
Abstract
Purpose of Review
Central sleep apnea (CSA) is associated with increased mortality, particularly in heart failure. This review discusses current treatment options with a focus on different positive airway pressure (PAP) modalities, the clinical implication of continuous PAP (CPAP) failure, and key advancements in adaptive servo-ventilation (ASV).
Recent Findings
CPAP reduces CSA by about 50% in patients with heart failure with reduced ejection fraction. The remaining patients are considered non-responsive and chronic use of CPAP has been associated with excess mortality. ASV is effective in several forms of CSA. While secondary analyses of the SERVE-HF trial limited its use in patients with predominant CSA and left ventricular ejection fraction < 45%, more recent data from ADVENT-HF using a newer ASV generation targeting peak flow has shown promising results.
Summary
Physicians should consider the underlying pathophysiology, overall prognosis, and evidence base prior to selecting CSA treatment with CPAP or ASV. Promising pharmaceutical and novel device options require more studies and long-term evidence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Central sleep apnea (CSA) represents a heterogeneous group of sleep related breathing disorders (SRBD) characterized by the recurrent cessation of airflow associated with absence of respiratory effort. Thus far, CSA classification has been based on the partial pressure of carbon dioxide in arterial blood (PaCO2) level with disorders classified under hypercapnic and hypocapnic categories [1]. However, there is considerable overlap. For example, heart failure with reduced ejection fraction (HFrEF) is in the hypocapnic category, yet many such patients have normal PaCO2 levels. In contrast, opioid-associated CSA is in the hypercapnic category, but again a number of such individuals have PaCO2 values within normal levels [2].
Recently a new classification of CSA was suggested by Javaheri and Badr [3]. This classification emphasizes that there is overlap between hypercapnic and non-hypercapnic CSA and seeks to categorize CSA according to the underlying pathophysiology:
-
•High loop gain due to high controller gain which is the most common (e.g. heart failure).
-
•High loop gain due to elevated plant gain (e.g. neuromuscular disorders).
-
•Failure of rhythm generation at the pre-Bötzinger compex/ Kolliker-fuse parabrachial neurons e.g. opioid-associated CSA.
-
•Unclassified.
The underlying cause and pathophysiology of CSA is varied resulting in a wide spectrum of clinical diseases and outcomes. CSA adversely affects cardiovascular function by causing tissue hypoxia, arousals from sleep, and activation of the sympathetic nervous system, thereby independently increasing the risk of death [1]. Heart failure (HF) is the most common condition associated with CSA such that the available literature focuses almost exclusively on this important group (Table 1). Other entities include CSA in musculoskeletal or neurological diseases, drug-induced CSA, treatment-induced CSA, high-altitude CSA and idiopathic CSA. Understanding the mechanism behind the CSA in each disease process is essential in the selection of treatment options.
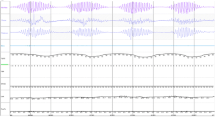
Periodic breathing (PB) is a polysomnographic subtype of CSA, with Hunter-Cheyne-Stokes breathing (HCSB) denoting the presence of PB in HF [4]. CSA with HCSB is the focus of this review, being more prevalent and therefore having a greater clinical impact.
Pathophysiological Mechanism of CSA in Heart Failure
The ratio of the size of the ventilatory response to the breathing disturbance can be described using the concept of loop gain (LG). This term, which has been extensively described [5, 6], characterizes this form of CSA. LG refers to the response of the ventilatory system to any disturbance, and includes the reactivity of the ventilatory system via the lungs (plant gain) as well as the peripheral chemoreceptors at the carotids and the central chemoreceptors at the brainstem (controller gain) to a disturbance. If the ventilatory response to this disturbance is excessive (high loop gain), overshoot will occur and result in hypocapnia which can result in central apneas. Chemostimulation due to CSA (hypoxia and increased PaCO2 stimulating peripheral and central chemoreceptors) leads to further overshoot and the cycle self-repeats rather than dissipates, as would be the case with a normal loop gain.
The PaCO2 in the blood has a semi-linear impact on ventilation through its influence at the central chemoreceptors [7]. Hypercapnia stimulates ventilation and hypocapnia reduces it. The level of PaCO2 below which breathing ceases – the apneic threshold (AT)—dictates the overall stability of the system. Whenever PaCO2 drops below the AT, a central apnea occurs [8]. A small distance between the AT and the actual PaCO2 (the so-called CO2 reserve) predisposes to unstable ventilation. Under these circumstances, even mild variations in minute ventilation reduce the PaCO2 below or elevate it above the AT. Hypersensitivity of the chemoreceptors and ensuing responses of the chemoreceptors induce a vicious cycle of alternating hyper- and hypoventilation. The resulting clinical and polysomnographic (PSG) pattern of PB appears with crescendo–decrescendo variations in tidal volume and respiratory effort (HCSB). Other investigators point out that sleep state instability with increased arousals can also contribute to a drop in CO2 level due to the associated ventilatory response [9,10,11].
CSA is primarily a disorder of non-rapid-eye-movement (NREM) sleep when ventilatory drive and minute ventilation are metabolically controlled by PaCO2 levels [3]. CSA is relatively uncommon in REM sleep.
Treatment Rationale and Therapy Options in CSA
The presence of sleep-related breathing disorders (SRBD) has been shown to have an independent impact on overall mortality regardless of the underlying disease process [12,13,14,15,16,17]. There is no convincing evidence from randomized controlled trials (RCT) to show that CSA-specific therapy improves mortality, particularly outside HF. However, large population-based studies of SRBD such as the Wisconsin sleep cohort [13] and retrospective analyses of HF patients show that those who are diagnosed and treated have better survival [18]. Several studies subsequently presented in this review do show an improvement in sleep quality and functionality and an improvement in quality of life (QoL), however the benefit is not consistently shown. The decision to initiate CSA-specific treatment should therefore be based on a combination of the severity of the breathing disorder, and the clinical and symptomatic impact based on patient-related outcome parameters.
Prior to selecting a specific therapy for management of CSA, any underlying cardiovascular, internal, neurological or pharmacological causes should be optimized, including optimal guideline directed medical therapy of HF. If CSA remains unresolved, additional therapy directed at resolving CSA should be considered. This includes careful history taking in the recognition of drug-induced CSA with drug withdrawal if possible and time for acclimatization or immediate descent in CSA associated with high-altitude.
Pharmacological Therapy
A variety of pharmaceutical agents addressing various pathophysiological components have been studied or are under current investigation. Long-term data on overall prognosis is limited with all these agents. In clinical practice, pharmacological therapy is considered in cases of primary CSA and treatment emergent central sleep apnea (TECSA) or in individual cases with either failure or inappropriateness of other treatment options [19, 20].
-
Buspirone, a 5-HT-receptor agonist, reduces central chemoreceptor sensitivity to CO2 (a decrease in controller gain) and consequently downregulates the high loop gain, stabilizing breathing [21].
-
Acetazolamide, a carbonic anhydrase inhibitor, is a respiratory stimulant that increases alveolar ventilation and widens the CO2 reserve, helping to stabilize breathing through decreased plant gain [22]. Short-term studies have shown improved sleep parameters, and symptom reduction with no serious adverse events [23,24,25]. The use of acetazolamide is well-established in high-altitude induced periodic breathing and acute mountain sickness [26].
-
Theophylline, a respiratory stimulant, also works by decreasing plant gain similar to acetazolamide [27].
-
Hypnotics such as Zolpidem reduce arousals and in an open label study of idiopathic CSA improved the total apnea-hypopnea index (AHI) [28]. However, in a RCT use of benzodiazepine receptor agonists reduced arousals but did not significantly reduce CSA in HF patients [29]
-
Novel pharmaceutical candidates that inhibit the signaling of neurotransmitters which underlie hypoxia-induced chemosensitivity in the carotid body (CO, H2S, and P2X3 receptors among others) may also eventually be used to treat PB [30,31,32,33].
Although these drugs alone may not suffice to resolve CSA completely, they may play a role in future multimodal concepts.
Transvenous Phrenic Nerve Stimulation (TPNS)
TPNS describes the use of an implanted neurostimulator to stimulate the phrenic nerve. The basic mechanism which overcomes CSA is the stimulation of the diaphragm. However, in the subtype of PB (high loop gain), the mechanism needs to be studied further. TPNS may additionally break the cycle of PB by interfering with the pathophysiology. It prevents periods of undershoot and hypercapnia, thus avoiding subsequent overshoot. RCTs as well as single-center and pooled studies have shown benefits of TPNS including significant improvement in CSA, desaturation, and arousals and quality of life (QoL). These studies also demonstrate that TPNS is well tolerated [34, 35]. A small prospective cohort study (n = 24) demonstrated safety and efficacy of TPNS as well as improvement in physical performance capacity and reduced hypoxemic burden in patients with HF [36]. Data from long-term RCTs for hard outcomes are needed concerning safety in HF. However, an adequately powered RCT along with long-term observational studies have demonstrated overall safety and effectiveness leading to Federal Drug Administration clearance of TPNS for CSA.
Nocturnal Low-Flow Oxygen Therapy
An increase in arterial O2 works to lower the carotid-body chemosensitivity and to improve myocardial function. Low-flow nocturnal oxygen therapy attenuates CSA and lessens the augmented sympathetic activity seen in subjects with HFrEF. Physiological improvement in maximum oxygen consumption with exercise and increased LVEF and (QoL) have also been demonstrated [37]. There is evidence that oxygen therapy lowers AHI [38], but no long-term prognostic benefit has been proven. The phase 3 RCT LOFT-HF (Impact of Low-Flow Nocturnal Oxygen Therapy on Hospital Admissions and Mortality in Patients with Heart Failure and CSA) was terminated early due to low patient recruitment during the COVID-19 pandemic. Oxygen therapy is easily available and well tolerated. However, there is no evidence to show that its use is comparable to that of PAP therapy or to prove that there is no harm in HFrEF patients long-term. Therefore, it remains an individual treatment for those unable to comply with or lacking access to PAP therapy. Oxygen therapy is also used in the treatment of high-altitude CSA [39].
Positive Pressure Therapy
Continuous Positive Airway Pressure (CPAP)
CPAP mechanically supports and opens up the upper airway without addressing the shallow breathing patterns and breathing cessation characteristic of CSA. CPAP does improve oxygenation through reduction of ventilation/perfusion (V/Q) mismatch, which has an effect on the pathophysiology of CSA. CPAP also affects the preload and afterload of the heart, leading to a decrease in systolic blood pressure and an improvement in LVEF and right ventricular function (RVF) [40,41,42].
Evidence was initially promising that CPAP may reduce sympathoneural activity [43] and improve QoL and mortality in HF [41]. The CANPAP trial studied the effect of CPAP therapy in 258 HF patients with CSA. The first polysomnography was performed at 3 months after use of CPAP. There was an improvement in nocturnal oxygenation, the number of respiratory disturbances and the LVEF; however, there was no improvement in QoL, reduction in hospitalization at 2 years or transplant-free survival [44]. Although CPAP reduced AHI overall by 53%, 43% of the study participants still had a residual AHI of ≥ 15/h. A post-hoc analysis by Arzt et al. stratifying by treatment efficacy (AHI less than 15/h versus those with AHI ≥ 15/h) demonstrated both improvement in LVEF and transplantation-free survival in those with effective suppression of CSA with CPAP [45].
Treatment-response may indicate a specific phenotype with better outcomes to CPAP. In this regard, Sands et al. examined the question as to why CPAP is only successful in half of the patients. They designed and validated a mathematical system to efficiently analyse LG and showed that CPAP is effective in HCSB if the loop gain was < 1.10 [46]. Herkenrath et al. showed that LG also depends on the sleep stage and body position with less ventilatory overshoot in REM sleep [47].
The practice of using automatic PAP (APAP) for home or in-lab titration for the initial treatment of obstructive sleep apnea (OSA) is well established. This allows physicians to identify the minimum pressure needed to keep airways patent. A recent large RCT of CPAP vs. APAP in the treatment of OSA was able to show that these modalities have similar effectiveness and adherence [48]. There is no similar research as to the effectiveness of APAP in the treatment of CSA so that this algorithm cannot be recommended in case of CPAP failure. As the mean pressure in APAP is substantially lower in CSA compared to when used in OSA (it is the obstruction which is the main trigger for the higher pressure), the above mentioned effects on lung ventilation and cardiac mechanics cannot be translated one-to-one to CSA [49].
CPAP may also have limited effect in opioid-associated CSA. Teichtahl et al. postulate that the dose-dependent development of SRDB with opioid use may be a cause for unexplained death in these patients [50]. Troitino et al. [51] performed a retrospective analysis and found that CPAP reduced the AHI to ≤ 10/h in only 24% of the studied patients. Similarly, evidence for the use of CPAP in the management of high-altitude CSA is limited. It may be discussed in combination with drugs and oxygen.
In routine clinical care, CPAP remains a cost-effective initial treatment option in most forms of CSA. As there is no evidence of prognostic benefit, close supervision of treatment response regarding improvement of both breathing disturbances and symptoms is required [1, 20]. If ineffective, the use of adaptive servo-ventilation (ASV) should be considered.
Bilevel Positive Airway Pressure (BPAP)
BPAP delivers two different but fixed pressure levels during inspiration and expiration. BPAP can be used in spontaneous (S), timed (T) or spontaneous-timed (ST) mode. BPAP is comparable to CPAP and APAP in that it stabilizes the upper airway, however, it also additionally provides mechanical ventilation. In contrast to S-mode, in the presence of insufficient ventilation in hypercapnic respiratory failure, the T-mode and ST-mode can apply mandatory breaths and non-invasively ventilate patients by increasing the difference between inspiratory and expiratory pressure. The fixed pressure and the pressure difference of BPAP leads to the danger of hyperventilation and may worsen central apnea by lowering the PaCO2 below the AT [52]. The persistence of central apneas under CPAP treatment in some patients and the lack of an alternative therapy however culminated in trials of BPAP therapy, which initially showed some acute effect over the course of a single night [53]. A 6-month follow-up of a small cohort of CPAP non-responders (n = 7) treated with BPAP showed some clinical benefit such as an improvement in LVEF [54]. A RCT of 30 patients with TECSA (previously treated with CPAP) assigned to either non-invasive ventilation (NIV) or ASV showed that respiratory events were treated more effectively with ASV [55]. Most importantly the initial positive effects seen after the first night of BPAP were attenuated at 6 weeks follow-up.
The risk of deterioration based on our understanding of physiology combined with the paucity of clinical evidence suggests that there can currently be no recommendation for the use of BPAP therapy in the treatment of non-hypercapnic CSA (high loop-gain CSA).
Adaptive Servo-Ventilation
ASV was developed as a treatment for CSA not responsive to CPAP therapy. It is a form of NIV that delivers variable servo-controlled inspiratory pressure support (IPS) when tidal volume wanes and withdraws that support when ventilation is excessive [56]. The devices measures instantaneous inspiratory airflow in order to calculate ventilation. The continuous measurement of airflow enables the calculation and maintenance of target ventilation, set at 90% to 95% of the recent average ventilation. ASV algorithms differ in the target parameters of minute ventilation (ASVmf) or peak flow (ASVpf). Mandatory breaths are applied in a timed backup mode to abort any frank apneas.
The first generation ASV devices applied a fixed expiratory PAP (EPAP) to suppress obstructive events [57]. The EPAP was set based on data from a previous PAP titration. Newer generations of ASV apply variable EPAP according to the actual upper airway obstruction. Moreover, the previous algorithms applied a minimal pressure support of 3 cmH2O, even during hyperventilation, while the newer algorithms allow for zero pressure support when it is not needed.
There is a large body of evidence dating back to 2001 to confirm the effectiveness of ASV in the treatment of CSA not responsive to CPAP, above all in HF, but also in CSA related to chronic opioid use and TECSA (Table 2). ASV normalizes both OSA and CSA including HCSB, reduces brain natriuretic peptide, and improves symptoms, LVEF, and sleep parameters. Treatment response appears to be superior to CPAP and oxygen. [2, 56, 58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74]. Sleep apnea is classified at PSG as either predominantly obstructive or predominantly central to guide therapy. However, the predominant mechanism of sleep apnea may vary throughout the night concurrent with changes in sleep stage and position, as well as fluid shifts due to the recumbent sleeping position. The variation of EPAP and pressure support of ASV addresses all these issues.
All of the smaller prospective cohort and retrospective studies show a positive or neutral effect of ASV on major outcome parameters, sleep and QoL (Table 2). However, the RCT SERVE-HF of 1325 patients with a LVEF of < 45% showed ASV had no improvement in the primary outcome of all-cause mortality or lifesaving cardiovascular intervention [75]. In the secondary analysis, there was a higher all-cause and cardiovascular mortality in the ASV group. Several factors need to be critically viewed when interpreting the mortality results:
-
The first generation ASV used in the SERVE-HF study may have favored ventilation over stabilization of breathing. These devices applied a minimal pressure support of 3 cmH2O even in periods of hyperventilation. This unnecessary elevation in minute ventilation reduces the CO2 level, which destabilizes ventilation. The accompanying electrolyte fluctuations may have precipitated arrhythmias.
-
The applied fixed EPAP failed to eliminate obstructive events and desaturation in this cohort, which may in part have contributed to excess mortality. Additionally, once the upper airway opened, excessive IPAP was applied by the device and this ASV-associated excessive rise in intrathoracic pressure may have contributed to mortality.
-
ASV adherence was low at only 3.4 h per night. Takama et al. showed that ASV use of < 4 h compared to ASV use > 4 h was associated with higher 1-year mortality [61].
-
There was a relevant switch between the treatment arms (29% of the patients randomized to the ASV group dropped out and 16% of the control patients switched to the ASV group).
Nevertheless, the results of the SERVE-HF trial had a significant impact on the treatment of HF with CSA with national guidelines contradicting the use of ASV in HF patients with EF < 45% [1, 20] soon after the study was published.
Most recently, the results of the ADVENT-HF study were presented. Similar to SERVE-HF, it aimed to evaluate long-term outcomes under ASV [76, 77]. The trial differed from SERVE-HF in several aspects:
-
It used the new generation of ASV, which allowed for a reduction of pressure support to zero in periods of hyperventilation as well as the already mentioned adaptive EPAP [57, 78, 79].
-
The device was based on peak flow (ASVpf), while ASVmf was used in SERVE-HF.
-
Moreover, ADVENT-HF included not only HF patients with CSA but also OSA.
The composite end-points were all-cause mortality, heart transplantation, ventricular assist device (VAD) implantation, cardiovascular disease-related hospitalization, implantable cardioverter-defibrillator shock and new atrial fibrillation. A follow-up PSG was carried out at 1 month. The centralized assessment of ASV titrations and prescription of pressure settings contributed to effective control of SRDB (the mean AHI taken from participants’ ASV devices ranged between 2.8 /h and 3.7 /h over the course of the trial). Unfortunately, the study had to be terminated prematurely and did not reach the pre-calculated figures due to the COVID-19 pandemic and the Philips device recall. In total, 356 patients were recruited to ASV (completed n = 324; age: 62.7 ± 11.1 y.; LVEF: 33.1 ± 7.1%; CSA 25.8%; AHI 41.1 ± 19.9) and 375 assigned to not receive ASVpf (completed: 332; age: 63.6 ± 10.1 y.; LVEF: 33.3 ± 7.9%; CSA 28.3%; AHI 41.3 ± 22.9). The results showed no difference in the cumulative incidence of primary end-points or all-cause mortality in the OSA or CSA patients allocated to ASV use compared to the control group [77]. Under ASVpf, there was no signal of harm and a trend to improvement of survival in CSA patients. The predefined Hazard Ratio of 0.74 was achieved but did not reach statistical significance. ASV significantly improved severity of SRDB, sleep parameters, sleepiness and New York Heart Association (NYHA) class in all patients and those randomized to ASVpf for up to 2 years. The findings on the available data on ASV in HF may be summarized:
-
The largest RCT (SERVE-HF) was neutral in the primary combined outcome parameter, but showed higher mortality in secondary analyses.
-
Several prospective, non-randomized trials showed beneficial effects in various parameters of heart function, sleep parameters and patient-reported outcomes.
-
This was supported by the results of ADVENT-HF, which did not show any harm and benefits in quality of sleep and life from ASV.
These findings warrant discussion about whether the ASV device and settings of ADVENT-HF can be applied in HF patients with EF < 45% (a contraindication to ASV based on the SERVE-HF results). There is evidence to show that the mortality risk of CSA patients with HF is influenced mainly by the phenotype and severity of HF [41]. The FACE trial examined unselected HF patients with differing degree of LV impairment [73]. A cluster analysis identified 6 clinical phenotypes based on LVEF, SRDB, age, comorbidities and ASV acceptance. The risk for the combined primary end-point of mortality, hospitalization, heart transplantation, and VAD implantation was significantly increased in the cluster of male patients with low LVEF and CSA, that is to say, the SERVE-HF phenotype. One of the clusters, however, was from the cohort enrolled in the SERVE-HF [80]. A network metanalysis of 14 RCTs showed ASV to be the treatment of choice for decreasing AHI in patients with HF and CSA [38].
There is evidence for a worse functional outcome and increased mortality in the presence of SRBD in stroke patients [12, 81]., Whilst the evidence base for OSA in stroke supports active diagnosis and therapy, direct evidence for treatment of CSA is limited [81]. In a retrospective single-center study by Brill et al. [82] AHI and Epworth sleepiness score (ESS) improved in 15 stroke patients treated with ASV (13 of whom were previously started on CPAP or BPAP). A prospective RCT of ASV following acute stroke (eSATIS: early Sleep Apnea Treatment in Stroke) [83] has been recruiting since 2015 and aims to make an impact on stroke care. ASV has been shown to be superior to CPAP in suppressing central events in opioid-induced CSA as well [51]. Additionally, there is evidence to show that the adherence to therapy in TECSA improves early after switching from CPAP to ASV [84].
In translating this available evidence to clinical practice, we conclude that ASV is a viable and suitable option for the majority of patients with CSA who are not responsive to CPAP. As discussed above, a small group of patients should not be offered treatment, although even within this small subgroup of HF patients there is evidence suggesting that the greatest risks lie for those with a LVEF ≤ 30% [85]. These findings indicate that a stratification of the CSA population regarding the severity of left ventricular impairment is crucial and may be an important step in a therapeutic algorithm.
Studies have been conducted to analyze current and past use of ASV in clinical practice in relation to the SERVE-HF results. An analysis of 293 unselected patients treated with ASV showed that only a minority of patients (9.6%) fulfilled the risk criteria as described in the SERVE-HF trial [86]. A further single-center study analyzing patients already established on ASV showed the risk criteria of the safety notice were fulfilled by 10.3% of patients (13/126) [87]. Termination of ASV therapy in these patients led to an immediate return of symptoms in 60% and need for an alternative treatment. The primary analysis of 801 ASV patients recruited into a European registry between 2017 until 2021 (READ-ASV) [88] showed that the most common indications for ASV use were TECSA (56% of cases) or CSA in cardiovascular disease provided LVEF was > 45% (constituting 31% of cases). The remaining patients were post-stroke, opioid-use, unclassified CSA, CSA with concomitant OSA or OSA alone. Patients using ASV in clinical practice had severe SRDB and were often symptomatic. Prior analysis of a German databank of 285 patients also showed TECSA to be the main clinical indication for ASV prescription. Patients with LVEF ≤ 45% and predominant CSA in whom ASV is now contraindicated represented only 12% of all patients [89]. It is hoped that follow-up from the READ-ASV will provide data on the effects of ASV on QoL, respiratory parameters and clinical outcomes in these patients in a real-life setting.
Treatment Algorithm
Therapy decisions in CSA should be based on the definition of the subtype and its underlying pathophysiology, on the individual comorbidities and prognosis, as well as patient-reported outcomes (Fig. 1). In accordance with the European Respiratory Society guidelines [1], once the diagnosis of CSA is confirmed at PSG and the underlying medical treatment has been optimized, a trial of CPAP can be considered. If CPAP fails to normalize central breathing disturbances and symptoms, consider conversion to ASV in cases where severe HFrEF can be ruled out. This limitation may change in the future in light of recent findings. Non-PAP therapies currently represent an alternative with a limited evidence base, to be used in the event of PAP failure or unavailability. As long-term data are scarce, these individual, alternative decisions require close supervision and continuous re-evaluation.

Treatment algorithm for all clinical forms of CSA. CRT cardiac resynchronization therapy, CPAP continuous positive airway pressure, LVEF left ventricular ejection fraction, ASV adaptive-servoventilation, TECSA treatment-emergent central sleep apnea, NIV non-invasive ventilation
Conclusion
CSA has a complex and diverse etiology and understanding the pathophysiology is essential for choosing the best treatment option. There is no long-term RCT data to show a reduction in mortality following initiation of CSA-specific therapy. The data discussed in this review present overwhelmingly positive or neutral benefits in terms of sleep parameters, organ function and symptoms, so that therapy can be considered on an individual basis. Once a decision to treat has been made, CPAP and ASV represent the first steps. The FACE data warns us that caution needs to be particularly exercised in specific subgroups with higher mortality. Potential harm in patients with severely reduced HFrEF has not been confirmed with newer generations of ASV devices that target peak flow (ASVpf), although available data do not allow for final conclusions. In this context, assumptions of safety of alternative treatment cannot be lightly made as larger powered studies may be required to demonstrate long-term effects. In disease processes associated with less mortality (for example drug-induced or high-altitude related CSA), there is a level of freedom with the choice of treatment and the sequence of use. In these cases, the physician can decide based on a combination of availability, cost and patient preferences.
Data Availability
No datasets were generated or analysed during the current study.
References
Randerath W, Verbraecken J, Andreas S, Arzt M, Bloch KE, Brack T, et al. Definition, discrimination, diagnosis and treatment of central breathing disturbances during sleep. Eur Respir J. 2017;49(1):1600959–1600959.
Javaheri S, Harris N, Howard J, Chung E. Adaptive Servoventilation for Treatment of Opioid-Associated Central Sleep Apnea. J Clin Sleep Med. 2014;10(06):637–43.
Javaheri S, Badr MS. Central sleep apnea: pathophysiologic classification. Sleep. 2023;46(3):zsac113.
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events: Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;08(05):597–619.
Wellman A, Malhotra A, Fogel RB, Edwards JK, Schory K, White DP. Respiratory system loop gain in normal men and women measured with proportional-assist ventilation. J Appl Physiol. 2003;94(1):205–12.
Khoo MC, Gottschalk A, Pack AI. Sleep-induced periodic breathing and apnea: a theoretical study. J Appl Physiol. 1991;70(5):2014–24.
Gothe B, Altose MD, Goldman MD, Cherniack NS. Effect of quiet sleep on resting and CO2-stimulated breathing in humans. J Appl Physiol. 1981;50(4):724–30.
Younes M. Measurement of the co 2 apneic threshold. Am J Respir Crit Care Med. 2003;167(3):472–3.
Horner RL. Autonomic consequences of arousal from sleep: mechanisms and implications. Sleep. 1996;19(10 Suppl):S193-195.
Jordan AS, Eckert DJ, Catcheside PG, McEvoy RD. Ventilatory Response to Brief Arousal from Non-Rapid Eye Movement Sleep Is Greater in Men Than in Women. Am J Respir Crit Care Med. 2003;168(12):1512–9.
Roberts EG, Raphelson JR, Orr JE, LaBuzetta JN, Malhotra A. The Pathogenesis of Central and Complex Sleep Apnea. Curr Neurol Neurosci Rep. 2022;22(7):405–12.
Parra O, Arboix A, Montserrat JM, Quintó L, Bechich S, García-Eroles L. Sleep-related breathing disorders: impact on mortality of cerebrovascular disease. Eur Respir J. 2004;24(2):267–72.
Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, et al. Sleep Disordered Breathing and Mortality: Eighteen-Year Follow-up of the Wisconsin Sleep Cohort. Sleep. 2008;31(8):1071–8.
Punjabi NM, Caffo BS, Goodwin JL, Gottlieb DJ, Newman AB, O’Connor GT, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009;6(8): e1000132.
Naito R, Kasai T, Narui K, Momomura S-I. Association between Frequency of Central Respiratory Events and Clinical Outcomes in Heart Failure Patients with Sleep Apnea. JCM. 2022;11(9):2403.
Brack T, Randerath W, Bloch KE. Cheyne-Stokes Respiration in Patients with Heart Failure: Prevalence, Causes. Conseq Treat Respirat. 2012;83(2):165–76.
Khayat R, Jarjoura D, Porter K, Sow A, Wannemacher J, Dohar R, et al. Sleep disordered breathing and post-discharge mortality in patients with acute heart failure. Eur Heart J. 2015;36(23):1463–9.
Javaheri S, Caref EB, Chen E, Tong KB, Abraham WT. Sleep Apnea Testing and Outcomes in a Large Cohort of Medicare Beneficiaries with Newly Diagnosed Heart Failure. Am J Respir Crit Care Med. 2011;183(4):539–46.
Zeineddine S, Badr MS. Treatment-Emergent Central Apnea. Chest. 2021;159(6):2449–57.
Aurora RN, Chowdhuri S, Ramar K, Bista SR, Casey KR, Lamm CI, et al. The Treatment of Central Sleep Apnea Syndromes in Adults: Practice Parameters with an Evidence-Based Literature Review and Meta-Analyses. Sleep. 2012;35(1):17–40.
Maresh S, Prowting J, Vaughan S, Kruppe E, Alsabri B, Yarandi H, et al. Buspirone decreases susceptibility to hypocapnic central sleep apnea in chronic SCI patients. J Appl Physiol. 2020;129(4):675–82.
Javaheri S, Germany R. Treatment of central sleep apnoea with oxygen, drugs and phrenic nerve stimulation. In: Bonsignore MR, Randerath W, Schiza SE, Simonds AK, editors. ERS Handbook of Respiratory Sleep Medicine. The European Respiratory Society; 2023. p. 215–21.
Giannoni A, Borrelli C, Mirizzi G, Richerson GB, Emdin M, Passino C. Benefit of buspirone on chemoreflex and central apnoeas in heart failure: a randomized controlled crossover trial. Euro J of Heart Fail. 2021;23(2):312–20.
Schmickl CN, Landry SA, Orr JE, Chin K, Murase K, Verbraecken J, et al. Acetazolamide for OSA and Central Sleep Apnea. Chest. 2020;158(6):2632–45.
Javaheri S. Acetazolamide Improves Central Sleep Apnea in Heart Failure: A Double-Blind, Prospective Study. Am J Respir Crit Care Med. 2006;173(2):234–7.
Toussaint CM, Kenefick RW, Petrassi FA, Muza SR, Charkoudian N. Altitude, Acute Mountain Sickness, and Acetazolamide: Recommendations for Rapid Ascent. High Alt Med Biol. 2021;22(1):5–13.
Javaheri S, Parker TJ, Wexler L, Liming JD, Lindower P, Roselle GA. Effect of theophylline on sleep-disordered breathing in heart failure. N Engl J Med. 1996;335(8):562–7.
Ahmad B, Sankari A, Eshraghi M, Aldwaikat A, Yarandi H, Zeineddine S, et al. Effect of Zolpidem on nocturnal arousals and susceptibility to central sleep apnea. Sleep Breath. 2023;27(1):173–80.
Biberdorf DJ, Steens R, Millar TW, Kryger MH. Benzodiazepines in Congestive Heart Failure: Effects of Temazepam on Arousability and Cheyne-Stokes Respiration. Sleep. 1993;16(6):529–38.
Marcus NJ, Del Rio R, Ding Y, Schultz HD. KLF2 mediates enhanced chemoreflex sensitivity, disordered breathing and autonomic dysregulation in heart failure. J Physiol. 2018;596(15):3171–85.
Huxtable AG, Smith SMC, Peterson TJ, Watters JJ, Mitchell GS. Intermittent Hypoxia-Induced Spinal Inflammation Impairs Respiratory Motor Plasticity by a Spinal p38 MAP Kinase-Dependent Mechanism. J Neurosci. 2015;35(17):6871–80.
Peng Y-J, Zhang X, Gridina A, Chupikova I, McCormick DL, Thomas RJ, et al. Complementary roles of gasotransmitters CO and H 2 S in sleep apnea. Proc Natl Acad Sci USA. 2017;114(6):1413–8.
Ford AP, Undem BJ, Birder LA, Grundy D, Pijacka W, Paton JFR. P2X3 receptors and sensitization of autonomic reflexes. Auton Neurosci. 2015;191:16–24.
Costanzo MR, Ponikowski P, Javaheri S, Augostini R, Goldberg L, Holcomb R, et al. Transvenous neurostimulation for central sleep apnoea: a randomised controlled trial. The Lancet. 2016;388(10048):974–82.
Fudim M, Spector AR, Costanzo M-R, Pokorney SD, Mentz RJ, Jagielski D, et al. Phrenic Nerve Stimulation for the Treatment of Central Sleep Apnea: A Pooled Cohort Analysis. J Clin Sleep Med. 2019;15(12):1747–55.
Potratz M, Sohns C, Dumitrescu D, Sommer P, Fox H. Phrenic Nerve Stimulation Improves Physical Performance and Hypoxemia in Heart Failure Patients with Central Sleep Apnea. JCM. 2021;10(2):202.
Nakao YM, Ueshima K, Yasuno S, Sasayama S. Effects of nocturnal oxygen therapy in patients with chronic heart failure and central sleep apnea: CHF-HOT study. Heart Vessels. 2016;31(2):165–72.
Chen C, Wen T, Liao W. Nocturnal supports for patients with central sleep apnea and heart failure: a systemic review and network meta-analysis of randomized controlled trials. Ann Transl Med. 2019;7(14):337–337.
Burgess KR, Ainslie PN. Central Sleep Apnea at High Altitude. In: Roach RC, Hackett PH, Wagner PD, editors. Hypoxia. Boston, MA: Springer, US; 2016. p. 275–83.
Sasayama S, Izumi T, Seino Y, Ueshima K, Asanoi H, for The CHF-HOT Study Group. Effects of Nocturnal Oxygen Therapy on Outcome Measures in Patients With Chronic Heart Failure and Cheyne-Stokes Respiration. Circ J. 2006;70(1):1–7.
Sin DD, Logan AG, Fitzgerald FS, Liu PP, Bradley TD. Effects of Continuous Positive Airway Pressure on Cardiovascular Outcomes in Heart Failure Patients With and Without Cheyne-Stokes Respiration. Circulation. 2000;102(1):61–6.
Yoshihisa A, Suzuki S, Yamauchi H, Sato T, Oikawa M, Kobayashi A, et al. Beneficial Effects of Positive Airway Pressure Therapy for Sleep-Disordered Breathing in Heart Failure Patients With Preserved Left Ventricular Ejection Fraction. Clin Cardiol. 2015;38(7):413–21.
Naughton MT, Benard DC, Liu PP, Rutherford R, Rankin F, Bradley TD. Effects of nasal CPAP on sympathetic activity in patients with heart failure and central sleep apnea. Am J Respir Crit Care Med. 1995;152(2):473–9.
Bradley TD, Logan AG, Kimoff RJ, Sériès F, Morrison D, Ferguson K, et al. Continuous Positive Airway Pressure for Central Sleep Apnea and Heart Failure. N Engl J Med. 2005;353(19):2025–33.
Arzt M, Floras JS, Logan AG, Kimoff RJ, Series F, Morrison D, et al. Suppression of Central Sleep Apnea by Continuous Positive Airway Pressure and Transplant-Free Survival in Heart Failure: A Post Hoc Analysis of the Canadian Continuous Positive Airway Pressure for Patients With Central Sleep Apnea and Heart Failure Trial (CANPAP). Circulation. 2007;115(25):3173–80.
Sands SA, Edwards BA, Kee K, Turton A, Skuza EM, Roebuck T, et al. Loop Gain As a Means to Predict a Positive Airway Pressure Suppression of Cheyne-Stokes Respiration in Patients with Heart Failure. Am J Respir Crit Care Med. 2011;184(9):1067–75.
Herkenrath SD, Lacerda C, Treml M, Pietzke-Calcagnile A, Richter K, Hagmeyer L, et al. Loop gain in heart failure with reduced ejection fraction and periodic breathing is associated with sleep stage and arousals. Ann Am Thorac Soc. 2019;16(12):1591–5.
Bironneau V, Ingrand P, Pontier S, Iamandi C, Portel L, Martin F, et al. Auto-adjusted versus fixed positive airway pressure in patients with severe OSA : A large randomized controlled trial. Respirology. 2023;28(11):1069–77.
Randerath W. Positive Airway Pressure for Sleep-Related Breathing Disorders in Heart Failure—Overview and Discussion of Potential Mechanisms of Harm. Curr Sleep Medicine Rep. 2018;4(2):149–59.
Teichtahl H, Prodromidis A, Miller B, Cherry G, Kronborg I. Sleep-disordered breathing in stable methadone programme patients: a pilot study. Addiction. 2001;96(3):395–403.
Troitino A, Labedi N, Kufel T, El-Solh AA. Positive airway pressure therapy in patients with opioid-related central sleep apnea. Sleep Breath. 2014;18(2):367–73.
Johnson KG, Johnson DC. Bilevel Positive Airway Pressure Worsens Central Apneas During Sleep. Chest. 2005;128(4):2141–50.
Arzt M, Wensel R, Montalvan S, Schichtl T, Schroll S, Budweiser S, et al. Effects of Dynamic Bilevel Positive Airway Pressure Support on Central Sleep Apnea in Men With Heart Failure*. Chest. 2008;134(1):61–6.
Dohi T, Kasai T, Narui K, Ishiwata S, Ohno M, Yamaguchi T, et al. Bi-Level Positive Airway Pressure Ventilation for Treating Heart Failure With Central Sleep Apnea That is Unresponsive to Continuous Positive Airway Pressure. Circ J. 2008;72(7):1100–5.
Dellweg D, Kerl J, Hoehn E, Wenzel M, Koehler D. Randomized Controlled Trial of Noninvasive Positive Pressure Ventilation (NPPV) Versus Servoventilation in Patients with CPAP-Induced Central Sleep Apnea (Complex Sleep Apnea). Sleep. 2013;36(8):1163–71.
Sharma BK, Bakker JP, McSharry DG, Desai AS, Javaheri S, Malhotra A. Adaptive Servoventilation for Treatment of Sleep-Disordered Breathing in Heart Failure. Chest. 2012;142(5):1211–21.
Javaheri S, Brown LK, Randerath WJ. Positive Airway Pressure Therapy With Adaptive Servoventilation. Chest. 2014;146(2):514–23.
Arzt M, Schroll S, Series F, Lewis K, Benjamin A, Escourrou P, et al. Auto-servoventilation in heart failure with sleep apnoea: a randomised controlled trial. Eur Respir J. 2013;42(5):1244–54.
Fietze I, Blau A, Glos M, Theres H, Baumann G, Penzel T. Bi-level positive pressure ventilation and adaptive servo ventilation in patients with heart failure and Cheyne-Stokes respiration. Sleep Med. 2008;9(6):652–9.
Randerath WJ, Nothofer G, Priegnitz C, Anduleit N, Treml M, Kehl V, et al. Long-term Auto-Servoventilation or Constant Positive Pressure in Heart Failure and Coexisting Central With Obstructive Sleep Apnea. Chest. 2012;142(2):440–7.
Takama N, Kurabayashi M. Safety and efficacy of adaptive servo-ventilation in patients with severe systolic heart failure. J Cardiol. 2014;63(4):302–7.
Koyama T, Watanabe H, Terada S, Makabe S, Igarashi G, Nobori K, et al. Adaptive servo-ventilation improves renal function in patients with heart failure. Respir Med. 2011;105(12):1946–53.
Yoshihisa A, Shimizu T, Owada T, Nakamura Y, Iwaya S, Yamauchi H, et al. Adaptive Servo Ventilation Improves Cardiac Dysfunction and Prognosis in Chronic Heart Failure Patients With Cheyne-Stokes Respiration. Int Heart J. 2011;52(4):218–23.
Oldenburg O, Bitter T, Lehmann R, Korte S, Dimitriadis Z, Faber L, et al. Adaptive servoventilation improves cardiac function and respiratory stability. Clin Res Cardiol. 2011;100(2):107–15.
Oldenburg O, Bitter T, Wellmann B, Fischbach T, Efken C, Schmidt A, et al. Trilevel adaptive servoventilation for the treatment of central and mixed sleep apnea in chronic heart failure patients. Sleep Med. 2013;14(5):422–7.
Morgenthaler TI, Kuzniar TJ, Wolfe LF, Willes L, McLain WC, Goldberg R. The Complex Sleep Apnea Resolution Study: A Prospective Randomized Controlled Trial of Continuous Positive Airway Pressure Versus Adaptive Servoventilation Therapy. Sleep. 2014;37(5):927–34.
Birner C, Series F, Lewis K, Benjamin A, Wunderlich S, Escourrou P, et al. Effects of Auto-Servo Ventilation on Patients with Sleep-Disordered Breathing, Stable Systolic Heart Failure and Concomitant Diastolic Dysfunction: Subanalysis of a Randomized Controlled Trial. Respiration. 2013;87(1):54–62.
Hetzenecker A, Escourrou P, Kuna ST, Series F, Lewis K, Birner C, et al. Treatment of sleep apnea in chronic heart failure patients with auto-servo ventilation improves sleep fragmentation: a randomized controlled trial. Sleep Med. 2016;17:25–31.
Toyama T, Hoshizaki H, Kasama S, Miyaishi Y, Kan H, Yamashita E, et al. Adaptive servo-ventilation therapy improves cardiac sympathetic nerve activity, cardiac function, exercise capacity, and symptom in patients with chronic heart failure and Cheyne-Stokes respiration. J Nucl Cardiol. 2017;24(6):1926–37.
O’Connor CM, Whellan DJ, Fiuzat M, Punjabi NM, Tasissa G, Anstrom KJ, et al. Cardiovascular Outcomes With Minute Ventilation-Targeted Adaptive Servo-Ventilation Therapy in Heart Failure: The CAT-HF Trial. J Am Coll Cardiol. 2017;69(12):1577–87.
Daubert MA, Whellan DJ, Woehrle H, Tasissa G, Anstrom KJ, Lindenfeld J, et al. Treatment of sleep-disordered breathing in heart failure impacts cardiac remodeling: Insights from the CAT-HF Trial. Am Heart J. 2018;201:40–8.
Cantero C, Adler D, Pasquina P, Uldry C, Egger B, Prella M, et al. Adaptive Servo-Ventilation: A Comprehensive Descriptive Study in the Geneva Lake Area. Front Med. 2020;7:105.
Tamisier R, Damy T, Bailly S, Davy JM, Verbraecken J, Lavergne F, et al. Adaptive servo ventilation for sleep apnoea in heart failure: the FACE study 3-month data. Thorax. 2022;77(2):178–85.
Baumert M, Linz D, Pfeifer M, Tafelmeier M, Felfeli P, Arzt M, et al. Hypoxaemic burden in heart failure patients receiving adaptive servo-ventilation. ESC Heart Failure. 2023;10(6):3725–8.
Cowie MR, Woehrle H, Wegscheider K, Angermann C, d’Ortho M-P, Erdmann E, et al. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure. N Engl J Med. 2015;373(12):1095–105.
Lyons OD, Floras JS, Logan AG, Beanlands R, Cantolla JD, Fitzpatrick M, et al. Design of the effect of adaptive servo-ventilation on survival and cardiovascular hospital admissions in patients with heart failure and sleep apnoea: the ADVENT-HF trial: Study design of ADVENT-HF. Eur J Heart Fail. 2017;19(4):579–87.
Bradley TD, Logan AG, Lorenzi Filho G, Kimoff RJ, Durán Cantolla J, Arzt M, et al. Adaptive servo-ventilation for sleep-disordered breathing in patients with heart failure with reduced ejection fraction (ADVENT-HF): a multicentre, multinational, parallel-group, open-label, phase 3 randomised controlled trial. Lancet Respirat Med. 2023 S2213260023003740.
Randerath WJ, Javaheri S. Adaptive Servoventilation in Central Sleep Apnea. Sleep Med Clin. 2014;9(1):69–85.
Herkenrath SD, Randerath WJ. More than Heart Failure: Central Sleep Apnea and Sleep-Related Hypoventilation. Respiration. 2019;98(2):95–110.
Parthasarathy S, Arzt M, Javaheri S. A call for precision medicine: Facing the challenge of sleep-disordered breathing in heart failure. Sleep Med. 2023;112:129–31.
Bassetti CLA, Randerath W, Vignatelli L, Ferini-Strambi L, Brill A-K, Bonsignore MR, et al. EAN/ERS/ESO/ESRS statement on the impact of sleep disorders on risk and outcome of stroke. Eur J Neurol. 2020;27(7):1117–36.
Brill A-K, Rösti R, Hefti JP, Bassetti C, Gugger M, Ott SR. Adaptive servo-ventilation as treatment of persistent central sleep apnea in post-acute ischemic stroke patients. Sleep Med. 2014;15(11):1309–13.
Duss SB, Brill A-K, Baillieul S, Horvath T, Zubler F, Flügel D, et al. Effect of early sleep apnoea treatment with adaptive servo-ventilation in acute stroke patients on cerebral lesion evolution and neurological outcomes: study protocol for a multicentre, randomized controlled, rater-blinded, clinical trial (eSATIS: early Sleep Apnoea Treatment in Stroke). Trials. 2021;22(1):83.
Pépin J-LD, Woehrle H, Liu D, Shao S, Armitstead JP, Cistulli PA, et al. Adherence to Positive Airway Therapy After Switching From CPAP to ASV: A Big Data Analysis. J Clin Sleep Med. 2018;14(01):57–63.
Eulenburg C, Wegscheider K, Woehrle H, Angermann C, d’Ortho M-P, Erdmann E, et al. Mechanisms underlying increased mortality risk in patients with heart failure and reduced ejection fraction randomly assigned to adaptive servoventilation in the SERVE-HF study: results of a secondary multistate modelling analysis. Lancet Respir Med. 2016;4(11):873–81.
Randerath W, Schumann K, Treml M, Herkenrath S, Castrogiovanni A, Javaheri S, et al. Adaptive servoventilation in clinical practice: beyond SERVE-HF? ERJ Open Res. 2017;3(4):00078–2017.
Brill A-K, PichlerHefti J, Geiser T, Ott SR. The SERVE-HF safety notice in clinical practice – experiences of a tertiary sleep center. Sleep Med. 2017;37:201–7.
Arzt M, Munt O, Pépin J-L, Heinzer R, Kübeck R, Von Hehn U, et al. Registry on the Treatment of Central and Complex Sleep-Disordered Breathing with Adaptive Servo-Ventilation (READ-ASV): protocol and cohort profile. ERJ Open Res. 2023;9(2):00618–2022.
Malfertheiner MV, Lerzer C, Kolb L, Heider K, Zeman F, Gfüllner F, et al. Whom are we treating with adaptive servo-ventilation? A clinical post hoc analysis. Clin Res Cardiol. 2017;106(9):702–10.
Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Töpfer V. Sleep-disordered breathing in patients with symptomatic heart failure A contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail. 2007;9(3):251–7.
Javaheri S. Sleep disorders in systolic heart failure: A prospective study of 100 male patients The final report. Intl J Cardiol. 2006;106(1):21–8.
Paulino A, Damy T, Margarit L, Stoïca M, Deswarte G, Khouri L, et al. Prevalence of sleep-disordered breathing in a 316-patient French cohort of stable congestive heart failure. Arch Cardiovasc Dis. 2009;102(3):169–75.
White DP. Pathogenesis of Obstructive and Central Sleep Apnea. Am J Respir Crit Care Med. 2005;172(11):1363–70.
Solin P, Roebuck T, Johns DP, Haydn Walters E, Naughton MT. Peripheral and Central Ventilatory Responses in Central Sleep Apnea with and without Congestive Heart Failure. Am J Respir Crit Care Med. 2000;162(6):2194–200.
Webster LR, Choi Y, Desai H, Webster L, Grant BJB. Sleep-Disordered Breathing and Chronic Opioid Therapy. Pain Med. 2008;9(4):425–32.
Piovezan RD, Kase C, Moizinho R, Tufik S, Poyares D. Gabapentin acutely increases the apnea–hypopnea index in older men: data from a randomized, double-blind, placebo-controlled study. J Sleep Res. 2017;26(2):166–70.
George CFP, Feldman N, Inhaber N, Steininger TL, Grzeschik SM, Lai C, et al. A safety trial of sodium oxybate in patients with obstructive sleep apnea: Acute effects on sleep-disordered breathing. Sleep Med. 2010;11(1):38–42.
Perogamvros L, Pépin JL, Thorens G, Mégevand P, Claudel E, Espa F, et al. Baclofen-Associated Onset of Central Sleep Apnea in Alcohol Use Disorder: A Case Report. Respiration. 2015;90(6):507–11.
Guichard K, Micoulaud-Franchi J-A, McGonigal A, Coulon P, Sureau C, Ghorayeb I, et al. Association of Valproic Acid With Central Sleep Apnea Syndrome: Two Case Reports. J Clin Psychopharmacol. 2019;39(6):681–4.
Giannoni A, Borrelli C, Gentile F, Mirizzi G, Coceani M, Paradossi U, et al. Central apnoeas and ticagrelor-related dyspnoea in patients with acute coronary syndrome. Euro Heart J Cardiovasc Pharmacother. 2021;7(3):180–8.
Meurin P, Ben Driss A, Defrance C, Dumaine R, Weber H, Renaud N, et al. Central sleep apnea after acute coronary syndrome and association with ticagrelor use. Sleep Med. 2021;80:39–45.
Johnson KG, Johnson DC. Frequency of sleep apnea in stroke and TIA patients: a meta-analysis. J Clin Sleep Med. 2010;6(2):131–7.
Baou K, Mermigkis C, Minaritzoglou A, Vagiakis E. Complex sleep apnea after full-night and split-night polysomnography: the Greek experience. Sleep Breath. 2018;22(3):713–9.
Kouri I, Kolla BP, Morgenthaler TI, Mansukhani MP. Frequency and outcomes of primary central sleep apnea in a population-based study. Sleep Med. 2020;68:177–83.
Takama N, Kurabayashi M. Effect of Adaptive Servo-Ventilation on 1-Year Prognosis in Heart Failure Patients. Circ J. 2012;76(3):661–7.
Shapiro CM, Chung SA, Wylie PE, Hossain NK, Holle RHO, Rosenberg RP, et al. Home-use servo-ventilation therapy in chronic pain patients with central sleep apnea: initial and 3-month follow-up. Sleep Breath. 2015;19(4):1285–92.
Momomura S, Seino Y, Kihara Y, Adachi H, Yasumura Y, Yokoyama H, et al. Adaptive Servo-Ventilation Therapy for Patients With Chronic Heart Failure in a Confirmatory, Multicenter, Randomized. Controlled Study Circ J. 2015;79(5):981–90.
Piccini JP, Pokorney SD, Anstrom KJ, Oldenburg O, Punjabi NM, Fiuzat M, et al. Adaptive servo-ventilation reduces atrial fibrillation burden in patients with heart failure and sleep apnea. Heart Rhythm. 2019;16(1):91–7.
Cowie MR, Woehrle H, Wegscheider K, Vettorazzi E, Lezius S, Koenig W, et al. Adaptive servo-ventilation for central sleep apnoea in systolic heart failure: results of the major substudy of SERVE-HF. Eur J Heart Fail. 2018;20(3):536–44.
Tamisier R, Pepin J, Cowie MR, Wegscheider K, Vettorazzi E, Suling A, et al. Effect of adaptive servo ventilation on central sleep apnea and sleep structure in systolic heart failure patients: polysomnography data from the SERVE-HF major sub study. J Sleep Res. 2022;31(6): e13694.
Sun P, Porter K, Randerath W, Jarjoura D, Khayat R. Adaptive servo-ventilation and mortality in patients with systolic heart failure and central sleep apnea: a single-center experience. Sleep Breath. 2023. https://doi.org/10.1007/s11325-023-02807-2.
Kida H, Hikoso S, Uruno T, Kusumoto S, Yamamoto K, Matsumoto H, et al. The efficacy and safety of adaptive servo-ventilation therapy for heart failure with preserved ejection fraction. Heart Vessels. 2023;38(12):1404–13.
Tamisier R, Damy T, Bailly S, Goutorbe F, Davy J-M, Lavergne F, et al. FACE study: 2-year follow-up of adaptive servo-ventilation for sleep-disordered breathing in a chronic heart failure cohort. Sleep Med. 2024;113:412–21.
Arzt M, Munt O, Pépin J-L, Heinzer R, Kübeck R, von Hehn U, et al. Effects of Adaptive Servo-Ventilation on Quality of Life: The READ-ASV Registry. Annals ATS. 2024. https://doi.org/10.1513/AnnalsATS.202310-908OC.
Funding
This review article did not receive funding.
Author information
Authors and Affiliations
Contributions
S. M, S.J, S.J, R.K and W.R all contributed substantially to writing the main manuscript text and preparing figures and tables.
Corresponding author
Ethics declarations
The Section Editor for the topical collection is Sleep and Cardiovascular Disease. Please note that Section Editor Rami Khayat was not involved in the editorial process of this article as he is a co-author.
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
All reported studies/experiments with human or animal subjects performed by the authors have been previously published and compiled with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Matthes, S., Javaheri, S., Javaheri, S. et al. Central Sleep Apnea: An Update of Current Treatment and the Role of Positive Pressure Devices. Curr Sleep Medicine Rep (2024). https://doi.org/10.1007/s40675-024-00311-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s40675-024-00311-x