
Abstract
Prior research consistently shows disgust propensity and/or state disgust correlated with lower sexual arousal; however, this work has largely excluded women with sexual trauma histories. We tested competing models of the effects of disgust on sexual arousal in women with sexual trauma histories: heightened avoidance of sexual stimuli vs. heightened affective antagonism between pathogen disgust and sexual arousal. Seventy-seven women (45 with an unwanted sexual contact history, 32 without) completed an online survey, avoidance task, and sexual arousal task following a pathogen disgust or neutral prime. We conducted preregistered and exploratory analyses of women’s self-reported arousal and behavioral avoidance of the sexual aspects of stimuli. Women who reported more unwanted sexual contact had lower subjective sexual arousal in response to sexual stimuli, particularly following a disgust prime. There was evidence of an interaction such that unwanted sexual contact history amplified the effects of disgust propensity, contributing to greater avoidance of sexual stimuli. Women with a history of forced sex had significantly higher behavioral avoidance of sexual stimuli, even when accounting for exposure to other types of unwanted sexual contact and history of pathogen exposure. Cumulative type and frequency of sexual assault may influence women’s sexual disgust, avoidance, and arousal. Lifetime history of pathogen exposure may not predict sexual disgust. Clinically, our results suggest that sexual avoidance may be a beneficial target of intervention when addressing sexual arousal concerns of survivors of unwanted sex, above and beyond reduction of sexual disgust responses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although early works cast disgust as an adaptive response specific to coordinating pathogen avoidance (Darwin, 1965), current theories on the function of disgust reveal a complex emotion that can be elicited by a range of stimuli (not limited to pathogen cues) and which may coordinate a variety of behaviors depending on context (Curtis et al., 2004; Tybur et al., 2013). Breaking from traditional models, the functional model of disgust posits that in addition to pathogen disgust and toxin avoidance, there are additional forms of disgust that coordinate information processing systems to help resolve potential reproductively-relevant tradeoffs (Tybur et al., 2009). In particular, sexual disgust promotes avoidance of sexual behaviors and partners with potentially low reproductive value, via cognitive (e.g., lowered attention), behavioral (e.g., rejection or expulsion-like behaviors), and affective mechanisms (increased sensitivity to other negative emotions such as contempt; Miceli & Castelfranchi, 2018; Rozin et al., 1999; Tybur et al., 2013).
While much work has proposed an antagonistic relationship between disgust and women’s sexual arousal as a key mechanism of sexual avoidance (e.g., de Jong et al., 2013), little consideration has been made of how disgust operates on sexual response in the context of survivors of sexual violence. This is a particularly critical gap in the literature for three reasons. Firstly, survivors of sexual violence show systematically higher state and trait sexual disgust as well as mental contamination (Brake et al., 2021), pointing to a particularly relevant subgroup for understanding the very nature of sexual disgust. Relatedly, much research points to the importance of body envelope violations for triggering disgust—a phenomenon that is clearly relevant to people whose bodily autonomy has been violated (Amoroso et al., 2020).
Secondly, sexual violence is thought to have shaped the nature of female sexual arousal (Lalumière et al., 2022; Suschinsky & Lalumière, 2011), highlighting the need for models of the relationship between disgust and arousal that account for exposure to sexual violence. Existing models of sexual excitation and inhibition have been criticized for insufficient attention to the dynamics of inhibitory emotions in the context of unwanted sex (Clephane et al., 2022). For example, the Dual Control model of sexual arousal, which posits that arousal is suppressed when excitatory factors are overwhelmed by inhibitory factors such as disgust (Bancroft et al., 2009), may not appropriately account for the potentially adaptive nature of disgust following assault in re-aligning sexual motivation (Toates et al., 2017).
Finally, trait-level disgust propensity is thought to contribute to women’s sexual arousal problems (de Jong et al., 2013), pointing to a potential mechanism underlying the stark disparities in sexual functioning observed in women with sexual violence histories (Schalk et al., 2023). Research on survivors of sexual assault points to different pathways by which disgust and fear become learned responses to erotic cues reinforced by both avoidance behaviors and negative experiences (Brake et al., 2021). Thus, traditional exposure-based therapeutic techniques that target fear, but not sexual disgust, may only partially address post-traumatic distress in women with sexual violence histories (Pascal et al., 2020). In sum, for both theoretic and clinical reasons, there is a clear need for empirical models that bring together research on the interactions of disgust and arousal in women with a history of unwanted sexual contact.
Trait vs. State Level Disgust Effects on Women’s Sexual Arousal
While some research has examined trait-level disgust as a risk factor for sexual arousal dysfunction, the role of state-level disgust on state-level sexual arousal is much more unclear. Trait-level disgust is an individual-level stable tendency to experience or feel disgust. In comparison, acute or state-level disgust is a current and temporary emotional experience, which can be situational. In either case, disgust is defined as a basic emotion that may be accompanied by a characteristic facial expression, physiological responses such as nausea, and behavioral avoidance responses; all of these elements function to protect an person from physical or social harm (for a review see Rozin & Fallon, 1987). Both trait and state disgust may differentially impact women’s sexual arousal and overall sexual functioning. Thus, the purpose of this study was to examine how trait and state disgust may moderate sexual arousal in women with and without unwanted sexual contact histories, to inform the treatment of sexual dysfunction in both groups.
When looking at disgust propensity, there are conflicting patterns of association with sexual arousal that may relate to sexual functioning status. Women with sexual pain dysfunctions such as vaginismus display a higher dispositional disgust propensity than women without sexual concerns (de Jong et al., 2009). Similarly, women diagnosed with vaginismus show increased automatic associations between subjective disgust and sexual stimuli (Borg et al., 2010). Relative to a healthy control group, women with female sexual interest/arousal disorder (FSAID) show higher negative facial affect and more subjective disgust in response to erotic stimuli (DePesa & Cassisi, 2017). In this study, negative facial affect was measured as an exploratory proxy for subjective disgust and could be seen as representative of trait disgust given that facial affect has been correlated with other trait level emotions such as anger (e.g., Godfrey et al., 2021). Additionally, high subjective disgust responses were correlated with more self-reported sexual avoidance behaviors in the FSAID group (DePesa & Cassisi, 2017). Combined, these studies suggest that, for women with diagnosed sexual dysfunction, subjective disgust propensity may play a role in decreasing arousal and increasing sexual avoidance behaviors.
Conversely, Fleischman et al. (2015) found that baseline disgust propensity was not correlated with sexual arousal to erotic stimuli among women without sexual dysfunction. Yet, in this study, women who were exposed to disgusting images before erotic content showed significantly less sexual arousal than women in the control condition (Fleischman et al., 2015). Similarly, in another study of women without sexual dysfunction, Andrews et al. (2015) found that neither pathogen nor sexual disgust propensity were significant in a hierarchical linear model predicting sexual arousal in response to erotic images. However, women in the experimentally induced pathogen disgust prime condition had lower arousal to visual stimuli compared to women in neutral prime condition (Andrews et al., 2015). This suggests that it is possible that state-level disgust responses may be a more salient moderator of sexual arousal than disgust propensity levels, particularly among women without sexual dysfunction. However, it is also possible that state disgust may inhibit arousal and this effect is greater for those with higher state disgust. Further investigation into how state-level vs. trait-level disgust may influence sexual arousal is warranted.
State and trait disgust can also be broken down into various subtypes, each of which may have different associations to sexual arousal. For example, the Three Domains of Disgust Scale (Tybur et al., 2009) measures disgust related to three domains: pathogen, moral, and sexual. Pathogen disgust is hypothesized to promote behavioral avoidance of potential sources of infection. Avoidance of potentially infectious pathogens can occur in sexual situations by promoting avoidance of bodily fluids which may transmit diseases or other infections. Bodily fluids such as vaginal secretions, saliva, blood, and semen are some of the strongest disgust elicitors (Rozin & Fallon, 1987).
In contrast to pathogen disgust, sexual disgust is hypothesized to deter people from engaging in sexual activities that are probabilistically detrimental to their reproductive fitness: that is, the ability to secure a mate who will invest in offspring, conceive, bear young, and raise an offspring to their reproductive maturity. As reproductive fitness is a broad construct, so too are the ways in which sexual disgust may act on sexual behavior. Taking into account cultural influences on the triggers for disgust (Kollareth et al., 2022), sexual disgust may act across six different domains: taboo, oral, promiscuity, BDSM, homosexuality, and hygiene (Crosby et al., 2020). In contrast with pathogen disgust, which is thought to reduce contact with sexual fluids specifically, these other domains of sexual disgust are thought to have evolved to promote avoidance of biologically costly mates and sexual behaviors (Fessler & Navarrete, 2003; Tybur et al., 2009). For example, sexual contact with someone carrying infections or disease, potentially demonstrated via cues of poor hygiene or through increased exposure to bodily fluids via oral sex, would be costly as it introduces risks for reproductive health (Curtis, 2007). Sexual behaviors that are taboo, such as sexual activity with a close relative, are also evolutionally costly by increasing the chance of passing on high-risk recessive genes. Further, sexual behaviors that are considered taboo or against societal norms may be associated with higher levels of moral disgust. Moral disgust is proposed to be evolutionarily beneficial, in part, as a form of disease avoidance (Donner et al., 2023; Van Leeuwen et al., 2023). Research examining the implications of different forms of sexual and pathogen disgust is limited in women with a history of unwanted sexual contact.
Sexual Disgust in Women with History of Unwanted Sexual Contact
The role of unwanted sexual contact in contributing to sexual disgust may also vary in relation to the type of contact and potential traumatic sequalae. Unwanted sexual contact is here defined as any history of unwanted sexual activity including but not limited to unwanted sexual touching including fondling, sexual kissing, manual or oral stimulation, and vaginal or anal intercourse. These activities may be forced, coerced, or conducted without consent due to intoxication or incapacitation. Conversely, sexual trauma broadly refers to the psychological trauma experienced following any sexual act that is imposed on another person without their consent including but not limited to activities such as sexual harassment, intimidation, stalking, and unwanted sexual contact. Such trauma can result in development of post-traumatic stress disorder (PTSD) and other mental health difficulties.
Notably, DePesa and Cassisi (2017) conducted one of few studies on sexual disgust and sexual functioning in women with a history of unwanted sexual contact. In this study, women with a history of unwanted sexual contact were included in both the control group (35%) and the FSAID group (70%). They found that among the FSAID group, a higher proportion of women with elevated disgust response to erotic images reported a history of unwanted sexual contact (87%) compared to women without an elevated disgust response (53.5%). Similarly, a higher proportion of women in the FSAID group who had an elevated disgust response (87%) reported a history of unwanted sexual contact compared to the control group (35.7%).
These findings suggest that sexual disgust sensitivity, which may have initially evolved to reduce contamination from sexually transmitted infections, may be co-opted to reduce arousal in survivors of unwanted sexual contact. To become aroused, survivors would need to be presented with a particularly high-quality sexual stimulus, such as a high-quality mate. Higher levels of disgust, associated with lower sexual arousal, could be adaptive if they slow down reproductive decision-making by increasing women’s selectiveness. If so, we would expect assault survivors to show a broad learned disgust response to sexual cues and higher state disgust. Such selectivity may be needed to counterbalance the effects of a history of unwanted sex sexual contact, particularly childhood sexual abuse, on hypersexuality (Aaron, 2012; Slavin et al., 2020). Further, childhood sexual abuse is associated with an accelerated reproductive timeline in some women such as earlier menarche (Schwab Zabin et al., 2005; Wise et al., 2009), earlier consensual sexual intercourse, and earlier age at first pregnancy (Fiscella et al., 1998). In other words, increased sexual disgust may be adaptive if it slows down an otherwise accelerating life history trajectory. To that end, there is some evidence of variance in reproductive outcomes following childhood sexual assault, with greater voluntary childlessness in survivors and approximately one fifth of survivors reporting delaying pregnancy (Ryan et al., 2014). Speculatively, these may be the survivors for whom disgust reactions are particularly impacted, lowering sexual interest and arousal. In any case, the timing of unwanted sexual contact will likely differentially impact the development of learned disgust response to sexual cues and state disgust, which would then explain differences in sexual behavior observed among women with childhood sexual abuse compared to adult unwanted sexual contact.
Two Mechanistic Models of Sexual Disgust and Arousal in Women with Unwanted Sex Histories
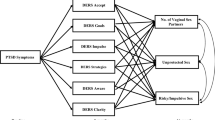
Taking these lines of research together, it is possible disgust may impact women with a history of unwanted sexual contact through one of two paths (Fig. 1A and B). One model suggests that disgust plays a role in women’s sexual arousal via an increased avoidance of sexual stimuli (model 1; Fig. 1A). Women with a history of unwanted sexual contact may develop negative expectations towards sex that could increase the disgust response, which in turn would motivate avoidance of sexual situations. Avoidance behaviors related to disgust include avoiding looking at cues, limiting or refusing physical contact with stimuli, and limiting attention to the stimuli (e.g., Olatunji & Puncochar, 2016). Therefore, it is possible that similar avoidance behaviors may extend to sexual situations corresponding with the development of negative expectations to sexual situations and stimuli.

Proposed theoretical models for the role of disgust on sexual arousal in women with a history of unwanted sexual contact
Andrews et al. (2015) found that behavioral avoidance, as measured by the number of time participants spent viewing sexual images following a disgust prime, was not significantly different among women in the disgust prime condition compared to the neutral condition. Notably in this study, researchers did not distinguish among participants with or without a history of unwanted sexual contact; however, unwanted sexual contact histories may increase avoidance associated with the disgust response. Further, it is possible that the behavioral avoidance tasks in this study were not able to record behavioral avoidance of stimuli as the behavioral tasks only allowed participants to skip through the images faster, not avoid viewing specific aspects of sexual stimuli altogether. Potentially a behavioral avoidance task more aptly measuring avoidance of sexual cues within an image could yield significant differences among people with a history of unwanted sexual contact.
The limited findings related to model 1 have been mixed. For instance, in a study using an approach-avoidance task, people with PTSD and a sexual trauma history avoided stimuli with higher levels of sexual threat (e.g., a sexual assault scene) and non-trauma related threat images when compared to the control group who reported no trauma history (Fleurkens et al., 2014). However, there was no difference between people with PTSD and unwanted sexual contact history in avoidance of stimuli containing consensual sexual images. Additionally, the more PTSD-related symptoms participants reported, the more they avoided threatening trauma-related pictures. These findings suggested there may be differences in avoidance of sexual stimuli corresponding to sexual trauma histories; however, the study was exploratory and did not assess for disgust directly.
A second model suggests that disgust may play a role in women’s sexual arousal via an increase in pathogen exposure leading to higher pathogen disgust (model 2; Fig. 1B). Bodily fluids present during sexual activity—including during unwanted sexual contact—are potentially infectious fluids and pose a risk of harm. Moreover, as emotional activation is often heightened during sexual assault, it is possible that exposure to pathogens may be experienced as particularly disgusting and contribute to a salient learned response to sexual cues. Disgust can be learned with relatively few pairings to a stimulus (Olatunji & Tomarken, 2023), especially under conditions of elevated emotional activity such as sexual assault (Pawłowska et al., 2020; Wang et al., 2021). Thus, in women with a history of unwanted sexual contact, increased disgust response—specifically, higher disgust response to pathogens or focus on disgust cues—may inhibit arousal. Previous research has shown that when exposed to a pathogen disgust prime, sexual arousal to subsequent sexual images was significantly lower compared to the neutral condition (Andrews et al., 2015). Further, people with a lifetime history of exposure to infectious pathogens (i.e., history of childhood illness) may also experience compounded effects. According to this model, we would expect to see women with high levels of lifetime pathogen exposure and/or with unwanted sexual contact histories to have the highest disgust response and lowest arousal.
The Current Study
We analyzed these two potential models of disgust and subjective sexual arousal in women with and without unwanted sexual contact history using a set of online behavioral tasks (see Figs. 2 and 3). While most prior research has examined the effects of trait-level disgust on unwanted sexual contact survivors’ trait sexual functioning, novel to this study, we measured the influence of state-level disgust on state sexual arousal in women with and without unwanted sexual contact histories. That is, this study adds consideration of how state vs. trait disgust influences both disgust response and avoidance to sexual stimuli in women with a history of unwanted sexual contact, and indicates directionality between these constructs. Also, by testing changes in disgust before and after a sexual avoidance task, we were able to disambiguate the direction of the association between disgust and avoidance, investigating whether higher baseline disgust drives greater avoidance, or if avoidance contributes to greater attribution of disgust.

Study procedure

Behavioral avoidance task description. A When viewing the images during the avoidance task, participants were asked to select a set number of boxes on the screen to advance to the next image. Each image was set up with three boxes that covered sexual elements of the stimulus (e.g., genitals) and three boxes that covered non-sexual elements of the image (e.g., background). B When selected, the boxes covered a portion of the image
In sum—while some research has found that higher levels of disgust propensity are correlated with women’s lower sexual arousal, other studies have found no differences in sexual arousal among women with varying levels of disgust propensity. Conversely, state disgust that is increased through experimental manipulation is consistently correlated with lower acute sexual arousal compared to people whose disgust was not experimentally manipulated. This suggests that differences in state-level responses may influence state arousal, independent of a person’s disgust propensity. However, as noted above, this research has typically excluded women with unwanted sexual contact histories. In the present study, we focus on survivors of unwanted sexual contact as opposed to sexual harassment or stalking, as these survivors are more likely to have had body envelope violations—including, importantly, possible contact with bodily fluids. It is possible that state-level disgust might differentially impact acute sexual arousal in women with unwanted sexual contact histories. Women with unwanted sexual contact histories may show a broad learned disgust response to sexual cues, and thus, higher state-level disgust responses, regardless of their disgust propensity. In other words, we may expect less effect of disgust priming in survivors of unwanted sexual contact. In women without unwanted sexual contact histories, however, disgust propensity may play a greater role in predicting state-level disgust responses to sexual stimuli. That is, disgust priming may be relatively more impactful in non-survivors. Finally, it is possible that people with a lifetime history of pathogen exposure will have a higher disgust response than people with a lower lifetime history of pathogen exposure.
Hypotheses
Behavioral Avoidance
We predicted that women with a history of unwanted sexual contact would engage in higher levels of behavioral avoidance of the sexual/erotic aspects of visual sexual stimuli (H1). We also hypothesized that higher levels of disgust would mediate this relationship such that women with higher levels of sexual disgust response, as measured by responses to a one-item question asking participants to rate their level of disgust to sexually explicit images, would have higher levels of behavioral avoidance of sexual stimuli (H2). Additionally, we hypothesized the direction of the effect would be from disgust to avoidance; that is, that pre-trial state disgust and disgust propensity would predict behavioral avoidance, but degree of behavioral avoidance would not predict changes in state disgust (H3).
Disgust and Subjective Arousal Following Experimental Manipulation
For the disgust priming task, we hypothesized that women with a history of unwanted sexual contact would have higher levels of state disgust than the control group, across both the disgust priming and neutral conditions (H4). Correspondingly, we hypothesized that women with a history of unwanted sexual contact would have lower levels of arousal response than the control group, across both the disgust priming and neutral conditions (H5). Further, we hypothesized that, for both women with and without histories of unwanted sexual contact, the disgust priming condition would result in lower sexual arousal compared to both the control and neutral conditions (H6). Moreover, we anticipated that women with a history of unwanted sexual contact in the disgust priming condition would have the highest disgust response and lowest self-reported sexual arousal (H7).
Overall, we theorized that if women with a history of unwanted sexual contact had higher levels of behavioral avoidance compared to the control group, controlling for differences in pathogen exposure, then the findings would support model 1, suggesting that disgust may play a role in women’s sexual arousal via an increased avoidance response of sexual stimuli (model 1). Alternatively, if there was no difference in behavioral avoidance with respect to unwanted sexual contact history, and lower self-reported sexual arousal corresponding with higher levels of pathogen exposure, then the findings would support model 2 (model 2). According to this model, we expected to see women with high levels of lifetime pathogen exposure compounded with unwanted sexual experiences to have the highest disgust response and lowest arousal. This would suggest that disgust may play a role in women’s sexual arousal via an increase in pathogen exposure leading to higher pathogen disgust.
Methods
Participants
Based on a power analysis using effect sizes conducted using G*Power derived from a similar study (Fleischman et al., 2015), we calculated that we would need to a sample of 80 women (40 with and 40 without unwanted sexual contact histories) to detect significant effects of unwanted sexual contact history on sexual disgust and behavioral avoidance of sexual stimuli. Participants were recruited from a participant pool affiliated with the Psychology department at a large university in the Midwestern United States and from Amazon Mechanical Turk (MTurk), an online crowdsourcing platform. The study was advertised as investigating how disgust and prior medical and sexual history influences women’s sexual desire and sexual behavior. Across both platforms, participant inclusion criteria included premenopausal adult women aged 19 or older who reported at least some history of arousal to sexual stimuli depicting mixed-sex couples. Participants could have a history of sexual assault (and indeed, half did), but could not report current significant distress related to their assault history. All participants provided informed consent, and the research protocol was approved by the university Institutional Review Board. Study compensation included credit towards Psychology course research requirements for participants recruited via the university participant pool and monetary compensation for participants recruited via MTurk.
Following a broad literature suggesting that only a minority of women with unwanted sexual experiences identify these experiences as assault or rape, and that women with acknowledged vs. unacknowledged sexual assault experiences may differ in psychological and sexual wellbeing outcomes (for a review see Cleere & Lynn, 2013; Kilimnik & Meston, 2019), we used a broad behavioral definition of unwanted sexual contact history rather than identity as an assault survivor. This accounted for participants who do not label past coercive sexual experiences as necessarily traumatic or victimizing.
Procedure
The current study consisted of three online behavioral tasks: (1) a behavioral avoidance task examining intentional behavioral avoidance of sexual stimuli, (2) disgusting priming task testing self-reported arousal in response to explicit sexual images following either a disgust prime or neutral stimuli set, and (3) a stimuli rating task in which participants viewed sexual images and rated each image in terms of their disgust and arousal. The study was conducted via two sessions, completed 1 to 3 days apart, with each session including all three online behavioral tasks. The study procedures were broken into 2 days to reduce participant burden of completing very long online sessions. Following completion of the first session, participants received reminder emails to complete the second session of the study beginning 24 h after completion of the first session for a total of 3 reminders across 3 days. See Fig. 2 for an overview of all tasks by session and the preregistration of this study for more details (https://shorturl.at/LMU14).
Sexual Avoidance Task
In each session, participants first completed a stimulus avoidance task using a randomly cued set of sexually explicit and neutral images (see “Materials” for details on stimuli validation). Before the avoidance task, participants completed a stimulus rating task, viewing 10 sexual images and rated each image in terms of their disgust and arousal. This served as the “pre-avoidance” rating for arousal and disgust. Participants then proceeded to the behavioral avoidance task.
When viewing the images during the avoidance task, participants were asked to select a set number of boxes on the screen to advance to the next image (Fig. 3A). When selected, the boxes covered a portion of the image (Fig. 3B). Participants were instructed that in order to advance to the next image, they needed to select three boxes and then wait for a few seconds. Each image was set up with three boxes that covered sexual elements of the stimulus (e.g., genitals) and three boxes that covered non-sexual elements of the image (e.g., background). Once participants selected the three boxes, they continued viewing the remaining elements of the image for 3 s. The number of times the participant chose to cover a portion of the image depicting sexual cues vs. peripheral non-sexual cues in the image was used as a measure of behavioral avoidance. Participants completed the cover task with both neutral and erotic images.
Finally, following the avoidance task, participants completed the stimulus rating task a second time, viewing10 different images depicting sexual cues and rating each image in terms of their disgust and arousal.
Disgust Priming Task
Participants then completed a series of prime-target stimuli pairings, using a blocked design. They were randomly assigned to complete either the disgust or the neutral prime block first, counterbalanced for history of unwanted sexual contact, following a within-subjects design. The disgust priming was created via images that have been validated to induce pathogenic disgust, while the neural prime included pictures of commonplace non-food neutral items (modeled after previously validated methods, e.g., Olatunji & Puncochar, 2016). All images were be matched for valence and intensity as validated from the Disgust-Related-Images (DIRTI) picture set (Haberkamp et al., 2017) (disgust prime), the Culpepper Disgust Image Set (C-DIS; Culpepper et al., 2018) (disgust prime), and Open Affective Standardized Image Set (OASIS; Kurdi et al., 2017) (neutral prime). The sexually explicit images (target images) included stimuli that have been previously validated in our lab and were different images than the images shown in the behavioral avoidance portion of the study.
Subjective evaluation of the target sexual stimuli, including self-reported subjective sexual arousal and lack of arousal (e.g., sexually turned off), perceived genital arousal (e.g., genital warmth and lubrication), and perceived general physical arousal (e.g., increased heart rate and breathing), anxiety and disgust were assessed after each individual stimulus presentation. Subjective evaluation of the target sexual stimuli consisted of a series of four questions/statements (e.g., “How sexually aroused are you feeling right now?”) with Likert scale responses from 0 (not at all) to 4 (very much) as used in previous studies (Weijters et al., 2010; Zsok et al., 2017). Participants viewed 30 images per condition, viewing the prime (disgust or neutral) image for 0.5 s and the target (sexual) image for 10 s. Each prime image was followed by questions related to subjective evaluation of the sexual target stimuli and a 45-s distractor task between images.
Survey Measures
Finally, at the end of each session, participants completed a battery of survey items. At the end of session 1, participant completed measures related to demographics, medical history/lifetime history of pathogen exposure, sexual shame, and sexual assault history including number and type of incidents. At the end of session 2, participants completed measures related to sexual shame, disgust propensity and sensitivity, and disgust. Participants also completed a variety of exploratory questions not used in the present analyses (see “Other Measures” below).
Materials
Sexual Arousal Images
Sexual arousal images depicted mixed-sex couples engaging in sexual intercourse. The sexually explicit images included stimuli that have been previously validated to be sexually arousing and highly pleasant and had no cues of sexual violence or qualities shown to interfere with automatic processing of emotional information (e.g., text). Average sexual arousal across images was 4.8 and average valence across images was 5.8 on a Likert-type response scale from 0 (low arousal/valence) to 9 (high arousal/valence).
Disgust Prime Images
Disgust primes were selected from the Disgust-Related-Images picture set (DIRTI; Haberkamp et al., 2017) and the Culpepper Disgust Image Set (C-DIS; Culpepper et al., 2018), which have been well validated to elicit disgust. Images specific to pathogen disgust (e.g., images of dirty sanitary items, fecal matter, and flesh-eating disease) were selected to assess the pathogen disgust responses specifically. All images have been validated to be equal in terms of disgust response level, valence, and intensity.
Neutral Images
Neutral images were drawn from the Open Affective Standardized Image Set (OASIS), which have been validated to demonstrated to elicit neutral responses in terms of valence and intensity (Kurdi et al., 2017). Images depicted neutral non-food commonplace objects (e.g., string). Neutral images were equal in terms of valence and intensity and correspond with the image quality, size, and color properties of the disgust images.
Measures
Behavioral Avoidance Measure
To determine the degree to which participants avoid viewing sexual cues, we analyzed the number of times the participant chose to cover a portion of the image depicting sexual cues or peripheral non-sexual cues in the image. Each image was set up with three boxes that covered sexual elements of the stimulus (e.g., genitals) and three boxes that covered non-sexual elements of the image (e.g., background). Behavioral avoidance was coded as an average score ranging from 0 to 1 with a value of 1 representing that, on average, the participant covered all sexual parts of the image (3 out of 3) and viewing zero (0 out of 3) of the boxes containing sexual parts of the image. Correspondingly, lower values represented higher behavioral avoidance of sexual stimuli. Behvaioral avoidancae was averaged across session 1 and session 2.
Subjective Arousal and Disgust
Subjective Sexual Arousal
Six facets of subjective sexual arousal were measured: perceived sexual arousal, perceived genital arousal, self-reported subjective sexual arousal, and lack of arousal (e.g., sexually turned off), perceived genital arousal (e.g., genital warmth and lubrication), and perceived general physical arousal (e.g., increased heart rate and breathing). Participants were asked to rate their subjective sexual arousal on a scale from 0 (not at all) to 5 (very much). Higher values represented more subjective sexual arousal. Subjective sexual arousal was averaged across session 1 and session 2.The use of this scale and method has been derived from the well-validated and widely used Film Scale (Heiman & Rowland, 1983).
Subjective Sexual Disgust
Subjective sexual disgust, also referred to as state disgust, in response to images was measured by response to a one-item question (“Please rate your level of disgust”) with a Likert-type response scale from 0 (not at all) to 5 (very much). Subjective sexual arousal was averaged across session 1 and session 2. Higher values represented more subjective sexual disgust.
Disgust Measures
Disgust Propensity and Sensitivity (DPSS-R)
Disgust propensity and sensitivity was measured using the 16-item Disgust Propensity and Sensitivity Scale (DPSS-R; van Overveld et al., 2006). Participants viewed eight items on disgust propensity (e.g., “I experience disgust”) and eight items on disgust sensitivity (e.g., “It scares me when I feel faint”). Participants responded to statements about disgust in terms of how often they feel like the statement is true for them on a scale from 0 (never) to 5 (always). Compositive sum scores were calculated for two subscales: disgust propensity and disgust sensitivity (range = 8–40). In the current sample, there was good reliability for both the superordinate factors (α = 0.76 for disgust propensity and α = 0.74 for disgust sensitivity) similar to previous studies (α = 0.78 for disgust propensity and α = 0.79 for disgust sensitivity; Fergus & Valentiner, 2009). Higher values represented higher scores equaling higher disgust propensity or sensitivity.
Sexual Disgust Inventory (SDGI)
The Sexual Disgust Inventory (SDGI) containing various sexual acts used to measure sexual disgust specifically (Crosby et al., 2020). Participants were asked to rate how sexually disgusting they find each item, on a scale from 1 (not at all sexually disgusting) to 7 (extremely sexually disgusting). The SDGI contains six subdomains: taboo, oral sex, BDSM, hygiene, same-sex attraction, and promiscuity, which can be averaged to represent an overall sexual disgust superordinate factor. The SDGI demonstrates high internal consistency within each sexual disgust subdomain (αs > 0.78) (Crosby et al., 2020). In the current sample, there was good reliability for the individual subfactors (αs > ranging from 0.79 to 0.97). This measure differs from the DPSS-R as it is a proxy for sexual disgust specifically, a subcomponent of disgust propensity overall.
Three-Domain Disgust Scale (TDDS)
The Three-Domain Disgust Scale (TDDS) is a 21-item self-report measure of disgust responding in three domains: moral disgust (e.g., deceiving a friend), sexual disgust (e.g., hearing two strangers having sex), and pathogen disgust (e.g., stepping on dog poop). Items are scored on a 7-point Likert-type scale ranging from not at all disgusting (0) to extremely disgusting (6). Higher scores represented higher levels of disgust within each subfactor: moral, sexual, and pathogen disgust. The TDDS demonstrates high internal consistency within each subdomain (α > 0.84) (Olatunji et al., 2012). In the current study, there was moderate reliability for the individual subfactors (αs > ranging from 0.64 to 0.75).
Sexuality and Sexual History Measures
Sexual Coercion Scale (SCS)
The 7-item Sexual Coercion Scale was used to assess lifetime history of unwanted sexual activities, including sexual activity that was coerced (via the use of emotional manipulation or peer pressure to force acquiescence), forced (via physical force) sexual activity, or intoxication-related (e.g., “you were too intoxicated (drunk or high) to say no”) (Mathes & McCoy, 2011). Participants were asked to report how many times they have experienced these events (“never,” “once,” or “more than once”). This measure accounts for participants who do not label past coercive sexual experiences as necessarily traumatic or victimizing. The scale demonstrated adequate internal reliability (α = 0.88; Mathes & McCoy, 2011).
Unwanted sex history was conceptualized as a dichotomous variable, coding any history of unwanted sex activities (1) or no history of unwanted sex activity (0). Further, the SCS was used to examine differences in arousal and disgust response behaviors among different types of unwanted sexual contact, using dichotomous scoring of item responses for any history of coercive, intoxication-related, or forced unwanted sexual contact separately. Lastly, the SCS was used to create a continuous measure of cumulative unwanted sexual trauma history that encompassed both frequency and type of unwanted activity, via summing each of the 7 item responses (“never” = 0, “once” = 1, or “more than once” = 2) with a range of 0–12. Low scores on the continuous SCS variable indicate low frequency and low exposure to different types of unwanted sex, while higher scores indicate higher lifetime frequency and/or exposure to different types of unwanted sex.
Kyle Inventory of Sexual Shame (KISS)
The KISS is a 20-item measure of sexual shame surrounding sexual thoughts, experiences, and behaviors (Kyle, 2013). Participants were asked to rate their agreement on a 6-point scale from 1 (strongly disagree) to 6 (strongly agree; range 20–100), with higher scores reflecting higher levels of sexual shame. The scale demonstrated good internal reliability in the current study (α = 0.81).
Lifetime History of Pathogen Exposure and Health Problems
Participants answered a series of questions on their health history to assess for a lifetime history of pathogen exposure. Questions assessed for exposure to early-life disease, childhood infections, and proximity to others with chronic infections as well as questions pertaining to both current and past health issues. The lifetime history of pathogen exposure measure was created by the authors to assess for a variety of factors related to potential lifetime history of pathogen exposure. Based on a review of the literature on history related to pathogen disgust, we created 5 subscales: general (e.g., “Do you consider yourself a child who was sick frequently?”), environmental (e.g., “Growing up, did you ever live in or near an area with high potential exposure to environmental toxins such as pesticides? For example, on or near a farm or agricultural center, industrial or manufacturing area, or waste disposal center?”), specific health condition (e.g., arthritis, asthma, heart disease), community (e.g., “Was anyone in your household or immediate family severely sick or immunocompromised during your childhood?”), and allergies (e.g., Do you have a history of any type of allergies? ). Based on item response patterns, each participant was coded as low, medium, or high for each subscale. Each subscale was then added together (range 0–15), and participants were again coded into three levels: low (0–2), medium (2–5), or high (3–8) with higher levels representing a higher cumulative lifetime history of pathogen exposure across multiple domains. Please refer to the data dictionary for a comprehensive list of each item included in this variable (https://shorturl.at/fuBX0).
Attention Check
Participants also responded to two attention check items per session embedded in within the survey measures to assess for attention (Berinsky et al., 2014). The first attention check item stated “Over the past month, how often did you time travel? (Please indicate “Almost never or never” below to indicate you are paying attention! )” with 6 response items from “Almost always or always” to “Almost never or never.” The second attention check item was “When was the last time you turned invisible?” with three response options: “Yesterday,” “One year ago,” and “Never.”
Other Measures
Participants were asked to report demographics such as age, gender identity, race/ethnicity, menopause status, pregnancy history, relationship status, sexual attraction, sexual behavior in the past month, use of barrier contraceptives, religious affiliation, religiosity, and a series of other relevant demographics to characterize the sample as part of the survey battery. Participants also reported on mental health history (e.g., PTSD, anxiety, and depression), currently most upsetting event (C-MUTE; Bird et al., 2018), menstruation, anxiety sensitivity, sexual functioning, sexual activity, disclosure of sexual assault, age of first unwanted experience, age of most recent unwanted experience, characteristics of the perpetrator such as relational status (family vs. friend vs. romantic partner vs. dating vs. stranger), and gender of the perpetrator(s).
Analysis Plan
Following our preregistration data analysis plan (https://shorturl.at/LMU14), we conducted a series of general linear models that specified the experimentally manipulated priming condition as a predictor, and the following independent variables and covariates: unwanted sexual contact history, lifetime history of pathogen exposure, disgust propensity, and disgust sensitivity. Outcome variables included behavioral avoidance of sexual stimuli; self-reported sexual disgust and sexual arousal across pre- and post-avoidance tasks; perceived genital arousal and perceived physical arousal across pre- and post-avoidance tasks; and subjective sexual arousal, perceived genital arousal, perceived general physical arousal, and sexual disgust following both the disgust priming and neutral conditions. We conducted both within-participant comparisons (e.g., arousal ratings between the neutral and disgust prime) and between-participants (e.g., disgust ratings and behavioral avoidance measures between women with a history of unwanted sexual contact and the control group). All analyses were performed in R version 4.3.1, adopting an α threshold 0.05 for determining statistical significance. Data for these analyses are publicly available at https://shorturl.at/fuBX0.
Results
Demographic Characteristics
In anticipation of attrition across both sessions, we over-recruited participants regardless of unwanted sexual contact history in. Of a total of 153 participants who completed session 1, 98 (64.05%) completed session 2. Of these, a total of 77 women (45 women with an unwanted sexual contact history, 32 without) passed at least one attention check per session and were included in the final analysis. Although this resulted in uneven groups, there were insufficient research funds to continue recruitment past this point, and thus, a pragmatic decision was made to work with the given data. There were no significant differences on key study variables (e.g., behavioral avoidance of sexual stimuli, disgust propensity, or sexual arousal following the disgust prime, all p values = ns) among women who passed one attention check compared to women who past two attention check. As such, the current analysis included women who passed at least one attention check.
All participants identified their sex assigned at birth as female and identified as cisgender women. Participants were aged 18–24 (Mage = 20.34) and identified as white non-Hispanic (65%), Hispanic/Latine (9%), Asian or Asian America (7%), Multiracial (8%), white Hispanic/Latine (5%), Black or African American (4%), Middle Eastern (1%), and Native Hawaiian or Pacific Islander (1%). See Table 1 for full demographics. Of the 45 women who reported a history of unwanted sexual contact, 20.0% reported unwanted sexual contact via force, 28.9% reported unwanted sexual contact that was intoxication-related, and 95.6% reported unwanted sexual contact via coercion (Fig. 4). Of note, all participants who reported assault by force also reported other forms of unwanted sexual contact (e.g., coercion; Fig. 4.)

Venn diagram depicting the number of participants who reported experiencing each type of unwanted sexual contact (N = 45): force (n = 9), non-intoxication related coercion (n = 43), and intoxication-related unwanted sexual contact (n = 14)
There were no significant difference in age (t(67.778) = 0.038, p = 0.96), relationship status (χ²(3) = 2.89, p = 0.41), racial identity (χ²(7) = 9.64, p = 0.21), or recruitment platform (χ²(1) = 0.09, p = 0.77), between women with and without a history of unwanted sexual contact.
Preregistered Analyses
There were no significant effects of history of unwanted sexual contact as measured by a binary (yes/no) on behavioral avoidance of sexual stimuli (H1 not supported), and no significant moderations of this effect by pathogen exposure (all p values = ns). There were also no significant effects of disgust sensitivity, disgust propensity, or changes in subjective disgust on behavioral avoidance (H3 not supported, all ps = ns). Similarly, sexual disgust did not mediate the relationship between unwanted sexual contact history and behavioral avoidance (H2 not supported). Additionally, there were no differences in average subjective sexual arousal or subjective sexual disgust in the disgust or neutral priming condition between women with a history of unwanted sexual contact and women without (H5 and H4 not supported, all ps = ns).
Across women with and without histories of unwanted sexual contact, the disgust priming condition was associated with lower average subjective sexual arousal compared to the neutral condition (β = 0.17, t(76) = 6.02, p < 0.001, H6 supported). There was also a significant main effect of unwanted sexual contact history on average subjective sexual arousal, such that women with a history of unwanted sexual contact had lower levels of sexual arousal compared to women without an unwanted sexual contact history (β = −0.19, t(84.08) = −1.56, p < 0.001) across conditions (Fig. 5). The interaction between priming condition and unwanted sexual history was not significant (H7 not supported). A complete report on all preregistered hypothesis testing is available here https://shorturl.at/vFNQ6.

Sexual arousal following disgust and neutral prime conditions in women with and without a history of unwanted sexual contact
Exploratory Analyses
All analyses listed in this section were conducted to follow up on the results of the preregistered analyses and should be interpreted as purely exploratory. As such, we did not make statistical adjustments for multiple comparisons.
Different types of unwanted sexual contact have been associated with differential negative outcomes such as survivor reported perception of severity (Abbey et al., 2004), post-traumatic stress symptoms (Brown et al., 2009; Kern & Peterson, 2020), and thoughts of blame/shame as well as negative thoughts about themselves and the world (Kern & Peterson, 2020). Additionally, the cumulative effects of revictimization have been shown to be associated with more aversive outcomes (e.g., Ullman & Najdowski, 2009; Walsh et al., 2011). Given the differences in aversive outcomes by both type and frequency of unwanted sexual contact, we explored the hypothesized models across different types of unwanted sexual contact (force, coercion, intoxication) as well as with unwanted sexual contact as a continuous score of both frequency and type.
Behavioral Avoidance Task Exploratory Analyses
Women with a history of unwanted sexual contact involving force had significantly higher behavioral avoidance of sexual stimuli when accounting for lifetime history of pathogen exposure and exposure to intoxication-related or coercion-related unwanted sex (β = −0.268, t(4, 71) = 6.915, p < 0.001); full model R2 = 0.210, F(4, 71) = 4.714, p = 0.002. There were no differences in behavioral avoidance of sexual stimuli among other types of unwanted sexual contact in this model. There was also a small but significant effect of lifetime history of pathogen exposure on behavioral avoidance when accounting for force, intoxication-related, and coercion-related unwanted sexual trauma histories (β = 0.075, t(4, 71) = 2.147, p = 0.035) (exploratory follow-up for H1).
When considering a history of unwanted sexual contact as a continuous score of both frequency and type, as opposed to a dichotomous “any/none” variable, there was tentative evidence of a interaction between disgust propensity and unwanted sexual history severity, such that for women with less unwanted sexual contact, higher pre-trial disgust propensity resulted in lower (albeit not significantly lower) avoidance of sexual stimuli (β = −0.005, t(3, 67) = −1.966, p = 0.053). For women with more unwanted sexual contact, higher pre-trial disgust propensity resulted in higher avoidance of sexual stimuli (exploratory follow-up for H3). Disgust sensitivity had a similar trending interaction (β = −0.004, t(3, 65) = −1.789, p = 0.078).
We then considered sexual disgust overall as measured by the SDGI (rather than general disgust as measured by the DPSS). There was no significant effect of the total score for the SDGI on avoidance of sexual stimuli (R2 = 0.0177, F(1, 71) = 1.282, p = 0.261). However, when investigating specific subtypes of sexual disgust, there was higher behavioral avoidance of sexual stimuli in women who reported higher levels of disgust to oral sex (R2 = 0.042, F(1, 75) = 3.323, p = 0.072) and to BDSM (R2 = 0.046, F(1, 75) = 3.648, p = 0.060); while these effects were not statistically significant, they approached significance. Further, there was evidence of a significant main effect and interaction between reported disgust on the oral sex subscale and unwanted sexual history severity (R2 = 0.126, F(3, 73) = 3.495, p = 0.020). As seen in Fig. 6, higher oral sex disgust is associated with more avoidance of sexual stimuli, with amplified effects at higher levels of unwanted sex history. While the overall model and main effect were statistically significant for the BDSM subscale (R2 = 0.112, F(3, 73) = 3.095, p = 0.032), the interaction was not significant (p = ns) (exploratory follow-up analyses for H3). However, women who reported higher levels of disgust to BDSM reported higher levels of moral disgust (R2 = 0.151, F(1, 73) = 14.480, p < 0.00). There were no significant effects for any of the other sexual disgust subscales (hygiene, incest, unusual sex, same sex, promiscuity, and taboo).

Behavioral avoidance of sexual stimuli among women with high and low levels of unwanted sexual contact history across levels of disgust to oral sex
Disgust Priming Task Exploratory Analyses
Finally, when considering a history of unwanted sexual contact as a continuous frequency score, as opposed to a dichotomous variable, women with more unwanted sexual contact had lower subjective sexual arousal in the disgust priming condition (R2 = 0.071, F(1, 75) = 5.751, p = 0. 018) and trending in the same direction for the neutral priming condition (R2 = 0.045, F(1, 75) = 3.561, p = 0.063; exploratory follow-up for H5). Additionally, women with higher levels of sexual shame, as measured by the KISS, had lower subjective sexual arousal in the disgust priming condition (R2 = 0.061, F(1, 75) = 4.945, p = 0.029) but not in the neutral priming condition (R2 = 0.030, F(1, 75) = 2.396, p = 0.126) (exploratory follow-up for H5).
Discussion
Combining separate lines of research on the impacts of disgust on sexual arousal in women with unwanted sexual contact history, we examined women’s behavioral avoidance of and subjective arousal responses to visual sexual stimuli following a pathogen disgust priming task, analyzing changes among different levels of state responses. Our results indicated that broadly, women who reported more unwanted sexual contact had lower subjective sexual arousal in response to sexual stimuli, particularly following a disgust prime. Additionally, women with a history of unwanted sexual contact by force had significantly higher behavioral avoidance of sexual stimuli, even when accounting for their exposure to other types of unwanted sexual contact and lifetime history of pathogen exposure. Lastly, there was evidence of an interaction between disgust propensity and unwanted sexual history, such that among women who reported more unwanted sexual contact, higher disgust propensity resulted in higher avoidance of sexual stimuli. This suggests that both trait-level disgust and cumulative experiences of unwanted sexual contact interact to impact sexual avoidance.
Disgust May Impact Subjective Arousal via Behavioral Avoidance
As hypothesized, across women with and without histories of unwanted sexual contact, the disgust priming condition was associated with lower average subjective sexual arousal compared to the neutral priming condition. These findings extend prior research on aversive classical conditioning learning of disgust in which pairing disgust cues with sexual stimuli is associated with a decrease in sexual arousal (Andrews et al., 2015; Fleischman et al., 2015; Pawłowska et al., 2020). These prior studies examined the effects of experimentally manipulated participant’s disgust on subsequent sexual arousal but did not consider factors that may influence both sexual arousal and disgust response such as experiencing sexual trauma. In the current study, when considering a history of unwanted sexual contact both as a binary variable and on a continuum, women with a history of unwanted sexual contact had lower arousal in response to the disgust prime. This suggests that the effects of the disgust prime on sexual arousal were more salient for women with unwanted sexual contact, and this finding was amplified in women with more diverse and frequent experiences of unwanted sex, possibly through their increased avoidance of sexual stimuli.
Separately, the results from the behavioral avoidance task suggest that women with a history unwanted sexual contact by force had significantly higher avoidance of sexual stimuli than women without such histories, even when accounting for their exposure to other types of unwanted sexual contact or pathogen exposure. Previous studies on behavioral avoidance found that avoidance of sexual stimuli was not significantly different among women in a disgust prime condition compared to a neutral condition (Andrews et al., 2015). It is possible that the behavioral avoidance task in the current study captured a different aspect of avoidance of sexual stimuli. In prior research, behavioral avoidance was measured in time spent looking at an entire sexual image, limiting the ability for investigators to measure avoidance of specific parts of the image. However, other research using eye-tracking suggests that degree of inattention to sexual elements of visual sexual stimuli (e.g., genitals) significantly predicts arousal dysfunction, pointing to the need to examine which parts of the image women are avoiding (Velten et al., 2021). In the current study, our measure of behavioral avoidance reflected a conscious decision by each participant to cover the sexual aspects (e.g., genitals) of sexual stimuli.
Taking the behavioral avoidance findings in conjunction with the results of the disgust priming task, the evidence broadly supports our model 1 (Fig. 1A), with disgust playing a role in women’s sexual decreased arousal via an increased avoidance of the arousing elements of sexual cues. Specifically, our results suggest that behavioral avoidance is a mechanism between disgust and lower arousal, particularly among survivors of forced sexual contact. This indicates that the effects of disgust on arousal response may be indirect, decreasing engagement with the arousing aspects of sexual cues, rather than a direct opposition between approach (arousal) and avoidance (disgust) related affect. Previous literature on disgust has indicated that disgust works antagonistically against arousal such that arousal is suppressed when excitatory factors are overwhelmed by inhibitory factors such as disgust (Bancroft et al., 2009). Such antagonism models would suggest that arousal does not arise when high levels of disgust are present. In contrast, our data suggest that arousal is not directly suppressed by disgust, but that sexual arousal is not being triggered due to the avoidance of sexual cues that is a result of disgust. In other words, it is not that excitatory cues are overwhelmed by inhibitory cues; rather, there is insufficient exposure to excitatory cues to generate an arousal response.
Disgust and Sexual Avoidance Differ Between Survivors of Forced Sex vs. Coercion
Notably, the effects of state disgust, as measured by subjective sexual disgust, on avoidance of sexual cues were most pronounced in women with a history of unwanted sexual contact involving force. In the current sample, all participants who reported a history of sexual assault involving force also reported a history of sexual coercion (Fig. 3). These trends are consistent with prior research (e.g., Norris et al., 2021). The cumulative effect of force and coercion may be more tightly associated with conscious behavioral avoidance of sexual stimuli than coercion alone. Experiences of unwanted sexual contact involving coercion are experienced at higher rates than other forms of unwanted sexual contact, with half of college age women reporting experiencing sexual coercion in their first year of college (Norris et al., 2021).
Given the prevalence of sexual coercion, women may normalize experiences of sexual coercion and integrate these experiences into typical sexual scripts (Krahé et al., 2021). Notably, research has shown that women broadly viewed unwanted sexual experiences and sexual assault as a “normal experience” (Canan et al., 2023). Building sexual coercion into normal sexual scripts may also include the underlying perception that women themselves have a less agency in their sexual experiences. Research on the observational stance suggests that women may be more likely to adopt an observer stance (imagining themselves as passive observers of the sexual stimuli) rather than an active stance (imaging themselves as the actors in the sexual stimuli; Bossio et al., 2014). Correspondingly, higher subjective sexual arousal is associated with imagining oneself as an active participant in the scenario (Bossio et al., 2014). It is possible that as women incorporate sexual coercion into their sexual scripts, they may adopt an observer stance when viewing sexual stimuli. As such, they may attend to and engage with sexual stimuli differently. As such, the normalization of sexually coercive experiences could be associated with preconscious avoidance and differential engagement, while cumulative experiences involving force, viewed as more severe, contribute to a more overt and conscious avoidance. Future research should examine how women with varying types of unwanted sexual contact histories vary in different in types of sexual avoidance such as behavioral, cognitive, and attentional.
Additionally, experiences of sexual coercion have varied effects on patterns of negative self-perception and self-blame as well as differences in feelings of helplessness and psychological outcomes (Brown et al., 2009; Ullman et al., 2007). For instance, women who experience sexual coercion do not conceptualize their experiences as “bad enough” and report higher levels of self-blame (Canan et al., 2023; Ullman et al., 2007). However, these differences in negative self-perception and psychological outcomes vary across a variety of societal and situation factors. It is possible that as sexually coercive experiences are interpreted differently, women experience variability in levels of sexual avoidance. Importantly, type of unwanted sexual contact is not the sole determinant for the level of distress and functioning and all people working with survivors should center each person’s experience.
Oral Sex and BDSM Disgust Correlates of Behavioral Avoidance
While research on disgust broadly has been associated with general behavioral avoidance, it has also been proposed that sexual disgust specifically may influence avoidance of sexual stimuli (Crosby et al., 2020). When investigating specific subtypes of sexual disgust, we found that there was higher behavioral avoidance of sexual stimuli in women who reported higher levels of disgust to oral sex and to BDSM (bondage, discipline, dominance, submission, and sadomasochism).
Oral sex is associated with bodily fluids such as vaginal secretions, saliva, and semen, which are some of the strongest disgust elicitors (Ballini et al., 2012). Additionally, research has shown salient threats of disease (such as bodily fluids) are associated with aversion of casual sex and future sexual intentions, particularly among women (Murray et al., 2013). This aversion of sexual activity is proposed to be protective in reducing risk of infection. Taken together, behavioral immunity theory supports our finding that higher oral sex disgust would be associated with more avoidance of sexual stimuli (Murray et al., 2013). However, in the current sample, we did not find pathogen sexual disgust associated with higher behavioral avoidance of sexual stimuli as research on behavioral immunity theory would predict. It is possible that pathogen disgust plays a role in avoidance of sexual stimuli across women with and without a history of unwanted sexual experiences, but the effects are not seen due to other factors. This may indicate that the suppressing effect of oral sex-related disgust on sexual avoidance is more nuanced.
The suppressing effect of oral sex-related disgust on sexual avoidance in our study appears to be more prominent among women without a history of unwanted sexual contact (Fig. 6). In other words, for women without a history of unwanted sexual contact, higher levels of oral sex disgust resulted in an amplified avoidance of sexual stimuli. One possibility is that, among women without a history of unwanted sexual experiences, oral sex is viewed as a more intimate form of sex. For heterosexual young people, oral sex can represents a continuation of gender inequality and the lack of sexual reciprocity (Lewis & Marston, 2016), with women and men reporting providing oral sex to men as “expected.” Further, women with a history of unwanted sex may have learned that engaging in activities such as oral sex reduces the risk for further sexual victimization. Indeed, women report acquiescing to oral sex to reduce the risk of sexual assault (Hlavka, 2014). However, ultimately these findings should be treated as exploratory as our analyses examining oral sex disgust were post hoc. Further testing is needed to disambiguate these surprising findings.
Women who reported higher levels of disgust to BDSM also had higher levels of behavioral avoidance of sexual stimuli. BDSM generally refers to sexual experiences that involve some sort of power exchange between consenting partners and/or the inclusion of pain or other sensations with the purpose of eliciting sexual pleasure (Holvoet et al., 2017). BDSM practices are rooted in continuous and affirmative consent. A recent study found that 68.8% of sexually active participants reported at least one BDSM fantasy or practice (Holvoet et al., 2017). Despite the interest and prevalence of BDSM fantasies and practice in current culture, historically BDSM was associated with psychopathology, paraphilic disorders (e.g., Moser & Kleinplatz, 2020), and childhood trauma; as such, BDSM practice is associated with stigmatization and social norms violations (e.g., Hansen-Brown & Jefferson, 2023; Kolmes et al., 2006). It is possible that participants who view BDSM as a violation of social norms may be experiencing higher levels of moral disgust to sexual stimuli. Correspondingly, in our sample, women who reported women who reported higher levels of disgust to BDSM reported higher levels of moral disgust The Moral Foundations Theory proposes that pathogen avoidance promotes moral disgust. Specifically, following moral rules and norms can serve, in part, as a disease avoidance (Van Leeuwen et al., 2023). Moral disgust has also been linked with behavioral strategies for pathogen avoidance (Donner et al., 2023. Additionally, activation of the behavioral immune system (i.e., behavioral responses to disease cues) has been associated with more negative attitudes towards stigmatized groups and prejudice and discrimination such as “sexually promiscuous people” (Petersen, 2017; Schaller & Murray, 2008)).
Additionally, engagement in BDSM practices are associated with an increased emphasis on the emotional experience and interpersonal connections (Simula, 2019). It is also possible that like oral sex disgust, BDSM disgust serves as avoidance of intimacy and emotional closeness among women with a history of unwanted sexual experiences. Taken together, it is possible that among people with higher sexual disgust towards BDSM practices, high behavioral avoidance to sexual stimuli is a product of both a learned behavioral response for pathogen-avoidance and conscious avoidance of interpersonal closeness. Again, given our BDSM findings were exploratory, these explanatory models should be treated as speculative.
Disgust Propensity
While some research has found that higher levels of disgust propensity are correlated with lower sexual arousal in women (de Jong et al., 2009; DePesa & Cassisi, 2017), other studies have found no differences in sexual arousal among women with varying levels of disgust propensity (e.g., Andrews et al., 2015; Fleischman et al., 2015; Grauvogl et al., 2015). In the current study, there was an interaction between disgust propensity and unwanted sexual history severity, such that for women with lower exposure to unwanted sexual contact, higher pre-trial disgust propensity resulted in lower avoidance of sexual stimuli. Women with higher disgust propensity broadly have more of a tendency to experience or feel disgust. Following de Jong’s model of sexual arousal, for women without an unwanted sexual trauma history, sexual arousal may persist in overcoming inhibitory factors such as disgust, and result in lower avoidance of sexual stimuli.
A prior study found that disgust propensity was higher in women with sexual pain dysfunction than women without sexual concerns (e.g., de Jong et al., 2009) while another found that disgust propensity was not correlated with sexual arousal in response to sexual stimuli (e.g., Fleischman et al., 2015). Notably, these studies did not distinguish among women with an unwanted sexual contact history. Our results suggest that the variance in prior research findings could be attributed to the lack of inclusion of unwanted sexual contact history in the models. It is possible that women with unwanted sexual contact histories may have a broad learned disgust response to sexual cues (that is, higher state disgust) regardless of their disgust propensity (i.e., trait disgust). For women with higher levels of exposure to unwanted sexual contact, state disgust may be a more salient influence on sexual arousal than trait disgust or disgust propensity. As such, behavioral avoidance differences were only seen among women with lower levels of unwanted sexual contact.
Evaluation of Theoretical Models
We proposed two potential models for how the disgust response impacts subjective sexual arousal in women with unwanted sexual contact history (Fig. 1). Overall, our results support model 1 (Fig. 1A), suggesting that disgust may play a role in women’s sexual arousal via an increased avoidance of sexual stimuli correlated with higher sexual disgust. For model 2 (Fig. 1B), we proposed that disgust may play a role in women’s sexual arousal via an increase in pathogen exposure leading to higher pathogen disgust. In general, our results related to pathogen exposure were not significant. There was a small but significant effect of lifetime history of pathogen exposure on behavioral avoidance when accounting for force, intoxication-related, and coercion-related unwanted sexual trauma histories. However, when accounting for the effects of lifetime history of pathogen exposure and exposure to intoxication-related or coercion-related unwanted sex, women with a history of with a history of unwanted sexual contact involving force had significantly higher behavioral avoidance of sexual stimuli. Taken together, a history of unwanted sexual contact involving force was a more significant predictor of behavioral avoidance above and beyond the effects of lifetime history of pathogens, supporting model 1.
Strengths of the Current Study
Behavioral Measurement of Avoidance
To examine conscious behavioral avoidance, we developed an online behavioral task that allowed us to measure conscious behavioral avoidance of specific parts of an image. While behavioral avoidance has been measured using online tasks of attention such as willingness to view an image for longer (e.g., Pawłowska et al., 2020) and eye-tracking (Garza et al., 2023), previous studies on behavioral avoidance of sexual stimuli in relationship to disgust have shown conflicting results, potentially due to the way in which avoidance is measured. The current study allows for measurement of conscious behavioral avoidance of sexual cues. Our findings suggest the feasibility of implementing a cost-effective and easily interpretable measurement of behavioral avoidance of the sexual cues within an image via an online platform, allowing for ease of replicability of the current study and future implementation.
Measurement Across the Range of Unwanted Sexual Contacts
Despite the theoretical implications of unwanted sexual assault on sexual functioning, to our knowledge, one study has been conducted on disgust, sexual arousal, and sexual avoidance in women with a history of unwanted sexual contact. In this study, sexual assault history was measured as a binary variable and was not a variable of interest in analyses (DePesa & Cassisi, 2017). In the current study, unwanted sexual contact was defined as an unwanted experience of any of the following: sexual touching including fondling, sexual kissing, and/or manual stimulation; oral stimulation of one’s own or another person’s genitals; and vaginal or anal intercourse. This activity may have been forced, coerced, or imposed due to lack of ability to consent (e.g., due to intoxication). Behavioral avoidance of sexual stimuli was associated specifically among women who experienced both force and coercion related unwanted sexual contact. Further, findings across the study were only significant when examining unwanted sexual contact on a continuum of both type and frequency as opposed to binary. This suggests that both a higher frequency of occurrences as well as experiencing multiple types of unwanted sexual contact act on women’s sexual arousal in the context of avoidance and disgust. The cumulative effects of unwanted sexual trauma history are associated with difficulties in emotion regulation (Walsh et al., 2011), increased alcohol use and alcohol expectancies (Palmer et al., 2010), and higher risk of revictimization (Norris et al., 2021). Given this, is not surprising that the cumulative effects of type and frequency of unwanted sexual contact was associated with differences in avoidance and arousal in the current study, suggesting the need for research to be inclusive of a wide array of unwanted sexual experiences. That said, although the proportion of participants reporting forced sexual experienced was substantial, owing to an overall small sample size the number of participants with these histories was low (n = 9), indicating a need to replicate and extend these findings. Such replications may also further illuminate the literature on how disgust and fear respond to exposure-based treatments, which has identified a critical role for change in disgust in reducing post-traumatic stress (Badour & Feldner, 2016) but which has to date largely focused on survivors of forced sexual assault (Pascal et al., 2020).
Limitations of the Current Study
In the current study, we measured life history of pathogen exposure using cross-sectional retrospective reporting on a variety of questions related to health history, including exposure to early-life disease, childhood infections, and proximity to others with chronic infections as well as questions pertaining to both current and past health issues. While this measure captures lifetime history of exposure to pathogens, a more intensive measure including specific questions related to cumulative exposure to bodily fluids, spoiled foods, or other salient pathogen carriers may measure possible effects of pathogens exposure more fully. In particular, bodily fluids such as vaginal secretions, saliva, blood, and semen are some of the strongest disgust elicitors (Rozin & Fallon, 1987). Further, participants reported subjective sexual arousal in the current study. Given that subjective sexual arousal and genital sexual arousal are, at times, non-concordant (Lalumière et al., 2022; Clephane et al., 2022), the next steps of this research should examine associations with measures of genital arousal. Additional variables such as sociosexual orientation (O’Shea et al., 2019) may also be important to consider in future studies given the association between sociosexual orientation and disgust propensity. Additionally, although we were appropriately powered to detect effects reported in a similar study on sexual disgust (Fleischman et al., 2015), a more diverse sample may yield more reliable and generalizable estimates of the true effect. For example, it possible that examining the role of unwanted sexual trauma and disgust on avoidance of sexual stimuli may look different in an older population of women with more potentially more cumulative life experience and different evolutionary pressures for sexual reproduction, which may also contribute to differences in sexual avoidance.
Implications
Broadly, our results indicate that not just a history of sexual assault, but cumulative type and frequency of sexual assault, influences sexual disgust, avoidance, and arousal. This adds to prior research, suggesting the necessity of using a broader definition of unwanted sexual experiences to examine effects of different types of unwanted sex.
Clinically, our results indicate that when working with sexual assault survivors, it is important to conceptualize the effects of both the type(s) and frequency of unwanted sexual experiences on sexual arousal. Moreover, in our behavioral avoidance task, the decision to avoid sexual aspects of the stimuli occurred at a conscious level. This suggests that, regardless of awareness, disgust may promote conscious avoidance of sexual stimuli as a default behavior. However, it is possible that when presented with specific instructions to attend to sexual stimuli (i.e., to override a default tendency towards behavioral avoidance), women with a history of unwanted sexual contact will experience a natural arousal response. Other research suggests that instruction to maintain deliberative and sustained attention to sexual stimuli increases arousal in women both with and without sexual dysfunction (Velten et al., 2021). In other words, if sexual avoidance is consciously controllable, it may be a particularly beneficial target for clinical intervention when addressing sexual arousal concerns of survivors of unwanted sex.
Some forms of treatment for women with increased disgust response have focused on reduction of the disgust response through use of exposure based treatments (Badour & Feldner, 2016; Meunier & Tolin, 2009). Our results suggest that interventions such as exposure therapy and cognitive behavioral therapy may work particularly well for women with higher levels of disgust response following an unwanted sexual contact history as both treatments can work towards targeting the avoidance specifically. Avoidance is a key mechanism in maintaining symptoms of post-traumatic stress among survivors of unwanted sex. Research has shown both cognitive and exposure-based therapies have been effective in reducing the avoidance (Foa et al., 2013; Watkins et al., 2018). Our results indicate that it might be beneficial to focus on reduction of avoidance of sexual stimuli, as opposed to a primary focus on reduction of the disgust response itself.
References
Aaron, M. (2012). The pathways of problematic sexual behavior: A literature review of factors affecting adult sexual b. Sexual Addiction & Compulsivity, 19(3), 21.
Abbey, A., BeShears, R., Clinton-Sherrod, A. M., & McAuslan, P. (2004). Similarities and differences in women’s sexual assault experiences based on tactics used by the perpetrator. Psychology of Women Quarterly, 28(4), 323–332. https://doi.org/10.1111/j.1471-6402.2004.00149.x.
Amoroso, C. R., Hanna, E. K., LaBar, K. S., Borg, S., Sinnott-Armstrong, J., W., & Zucker, N. L. (2020). Disgust theory through the lens of psychiatric medicine. Clinical Psychological Science, 8(1), 3–24. https://doi.org/10.1177/2167702619863769.
Andrews, A. R., Crone, T., Cholka, C. B., Cooper, T. V., & Bridges, A. J. (2015). Correlational and experimental analyses of the relation between disgust and sexual arousal. Motivation and Emotion, 39(5), 766–779. https://doi.org/10.1007/s11031-015-9485-y.
Badour, C. L., & Feldner, M. T. (2016). Disgust and imaginal exposure to memories of sexual trauma: Implications for the treatment of posttraumatic stress. Psychological Trauma: Theory Research Practice and Policy, 8(3), 267–275. https://doi.org/10.1037/tra0000079
Ballini, A., Cantore, S., Fatone, L., Montenegro, V., De Vito, D., Pettini, F., Crincoli, V., Antelmi, A., Romita, P., Rapone, B., Miniello, G., Perillo, L., Grassi, F. R., & Foti, C. (2012). Transmission of nonviral sexually transmitted infections and oral sex. The Journal of Sexual Medicine, 9(2), 372–384. https://doi.org/10.1111/j.1743-6109.2011.02515.x
Bancroft, J., Graham, C. A., Janssen, E., & Sanders, S. A. (2009). The dual control model: Current status and future directions. Journal of Sex Research, 46(2–3), 121–142. https://doi.org/10.1080/00224490902747222.
Berinsky, A. J., Margolis, M. F., & Sances, M. W. (2014). Separating the shirkers from the workers? Making sure respondents pay attention on self-administered surveys. American Journal of Political Science, 58(3), 739–753. https://doi.org/10.1111/ajps.12081.
Bird, E. R., Seehuus, M., Heiman, J. R., Davis, K. C., Norris, J., & George, W. H. (2018). Sexual vs. nonsexual currently most upsetting trauma: A fresh look at attenuation of sexual response, alcohol intoxication, and post-traumatic stress. The Journal of Sex Research, 55(7), 915–926. https://doi.org/10.1080/00224499.2017.1380159.
Borg, C., de Jong, P. J., & Schultz, W. W. (2010). Vaginismus and dyspareunia: Automatic vs. deliberate disgust responsivity. The Journal of Sexual Medicine, 7(6), 2149–2157. https://doi.org/10.1111/j.1743-6109.2010.01800.x.
Bossio, J. A., Spape, J., Lykins, A. D., & Chivers, M. L. (2014). Observational stance as a predictor of subjective and genital sexual arousal in men and women. The Journal of Sex Research, 51(3), 303–315. https://doi.org/10.1080/00224499.2012.729276.
Brake, C. A., Tipsword, J. M., & Badour, C. L. (2021). Mental contamination, disgust, and other negative emotions among survivors of sexual trauma: Results from a daily monitoring study. Journal of Anxiety Disorders, 84, 102477. https://doi.org/10.1016/j.janxdis.2021.102477.
Brown, A. L., Testa, M., & Messman-Moore, T. L. (2009). Psychological consequences of sexual victimization resulting from force, incapacitation, or verbal coercion. Violence against Women, 15(8), 898–919. https://doi.org/10.1177/1077801209335491.
Canan, S. N., Kaplan, A. M., & Jozkowski, K. N. (2023). A national us study of 906 women’s qualitative accounts of their reactions during sexual assault. Sexuality Research and Social Policy, 20(3), 977–992. https://doi.org/10.1007/s13178-022-00772-1.
Cleere, C., & Lynn, S. J. (2013). Acknowledged versus unacknowledged sexual assault among college women. Journal of Interpersonal Violence, 28(12), 2593–2611. https://doi.org/10.1177/0886260513479033.
Clephane, K., Sartin-Tarm, A., & Lorenz, T. K. (2022). Four additional questions for the preparation hypothesis. Archives of Sexual Behavior, 51, 737–742. https://doi.org/10.1007/s10508-020-01798-5
Crosby, C. L., Durkee, P. K., Meston, C. M., & Buss, D. M. (2020). Six dimensions of sexual disgust. Personality and Individual Differences, 156, 109714. https://doi.org/10.1016/j.paid.2019.109714.
Culpepper, P. D., Havlíček, J., Leongómez, J. D., & Roberts, S. C. (2018). Visually activating pathogen disgust: A new instrument for studying the behavioral immune system. Frontiers in Psychology, 9, 1397. https://doi.org/10.3389/fpsyg.2018.01397.
Curtis, V. A. (2007). A natural history of hygiene. Canadian Journal of Infectious Diseases and Medical Microbiology, 18(1), 11–14. https://doi.org/10.1155/2007/749190.
Curtis, V., Aunger, R., & Rabie, T. (2004). Evidence that disgust evolved to protect from risk of disease. Proceedings of the Royal Society of London. Series B: Biological Sciences, 271(suppl_4). https://doi.org/10.1098/rsbl.2003.0144.
Darwin, C. (1965). The expression of emotions in man and animal. University of Chicago Press. (Original work published 1872).
de Jong, P. J., van Overveld, M., & Borg, C. (2013). Giving in to arousal or staying stuck in disgust? Disgust-based mechanisms in sex and sexual dysfunction. Journal of Sex Research, 50(3/4), 247–262. https://doi.org/10.1080/00224499.2012.746280
de Jong, P. J., van Overveld, M., Weijmar Schultz, W., Peters, M. L., & Buwalda, F. M. (2009). Disgust and contamination sensitivity in vaginismus and dyspareunia. Archives of Sexual Behavior, 38(2), 244–252. https://doi.org/10.1007/s10508-007-9240-x
DePesa, N. S., & Cassisi, J. E. (2017). Affective and autonomic responses to erotic images: Evidence of disgust-based mechanisms in female sexual interest/arousal disorder. The Journal of Sex Research, 54(7), 877–886. https://doi.org/10.1080/00224499.2016.1252307.
Donner, M. R., Chagas-Bastos, F. H., Jeremiah, R. W., & Laham, S. M. (2023). Pathogens or promiscuity? Testing two accounts of the relation between disgust sensitivity and binding moral values. Emotion. https://doi.org/10.1037/emo0001280.
Fergus, T. A., & Valentiner, D. P. (2009). The disgust propensity and sensitivity scale–revised: An examination of a reduced-item version. Journal of Anxiety Disorders, 23(5), 703–710. https://doi.org/10.1016/j.janxdis.2009.02.009.
Fessler, D. M. T., & Navarrete, C. D. (2003). Domain-specific variation in disgust sensitivity across the menstrual cycle. Evolution and Human Behavior, 24(6), 406–417. https://doi.org/10.1016/S1090-5138(03)00054-0.
Fiscella, K., Kitzman, H. J., Cole, R. E., Sidora, K. J., & Olds, D. (1998). Does child abuse predict adolescent pregnancy? Pediatrics, 101(4), 620–624. https://doi.org/10.1542/peds.101.4.620.
Fleischman, D. S., Hamilton, L. D., Fessler, D. M. T., & Meston, C. M. (2015). Disgust versus lust: Exploring the interactions of disgust and fear with sexual arousal in women. PLOS ONE, 10(6), e0118151. https://doi.org/10.1371/journal.pone.0118151.
Fleurkens, P., Rinck, M., & van Minnen, A. (2014). Implicit and explicit avoidance in sexual trauma victims suffering from posttraumatic stress disorder: A pilot study. European Journal of Psychotraumatology, 5(1), 21359. https://doi.org/10.3402/ejpt.v5.21359.
Foa, E. B., McLean, C. P., Capaldi, S., & Rosenfield, D. (2013). Prolonged exposure vs supportive counseling for sexual abuse–related ptsd in adolescent girls: A randomized clinical trial. Journal of the American Medical Association, 310(24), 2650. https://doi.org/10.1001/jama.2013.282829.
Garza, R., Pazhoohi, F., Al-Shawaf, L., & Byrd-Craven, J. (2023). An eye tracking study examining the role of mating strategies, perceived vulnerability to disease, and disgust in attention to pathogenic cues. Adaptive Human Behavior and Physiology, 9(1), 72–87. https://doi.org/10.1007/s40750-023-00211-4
Godfrey, D. A., Bennett, V. E., & Babcock, J. C. (2021). Trait anger moderates the relation between facial affect recognition ability and perpetration of male-to-female physical and psychological intimate partner aggression. Journal of Family Violence, 36(3), 361–369. https://doi.org/10.1007/s10896-020-00162-4
Grauvogl, A., De Jong, P., Peters, M., Evers, S., Van Overveld, M., & Van Lankveld, J. (2015). Disgust and sexual arousal in young adult men and women. Archives of Sexual Behavior, 44(6), 1515–1525. https://doi.org/10.1007/s10508-014-0349-4.
Haberkamp, A., Glombiewski, J. A., Schmidt, F., & Barke, A. (2017). The disgust-related-images (dirti) database: Validation of a novel standardized set of disgust pictures. Behaviour Research and Therapy, 89, 86–94. https://doi.org/10.1016/j.brat.2016.11.010.
Hansen-Brown, A. A., & Jefferson, S. E. (2023). Perceptions of and stigma toward BDSM practitioners. Current Psychology, 42(23), 19721–19729. https://doi.org/10.1007/s12144-022-03112-z.
Heiman, J. R., & Rowland, D. L. (1983). Affective and physiological sexual response patterns: The effects of instructions on sexually functional and dysfunctional men. Journal of Psychosomatic Research, 27(2), 105–116. https://doi.org/10.1016/0022-3999(83)90086-7.
Hlavka, H. R. (2014). Normalizing sexual violence: Young women account for harassment and abuse. Gender & Society, 28(3), 337–358. https://doi.org/10.1177/0891243214526468
Holvoet, L., Huys, W., Coppens, V., Seeuws, J., Goethals, K., & Morrens, M. (2017). Fifty shades of Belgian gray: The prevalence of BDSM-related fantasies and activities in the general population. The Journal of Sexual Medicine, 14(9), 1152–1159. https://doi.org/10.1016/j.jsxm.2017.07.003
Kern, S. G., & Peterson, Z. D. (2020). From freewill to force: Examining types of coercion and psychological outcomes in unwanted sex. The Journal of Sex Research, 57(5), 570–584. https://doi.org/10.1080/00224499.2019.1671302.
Kilimnik, C. D., & Meston, C. M. (2019). Sexual violence identification and women’s sexual well-being. Current Sexual Health Reports, 11(1), 1–8. https://doi.org/10.1007/s11930-019-00186-y.
Kollareth, D., Shirai, M., Helmy, M., & Russell, J. A. (2022). Deconstructing disgust as the emotion of violations of body and soul. Emotion, 22(8), 1919–1928. https://doi.org/10.1037/emo0000886.
Kolmes, K., Stock, W., & Moser, C. (2006). Investigating bias in psychotherapy with BDSM clients. Journal of Homosexuality, 50(2–3), 301–324. https://doi.org/10.1300/J082v50n02_15
Krahé, B., Tomaszewska, P., & Schuster, I. (2021). Links of perceived pornography realism with sexual aggression via sexual scripts, sexual behavior, and acceptance of sexual coercion: A study with German university students. International Journal of Environmental Research and Public Health, 19(1), 63. https://doi.org/10.3390/ijerph19010063.
Kurdi, B., Lozano, S., & Banaji, M. R. (2017). Introducing the open affective standardized image set (oasis). Behavior Research Methods, 49(2), 457–470. https://doi.org/10.3758/s13428-016-0715-3.
Kyle, S. E. (2013). Identification and treatment of sexual shame: Development of a measurement tool and group therapy protocol. Dissertation Abstracts International, 1(83).
Lalumière, M. L., Sawatsky, M. L., Dawson, S. J., & Suschinsky, K. D. (2022). The empirical status of the preparation hypothesis: Explicating women’s genital responses to sexual stimuli in the laboratory. Archives of Sexual Behavior, 51(2), 709–728. https://doi.org/10.1007/s10508-019-01599-5.
Lewis, R., & Marston, C. (2016). Oral sex, young people, and gendered narratives of reciprocity. The Journal of Sex Research, 53(7), 776–787. https://doi.org/10.1080/00224499.2015.1117564.
Mathes, E. W., & McCoy, J. (2011). Perpetration of sexual coercion and victim of sexual coercion scales: Development and validation. Psychological Reports, 108(2), 449–469. https://doi.org/10.2466/08.09.16.PR0.108.2.449-469.
Meunier, S. A., & Tolin, D. F. (2009). The treatment of disgust. In B. O. Olatunji & D. McKay, Disgust and its disorders: Theory, assessment, and treatment implications (pp. 271–283). American Psychological Association. https://doi.org/10.1037/11856-013.
Miceli, M., & Castelfranchi, C. (2018). Contempt and disgust: The emotions of disrespect. Journal for the Theory of Social Behaviour, 48(2), 205–229. https://doi.org/10.1111/jtsb.12159.
Moser, C., & Kleinplatz, P. J. (2020). Conceptualization, history, and future of the paraphilias. Annual Review of Clinical Psychology, 16(1), 379–399. https://doi.org/10.1146/annurev-clinpsy-050718-095548.
Murray, D. R., Jones, D. N., & Schaller, M. (2013). Perceived threat of infectious disease and its implications for sexual attitudes. Personality and Individual Differences, 54(1), 103–108. https://doi.org/10.1016/j.paid.2012.08.021.
Norris, A. L., Carey, K. B., Shepardson, R. L., & Carey, M. P. (2021). Sexual revictimization in college women: Mediational analyses testing hypothesized mechanisms for sexual coercion and sexual assault. Journal of Interpersonal Violence, 36(13–14), 6440–6465. https://doi.org/10.1177/0886260518817778.
O’Shea, K. J., DeBruine, L. M., & Jones, B. C. (2019). Further evidence for associations between short-term mating strategy and sexual disgust. Personality and Individual Differences, 138, 333–335. https://doi.org/10.1016/j.paid.2018.10.019.
Olatunji, B. O., & Puncochar, B. D. (2016). Effects of disgust priming and disgust sensitivity on moral judgement: disgust and morality. International Journal of Psychology, 51(2), 102–108. https://doi.org/10.1002/ijop.12143
Olatunji, B. O., & Tomarken, A. (2023). Pavlovian disgust conditioning and generalization: Specificity and associations with individual differences. Behavior Therapy, 54(1), 1–13. https://doi.org/10.1016/j.beth.2022.06.008.
Olatunji, B. O., Adams, T., Ciesielski, B., David, B., Sarawgi, S., & Broman-Fulks, J. (2012). The three domains of disgust scale: Factor structure, psychometric properties, and conceptual limitations. Assessment, 19(2), 205–225. https://doi.org/10.1177/1073191111432881.
Palmer, R. S., McMahon, T. J., Rounsaville, B. J., & Ball, S. A. (2010). Coercive sexual experiences, protective behavioral strategies, alcohol expectancies and consumption among male and female college students. Journal of Interpersonal Violence, 25(9), 1563–1578. https://doi.org/10.1177/0886260509354581.
Pascal, S. A., Podina, I. R., & Nedelcea, C. (2020). A meta-analysis on the efficacy of exposure-based treatment in anxiety disorders: Implications for disgust. Journal of Evidence-Based Psychotherapies, 20(2), 31–49. https://doi.org/10.24193/jebp.2020.2.10.
Pawłowska, A., Borg, C., de Jong, P. J., & Both, S. (2020). The effect of differential disgust conditioning and subsequent extinction versus counterconditioning procedures on women’s sexual responses to erotic stimuli. Behaviour Research and Therapy, 134, 103714. https://doi.org/10.1016/j.brat.2020.103714.
Petersen, M. B. (2017). Healthy out-group members are represented psychologically as infected in-group members. Psychological Science, 28(12), 1857–1863. https://doi.org/10.1177/0956797617728270
Rozin, P., & Fallon, A. E. (1987). A perspective on disgust. Psychological Review, 94(1), 23–41. https://doi.org/10.1037/0033-295X.94.1.23.
Rozin, P., Haidt, J., & McCauley, C. R. (1999). Disgust: The body and soul emotion. In T. Dalgleish & M. J. Power (Eds.), Handbook of cognition and emotion (1st ed., pp. 429–445). Wiley. https://doi.org/10.1002/0470013494.ch21.
Ryan, G. L., Mengeling, M. A., Booth, B. M., Torner, J. C., Syrop, C. H., & Sadler, A. G. (2014). Voluntary and involuntary childlessness in female veterans: Associations with sexual assault. Fertility and Sterility, 102(2), 539–547. https://doi.org/10.1016/j.fertnstert.2014.04.042.
Schalk, T., Oliero, J., Fedele, E., Trousset, V., & Lefèvre, T. (2023). Evaluation of multidimensional functional impairment in adult sexual assault survivors, with a focus on its psychological, physical, and social dimensions, based on validated measurements: A prisma systematic review. International Journal of Environmental Research and Public Health, 20(14), 6373. https://doi.org/10.3390/ijerph20146373.
Schaller, M., & Murray, D. R. (2008). Pathogens, personality, and culture: Disease prevalence predicts worldwide variability in sociosexuality, extraversion, and openness to experience. Journal of Personality and Social Psychology, 95(1), 212–221. https://doi.org/10.1037/0022-3514.95.1.212.
Schwab Zabin, L., Emerson, M. R., & Rowland, D. L. (2005). Childhood sexual abuse and early menarche: The direction of their relationship and its implications. Journal of Adolescent Health, 36(5), 393–400. https://doi.org/10.1016/j.jadohealth.2004.07.013.
Simula, B. L. (2019). A different economy of bodies and pleasures? Differentiating and evaluating sex and sexual BDSM experiences. Journal of Homosexuality, 66(2), 209–237. https://doi.org/10.1080/00918369.2017.1398017.
Slavin, M. N., Scoglio, A. A. J., Blycker, G. R., Potenza, M. N., & Kraus, S. W. (2020). Child sexual abuse and compulsive sexual behavior: A systematic literature review. Current Addiction Reports, 7(1), 76–88. https://doi.org/10.1007/s40429-020-00298-9.
Suschinsky, K. D., & Lalumière, M. L. (2011). Prepared for anything? An investigation of female genital arousal in response to rape cues. Psychological Science, 22(2), 159–165. https://doi.org/10.1177/0956797610394660.
Toates, F., Smid, W., & Van Den Berg, J. W. (2017). A framework for understanding sexual violence: Incentive-motivation and hierarchical control. Aggression and Violent Behavior, 34, 238–253. https://doi.org/10.1016/j.avb.2017.01.001.
Tybur, J. M., Lieberman, D., & Griskevicius, V. (2009). Microbes, mating, and morality: Individual differences in three functional domains of disgust. Journal of Personality and Social Psychology, 97(1), 103–122. https://doi.org/10.1037/a0015474.
Tybur, J. M., Lieberman, D., Kurzban, R., & DeScioli, P. (2013). Disgust: Evolved function and structure. Psychological Review, 120(1), 65–84. https://doi.org/10.1037/a0030778.
Ullman, S. E., & Najdowski, C. J. (2009). Revictimization as a moderator of psychosocial risk factors for problem drinking in female sexual assault survivors. Journal of Studies on Alcohol and Drugs, 70(1), 41–49. https://doi.org/10.15288/jsad.2009.70.41.
Ullman, S. E., Townsend, S. M., Filipas, H. H., & Starzynski, L. L. (2007). Structural models of the relations of assault severity, social support, avoidance coping, self-blame, and PTSD among sexual assault survivors. Psychology of Women Quarterly, 31(1), 23–37. https://doi.org/10.1111/j.1471-6402.2007.00328.x
Van Leeuwen, F., Inbar, Y., Petersen, M. B., Aarøe, L., Barclay, P., Barlow, F. K., De Barra, M., Becker, D. V., Borovoi, L., Choi, J., Consedine, N. S., Conway, J. R., Conway, P., Adoric, V. C., Demirci, E., Fernández, A. M., Ferreira, D. C. S., Ishii, K., Jakšić, I., & Tybur, J. M. (2023). Disgust sensitivity relates to attitudes toward gay men and lesbian women across 31 nations. Group Processes & Intergroup Relations, 26(3), 629–651. https://doi.org/10.1177/13684302211067151.
Velten, J., Milani, S., Margraf, J., & Brotto, L. A. (2021). Visual attention to sexual stimuli in women with clinical, subclinical, and normal sexual functioning: An eye-tracking study. The Journal of Sexual Medicine, 18(1), 144–155. https://doi.org/10.1016/j.jsxm.2020.10.005.
Walsh, K., DiLillo, D., & Scalora, M. J. (2011). The cumulative impact of sexual revictimization on emotion regulation difficulties: An examination of female inmates. Violence against Women, 17(8), 1103–1118. https://doi.org/10.1177/1077801211414165.
Wang, J., Sun, X., Lu, J., Dou, H., & Lei, Y. (2021). Generalization gradients for fear and disgust in human associative learning. Scientific Reports, 11(1), 14210. https://doi.org/10.1038/s41598-021-93544-7.
Watkins, L. E., Sprang, K. R., & Rothbaum, B. O. (2018). Treating PTSD: A review of evidence-based psychotherapy interventions. Frontiers in Behavioral Neuroscience, 12, 258. https://doi.org/10.3389/fnbeh.2018.00258.
Weijters, B., Cabooter, E., & Schillewaert, N. (2010). The effect of rating scale format on response styles: The number of response categories and response category labels. International Journal of Research in Marketing, 27(3), 236–247. https://doi.org/10.1016/j.ijresmar.2010.02.004.
Wise, L. A., Palmer, J. R., Rothman, E. F., & Rosenberg, L. (2009). Childhood abuse and early menarche: Findings from the black women’s health study. American Journal of Public Health, 99(S2), S460–S466. https://doi.org/10.2105/AJPH.2008.149005.
Zsok, F., Fleischman, D. S., Borg, C., & Morrison, E. (2017). Disgust trumps lust: Women’s disgust and attraction towards men is unaffected by sexual arousal. Evolutionary Psychological Science, 3(4), 353–363. https://doi.org/10.1007/s40806-017-0106-8
Funding
The project was made possible by the Nebraska Tobacco Settlement Biomedical Research Development Funds. The authors were supported by funds from the National Institute of General Medical Sciences of the National Institutes of Health [P20GM130461] and the Rural Drug Addiction Research Center at the University of Nebraska—Lincoln. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the University of Nebraska.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Harper R. Jones. The first draft of the manuscript was written by Harper R. Jones and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Informed Consent and Ethics Approval
Informed consent was obtained from all individual participants included in the study as well as informed consent for research publication and inclusion in an anonymous dataset on the OSF data repository. This research protocol was approved by the University of Nebraska Institutional Review Board.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jones, H., Lorenz, T. Higher Sexual Avoidance, not Higher Pathogen Disgust, Is Associated with Lower Arousal in Women with a History of Unwanted Sex. Evolutionary Psychological Science (2024). https://doi.org/10.1007/s40806-024-00392-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40806-024-00392-5