
Abstract
Within the U.S., risky sexual behavior (RSB) is the primary mode of HIV transmission. The role of emotion dysregulation in RSB has received growing attention over the past decade. However, this literature has been limited in its focus on emotion dysregulation stemming from negative (but not positive) emotions. The goal of the current study was to extend research by examining the relative and unique contributions of dimensions of difficulties regulating positive emotions (i.e., nonacceptance of positive emotions [Accept], difficulties controlling impulsive behaviors when experiencing positive emotions [Impulse], and difficulties engaging in goal-directed behaviors when experiencing positive emotions [Goals]) to RSB. Participants were 386 trauma-exposed individuals recruited from Amazon’s MTurk (M age = 35.85 years; 57.5% female; 76.4% White). At the bivariate level, dimensions of difficulties regulating positive emotions were significantly positively associated with sexual risk taking with uncommitted partners, impulsive sex behaviors, and intent to engage in risky sexual behaviors (with the exception of Goals to sexual risk taking with uncommitted partners), and significantly negatively associated with risky sex acts. Regarding the unique contributions of difficulties regulating positive emotions to RSB, (1) Accept was significantly positively associated with impulsive sexual behaviors and intent to engage in risky sexual behaviors; (2) Impulse was significantly positively associated with risky anal sex acts; and (3) Goals was significantly negatively associated with risky anal sex acts. Findings suggest the potential utility of targeting difficulties regulating positive emotions in treatments aimed at reducing RSB.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Centers for Disease Control and Prevention (CDC, 2016) estimates that approximately 1.2 million people in the U.S. are living with HIV/AIDS. Prevention efforts have led to a notable reduction in the annual number of new HIV infections among some populations in the U.S. (e.g., people who inject drugs or identify as heterosexual). Yet, despite important advances, the annual number of new HIV infections remains stable from the mid-1990s to 2010, with approximately 38,000 people becoming newly infected each year (CDC, 2016). The considerable economic, societal, and personal costs associated with HIV/AIDS (Hellinger, 1998; Holtgrave & Pinkerton, 1997; Hutchinson, Branson, Kim, & Farnham, 2006) underscore the need for research in this area.
Within the U.S., risky sexual behavior (RSB) is the primary mode of HIV transmission (CDC, 2016). RSB refers to sexual behavior that increases the likelihood of HIV, other sexually transmitted infections (STIs), and/or unintended pregnancy, including the use of substances prior to or during sexual activity, sex with multiple partners, inconsistent condom use, and not engaging in safe sex communication (Turchick & Garske, 2009). An expansive body of research has sought to pinpoint factors that heighten risk for RSB, with the goal of informing prevention and intervention efforts aimed at reducing new HIV infections. One factor that has received growing attention in the past decade is emotion dysregulation. Emotion dysregulation is a multi-faceted construct involving maladaptive ways of responding to emotions, regardless of their intensity or reactivity, including (1) lack of emotional awareness, clarity and acceptance; (2) behavioral dyscontrol in the context of intense emotions; (3) unwillingness to experience emotional distress to pursue meaningful activities; and (4) inflexible use of adaptive strategies to modulate (versus eliminate) the intensity and/or duration of emotional experiences (Gratz & Roemer, 2004; Gratz & Tull, 2010). Theoretical evidence underscores the relevance of emotion dysregulation to RSB. Intense emotions have been shown to increase the likelihood of later RSB (Crepaz & Marks, 2001; Fortenberry, Temkit, Tu, Katz, & Orr, 2003; Lucenko, Malow, Sanchez-Martinez, Jennings, & Dévieux, 2003), suggesting that RSB may function to down-regulate emotions by alleviating or distracting attention away from such affective states. Alternatively, RSB may be associated with short-term pleasure that may serve to counter or distract from intense emotions (Briere & Elliott, 1994), consistent with positive reinforcement models of sexual risk taking (Cooper, Shapiro, & Powers, 1998). Finally, heightened levels of emotion dysregulation are theorized to interfere with the ability to control behaviors and increase the risk for maladaptive behavioral responses in general, including RSB (Linehan, 1993). Consistent with these theories, a growing number of investigations provide empirical support for the role of emotion dysregulation in RSB generally (Artime & Peterson, 2012; Messman-Moore, Walsh, & DiLillo, 2010) and above and beyond other relevant factors, including demographics, depression, sensation seeking, traumatic experiences, and substance use severity (Tull, Weiss, Adams, & Gratz, 2012).
Notably, however, research in this area has focused exclusively on the contribution of emotion dysregulation stemming from negative emotions to RSB. This is a critical limitation given recent evidence that individuals experience difficulties regulating positive emotions that parallel the difficulties observed in negative emotions (Cyders et al., 2007; Weiss, Gratz, & Lavender, 2015a; Weiss, Tull, Dixon-Gordon, & Gratz, 2018c). To aid the assessment of emotion dysregulation stemming from positive emotions, Weiss et al. (2015a) developed and validated the Difficulties in Emotion Regulation Scale-Positive (DERS-P) that maps onto the broader multiple facets of emotion dysregulation; specifically, this measure assesses nonacceptance of positive emotions (Accept), difficulties controlling impulsive behaviors when experiencing positive emotions (Impulse), and difficulties engaging in goal-directed behaviors in the context of positive emotions (Goals). Accept refers to the tendency to take an evaluative stance toward positive emotions, judging these emotion states to be undesirable, unpredictable, and/or frightening. One example item of Accept on the DERS-P is: “When I’m happy, I become scared and fearful of those feelings.” While seemingly counterintuitive, several explanations for this construct have been proposed in the literature. For instance, some theorists have suggested that individuals may experience negative affect interference, or negative emotion states in response to situations or stimuli that are typically positive (Frewen, Dean, & Lanius, 2012a; Frewen, Dozois, & Lanius, 2012b). Alternatively, Roemer, Litz, Orsillo, and Wagner (2001) theorized that, through stimulus generalization, fear of physiological arousal originally associated with negative emotional experiences may expand to positive emotions. Impulse refers to the tendency to engage in rash action in response to a very positive mood. One example item of Impulse on the DERS-P is: “When I’m happy, I have difficulty controlling my behaviors.” Research suggests that this dimension of difficulties regulating positive emotions reflects limited capacity for delay discounting and prepotent response inhibition in the context of positive emotions. For instance, when experiencing positive emotions, individuals tend to have a heightened focus on immediate needs, without considering long-term consequences (Cyders & Coskunpinar, 2012). Further, Billieux, Gay, Rochat, and Van der Linden (2010) found evidence of greater difficulties deliberately controlling or suppressing automatic responses in the context of positive emotions. Finally, Goals refers to the ability to continue present moment activities in the context of positive emotions. One example item of Accept on the DERS-P is: “When I’m happy, I have difficulty focusing on other things.” Persistence in goal-directed behaviors may be negatively impacted by positive emotional experiences through several cognitive mechanisms, including reduced cognitive flexibility (Price & Harmon-Jones, 2010), increased attentional narrowing (Gable & Harmon-Jones, 2008), and shortened time perception (Gable & Poole, 2012).
Preliminary studies provide support for the role of difficulties regulating positive emotions in other risky behaviors (i.e., alcohol and drug misuse; Weiss et al., 2018a; Weiss, Forkus, Contractor, & Schick, 2018b; Weiss, Risi, Bold, Sullivan, & Dixon-Gordon, in press). These findings suggest that difficulties regulating positive emotions may also inform our understanding of RSB. Indeed, research supports the role of positive urgency (a dimension of impulsivity that demonstrates conceptual overlap with Impulse; Cyders et al., 2007; Weiss et al., 2015a) in RSB (Birthrong & Latzman, 2014; Deckman & DeWall, 2011; Simons, Maisto, & Wray, 2010; Zapolski, Cyders, & Smith, 2009). Conversely, we are not aware of any investigations that have examined the relation of the other domains of difficulties regulating positive emotions—Accept and Goals—to RSB. Regarding the relation of Accept to RSB, individuals who take a judgmental and evaluative stance toward their positive emotions may be more likely to engage in attempts to suppress (e.g., reduce) positive emotional experiences (Beblo et al., 2012, 2013; Roemer et al., 2001), possibly through RSB. For instance, Cooper et al. (1998) found evidence that individuals may use sex to escape, avoid, or minimize emotions, and higher levels of this sex motive were associated with a greater number of lifetime partners and more lifetime risky sexual behaviors. Regarding the relation of Goals to RSB, the increased positive distractibility (Dreisbach & Goschke, 2004) and narrowed attention (Gable & Harmon-Jones, 2008) resulting from positive emotions may interfere with goal-directed behavior by shifting the focus from long- to short-term goals (Slovic, Finucane, Peters, & MacGregor, 2004). This, in turn, may heighten risk for RSB, consistent with evidence that a failure to reflect on the consequences of a behavior is associated with higher rates of RSB (Birthrong & Latzman, 2014).
Extending extant research, the goal of the current study was to examine the relative and unique contribution of difficulties regulating positive emotions to RSB among trauma-exposed individuals. Both emotion dysregulation and RSB are heightened among individuals with a history of traumatic exposure. Heightened levels of difficulties regulating negative emotions have been detected among trauma-exposed individuals (Ehring & Quack, 2010), and traumatic exposure has been shown to prospectively predict later difficulties regulating negative emotions (Bardeen, Kumpula, & Orcutt, 2013). Traumatic exposure may undermine the development of adaptive emotion regulation. For example, exposure to a traumatic event may overwhelm one’s regulatory capacities (Cloitre et al., 2009), making it difficult to modify emotional experiences (Flett, Blankstein, & Obertynski, 1996). Further, trauma-exposed individuals may come to rely on maladaptive strategies for regulating their emotions that reduce emotional distress in the short-term but have paradoxical effects in the long-term (Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). Additionally, trauma may interfere with the ability to identify and describe emotional states (Kooiman et al., 2004). While empirical work in this area has focused exclusively on difficulties regulating negative emotions, there is some indirect evidence to suggest that trauma-exposed individuals also exhibit difficulties regulating positive emotions. For instance, trauma-exposed individuals have been found to exhibit negative responses to positive emotional stimuli that may result in nonacceptance of positive emotions such as negative affect interference (Frewen et al., 2012a, 2012b). One explanation for this finding is that the physiological arousal that accompanies positive emotions may be experienced as distressing among trauma-exposed individuals, perhaps because of its association with trauma-related symptoms and distress (Taylor, Koch, & McNally, 1992). Finally, traumatic exposure has been found to have a well-established relation with RSB (Hillis, Anda, Felitti, & Marchbanks, 2001; Widom & Kuhns, 1996; Wilson & Widom, 2008). These above findings underscore the need for additional research on emotion dysregulation (and difficulties regulating positive emotions in particular) and RSB among trauma-exposed individuals.
Parallel to research on difficulties regulating negative emotions (Artime & Peterson, 2012; Messman-Moore et al., 2010; Tull et al., 2012), we hypothesized that difficulties regulating positive emotions would be significantly and positively related to RSB. Given the dearth of research in this area, no a priori hypotheses were made regarding the unique associations among dimensions of difficulties regulating positive emotions and RSB.
Method
Participants and Procedure
Data for the present study were collected as part of a larger study developing a novel measure assessing risky behaviors among individuals with stressful life experiences. Participants were recruited from Amazon’s Mechanical Turk (MTurk) platform. Beyond generating reliable data (Buhrmester, Kwang, & Gosling, 2011; Shapiro, Chandler, & Mueller, 2013), MTurk’s subject pool is diverse (Buhrmester et al., 2011) and represents the general population in terms of demographics (Mischra & Carleton, 2017) and prevalence of mental health problems (Shapiro et al., 2013). Relevant to the current study, research indicates similar prevalence rates of PTSD in the MTurk sample compared to epidemiological studies, and higher PTSD severity compared to a college sample (van Stolk-Cooke et al., 2018). MTurk may be able to capture individuals with greater PTSD severity in a cost-effective manner and within a reasonable amount of time (Shapiro et al., 2013; van Stolk-Cooke et al., 2018). To improve data quality, we embedded validity checks in the MTurk survey assessing attentive responding and comprehension (Aust, Diedenhofen, Ullrich & Musch, 2013; Meade & Craig, 2012; Oppenheimer, Meyvis, & Davidenko, 2009; Thomas & Clifford, 2017).
Participants 18 years of age and older were screened for the larger study based upon three inclusionary criteria: living in North America; working knowledge of the English language; and experience of a traumatic event screened with the Criterion A question of the Primary Care PTSD Screen for DSM-5 (Prins et al., 2016). Participants who met eligibility criteria provided informed consent and completed the survey on Qualtrics (data collection platform). Participants were compensated $1.25 for study participation. All procedures were approved by the Institutional Review Board at a U.S. university.
Of the obtained 891 responses, duplicate responses were excluded of 18 participants who attempted to answer the questionnaire more than once (47 responses; remainder n = 844). We then excluded 150 participants not meeting one or more inclusionary criteria (remainder n = 694), 122 participants who failed to pass any of four validity checks (approximately 14% of the original sample; remainder n = 572), and 97 participants for missing data on all measures (approximately 11% of the original sample; remainder n = 475). The decrease in sample size attributed to failing validity checks parallels other studies using similar methodology (e.g., 17% of respondents; van Stolk-Cooke et al., 2018). Further, using data obtained from the Life Event Checklist for DSM-5 (Weathers et al., 2013), we excluded 11 participants who either did not endorse a traumatic event, or did not identify their distressing traumatic event (remainder n = 464). Finally, we excluded 78 participants missing more than 30% item-level data on any primary variable of interest (see Measures). The final sample included 386 participants. Average age of participants was 35.85 years (SD = 11.18), and approximately 222 were female (57.50%). Additional information on demographics is indicated in Table 1.
Measures
Primary Care PTSD Screen for DSM-5 (PC-PTSD-5; Prins et al., 2016)
PC-PTSD-5 is a self-report measure that screens for the presence of a history of Criterion A traumatic exposure as well as posttraumatic stress disorder symptoms. The current study utilized the traumatic event item, which asks about the experience of six different types of traumatic events: a serious accident or fire, a physical or sexual assault or abuse, an earthquake or flood, a war, seeing someone be killed or seriously injured, and having a loved one die through homicide or suicide. Participants indicate whether they experienced any of these events (yes/no). The PC-PTSD-5 has been found to have good psychometric properties.
Difficulties in Emotion Regulation Scale-Positive (DERS-P; Weiss et al., 2015a)
The DERS-P is a 13-item self-report measure that assesses difficulties regulating positive emotions on three subscales: Accept, Impulse, and Goals. Higher scores indicate greater difficulties regulating positive emotions. Participants rate each item using a 5-point Likert-type scale (1 = almost never, 5 = almost always). The subscales of the DERS-P have good psychometric properties. Cronbach’s αs in the current sample were .93, .94, and .87 for the DERS-P Accept, DERS-P Impulse, and DERS-P Goals, respectively.
Difficulties in Emotion Regulation Scale-16 (DERS; Bjureberg et al., 2016)
The DERS-16 is a 16-item self-report measure modified from the original 36-item DERS (Gratz & Roemer, 2004). The DERS-16 assesses individuals’ typical levels of emotion dysregulation across five domains: nonacceptance of negative emotions, difficulties engaging in goal-directed behaviors when experiencing negative emotions, difficulties controlling impulsive behaviors when experiencing negative emotions, limited access to emotion regulation strategies perceived as effective, and lack of emotional clarity. Participants rate each item using a 5-point Likert-type scale (1 = almost never, 5 = almost always). For the current study, the three DERS domains that correspond with the DERS-P were included (i.e., nonacceptance of negative emotions, difficulties engaging in goal-directed behaviors when experiencing negative emotions, difficulties controlling impulsive behaviors when experiencing negative emotions). A total score was calculated by summing the 9 DERS items on these three domains. Higher scores indicate greater difficulties regulating negative emotions. Cronbach’s α for the difficulties regulating negative emotions total score was .94.
Sexual Risk Survey (SRS; Turchik & Garske, 2009)
The SRS is a 23-item self-report measure to assess RSB in the past 6 months. The SRS contains five subscales, including: sexual risk taking with uncommitted partners (e.g., sex with someone don’t know well, sex with partner didn’t trust), risky sex acts (e.g., vaginal sex without a condom, sex under the influence of substances), impulsive sexual behaviors (e.g., number of sexual behavior partners, unexpected sexual experience), intent to engage in risky sexual behaviors (e.g., intent of engaging in sex), and risky anal sex acts (e.g., unprotected anal penetration). Participants are asked to indicate how many times they have engaged in each of the behaviors in the past 6 months, and frequencies are then recoded into five ordinal categories (for a full description of this scoring procedure, see Turchik & Garske, 2009; Turchik, Walsh, & Marcus, 2015). Codes of “0” only included frequencies of 0. The remaining frequencies were recoded as if they represented 100% of the frequencies. Specifically, since scores on the SRS are negatively skewed, frequencies that were greater than 0 were coded as: 1 = approximately 40% of responses, 2 = approximately 30% of responses, 3 = approximately 20% of responses, and 4 = approximately 10% of responses. Higher scores indicate greater RSB. The subscales of the SRS have demonstrated good internal consistency, test–retest reliability, and validity (i.e., demonstrated relations with health consequences due to sexual risk taking such as pregnancy and STIs, including HIV/AIDS). In the current study, sexual risk taking with uncommitted partners (α = .89), risky sex acts (α = .83), impulsive sexual behaviors (α = .86), intent to engage in risky sexual behaviors (α = .79), and risky anal sex acts (α = .77) all demonstrated good internal consistency.
Demographic Information
Information regarding age, gender, ethnicity, race, income, educational level, employment status, ethnicity, and relationship status was obtained.
Data Analysis
Descriptive information and Pearson correlations were calculated to examine correlations among the primary study variables. Path analysis was then used to evaluate the relation between overall difficulties regulating positive emotions and each RSB domain (i.e., sexual risk taking with uncommitted partners, risky sex acts, impulsive sexual behaviors, intent to engage in risky sexual behaviors, and risky anal sex acts). Next, analyses were conducted to identify relevant covariates. Specifically, we explored the relations among demographic and relationship characteristics known to be associated with RSB, including relationship status (Brown & Vanable, 2007; Dodge, Reece, Cole, & Sandfort, 2004), gender (Byrnes, Miller, & Schafer, 1999; Poppen 1995), and age (Mata, Josef, Samanez-Larkin, & Hertwig, 2011), and RSB domains. We also examined the associations among difficulties regulating negative emotions (total score) as a covariate given its association with RSB (Tull et al., 2012). The path model was then re-run with the inclusion of these relevant covariates. This was done to examine whether the paths remained significant with and without the inclusion of relevant covariates. Finally, a supplemental analysis was conducted to evaluate the unique relation between each dimension of difficulties regulating positive emotions (i.e., Accept, Impulse, and Goals) with each RSB domain. Similar to the primary analyses, this analysis was conducted with and without the inclusion of relevant covariates (i.e., relationship status, gender, age, and difficulties regulating negative emotions).
Analyses were conducted using the EQS 6.3 statistical package (Bentler, 2006), which uses the maximum likelihood (ML) method of estimation to obtain maximum likelihood parameter estimates, and provide goodness-of-fit indices. The adequacy of the model was evaluated by examining several fit indices: the root-mean-square error of approximation (RMSEA; Steiger, 1990), the standardized root-mean-square residual (SRMR; Hu & Bentler, 1999), and the comparative fit index (CFI; Bentler, 1990). The RMSEA assessed closeness of fit with preferred values < 0.10 (Browne & Cudeck, 1993). The SRMR is the standardized difference between the observed correlation and the predicted correlation with a value < 0.08 generally considered good fit (Hu & Bentler, 1999). The CFI, an incremental fit index, assessed fit relative to a null model with values > 0.95 indicating good fit. Standardized regression coefficients (β) were evaluated to determine the strength and direction of the relations among the independent and dependent variables while controlling for all other variables in the model (and possibly any significant covariates). The absolute values of these βs were examined comparatively to other regression coefficients in model, with larger values indicating stronger relations. Significant regression paths indicated unique associations between dimensions of difficulties regulating positive emotions with each RSB domain, while simultaneously controlling for the other dimensions of difficulties regulating positive emotions in the model.
Results
Descriptive information and Pearson correlations for the primary study variables are presented in Table 2. Accept, Impulse, and Goals were significantly positively associated with impulsive sexual behaviors and intent to engage in risky sexual behaviors. Accept and Impulse were significantly positively associated with sexual risk taking with uncommitted partners. Accept, Impulse, and Goals were significantly negatively associated with risky sex acts.
We first tested a fully saturated model with all paths being freely estimated between difficulties regulating positive emotions and RSB domains. Fit indices are not reported because the conceptual model is fully saturated and therefore perfectly fits the data. In this model, difficulties regulating positive emotions were significantly positively associated with sexual risk taking with uncommitted partners (b = .05, SE = .02, β =.12, 95% CI [.08, .16]; p =.02), impulsive sexual behaviors (b = .08, SE = .02, β =.27, 95% CI [.23, .31]; p < .001), and intent to engage in risky sexual behavior (b = .02, SE = .004, β =.25, 95% CI [.24, .26]; p < .001), and significantly negatively associated with risky sex acts (b = − .09, SE = .03, β =− .18, 95% CI [− .24, − .12]; p < .001).
To test the sensitivity of this proposed model, we re-ran the analysis adjusting for relevant covariates. We first identified relevant covariates by examining the associations among RSB facets and demographic (i.e., age and gender), relationship (i.e., relationship status) factors and difficulties regulating negative emotions. At the bivariate level, gender was found to be significantly associated with sexual risk taking with uncommitted partners (r = − .14, p = .01), impulsive sexual behaviors (r = − .12, p = .02), and intent to engage in risky sexual behaviors (r = − .16, p < .001). Age was found to be associated with impulsive sexual behaviors (r = − .17, p = .001), intent to engage in risky sexual behaviors (r = − .14, p = .01), and risky anal sex acts (r = − .11, p = .03). Relationship status was found to be associated with risky sex acts (r = .17, p = .01), impulsive sexual behaviors (r = − .14, p = .01), and intent to engage in risky sexual behaviors (r = − .14, p = .01). Difficulties regulating negative emotions were found to be associated with impulsive sexual behaviors (r = .15, p = .004) and intent to engage in risky sexual behaviors (r = .11, p = .03).
Next, we re-ran the analysis adjusting for these covariates to see if the associations remained (see Fig. 1). This model demonstrated acceptable fit to the data: χ2 (16, n = 361) = 156.93, p < .0001; CFI = .83, RMSEA = .16, 90% CI [.13, .18], SRMR = 0.09. In this model, the same paths remained significant, including difficulties regulating positive emotions to sexual risk taking with uncommitted partners (b = .04, SE = .02, β =.10, 95% CI [.06, .14]; p =.05), impulsive sexual behaviors (b = .07, SE = .02, β =.23, 95% CI [.19, .27]; p < .001), intent to engage in risky sexual behavior (b = .02, SE = .004, β =.21, 95% CI [.20, .22]; p < .001), and risky sex acts (b = − .10, SE = .03, β =− .19, 95% CI [− .25, − .13]; p < .001). See Table 3 for a summary of test statistics.

Final model of overall difficulties regulating positive emotions and risky sexual behaviors. Note Standardized regression coefficients are displayed in figure. Solid lines = significant relations. All possible paths from the predictors to the outcome variables were included in the analysis. Gender, age, relationship status, and difficulties regulating negative emotions were included as covariates in this model. See Table 3 for a summary of test statistics. *p <.05. **p < .001
Supplemental Analyses
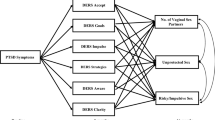
In the supplemental analyses, we examined the unique relations between each dimension of difficulties regulating positive emotions and RSB domains. As was done with the primary analyses, we first tested a fully saturated model with all paths being freely estimated between the dimensions of difficulties regulating positive emotions and RSB domains. Fit indices are not reported because the conceptual model is fully saturated and therefore perfectly fits the data. In this model, Accept was significantly positively associated with impulsive sexual behaviors (b = 23, SE = .11, β =.25, 95% CI [.03, .47]; p =.029) and intent to engage in risky sexual behaviors (b = .06, SE = .03, β =.25, 95% CI [.19, .31]; p =.028). Impulse was significantly positively associated with risky anal sex acts (b = .14, SE = .07, β =.27, 95% CI [.13, .41]; p =.043). Goals was significantly negatively associated with risky anal sex acts (b = − .12, SE = .06, β =− .19, 95% CI [− .31, − .07]; p =.037).
To test the sensitivity of this proposed model, we adjusted for relevant covariates (i.e., gender, age, relationship status, and difficulties regulating negative emotions). Next, we re-ran the analysis adjusting for these covariates to see if the associations remained. This model demonstrated acceptable fit to the data: χ2 (24, n = 362) = 173.06, p < .0001; CFI = .92, RMSEA = .13, 90% CI [.11, .15], SRMR = 0.11 (see Fig. 2). In this model, with the exception of Impulse to risky anal sex acts (b = .13, SE = .07, β =.25, 95% CI [.11, .39]; p =.059), all other paths remained significant, including Accept to impulsive sexual behaviors (b = .21, SE = .11, β =.23, 95% CI [.01, .45]; p =.046), Accept to intent to engage in risky sexual behaviors (b = .06, SE = .03, β =.25, 95% CI [.19, .31]; p =.028), and Goals to risky anal sex acts (b = − .12, SE = .06, β =− .19, 95% CI [− .31, − .07]; p =.035). See Table 3 for a summary of test statistics.

Final model of dimensions of difficulties regulating positive emotions and risky sexual behaviors. Standardized regression coefficients are displayed in figure. Solid lines = significant relations. All possible paths from the predictors to the outcome variables were included in the analysis. See Table 2 for a summary of test statistics. *p <.05
Discussion
RSB is the primary mode of HIV transmission in the U.S. (CDC, 2016); therefore, it is critical to increase our understanding of potential risk vulnerability factors for engaging in RSB. The goal of the current study was to extend existing research by examining the relative and unique contributions of difficulties regulating positive emotions to RSB among trauma-exposed individuals. At the bivariate level, and consistent with expectations, each of the dimensions of difficulties regulating positive emotions was significantly positively associated with sexual risk taking with uncommitted partners, impulsive sex behaviors, and intent to engage in risky sexual behaviors, with the exception of the path representing the relation of Goals to sexual risk taking with uncommitted partners, which was non-significant. Inconsistent with study hypotheses, each of the dimensions of difficulties regulating positive emotions was significantly negatively associated with risky sex acts and non-significantly associated with risky anal sex acts at the bivariate level. In a path model, overall difficulties regulating positive emotions were found to be significantly positively associated with sexual risk taking with uncommitted partners, impulsive sexual behaviors, and intent to engage in risky sexual behavior, and significantly negatively associated with risky sex acts. Regarding the relation of the specific dimensions of difficulties regulating positive emotions to RSB, (1) nonacceptance was significantly positively associated with impulsive sexual behaviors and intent to engage in risky sexual behaviors; (2) Impulse was significantly positively associated with risky anal sex acts; and (3) Goals was significantly negatively associated with risky anal sex acts. These above findings expand our understanding of the relation of emotion dysregulation to RSB, highlighting the role of dimensions of difficulties regulating positive emotions in specific RSB outcomes among trauma-exposed individuals.
Research on per-act HIV transmission risk has found anal intercourse (receptive, in particular) to be associated with the highest risk of HIV acquisition from sexual exposure, with an estimate of transmission risk for receptive anal intercourse of 138 per 10,000 exposures (compared to 8 per 10,000 exposures for receptive vaginal intercourse; Patel et al., 2014). As such, investigations that identify factors that may modify risk for risky anal sex acts are critical to informing efficacious prevention and intervention efforts aimed at reducing HIV transmission. The results of the current study provide support for the unique contributions of two dimensions of difficulties regulating positive emotions—Impulse and Goals—to risky anal sex acts. Specifically, we found that individuals who reported greater difficulties controlling impulsive behaviors in the context of positive emotions reported more engagement in risky anal sex acts. Indeed, behavioral dyscontrol in the context of positive emotions has been linked to risky anal sex acts (Birthrong & Latzman, 2014; Dudley, Rostosky, Korfhage, & Zimmerman, 2004). For instance, Birthrong and Latzman examined the relations among positive urgency and RSB (as assessed by the SRS); findings provided support for the unique role of positive urgency in risky anal sex acts, above and beyond demographics, relationship status, and other impulsivity dimensions.
Counter to study hypotheses, risky anal sex acts were more likely among individuals who reported fewer difficulties continuing goal-directed behavior in the context of positive emotions. Although not generally associated with longer-term goals or values (e.g., safe sex), it is possible that risky anal sex acts conferred some immediate (short-term) benefits for participants in our sample. For example, it has been proposed that unprotected anal sex may be “rational” if the benefits (e.g., pleasure, intimacy) outweigh the perceived threat of HIV transmission; this perceived risk may vary as a function of partner characteristics (e.g., drug use, promiscuity), biology (e.g., viral load), sexual practices (e.g., withdrawal, insertive anal intercourse; use of spermicides; Pinkerton & Abramson, 1992). Alternatively, the rationality of anal sex practices may be less relevant than other health behaviors given that the desire for sex is an innate human drive. Future research is needed to better understand the perceived benefits and consequences of risky anal sex acts and their relation to known predictors, correlates, and outcomes of risky anal sex acts.
Finally, higher levels of nonacceptance of positive emotions were associated with greater engagement in impulsive sexual behaviors and intent to engage in risky sexual behaviors. While seemingly counterintuitive, there is growing evidence that individuals may take an evaluative and judgmental stance toward positive emotions (Weiss et al., 2015a). Theory and empirical work links nonacceptance of emotions more generally to maladaptive behaviors (Chapman, Gratz, & Brown, 2006; Weiss et al., 2015c; Weiss, Williams, & Connolly, 2015e). More recent work underscores a link between nonacceptance of positive emotions in particular and risky behavior, specifically alcohol and drug misuse (Weiss et al., 2018a, b, in press). Our current findings extend this work by indicating that nonacceptance of positive emotions also contributes to specific domains of RSB. Given evidence to suggest that positive emotions may be experienced as aversive (e.g., due to stimulus generalization [Roemer et al., 2001] and negative affect interference [Frewen et al., 2012a]), it is possible that individuals may engage in impulsive sexual behaviors or intend to engage in risky sexual behaviors to reduce distress stemming from positive emotions. Indeed, meta-analytic findings suggest that aversive emotions are associated with increased risk for RSB (Crepaz & Marks, 2001), and a functional relation between aversive emotions and RSB has been demonstrated, such that more aversive emotions predict engagement in RSB (Fortenberry et al., 2003; Lucenko et al., 2003) and engagement in RSB predicts fewer aversive emotions (Orcutt, Cooper, & Garcia, 2005). Future research is needed to test this hypothesis.
Notably, it warrants mention that each of the dimensions of difficulties regulating positive emotions was significantly negatively related to risky sex acts at the bivariate level. Risky sex acts include four items assessing unprotected (e.g., condomless, without birth control) vaginal and oral sex as well as one item assessing sex under the influence of substances. Our results suggest that these behaviors may have been premediated (i.e., not impulsive) and congruent with participants’ short-term objectives (i.e., goal-directed). Several theoretical models (Albarracin, Johnson, Fishbein, & Muellerleile, 2001; Morrison, Gillmore, & Baker, 1995; Rosenstock, Strecher, & Becker, 1994; Van der Velde & Van der Pligt, 1991) have applied a decision-making framework to unprotected sex, finding that individuals are less likely to use protection if the advantages (e.g., reduced risk for sexually transmitted infections) do not outweigh the downsides (e.g., reduced satisfaction, discomfort). In support of these theories, Gebhardt, Kuyper, and Greunsven (2003) found that individuals were more likely to engage in unprotected sex if it facilitated intimacy, and Cooper et al. (1998) found that individuals may engage in unprotected sex to gain approval from peers and partners. More nuanced investigations are needed to better understand the function risky sex acts may serve and their relation to emotion dysregulation.
Finally, it is worth mentioning that there were differences in some of the bivariate versus path analysis findings. For instance, although each of the DERS-P dimensions was significantly negatively related to risky sex acts at the bivariate level, Impulse was significantly positively related to this RSB facet in the path analysis. A statistical reason for this discrepancy relates to the goals of the analyses. Bivariate analyses reference a relation between each DERS-P dimension (e.g., Accept) with an RSB facet (e.g., risky sex). In contrast, the path analysis references relations between each DERS-P dimension (e.g., Accept) with an RSB facet (e.g., risky sex) accounting for the influence of the other DERS-P dimensions (e.g., Impulse and Goals). Path analysis is used to explore the unique role of the dimensions of difficulties regulating positive emotions in RSB outcomes. Based on these statistical computation differences, unsurprisingly, many of the significant bivariate findings were non-significant in the path model. In many cases, particular dimensions of difficulties regulating positive emotions may have exerted a stronger unique influence on specific RSB facets.
Results should be considered in the context of study limitations. First, the cross-sectional and correlational nature of the data precludes causal determination of the relations examined. Future research is needed to investigate the nature and direction of these relations through prospective, longitudinal investigations. Second, this study relied exclusively on self-report measures, which may be influenced by one’s willingness and/or ability to report accurately. Future investigations should include objective (e.g., behavioral, physiological) measures of emotion dysregulation (Gratz, Rosenthal, Tull, Lejuez, & Gunderson, 2006; Thayer & Lane, 2000; Vasilev, Crowell, Beauchaine, Mead, & Gatzke-Kopp, 2009). Third, while we controlled for relationship status in our analyses, we do not have additional data on partner characteristics (e.g., whether participants were in a mutually monogamous relationship with an HIV uninfected or virally suppressed partner) or PrEP use, which may be associated with a lower risk for HIV following sexual behavior assessed here. Fourth, the trauma measure utilized here does not assess one’s experience with specific traumatic events (e.g., sexual trauma). Future studies would benefit from a more comprehensive evaluation of trauma. Fifth, while the MTurk recruitment platform is a notable strength of our study (e.g., given its diversity, representativeness, and reliability; Buhrmester et al., 2011; Mischra & Carleton, 2017; Shapiro et al., 2013), collecting data via the internet using an online format has disadvantages that may limit generalizability of results, such as sample biases (because of self-selection) and lack of control over the research environment (e.g., no opportunity to clarify questions; distractions; Kraut et al., 2004). Thus, future research that integrates other data collection methods (e.g., interviewing, focus groups) is warranted. While using attention checks and limiting the sample to individuals not missing too much data improves MTurk data quality (Aust et al., 2013; Buhrmester et al., 2011; Oppenheimer et al., 2009), it also creates a selection bias. To counter such selection bias, restricting participation to MTurk workers with high reputation (> 95% approval ratings) is recommended as a quality control measure compared to using validity checks (Peer, Vosgerau, & Acquisti 2014). Finally, while examination of the relations among difficulties regulating positive emotions and RSB in a sample of trauma-exposed individuals is a strength of the current study, our findings cannot be assumed to generalize to non-trauma-exposed populations and require replication across more diverse samples of trauma-exposed individuals (e.g., treatment-seeking).
Despite study limitations, results of the current study add to the literature on emotion dysregulation, providing support for the role of difficulties regulating positive emotions in RSB among trauma-exposed individuals. These findings extend theory, research, and practice in meaningful ways. Existing theoretical accounts and related research have almost exclusively focused on the influence of emotion dysregulation stemming from negative (but not positive) emotions in maladaptive behaviors, including RSB (Weiss, Sullivan, & Tull, 2015b; Weiss, Tull, & Sullivan, 2015d). Current conceptualizations that include a focus on positive emotions emphasize their role in facilitating adaptive action (Fredrickson, 2002), neglecting the possible deleterious outcomes of positive emotions (Gruber & Moskowitz, 2014). Our findings suggest the need for further refinement of existing theoretical accounts to more comprehensively account for the role of positive emotional experiences (both positive and negative) in RSB. Moreover, if replicated, results of the current study may be used to inform clinical practice. For instance, our findings suggest the potential utility of assessing difficulties regulating positive emotions among populations at risk for (e.g., individuals with posttraumatic stress disorder; Weiss, Tull, Borne, & Gratz, 2013) or identified by (e.g., individuals attending a sexually transmitted infection clinic) RSB. Further, results of our study highlight potential targets for interventions aimed at preventing or reducing RSB among trauma-exposed individuals. For instance, pending replication, potential treatment aims include teaching skills to decrease judgmental and nonaccepting responses to positive emotions, facilitating behavioral control in the context of positive emotional states, and promoting value-based acting when experiencing positive emotions. Future research in this area is needed to explore whether interventions that target difficulties regulating positive emotions reduce RSB among trauma-exposed individuals.
References
Albarracin, D., Johnson, B. T., Fishbein, M., & Muellerleile, P. A. (2001). Theories of reasoned action and planned behavior as models of condom use: A meta-analysis. Psychological Bulletin, 127, 142–161.
Artime, T. M., & Peterson, Z. D. (2012). The relationships among childhood maltreatment, emotion regulation, and sexual risk taking in men from urban STD clinics. Journal of Aggression, Maltreatreatment, and Trauma, 21, 277–299.
Aust, F., Diedenhofen, B., Ullrich, S., & Musch, J. (2013). Seriousness checks are useful to improve data validity in online research. Behavior Research Methods, 45, 527–535.
Bardeen, J. R., Kumpula, M. J., & Orcutt, H. K. (2013). Emotion regulation difficulties as a prospective predictor of posttraumatic stress symptoms following a mass shooting. Journal of Anxiety Disorders, 27, 188–196.
Beblo, T., Fernando, S., Kamper, P., Griepenstroh, J., Aschenbrenner, S., Pastuszak, A., … Driessen, M. (2013). Increased attempts to suppress negative and positive emotions in borderline personality disorder. Psychiatry Research, 210, 505–509.
Beblo, T., Fernando, S., Klocke, S., Griepenstroh, J., Aschenbrenner, S., & Driessen, M. (2012). Increased suppression of negative and positive emotions in major depression. Journal of Affective Disorders, 141, 474–479.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246.
Bentler, P. M. (2006). EQS 6 structural equations program manual. Encino, CA: Multivariate Software Inc.
Billieux, J., Gay, P., Rochat, L., & Van der Linden, M. (2010). The role of urgency and its underlying psychological mechanisms in problematic behaviours. Behaviour Research and Therapy, 48, 1085–1096.
Birthrong, A., & Latzman, R. D. (2014). Aspects of impulsivity are differentially associated with risky sexual behaviors. Personality and Individual Differences, 57, 8–13.
Bjureberg, J., Ljótsson, B., Tull, M. T., Hedman, E., Sahlin, H., Lundh, L. G., … Gratz, K. L. (2016). Development and validation of a brief version of the Difficulties in Emotion Regulation scale: The DERS-16. Journal of Psychopathology and Behavioral Assessment, 38, 284–296.
Briere, J. N., & Elliott, D. M. (1994). Immediate and long-term impacts of child sexual abuse. Future of Children, 4, 54–69.
Brown, J. L., & Vanable, P. A. (2007). Alcohol use, partner type, and risky sexual behavior among college students: Findings from an event-level study. Addictive Behaviors, 32, 2940–2952.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Newbury Park, CA: Sage.
Buhrmester, M., Kwang, T., & Gosling, S. D. (2011). Amazon’s Mechanical Turk a new source of inexpensive, yet high-quality, data? Perspectives on Psychological Science, 6, 3–5.
Byrnes, J. P., Miller, D. C., & Schafer, W. D. (1999). Gender differences in risk taking: A meta-analysis. Psychological Bulletin, 125, 367–383.
Centers for Disease Control. (2016). CDC fact sheet: Today’s HIV/AIDS epidemic. Retrieved May 22, 2018 from https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/todaysepidemic-508.pdf.
Chapman, A. L., Gratz, K. L., & Brown, M. Z. (2006). Solving the puzzle of deliberate self-harm: The experiential avoidance model. Behaviour Research and Therapy, 44, 371–394.
Cloitre, M., Stolbach, B. C., Herman, J. L., Kolk, B. V. D., Pynoos, R., Wang, J., & Petkova, E. (2009). A developmental approach to complex PTSD: Childhood and adult cumulative trauma as predictors of symptom complexity. Journal of Traumatic Stress, 22, 399–408.
Cooper, M. L., Shapiro, C. M., & Powers, A. M. (1998). Motivations for sex and risky sexual behavior among adolescents and young adults: A functional perspective. Journal of Personality and Social Psychology, 75, 1528–1558.
Crepaz, N., & Marks, G. (2001). Are negative affective states associated with HIV sexual risk behaviors? A meta-analytic review. Health Psychology, 20, 291–299.
Cyders, M. A., & Coskunpinar, A. (2012). The relationship between self-report and lab task conceptualizations of impulsivity. Journal of Research in Personality, 46, 121–124.
Cyders, M. A., Smith, G. T., Spillane, N. S., Fischer, S., Annus, A. M., & Peterson, C. (2007). Integration of impulsivity and positive mood to predict risky behavior: Development and validation of a measure of positive urgency. Psychological Assessment, 19, 107–118.
Deckman, T., & DeWall, C. N. (2011). Negative urgency and risky sexual behaviors: A clarification of the relationship between impulsivity and risky sexual behavior. Personality and Individual Differences, 51, 674–678.
Dodge, B., Reece, M., Cole, S. L., & Sandfort, T. G. (2004). Sexual compulsivity among heterosexual college students. Journal of Sex Research, 41, 343–350.
Dreisbach, G., & Goschke, T. (2004). How positive affect modulates cognitive control: Reduced perseveration at the cost of increased distractibility. Journal of Experimental Psychology. Learning, Memory, and Cognition, 30, 343–353.
Dudley, M. G., Rostosky, S. S., Korfhage, B. A., & Zimmerman, R. S. (2004). Correlates of high-risk sexual behavior among young men who have sex with men. AIDS Education and Prevention, 16, 328–340.
Ehring, T., & Quack, D. (2010). Emotion regulation difficulties in trauma survivors: The role of trauma type and PTSD symptom severity. Behavior Therapy, 41, 587–598.
Flett, G. L., Blankstein, K. R., & Obertynski, M. (1996). Affect intensity, coping styles, mood regulation expectancies, and depressive symptoms. Personality and Individual Differences, 20, 221–228.
Fortenberry, J. D., Temkit, M. H., Tu, W., Katz, B. P., & Orr, D. P. (2003). Mood, mood change, sexual activity and condom use among adolescent women. Journal of Adolescent Health, 32, 157.
Fredrickson, B. L. (2002). Positive emotions. In C. R. Snyder & S. J. Lopez (Eds.), Handbook of positive psychology (pp. 120–134). New York: Oxford University Press.
Frewen, P. A., Dean, J. A., & Lanius, R. A. (2012a). Assessment of anhedonia in psychological trauma: Development of the Hedonic Deficit and Interference Scale. European Journal of Psychotraumatology, 3, 8585.
Frewen, P. A., Dozois, D. J., & Lanius, R. A. (2012b). Assessment of anhedonia in psychological trauma: Psychometric and neuroimaging perspectives. European Journal of Psychotraumatology, 3, 8587.
Gable, P. A., & Harmon-Jones, E. (2008). Approach-motivated positive affect reduces breadth of attention. Psychological Science, 19, 476–482.
Gable, P. A., & Poole, B. D. (2012). Time flies when you’re having approach-motivated fun: Effects of motivational intensity on time perception. Psychological Science, 23, 879–886.
Gebhardt, W. A., Kuyper, L., & Greunsven, G. (2003). Need for intimacy in relationships and motives for sex as determinants of adolescent condom use. Journal of Adolescent Health, 33, 154–164.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation scale. Journal of Psychopathology and Behavioral Assessment, 26, 41–54.
Gratz, K. L., Rosenthal, M. Z., Tull, M. T., Lejuez, C. W., & Gunderson, J. G. (2006). An experimental investigation of emotion dysregulation in borderline personality disorder. Journal of Abnormal Psychology, 115, 850–855.
Gratz, K. L., & Tull, M. T. (2010). Emotion regulation as a mechanism of change in acceptance-and mindfulness-based treatments. In R. A. Baer (Ed.), Assessing mindfulness and acceptance: Illuminating the theory and practice of change (pp. 105–133). Oakland, CA: New Harbinger Publications.
Gruber, J., & Moskowitz, J. T. (2014). Positive emotion: Integrating the light sides and dark sides. Oxford, UK: Oxford University Press.
Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., & Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64, 1152–1168.
Hellinger, F. J. (1998). Cost and financing of care for persons with HIV disease: An overview. Health Care Financial Review, 19, 1–14.
Hillis, S. D., Anda, R. F., Felitti, V. J., & Marchbanks, P. A. (2001). Adverse childhood experiences and sexual risk behaviors in women: A retrospective cohort study. Family Planning Perspectives, 33, 206–211.
Holtgrave, D. R., & Pinkerton, S. D. (1997). Updates of cost of illness and quality of life estimates for use in economic evaluations of HIV prevention programs. Journal of Acquired Immune Deficiency Syndromes, 16, 54–62.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1–55.
Hutchinson, A. B., Branson, B. M., Kim, A., & Farnham, P. G. (2006). A meta-analysis of the effectiveness of alternative HIV counseling and testing methods to increase knowledge of HIV status. AIDS, 20, 1597–1604.
Kooiman, C. G., van Rees Vellinga, S., Spinhoven, P., Draijer, N., Trijsburg, R. W., & Rooijmans, H. G. (2004). Childhood adversities as risk factors for alexithymia and other aspects of affect dysregulation in adulthood. Psychotherapy and Psychosomatics, 73, 107–116.
Kraut, R., Olson, J., Banaji, M., Bruckman, A., Cohen, J., & Couper, M. (2004). Psychological research online: Report of Board of Scientific Affairs’ Advisory Group on the conduct of research on the internet. American Psychologist, 59, 105–117.
Linehan, M. M. (1993). Cognitive behavioral treatment of borderline personality disorder. New York, NY: Guilford Press.
Lucenko, B. A., Malow, R. M., Sanchez-Martinez, M., Jennings, T., & Dévieux, J. G. (2003). Negative affect and HIV risk in alcohol and other drug (AOD) abusing adolescent offenders. Journal of Child and Adolescent Substance Abuse, 13, 1–17.
Mata, R., Josef, A. K., Samanez-Larkin, G. R., & Hertwig, R. (2011). Age differences in risky choice: A meta-analysis. Annals of the New York Academy of Sciences, 1235, 18–29.
Meade, A. W., & Craig, S. B. (2012). Identifying careless responses in survey data. Psychological Methods, 17, 437–455.
Messman-Moore, T. L., Walsh, K. L., & DiLillo, D. (2010). Emotion dysregulation and risky sexual behavior in revictimization. Child Abuse and Neglect, 34, 967–976.
Mischra, S., & Carleton, N. (2017). Use of online crowdsourcing platforms for gambling research. International Gambling Studies, 17, 125–143.
Morrison, D. M., Gillmore, M. R., & Baker, S. A. (1995). Determinants of condom use among high-risk heterosexual adults: A test of the theory of reasoned action. Journal of Applied Social Psychology, 25, 651–676.
Oppenheimer, D. M., Meyvis, T., & Davidenko, N. (2009). Instructional manipulation checks: Detecting satisficing to increase statistical power. Journal of Experimental Social Psychology, 45, 867–872.
Orcutt, H. K., Cooper, M. L., & Garcia, M. (2005). Use of sexual intercourse to reduce negative affect as a prospective mediator of sexual revictimization. Journal of Traumatic Stress, 18, 729–739.
Patel, P., Borkowf, C. B., Brooks, J. T., Lasry, A., Lansky, A., & Mermin, J. (2014). Estimating per-act HIV transmission risk: A systematic review. AIDS, 28, 1509–1519.
Peer, E., Vosgerau, J., & Acquisti, A. (2014). Reputation as a sufficient condition for data quality on Amazon Mechanical Turk. Behavior Research Methods, 46, 1023–1031.
Pinkerton, S. D., & Abramson, P. R. (1992). Is risky sex rational? Journal of Sex Research, 29, 561–568.
Poppen, P. J. (1995). Gender and patterns of sexual risk taking in college students. Sex Roles, 32, 545–555.
Price, T. F., & Harmon-Jones, E. (2010). The effect of embodied emotive states on cognitive categorization. Emotion, 10, 934–938.
Prins, A., Bovin, M. J., Smolenski, D. J., Marx, B. P., Kimerling, R., Jenkins-Guarnieri, M. A., … Tiet, Q. Q. (2016). The primary care PTSD screen for DSM-5 (PC-PTSD-5): Development and evaluation within a veteran primary care sample. Journal of General Internal Medicine, 31, 1206–1211.
Roemer, L., Litz, B. T., Orsillo, S. M., & Wagner, A. W. (2001). A preliminary investigation of the role of strategic withholding of emotions in PTSD. Journal of Traumatic Stress, 14, 149–156.
Rosenstock, I. L., Strecher, V. J., & Becker, M. J. (1994). The health belief model and HIV risk behaviour change. In R. J. DiClimente & J. L. Peterson (Eds.), Preventing AIDS: Theories and methods of behavioural interventions (pp. 5–24). New York: Plenum Press.
Shapiro, D. N., Chandler, J., & Mueller, P. A. (2013). Using mechanical turk to study clinical populations. Clinical Psychological Science, 1, 213–220.
Simons, J. S., Maisto, S. A., & Wray, T. B. (2010). Sexual risk taking among young adult dual alcohol and marijuana users. Addictive Behaviors, 35, 533–536.
Slovic, P., Finucane, M. L., Peters, E., & MacGregor, D. G. (2004). Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Analysis, 24, 311–322.
Steiger, J. H. (1990). Structural model evaluation and modification: An interval estimation approach. Multivariate Behavioral Research, 25, 173–180.
Taylor, S., Koch, W. J., & McNally, R. J. (1992). How does anxiety sensitivity vary across the anxiety disorders? Journal of Anxiety Disorders, 6, 249–259.
Thayer, J. F., & Lane, R. D. (2000). A model of neurovisceral integration in emotion regulation and dysregulation. Journal of Affective Disorders, 61, 201–216.
Thomas, K. A., & Clifford, S. (2017). Validity and mechanical turk: An assessment of exclusion methods and interactive experiments. Computers in Human Behavior, 77, 184–197.
Tull, M. T., Weiss, N. H., Adams, C. E., & Gratz, K. L. (2012). The contribution of emotion regulation difficulties to risky sexual behavior within a sample of patients in residential substance abuse treatment. Addictive Behaviors, 37, 1084–1092.
Turchik, J. A., & Garske, J. P. (2009). Measurement of sexual risk taking among college students. Archives of Sexual Behavior, 38, 936–948.
Turchik, J. A., Walsh, K., & Marcus, D. K. (2015). Confirmatory validation of the factor structure and reliability of the Sexual Risk Survey in a large multiuniversity sample of US students. International Journal of Sexual Health, 27, 93–105.
Van der Velde, F. W., & Van der Pligt, J. (1991). AIDS-related health behavior: Coping, protection motivation, and previous behavior. Journal of Behavioral Medicine, 14, 429–451.
van Stolk-Cooke, K., Brown, A., Maheux, A., Parent, J., Forehand, R., & Price, M. (2018). Crowdsourcing trauma: Psychopathology in a trauma-exposed sample recruited via Mechanical Turk. Journal of Traumatic Stress, 31, 549–557.
Vasilev, C. A., Crowell, S. E., Beauchaine, T. P., Mead, H. K., & Gatzke-Kopp, L. M. (2009). Correspondence between physiological and self-report measures of emotion dysregulation: A longitudinal investigation of youth with and without psychopathology. Journal of Child Psychology and Psychiatry, 50, 1357–1364.
Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The PTSD Checklist for DSM–5 (PCL-5). Boston, MA: National Center for PTSD.
Weiss, N. H., Darosh, A., Contractor, A. A., Forkus, S. R., Dixon-Gordon, K. L., & Sullivan, T. P. (2018a). Heterogeneity in emotion regulation difficulties among women victims of domestic violence: A latent profile analysis. Journal of Affective Disorders, 239, 192–200.
Weiss, N. H., Forkus, S. R., Contractor, A. A., & Schick, M. R. (2018b). Difficulties regulating positive emotions and alcohol and drug misuse: A path analysis. Addictive Behaviors, 84, 45–52.
Weiss, N. H., Gratz, K. L., & Lavender, J. M. (2015a). Factor structure and initial validation of a multidimensional measure of difficulties in the regulation of positive emotions: The DERS-positive. Behavior Modification, 39, 431–453.
Weiss, N. H., Risi, M. M., Bold, K. W., Sullivan, T. P., & Dixon-Gordon, K. L. (in press). Daily relationship between positive affect and drinking to cope: The moderating role of difficulties regulating positive emotions. American Journal of Drug and Alcohol Abuse.
Weiss, N. H., Sullivan, T. P., & Tull, M. T. (2015b). Explicating the role of emotion dysregulation in risky behaviors: A review and synthesis of the literature with directions for future research and clinical practice. Current Opinion in Psychology, 3, 22–29.
Weiss, N. H., Tull, M. T., Borne, M. E., & Gratz, K. L. (2013). Posttraumatic stress disorder symptom severity and HIV-risk behaviors among substance-dependent inpatients. AIDS Care, 25, 1219–1226.
Weiss, N. H., Tull, M. T., Davis, L. T., Searcy, J., Williams, I., & Gratz, K. L. (2015c). A preliminary experimental investigation of emotion dysregulation and impulsivity in risky behaviours. Behaviour Change, 32, 127–142.
Weiss, N. H., Tull, M. T., Dixon-Gordon, K., & Gratz, K. L. (2018c). Assessing the negative and positive emotion-dependent nature of risky behaviors among substance dependent patients. Assessment, 25, 702–715.
Weiss, N. H., Tull, M. T., & Sullivan, T. P. (2015d). Emotion dysregulation and risky, self-destructive, and health compromising behaviors: A review of the literature. In M. L. Bryant (Ed.), Handbook on emotion regulation: Processes, cognitive effects and social consequences (pp. 37–56). Hauppauge, NY: Nova Science Publishers.
Weiss, N. H., Williams, D. C., & Connolly, K. M. (2015e). A preliminary examination of negative affect, emotion dysregulation, and risky behaviors among military veterans in residential substance abuse treatment. Military Behavioral Health, 3, 212–218.
Widom, C. S., & Kuhns, J. B. (1996). Childhood victimization and subsequent risk for promiscuity, prostitution, and teenage pregnancy: A prospective study. American Journal of Public Health, 86, 1607–1612.
Wilson, H. W., & Widom, C. S. (2008). An examination of risky sexual behavior and HIV in victims of child abuse and neglect: A 30-year follow-up. Health Psychology, 27, 149–158.
Zapolski, T. C., Cyders, M. A., & Smith, G. T. (2009). Positive urgency predicts illegal drug use and risky sexual behavior. Psychology of Addictive Behaviors, 23, 348–354.
Funding
This study was funded by the National Institute on Drug Abuse (K23DA039327; L30DA038349).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Weiss, N.H., Forkus, S.R., Contractor, A.A. et al. Do Difficulties Regulating Positive Emotions Contribute to Risky Sexual Behavior? A Path Analysis. Arch Sex Behav 48, 2075–2087 (2019). https://doi.org/10.1007/s10508-019-1410-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-019-1410-0