical properties of a new calcium silicate–based sealer, Bio-C Sealer. J Endod. 2019;45:1248–52.
Yang DK, Kim S, Park JW, Kim E, Shin SJ. Different setting conditions affect surface characteristics and microhardness of calcium silicate-based sealers. Scanning. 2018;2018:7136345. https://doi.org/10.1155/2018/7136345.
Boyadzhieva E, Dimitrova S, Filipov I, Zagorchev P. Setting time and solubility of premixed bioceramic root canal sealer when applicated with warm gutta percha obturation techniques. IOSR J Dent Med Sci. 2017;16:125–9.
Loushine BA, Bryan TE, Looney SW, Gillen BM, Loushine RJ, Weller RN, et al. Setting properties and cytotoxicity evaluation of a premixed bioceramic root canal sealer. J Endod. 2011;37:673–7.
Xuereb M, Vella P, Damidot D, Sammut CV, Camilleri J. In situ assessment of the setting of tricalcium silicate-based sealers using a dentin pressure model. J Endod. 2015;41:111–24.
Ghoneim AG, Lutfy RA, Sabet NE, Fayyad DM. Resistance to fracture of roots obturated with novel canal-filling systems. J Endod. 2011;37:1590–2.
Donnermeyer D, Bürklein S, Dammaschke T, Schäfer E. Endodontic sealers based on calcium silicates: a systematic review. Odontology. 2019;107:421–36.
Lee JK, Kim S, Lee S, Kim H-C, Kim E. In vitro comparison of biocompatibility of calcium silicate-based root canal sealers. Materials (Basel). 2019;12:2411. https://doi.org/10.3390/ma12152411.
Chen B, Haapasalo M, Mobuchon C, Li X, Ma J, Shen Y. Cytotoxicity and the effect of temperature on physical properties and chemical composition of a new calcium silicate–based root canal sealer. J Endod. 2020;46:531–8.
Oltra E, Cox TC, LaCourse MR, Johnson JD, Paranjpe A. Retreatability of two endodontic sealers, EndoSequence BC Sealer and AH Plus: a micro-computed tomographic comparison. Restor Dent Endod. 2017;42:19.
Heran J, Khalid S, Albaaj F, Tomson PL, Camilleri J. The single cone obturation technique with a modified warm filler. J Dent. 2019;89:103181.
Camilleri J. Sealers and warm gutta-percha obturation techniques. J Endod. 2015;41:72–8.
Duarte MAH, Marciano MA, Vivan RR, Tanomaru Filho M, Tanomaru JMG, Camilleri J. Tricalcium silicate-based cements: properties and modifications. Braz Oral Res. 2018;32:111–8.
http://media.brasselerusa.com/userfiles/IFU%2CManuals%2CBrochures/B_5019_ENG_HiFlow%20NPR.pdf.
Dammaschke T. Sealer auf Kalzium-silikatbasis. Der Freie Zahnarzt. 2020;64:64–71.
http://www.angelusdental.com/img/arquivos/3823_10503823_0321052018_bio_c_sealer_bula_fechado.pdf.
López-García S, Lozano A, García-Bernal D, Forner L, Llena C, Guerrero-Gironés J, et al. Biological effects of new hydraulic materials on human periodontal ligament stem cells. J Clin Med. 2019;8:1216. https://doi.org/10.3390/jcm8081216.
Reszka P, Nowicka A, Lipski M, Dura W, Droździk A, Woźniak K. A comparative chemical study of calcium silicate-containing and epoxy resin-based root canal sealers. Biomed Res Int. 2016;2016:9808432. https://doi.org/10.1155/2016/9808432.
Olcay K, Taşli PN, Güven EP, Ülker GMY, Öğüt EE, Çiftçioğlu E, et al. Effect of a novel bioceramic root canal sealer on the angiogenesis-enhancing potential of assorted human odontogenic stem cells compared with principal tricalcium silicate-based cements. J Appl Oral Sci. 2020;28:e20190215. https://doi.org/10.1590/1678-7757-2019-0215.
Komabayashi T, Colmenar D, Cvach N, Bhat A, Primus C, Imai Y. Comprehensive review of current endodontic sealers. Dent Mater J. 2020; https://doi.org/10.4012/dmj.2019-288.
López-García S, Myong-Hyun B, Lozano A, García-Bernal D, Forner L, Llena C, et al. Cytocompatibility, bioactivity potential, and ion release of three premixed calcium silicate-based sealers. Clin Oral Investig. 2020;24:1749. https://doi.org/10.1007/s00784-019-03036-2.
Colombo M, Poggio C, Dagna A, Meravini M-V, Riva P, Trovati F, et al. Biological and physico-chemical properties of new root canal sealers. J Clin Exp Dent. 2018;10:120–6.
Camps J, Jeanneau C, El Ayachi I, Laurent P, About I. Bioactivity of a calcium silicate-based endodontic cement (BioRoot RCS): interactions with human periodontal ligament cells in vitro. J Endod. 2015;41:1469–73.
Dimitrova-Nakov S, Uzunoglu E, Ardila-Osorio H, Baudry A, Richard G, Kellermann O, et al. In vitro bioactivity of Bioroot™ RCS, via A4 mouse pulpal stem cells. Dent Mater. 2015;31:1290–7.
Prüllage RK, Urban K, Schäfer E, Dammaschke T. Material properties of a tricalcium silicate–containing, a mineral trioxide aggregate–containing, and an epoxy resin–based root canal sealer. J Endod. 2016;42:1784–8.
Arias-Moliz MT, Camilleri J. The effect of the final irrigant on the antimicrobial activity of root canal sealers. J Dent. 2016;52:30–6.
https://www.septodont.ie/sites/ie/files/2016-11/BioRoot-brochure-UK_0.pdf.
Prati C, Gandolfi MG. Calcium silicate bioactive cements: biological perspectives and clinical applications. Dent Mater. 2015;31:351–70.
Tomson RME, Polycarpou N, Tomson PL. Contemporary obturation of the root canal system. Br Dent J. 2014;216:315–22.
Cailleteau JG. Prevalence of teaching apical patency and various instrumentation and obturation techniques in United States dental schools. J Endod. 1997;23:394–6.
Siboni F, Taddei P, Zamparini F, Prati C, Gandolfi MG. Properties of BioRoot RCS, a tricalcium silicate endodontic sealer modified with povidone and polycarboxylate. Int Endod J. 2017;50(Suppl 2):120–36.
Dawood AE, Parashos P, Wong RHK, Reynolds EC, Manton DJ. Calcium silicate-based cements: composition, properties, and clinical applications. J Investig Clin Dent. 2017;8(2) https://doi.org/10.1111/jicd.12195.
Gordon MPJ, Love RM, Chandler NP. An evaluation of .06 tapered gutta-percha cones for filling of .06 taper prepared curved root canals. Int Endod J. 2005;38:87–96.
Romania C, Beltes P, Boutsioukis C, Dandakis C. Ex-vivo area-metric analysis of root canal obturation using gutta-percha cones of different taper. Int Endod J. 2009;42:491–8.
Shahi S, Zand V, Oskoee SS, Abdolrahimi M, Rahnema AH. An in vitro study of the effect of spreader penetration depth on apical microleakage. J Oral Sci. 2007;49:283–6.
Allison DA, Michelich RJ, Walton RE. The influence of master cone adaptation on the quality of the apical seal. J Endod. 1981;7:61–5.
Schmidt KJ, Walker TL, Johnson JD, Nicoll BK. Comparison of nickel-titanium and stainless-steel spreader penetration and accessory cone fit in curved canals. J Endod. 2000;26:42–4.
Berry KA, Loushine RJ, Primack PD, Runyan DA. Nickel-titanium versus stainless-steel finger spreaders in curved canals. J Endod. 1998;24:752–4.
Tanomaru-Filho M, Trindade DVB, De Almeida LT, Espir CG, Bonetti-Filho I, Guerreiro-Tanomaru JM. Effect of ProTaper and Reciproc preparation and gutta-percha cone on cold lateral compaction. J Conserv Dent. 2016;19:410–3.
Mazotti D, Sivieri-Araújo G, Berbert FLCV, Bonetti-Filho I. In vitro evaluation of the obturation ability, adaptation and compaction of gutta-percha in the root canal system employing different filling techniques. Acta Odontol Latinoam. 2008;21:3–9.
Viapiana R, Guerreiro-Tanomaru JM, Tanomaru-Filho M, Camilleri J. Investigation of the effect of sealer use on the heat generated at the external root surface during root canal obturation using warm vertical compaction technique with system b heat source. J Endod. 2014;40:555–61.
Viapiana R, Moinzadeh AT, Camilleri L, Wesselink PR, Tanomaru Filho M, Camilleri J. Porosity and sealing ability of root fillings with gutta-percha and BioRoot RCS or AH Plus sealers. Evaluation by three ex vivo methods. Int Endod J. 2016;49:774–82.
Nasseh AA, Brave D. Using a bioceramic sealer in conjunction with vertical condensation. Endod Prac. 2015;8:16–20.
Buchanan S. Warm gutta-percha obturation with BC HiFlow™ Sealer. Endod Prac. 2018;11:32–5.
Koch K, Brave D, Nasseh AA. A review of bioceramic technology in endodontics. Roots. 2013;1:6–13.
Germain S, Meetu K, Issam K, Alfred N, Carla Z. Impact of the root canal taper on the apical adaptability of sealers used in a single-cone technique: a micro-computed tomography study. J Contemp Dent Pract. 2018;19:808–15.
Celikten B, Uzuntas CF, Orhan AI, Orhan K, Tufenkci P, Kursun S, et al. Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: an in vitro Micro-CT study. Scanning. 2016;38:133–40.
Drukteinis S, Peciuliene V, Shemesh H, Tusas P, Bendinskaite R. Porosity distribution in apically perforated curved root canals filled with two different calcium silicate based materials and techniques: a micro-computed tomography study. Materials (Basel). 2019;12:1729. https://doi.org/10.3390/ma12111729.
Moinzadeh AT, Zerbst W, Boutsioukis C, Shemesh H, Zaslansky P. Porosity distribution in root canals filled with gutta percha and calcium silicate cement. Dent Mater. 2015;31:1100–8.
Pérez Heredia M, Clavero González J, Ferrer Luque CM, González Rodríguez MP. Apical seal comparison of low-temperature thermoplasticized gutta-percha technique and lateral condensation with two different master cones. Med Oral Patol Oral Cir Bucal. 2007;12:175–9.
de Figueiredo FED, Lima LF, Oliveira LS, Ribeiro MA, Correa MB, Brito-Junior M, et al. Effectiveness of a reciprocating single file, single cone endodontic treatment approach: a randomized controlled pragmatic clinical trial. Clin Oral Investig. 2019; https://doi.org/10.1007/s00784-019-03077-7.
Kakoura F, Pantelidou O. Retreatability of root canals filled with Gutta percha and a novel bioceramic sealer: a scanning electron microscopy study. J Conserv Dent. 2018;21:632–6.
Ersev H, Yilmaz B, Dinçol ME, Dağlaroğlu R. The efficacy of ProTaper Universal rotary retreatment instrumentation to remove single gutta-percha cones cemented with several endodontic sealers. Int Endod J. 2012;45:756–62.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Drukteinis, S. (2021). Bioceramic Materials for Root Canal Obturation. In: Drukteinis, S., Camilleri, J. (eds) Bioceramic Materials in Clinical Endodontics. Springer, Cham. https://doi.org/10.1007/978-3-030-58170-1_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-58170-1_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-58169-5
Online ISBN: 978-3-030-58170-1
eBook Packages: MedicineMedicine (R0)