
Abstract
We investigated plausible changes in spectral and higher order statistical properties of tracheal respiratory sounds from wakefulness to sleep in relation to obstructive sleep apnea (OSA). Data consisted of expiratory sounds of 30 participants suspected of OSA during wakefulness and sleep, both recorded in supine position. Participants were divided into two groups of mild and severe OSA (15 in each group) based on their apnea/hypopnea index (AHI) per hour. Three different frequency-based features of their power spectra in addition to Kurtosis and Katz fractal dimension (KFD) were estimated from each normalized expiratory sound; they were compared within and between the groups. During wakefulness, the sounds average power at low-frequency components in severe group was lesser than that of the mild group. However, during sleep, the average power of high-frequency components in severe subjects was more than that of the mild group. The kurtosis value of both mild and severe OSA groups increased significantly from wakefulness to sleep using both mouth and nasal breathing sounds during wakefulness. The KFD increased significantly from wakefulness to sleep for both mild and severe OSA group using only nasal breathing sounds during wakefulness. These changes are indicative that the upper airway of severe OSA show more compliance and thickness compare to that of the mild OSA during both wakefulness and sleep and represent an increased stiffness during sleep. This implies a regional narrowing which cause both more compliance and stiffness simultaneously in different regions of the upper airway.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Obstructive sleep apnea (OSA) syndrome is due to the partial or complete collapse of the upper airway (UA) [1], resulting from relaxation of muscles controlling the soft palate or tongue. [2]. An individual with OSA, despite persistent efforts to breathe, may experience periods of cessation of breathing (apnea) and/or more than 50% reduction in airflow (hypopnea). Such event is called apnea or hypopnea if it lasts at least 10 s and is associated with a minimum of 4% drop in oxygen saturation level in blood [1]. The severity of OSA is measured by apnea/hypopnea index (AHI) per hour of sleep.
OSA is a prevalent health problem that affects both children and adults. It has been reported that about 10% of the North American population suffer from OSA [3], while it is believed there are many undiagnosed cases [4]. OSA is associated with an increased risk of cardiovascular disease, daytime sleepiness, reduced concentration and increased risk of car accidents [1]. The current gold standard for diagnosis of OSA is full-night polysomnography (PSG). Many physiological signals such as heart and muscle signals, respiratory effort, respiratory flow, and brain waves (EEG) are recorded during a PSG assessment to provide a full physiological picture of the patients’ sleep apnea and sleep quality. However, PSG assessment is time-consuming, cumbersome and expensive with long waiting list around the world. Therefore, designing simpler assessment methods such as portable home monitoring devices offer an alternative way to detect sleep apnea while overcoming the drawbacks of PSG. In this study, we aimed to explore the use of breathing sounds in understanding UA differences in OSA individuals with different levels of OSA severity during both wakefulness and sleep. The outcomes of our study may lead to a better physiological understanding of the mechanism of the UA collapse during sleep using only breathing sound analysis.
Various features of UA anatomy and neuromuscular control contribute to OSA development [5]. Therefore, the cause of OSA may vary considerably between individuals. Some of the previous studies using MRI/CT imaging during wakefulness have shown that OSA individuals have a narrower and thicker UA compared to non-OSA individuals [6]. Also, the lateral narrowing of the UA in OSA individuals was found to be of an elliptical configuration in the anterior-posterior dimension in contrast to a more laterally open in non-OSA individuals [7, 8]. Nevertheless, it has been reported that the patency of the UA of OSA individuals during wakefulness is well maintained due to an increase in their dilator muscles activities [9, 10]. On the other hand, the UA of OSA participants during sleep has been shown to be more collapsible [11], most probably due to the changes in neuromuscular control and airway physiology at the onset of sleep [12].
Our team and a few others around the world have been using tracheal respiratory sounds to monitor and assess OSA. It is known that structural and physiological properties of the UA (such as diameter, wall thickness, and length) will affect the breathing sound generation mechanism [13]. Therefore, we hypothesize that respiratory sounds are able to convey valuable information in relation to monitoring and detecting OSA. Some previous studies focused on analyzing respiratory sound during wakefulness for OSA assessment and classification [14, 15]. In this study, however, we investigated breathing sound features during both wakefulness and sleep to determine which sound features change the most from wakefulness to sleep differently among people with different levels of OSA severity. We focused on investigating the spectral and higher order statistical characteristics of respiratory sounds during both wakefulness and sleep in relation to OSA.
2 Method
2.1 Data
We used tracheal respiratory sounds of 30 individuals with OSA. Tracheal breathing sounds during both wakefulness and sleep were recorded in the supine position with head resting on a pillow. During wakefulness, participants were instructed to breathe at their normal rate in two maneuvers: first through the nose with mouth closed and second through the mouth with a nose clip in place; five full breathing cycles in each maneuver were recorded. After wakefulness recording, participants were prepared for PSG assessment. Breathing sounds recording during sleep were conducted simultaneously with full-night PSG assessment at Misericordia Health Center (Winnipeg, Canada). The severity of OSA was determined using the PSG report and an AHI threshold of 15. Data included 15 participants with mild-OSA (11 male, AHI < 15) and 15 severe-OSA (13 male, AHI > 15). Demographic information of the participants is shown in Table 1. This study was approved by the Biomedical Research Ethics Board of the University Of Manitoba and all the participants signed an informed consent form prior to data collection.
The breathing sounds during both wakefulness and sleep were collected with a small microphone (Sony ECM-77B). The Microphone was inserted into a small chamber which allowed 2 mm cone-shape space with skin to ensure that it never connects the skin of participants during the recording, and mounted over the suprasternal notch of their trachea. A soft neckband was wrapped around the patient’s neck to sustain the microphone and chamber in place, and to ensure that the microphone would not be misplaced during the night. The recorded breathing sounds were amplified by a Biopac (DA100C) amplifier with the band-pass filter in the range of 0.5–5000 Hz and digitized at 10,240 Hz sampling rate.
2.2 Signal Analysis
All the recorded tracheal breathing sounds data were examined manually by listening to and observing the sounds in the time-and-frequency domain for plausible occasional swallow that may interfere with altering breath phases and to exclude noisy signals or those associated with snoring sounds. As the respiratory flow was not recorded in this study, to insure the accuracy of the phase labels during wakefulness, each recording was always started at the inspiration. The inspiratory and expiratory phases during wakefulness and sleep were identified semi-manually using the technique elaborated in [16]. Briefly, the log of the variance of each phase is calculated and the onset of each phase is identified by an automatic algorithm. Then, based on different features from duration, shape and volume of the sound envelope each phase is labeled as inspiration or expiration. During sleep, snoring usually occurs within the inspiration phase. Therefore, to avoid plausible snoring sounds, we selected four noise-free expiratory sounds in supine position (determined using the PSG assessment). During wakefulness, we also analyzed four noise-free expiratory sounds for comparison to those during sleep. We extracted sleep data from only stage 2 of sleep because that was the most common stage in our dataset. To remove the effect of low and high-frequency noises, including heart and muscle sounds and ambient noise, each individual expiratory sound segment was passed through a 5th-order Butterworth band-pass filter in the range of [75–2500 Hz].
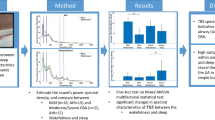
Next, the same procedure as in [15], was applied to each selected expiratory sound: each expiratory phase was first normalized by its variance envelope (moving average filter of the signal with 64 sample sequence) to remove its extra fluctuations. Subsequently, they were normalized by their energy to compensate for plausible different flow rates in each breathing cycle. To capture the stationary part of the expiratory breathing sounds, we calculated the logarithm of the sound’s variance using the method in [17], and the sounds segments corresponding to its middle part (50% duration around the maximum) was considered for further analysis. Next, we estimated the power spectrum density (PSD) of the stationary portion of each expiratory sound signal using Welch’s method in windows of 205-point (~ 20 ms) with 50% overlap between successive windows, and averaged over the four expiratory phases of each participant. Next, three frequency-based features were calculated from the average PSD: 30%-freq, 50%-freq and 70%-freq, the frequency at which the PSD reaches 30, 50 and 70% of the total power, respectively. In addition, the kurtosis and Katz fractal dimension (KFD) [18] were also calculated in every 20 ms window with 50% overlap with the adjacent windows and then averaged within the stationary part of each expiratory phase. They were then averaged over the four expiratory phases of each participant.
The extracted features were then compared within the mild and severe groups and between the wakefulness and sleep. For comparison, we used paired and unpaired t-tests (for within and between group comparisons); a p value of 0.05 was considered as significant.
3 Results
Investigating different frequency-based features showed that the PSD of mild OSA reached their 30%-freq in lower frequencies compared to that of severe OSA using both mouth and nasal breathing sounds of wakefulness; though, it was only significant (p < 0.008) during mouth breathing maneuver (Fig. 1). The same pattern was also observed during sleep (p < 0.05) (Fig. 1). These results imply that the PSD of the mild group at the lower frequencies are more powerful than that of the severe participants during both wakefulness and sleep.

Mean and standard error of 30%-freq feature extracted from average expiratory breathing sounds PSD of mild and severe OSA groups during mouth breathing in wakefulness and stage 2 of sleep
As shown in Fig. 2, the average power spectra of severe OSA reached both their 50 and 70% power in significantly higher frequencies than the mild OSA (p < 0.02, p < 0.05, respectively). This finding implies that, the average PSD of severe participants during sleep has more power in higher frequencies compare to the average PSD of mild participants. No significant difference between the 50%-freq and 70%-freq of mild and severe OSA groups was observed during either mouth or nasal breathing sounds of wakefulness (Fig. 2).

Mean and standard error of a 50%-freq and b 70%-freq feature. These features were extracted from the average expiratory breathing sounds PSD of mild and severe OSA groups during mouth breathing maneuver in wakefulness and stage 2 of sleep
Higher order statistical analysis showed that there was a significant change in the kurtosis of the breathing sounds from wakefulness to sleep in both mild (p < 0.007) and severe (p < 0.002) OSA groups, using the nasal breathing sounds during wakefulness (Fig. 3). The same pattern was also observed when we used expiratory mouth breathing sounds instead of nasal breathing sounds during wakefulness (p < 0.02 and p < 0.04 for mild and severe OSA groups, respectively).

t-test outcome of kurtosis change from wakefulness to sleep in mild and severe OSA groups using nasal breathing sounds during wakefulness
The KFD analysis revealed that for both mild and severe OSA groups, there was no significant change in this feature from wakefulness to sleep when using mouth-breathing sounds during wakefulness. However, the change of the KFD from wakefulness to sleep using nasal breathing sounds was significant for both mild and severe OSA group (p < 0.05 and p < 0.005, respectively) (Fig. 4). It should be noted that we could not be sure the breathing sounds during sleep were nasal or mouth breathing. In addition, there was no significant differences in KFD values of nasal and mouth breathing sounds during wakefulness. There was also a marginally significant (p < 0.06) difference between KFD of mild and severe OSA during sleep.

t-test outcome of Katz fractal dimension change from wakefulness to sleep in mild and severe OSA group using nasal breathing sounds during wakefulness
Table 2 summarizes the score of statistical tests for the three frequency-based features and the kurtosis and KFD characteristics of expiratory breathing sounds during both wakefulness and sleep.
4 Discussion
Tracheal breathing sounds analysis is a non-invasive method for studying the pathophysiology of the airway [19]. They have been shown to be affected by the structural and physiological changes of the UA [13]. In this study, we hypothesized that respiratory sounds’ spectral and higher order statistical characteristics are able to convey valuable information in relation to OSA severity and how they change from wakefulness to sleep.
The UA anatomical structure depends on body position. Thus, during both wakefulness and sleep, we analyzed breathing sounds recorded in supine position. The AHI in supine position is also usually higher than that in lateral body positions [20].
The 30%-freq feature revealed that during wakefulness and sleep the average power at low frequencies of breathings sounds of severe OSA is less than that of the mild OSA. This pattern was expected because different imaging studies [6, 11, 21] and our previous tracheal breathing sound studies [15, 22] have shown that the UAs of severe OSA compared to mild OSA are thicker and more compliant during both wakefulness and sleep. It is known that the low frequency sounds are absorbed more by more compliant tubes [23]. Thus, we expected to see a lower average power at low frequencies during wakefulness and sleep in severe OSA individuals (Fig. 1).
Based on the results of the 50%-freq and 70%-freq features, the average PSD during sleep at high frequencies was higher for severe OSA compared to that of mild OSA participants. As increased in high frequency power represents the increase in stiffness, we speculate that this finding may suggest an increased stiffness of the UAs of severe OSA subjects during sleep. That is congruent with imaging studies results [7, 8] and the tube law [24] that have suggests more regional compliance and stiffness of the UA due to the structural regional changes of the UA shape in severe OSA. In addition, in one study based on electromyography of anesthetized rats it was shown that simultaneous stimulation of protrudor and retractor muscles of tongue in the case of hypercapnia and hypoxia, as in severe OSA, leads to tongue retraction and results a narrower but stiffer pharyngeal airway [25]. Therefore, in agreement with aforementioned studies, the observed spectral pattern at low and high frequencies are representative of OSA pathophysiology during wakefulness and sleep.
The higher order statistical analysis (Kurtosis analysis) showed an increase in kurtosis from wakefulness to sleep in both mild and severe OSA groups, using both mouth and nasal breathing sounds during wakefulness. The kurtosis represents peakedness of the probability distribution of the time series signals. Thus, the higher kurtosis during sleep means the power distribution of tracheal expiratory sounds is more clustered around its mean and has relatively small standard deviation. We speculate this might be representative of the higher stiffness of the UA during sleep.
Fractal dimension analysis, including KFD that was used in this study, has often been used as a measure of the complexity of biological signals [26]. Our results showed a significant change in KFD from wakefulness to sleep in both groups of mild and severe OSA. We believe this is in support of the kurtosis results that showed more peakedness during sleep. Thus, this might also be due to higher stiffness of the UA during sleep in OSA individuals.
5 Conclusion
In this study, we investigated the spectral and higher order statistical characteristics of expiratory sounds during both wakefulness and sleep in mild and severe OSA groups. Our results, congruent with imaging studies of the UA in OSA population, are indicative that the UAs of severe OSA are mainly characterized by having more compliance (presented by lower average power at low frequencies) and also more stiffness (presented by higher average power at high frequencies). This implies there must be a regional narrowing to cause both more compliance and stiffness simultaneously in different regions of the UA. We also observed an increased stiffness during sleep particularly in severe OSA group. In addition, the results of higher order statistical analysis (kurtosis) and complexity measure are indicative of more stiffness as one sleeps; this was observed in both mild and severe OSA groups. Overall, the results of this study, although with a limited sample size, are encouraging for the use of tracheal breathing sounds for examining UA structural changes due to OSA during both wakefulness and sleep.
References
Malhotra, A., & White, D. P. (2002). Obstructive sleep apnoea. Lancet, 360, 237–245. https://doi.org/10.1016/S0140-6736(02)09464-3.
Remmers, J. E., deGroot, W. J., Sauerland, E. K., & Anch, A. M. (1978). Pathogenesis of upper airway occlusion during sleep. Journal of Applied Physiology, 44, 931–938.
Young, T., Finn, L., Peppard, P. E., et al. (2008). Sleep disordered breathing and mortality: Eighteen-year follow-up of the Wisconsin sleep cohort. Sleep, 31, 1071–1078. https://doi.org/10.1016/S8756-3452(08)79181-3.
Punjabi, N. M. (2008). The epidemiology of adult obstructive sleep apnea. Proceedings of the American Thoracic Society, 5, 136–143. https://doi.org/10.1513/pats.200709-155MG.
Deacon, N., & Malhotra, A. (2016). Potential protective mechanism of arousal in obstructive sleep apnea. Journal of Thoracic Disease, 8, S545–S546. https://doi.org/10.21037/jtd.2016.07.43.
Finkelstein, Y., Wolf, L., Nachmani, A., et al. (2014). Velopharyngeal anatomy in patients with obstructive sleep apnea versus normal subjects. Journal of Oral and Maxillofacial Surgery, 72, 1350–1372. https://doi.org/10.1016/j.joms.2013.12.006.
Liu, K.-H., Chu, W. C. W., To, K.-W., et al. (2007). Sonographic measurement of lateral parapharyngeal wall thickness in patients with obstructive sleep apnea. Sleep, 30, 1503–1508.
Barkdull, G. C., Kohl, C. A., Patel, M., & Davidson, T. M. (2008). Computed tomography imaging of patients with obstructive sleep apnea. Laryngoscope, 118, 1486–1492. https://doi.org/10.1097/MLG.0b013e3181782706.
Dempsey, J. A., Veasey, S. C., Morgan, B. J., & O’Donnell, C. P. (2010). Pathophysiology of sleep apnea. Physiological Reviews, 90, 47–112. https://doi.org/10.1152/physrev.00043.
Younes, M. (2008). Role of respiratory control mechanisms in the pathogenesis of obstructive sleep disorders. Journal of Applied Physiology, 105, 1389–1405. https://doi.org/10.1152/japplphysiol.90408.2008.
Schwab, R. J., Pasirstein, M., Pierson, R., et al. (2003). Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic resonance imaging. American Journal of Respiratory and Critical Care Medicine, 168, 522–530. https://doi.org/10.1164/rccm.200208-866OC.
Fogel, R. B., Trinder, J., White, D. P., et al. (2005). The effect of sleep onset on upper airway muscle activity in patients with sleep apnoea versus controls. Journal of Physiology, 564, 549–562. https://doi.org/10.1113/jphysiol.2005.083659.
Fredberg, J. J. (1974). Pseudo-sound generation at atherosclerotic constructions in arteries. Bulletin of Mathematical Biology, 36, 143–155.
Montazeri, A., Giannouli, E., & Moussavi, Z. (2012). Assessment of obstructive sleep apnea and its severity during wakefulness. Annals of Biomedical Engineering, 40, 916–924. https://doi.org/10.1007/s10439-011-0456-5.
Elwali, A., & Moussavi, Z. (2016). Obstructive sleep apnea screening and airway structure characterization during wakefulness using tracheal breathing sounds. Annals of Biomedical Engineering. https://doi.org/10.1007/s10439-016-1720-5.
Huq, S., & Moussavi, Z. (2012). Acoustic breath-phase detection using tracheal breath sounds. Medical and Biological Engineering and Computing, 50, 297–308. https://doi.org/10.1007/s11517-012-0869-9.
Yadollahi, A., & Moussavi, Z. M. K. (2007). Acoustical respiratory flow: A review of reliable methods for measuring air flow. IEEE Engineering in Medicine and Biology Magazine, 26, 56–61. https://doi.org/10.1109/MEMB.2007.289122.
Katz, M. J. (1988). Fractals and the analysis of waveforms. Computers in Biology and Medicine, 18, 145–156. https://doi.org/10.1016/0010-4825(88)90041-8.
Que, C., Kolmaga, C., Durand, L., et al. (2002). Phonospirometry for noninvasive measurement of ventilation: Methodology and preliminary results. Journal of Applied Physiology, 93, 1515–1526.
Walter, L. M., Dassanayake, D. U., Weichard, A. J., et al. (2017). Back to sleep- or not: The impact of the supine position in pediatric OSA. Sleep Medicine. https://doi.org/10.1016/j.sleep.2017.06.014.
Lan, Z., Itoi, A., Takashima, M., et al. (2006). Difference of pharyngeal morphology and mechanical property between OSAHS patients and normal subjects. Auris Nasus Larynx, 33, 433–439. https://doi.org/10.1016/j.anl.2006.03.009.
Moussavi, Z., Elwali, A., Soltanzadeh, R., et al. (2015). Breathing sounds characteristics correlate with structural changes of upper airway due to obstructive sleep apnea. In: Engineering in Medicine and Biology Society, pp. 5956–5959.
Bechwati, F., Avis, M. R., Bull, D. J., et al. (2012). Low frequency sound propagation in activated carbon. Journal of the Acoustical Society of America, 132, 239–248. https://doi.org/10.1121/1.4725761.
Jensen, O. E. (2002). Flows through deformable airways. Centre for Mathematical Medicine, School of Mathematical Sciences, University of Nottingham, Dynamical Systems in Physiology and Medicine. www.biomatematica.it/urbino2002/programmi/oejnotes.pdf.
Fregosi, R. F., & Fuller, D. D. (1997). Respiratory-related control of extrinsic tongue muscle activity. Respiration Physiology, 110, 295–306. https://doi.org/10.1016/S0034-5687(97)00095-9.
Savi, A., Nikoli, L., Budimir, S., Janoševi, D. (2012). Applications of Higuchi’ s fractal dimension in the analysis of biological signals. In: Telecommunications Forum (TELFOR), pp. 639–641.
Acknowledgement
This study has been supported by Natural Sciences and Engineering Research Council of Canada (NSERC).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hajipour, F., Moussavi, Z. Spectral and Higher Order Statistical Characteristics of Expiratory Tracheal Breathing Sounds During Wakefulness and Sleep in People with Different Levels of Obstructive Sleep Apnea. J. Med. Biol. Eng. 39, 244–250 (2019). https://doi.org/10.1007/s40846-018-0409-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40846-018-0409-7