
Abstract
Purpose of review
This study aims to summarize the current body of literature on the relationship between various toxic metals exposures (i.e., aluminum, antimony, arsenic, beryllium, cadmium, chromium, lead, manganese, and nickel) and autism spectrum disorder (ASD), with a focus on potential sex differences in these associations.
Recent findings
Sex differences in ASD diagnosis and mutagenic effects of toxic exposures indicate that sex differences may play a major part in the causal relationship of any potential associations seen; however, we were only able to find three studies that reported on sex differences in observed associations with toxic metals exposure and ASD. We also found several studies investigating associations between ASD and metals exposures, including 11 on aluminum, 6 on antimony, 15 on arsenic, 5 on beryllium, 17 on cadmium, 11 on chromium, 25 on lead, 14 on manganese, and 13 on nickel with markers of exposure in hair, urine, blood, teeth, fingernails, and air pollution. Results for each metal were conflicting, but studies on cadmium and lead yielded the highest proportion of studies with positive results (72% and 36%, respectively).
Summary
Based on our examination of existing literature, the current evidence warrants a considerable need for evaluations of sex differences in future studies assessing the association between metals exposures and ASD. Additionally, failure to account for potential sex differences could result in bias and misinterpretation of exposure-disease relationships.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental disorder that manifests in early childhood or infancy and is characterized by impairments in communication and social interaction [1]. Although the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) was released in 2013 [1], recent research has used criteria based on the DSM-IV-TR for diagnosis of ASD [2]. According to the most recent report from the Centers for Disease Control and Prevention (CDC) surveillance, ASD prevalence estimates have steadily increased from 1 in 150 in the year 2000 to a current 1 in 68 [3]; however, these increases could be due to changes in diagnosis or familiarity of symptoms.
The skewed sex distribution in ASD is well documented with a 5:1 male to female ratio in overall diagnosis [3], and less severe symptomology in females [4,5,6]. Because girls often develop language skills earlier than boys [7] and exhibit better understanding of non-verbal gestures [8], it has been hypothesized that girls possess a protective factor from developing ASD. However, there has been a recognized potential sex bias in assessment of neurodevelopmental disorders due to frequency of comorbidities in boys [9, 10]. Additionally, cerebral abnormalities and physical anomalies have been more commonly observed in males with ASD [11], reflecting underlying genetic variances, and increasing interest in potential reasons for sex differences in ASD.
Although the etiology of ASD is not well understood [12], one common hypothesis is that this disorder is a result of interplaying genetic factors and environmental triggers [13, 14]. In particular, due to prior documented associations between metals exposures and adverse neurodevelopment [15], along with the ability of certain metals, including lead, iron, manganese, and mercury, to easily cross the blood-brain barrier [16], metals have been an exposure of interest in the investigation of risk factors for ASD [17,18,19,20, 21••]. Exposures in infancy and early childhood may also differ from other time periods in life, as well as by sex due to exposure from parental-imposed gender roles, such as jewelry worn in the pierced ears of girls.
Several studies have also investigated the ability of children with ASD to process metals and have shown a reduced capacity to metabolize metals in children with ASD [22, 23]. There is also a growing concern over differences in associations between metals and ASD for males versus females. Research has indicated that exposure to various toxicants, including metals, may elicit epigenetic changes with potential implication for ASD [24, 25]. Furthermore, children with ASD have a higher rate of mutations in genes involved in preventing oxidative stress [26, 27], potentially increasing the occurrence of oxidative stress resulting from environmental exposures. Sex-specific genetic mutation could be one underlying reason for the sex-specific difference in ASD prevalence and severity [28].
Distinguishing the impact of biological and social differences between males and females could assist in deciphering the mechanisms for potential associations between metals exposures and ASD diagnosis. The purpose of this review is to (1) summarize the current body of literature on the relationship between ASD and various toxic metals: aluminum, antimony, arsenic, beryllium, cadmium, chromium, lead, manganese, and nickel, herein referred to as “toxic metals”; (2) discuss the sex differences in absorption, metabolism, and storage of metals; (3) summarize previous investigations of sex difference in metals exposure and ASD; and (4) highlight the need for research investigating the influence of effect modification by sex in studies of metals exposures and ASD. Although we will present information from epidemiologic studies from the past 15 years, we will focus our discussion on studies from the past 5 years. As there have been numerous previous reviews of the association between mercury and ASD [29,30,31], we will not present information on this particular metal exposure. We also do not include information on metals commonly consumed as dietary supplements, such as iron and zinc.
Methods
We used the following summarized participants, exposures, comparator, and outcome (PECO) guidelines: (1) participants were children (younger than 18 years of age); (2) exposure to toxic metals was measured via biological samples (i.e., urine, blood, hair, teeth, or nails) or estimated proxy measurements (i.e., air concentrations); (3) comparators were children without an ASD diagnosis or designation; and (4) outcome was ASD diagnosis or special education autism classification (based on DSM-IV criteria) on a dichotomous scale.
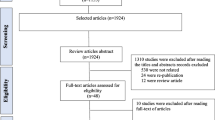
A literature search for manuscripts evaluating the association between exposures to toxic metals was conducted using PubMed, Ovid Medline, and Web of Science for articles on human subjects between January 2002 and March 2017. Queries of titles, abstracts, and key words included “autism,” “autism spectrum disorder,” “neurodevelopmental disorder,” “ASD,” AND “metals,” “trace elements,” “aluminum,” “antimony,” “arsenic,” “beryllium,” “cadmium,” “chromium,” “lead,” “manganese,” or “nickel.” All non-human studies, including animal and mode-of-action, were eliminated. Case reports, secondary studies (i.e., reviews and commentaries), preliminary studies analyzing the same sample using the same biomarker, and studies not in English were removed from the review inclusion list. There were a total of 32 original research articles that met these criteria.
Measures of Exposure and Outcome
In this review, we included case-control and cross-sectional studies, many of which measured metal exposures using biomarkers obtained after ASD diagnosis or special education ASD designation, including blood (i.e., red blood cells, whole blood, and serum), urine, hair, teeth, fingernails, and area-based exposures (e.g., estimated air pollutant concentrations during or prior to birth). Studies also used differing methods of ASD classification. While most used DSM-IV classification either based on clinician observation or medical records review, others used any questionnaire responses, special education designations of autism, or a myriad of ASD assessments: Autism Diagnostic Observation Schedule (ADOS), Autism Diagnostic Interview-Revised (ADI-R), Childhood Autism Rating Scale (CARS), Social Communication Questionnaire (SCQ), Modified Checklist for Autism in Toddlers (M-CHAT), Autism Research Institute (ARI) Form E2, and Autism Behavioral Checklist (ABC).
Results
In this section, we will present results for studies assessing relationships between ASD and the previously listed nine metals of interest according to the measurement of exposure used in each study (i.e., hair, urine, blood, teeth and fingernails, and ambient air pollution). Each Appendix table lists the metals measured in recent studies using said markers and summarized results from each manuscript.
ASD and Hair Metal Concentrations
Human hair has been found to be a mode of excretion of metals, with 10 times higher accumulated concentrations than levels seen in blood and urine [32]. Because it grows about 10 mm per month, it is considered to be more indicative of exposures over several months [32]. However, for some metals, concentrations in hair, similar to toenail, do not necessarily correlate with exposure levels, potentially limiting the utility of hair as a biomarker. For instance, cadmium levels in hair and toenail do not correlate with smoking and tobacco smoke exposure, which is one of the best-known sources of cadmium [33]. We included nine studies reporting on ASD and aluminum in hair. There were two studies with slightly higher hair aluminum concentrations that were not statistically significant (Appendix Table 1) [23, 34]. However, a study in Egypt reported significantly higher mean (SD) aluminum concentrations in hair of cases compared to controls [59.19 (37.98) mg/kg in cases and 16.78 (17.31) mg/kg in controls; p = 0.0001] [35], while a different study in Oman also reported higher median (IQR) concentrations in cases compared to controls [2.3 (0.3) μg/g in cases; 1.2 (0.2) μg/g in controls; p = 0.002] [36]. Conversely, five of the studies included in this review reported slightly higher hair aluminum concentrations in controls than cases, though none of these inverse results were statistically significant [37,38,39,40,41]. There were three studies assessing ASD and hair antimony concentrations [39,40,41]. Although all reported higher hair antimony concentrations in cases, only one reported statistically significant results [mean (SD) = 0.02 (0.01) ppm in cases and 0.002 (0.007) ppm in controls; p < 0.05] [40].
Results for hair arsenic analyses varied greatly. Of the eight studies evaluating associations between hair arsenic concentrations and ASD, over half reported higher hair concentrations in ASD cases compared to controls [18, 23, 40, 41], and the other half reported lower hair concentrations in cases compared to controls [34, 38, 39, 42]. Of those indicating higher concentrations in cases, only two were significantly higher [18, 40], while two contrasting studies indicated significantly higher hair arsenic concentrations in controls [38, 42]. Regarding the four studies with beryllium concentrations in hair [23, 38, 39, 41], only Skalny et al. (2017) reported statistically significant results, with concentrations higher in controls compared to cases [23]. We included nine studies of cadmium exposures through hair measurements [23, 34, 36,37,38,39,40,41,42]; four of which reported significantly higher hair concentrations in cases versus controls [36, 38, 40, 42]. All others reported null results, with three having slightly higher hair cadmium concentrations in controls compared to cases [39, 41, 42].
There were five studies investigating ASD and hair chromium levels [23, 34, 36, 38, 39]. Although one study in Arizona showed slightly higher hair chromium concentrations in cases than in controls [39], another in Oman reported a significantly higher median (IQR) concentration in cases of 23.6 (2.3) μg/g compared to 9.9 (1.6) μg/g in controls (p = 0.001) [36]. All other studies reported higher hair chromium concentrations in controls than in cases [23, 34, 38], with Skalny et al. (2017) reporting statistically significant results [median (IQR) = 0.155 (0.090–0.360) μg/g in controls and 0.110 (0.082–0.156) μg/g in cases; p = 0.003] [23].
Lead is one of the most recognized neurotoxicants associated with neurodevelopmental impairment [43]. Due to its persistence, ability to cause adverse outcomes at even low levels, and capacity to cross the blood-brain barrier, it has been of substantial interest to researchers investigating environmental risk factors for ASD. This metal comprises the largest list of manuscripts for our review, with 10 reporting results on hair concentrations [18, 23, 34, 35, 37, 39,40,41,42, 44]. Half of these studies reported null results [18, 23, 34, 37, 39], with three being inverse [23, 37, 39], but four did report higher hair lead concentrations in ASD cases [35, 40, 41, 44]. Kern et al. (2007) reported significantly higher hair lead concentrations in controls than cases [mean (SD) = 0.20 (0.37) μg/g in controls and 0.19 (0.65) μg/g in cases; p < 0.05] [42].
A total of six studies looked at hair concentrations of manganese and ASD [18, 23, 34, 38,39,40], with all but one producing null associations. Notably, Al-Ayadhi et al. (2005) was the only study of hair concentrations to report statistically significant results, with higher concentrations in controls than cases [mean (SD) = 0.6 (0.06) ppm in controls and 0.33 (0.04) ppm in cases; p < 0.05] [40]. There were also seven studies of hair nickel concentrations [18, 34, 36, 38,39,40, 45], and three of those reported slightly higher hair nickel concentrations in controls than in cases [38, 40, 45]. The study in Oman, however, reported significantly higher hair nickel concentrations (p = 0.003) in cases compared to controls [36].
Reviewing all of the studies of ASD and hair metals concentrations, we were only able to find one that looked at sex differences in these associations. De Palma et al. (2012) reported higher cadmium concentrations in boys with ASD in stratified analysis [median (IQR) = 0.0003 (0.0003–0.02) μg/g in controls; 0.01 (0.006–0.03) μg/g in cases, p = 0.006] [34].
ASD and Urine Metal Concentrations
As a biomarker, urine serves primarily as a reflection of relatively recent exposure levels, although if exposure is continuous, urine can be useful to assess long-term exposure [46]. Urine itself is a typical elimination method for metals from the body, and thus serves as a marker for general day to day exposure for most metals [32]. Cadmium is the exception, where most of the accumulation in the body is in the kidney, which subsequently is highly related to cadmium in urine [47]. Appendix Table 2 shows six studies investigating associations between ASD and urine concentrations of metals. Of the three with urine aluminum concentrations, two studies indicated slightly higher concentrations in cases than controls, but none of these results were statistically significant [38, 39]. There was only one study of urine antimony concentrations, which found the same mean (SD) in cases and controls of 0.17 (0.25) μg/g creatinine [17]. Although all studies assessing urinary arsenic concentrations reported slightly higher levels in cases compared to controls, none of the effect estimates reported were statistically significant [17, 38]. The study on Saudi Arabian children was also the only to report on urine beryllium concentrations, producing null results [mean (SD) = 0.28 (0.35) μg/g in controls and 0.67 (1.44) μg/g creatinine in cases; p = 0.2] [38]. Of the five studies with urinary cadmium concentrations, four reported slightly higher concentrations in cases [17, 37, 48, 49], while one had slightly higher concentrations in controls [38], but none of the results were statistically significant. Blaurock-Busch et al. (2011) reported slightly higher urinary chromium concentrations in children in Saudi Arabia [38], and Yorbik et al. (2010) reported significantly higher mean (SD) creatinine-adjusted concentrations in cases of 26.4 (16.07) μg/g compared to controls with 11.27 (5.04) μg/g in Turkish children (p < 0.001) [48]. Of the five studies with urinary lead concentrations (which is not considered an established biomarker of lead exposure), two reported inverse associations [37, 48], with one of these having statistically significant results [mean (SD) = 0.73 (0.29) ppb/mL in controls and 0.71 (0.29) ppb/mL cases; p = 0.446] [48]. Additionally, of the three studies indicating higher urinary lead concentrations in cases than controls [17, 49, 50], both studies in Arizona reported statistically significant results [17, 50]. The higher mean urinary manganese concentration seen in cases in the one study investigating this metal in urine was not statically significant [mean (SD) = 4.81 (3.67) μg/g in controls and 7.32 (7.22) μg/g creatinine in cases; p = 0.13] [38]. Furthermore, results for two studies of urinary nickel concentrations were similar [17, 38]. There were no studies that evaluated sex differences in urine metals concentrations and ASD.
ASD and Blood Metal Concentrations
Blood metal concentrations are a more consistent biomarker of metals absorbed in the body, especially for metals that are particularly found in red blood cells such as lead and cadmium. As an essential mechanism of transporting metals, blood is commonly assumed to have a direct correlation of measurement from the deposition in sensitive tissues. Blood is generally thought to have a longer overall half-life than urine, except for cadmium for which urine cadmium has a longer half-life than blood. Blood metals in general have a half-life of about 1 month [51]. The two studies of blood aluminum reported slightly higher concentrations in controls compared to cases (Appendix Table 3) [37, 52]. Adams et al. (2013) investigated arsenic concentrations in both whole blood and red blood cells, and found slightly higher concentrations in controls for both biomarkers, though neither was significant [17]. A study of children in Jamaica (2012) also observed significantly higher mean whole blood arsenic concentrations in controls compared to ASD cases after adjusting for water source, parental education, SES, maternal age, fruit and vegetable consumption, and frequency of seafood consumption per week as potentially confounding factors (4.44 μg/L in controls and 4.01 μg/L in cases; p = 0.01) [53]. In the same study samples, Adams et al. (2013) found significantly higher mean (SD) blood cadmium concentrations in controls [0.79 (0.23) μg/L in controls and 0.64 (0.23) μg/L in cases; p = 0.003] [17], while Rahbar et al. (2014) conversely found slightly higher blood cadmium concentrations in cases compared to controls [54]. The one study of blood chromium concentrations and ASD showed only slight differences between cases and controls [55]. There were five studies with either whole blood or red blood cell lead concentrations [17, 37, 56,57,58]. Although most studies of blood lead levels reported null results, the most recent study conducted in a small sample of children ages 3–12 years in Saudi Arabia reported significantly higher mean blood concentrations in cases versus controls [mean (SD) = 6.04 (1.11) μg/dL in cases and 3.89 (0.88) μg/dL in controls, p < 0.001]. Adam et al. (2013) reported null results for the analysis of whole blood concentrations, but analysis of red blood cells, which is the primary site of deposition of blood lead, revealed a statistically significant positive association (p = 0.002) [17]. Neither of the two studies reporting blood manganese concentrations showed strong differences between cases and controls [55, 59]. Although 7 of the 10 papers indicated null associations between blood metals concentrations and ASD, none of the studies indicated additional analyses to evaluate potential sex differences in these associations.
ASD and Metal Concentrations in Teeth and Fingernails
Nail and teeth biomarkers are typically used to assess cumulative exposure (Appendix Table 4). Metals in nails typically have a half-life of about 7–12 months [60]. However, dependent upon the tooth and the area of the tooth sampled for the study, whole deciduous teeth can be used as a reflection of exposure in the first few years of life and including prenatal exposures [61]. Whole deciduous teeth typically provide average exposure measurements over the years of growth of the teeth, but measuring only certain regions of the enamel or dentin allows for more specific pre- or post-natal exposures [61]. There was only one study in India that reported on potential associations of lead concentrations using fingernails as a biomarker; however, results were only significant for the relationship seen in children with lower functioning ASD [mean (SD) = 16.2 (1.94) μg/g in controls and 26.38 (3.16) μg/g in low functioning cases; p < 0.00] [44]. Because lead can deposit in calcium-rich tissues, deciduous teeth have been suggested as one of the most reliable biomarkers for determining early-life lead exposures. Nevertheless, both studies of teeth lead concentrations reported null results with minimally higher concentrations in controls than cases [62, 63]. Furthermore, Abdullah et al. (2012) also reported null associations with measures of teeth manganese and ASD with higher concentrations in controls than cases [63]. None of the studies included in this review evaluated sex differences in metals concentrations of fingernails or teeth and ASD.
ASD and Ambient Metal Concentrations
The prior mentioned studies provide important contributions to ASD research; however, the biomarkers of exposures may measure levels of exposures following ASD diagnosis. For example, previous studies have demonstrated that food preferences and differences in diet for children with ASD, including fruit, vegetable, and seafood consumption, could affect blood metal levels [53, 54, 64, 65]. Though exposure assessment through perinatal air concentrations may not be on an individual level, it provides a more temporal association for measurement through physical environment, avoiding some of the potential reverse causality and other limitations that biomarkers have [66]. For this reason, we included six studies investigating the association between ASD and hazardous air pollutants in Appendix Table 5 [19, 20, 21••, 67,68,69]. Only two studies examined estimated ambient air exposures to antimony on or around birth years [21••, 69]. Of these, Roberts et al. (2013) found somewhat increased odds of ASD in those living in areas with the highest quintile concentrations of ambient antimony compared to those in the lowest quintile [odds ratio (OR) = 1.5, 95% CI 1.0, 2.3]. Notably, there were five area-based studies of estimated ambient air arsenic concentrations around pregnancy or infancy, with none reporting statistically significant results [19, 20, 21••, 67, 68]. Kalkbrenner et al. (2010) was the only study of pre-diagnostic beryllium exposures in ambient air and reported inverse, yet not significant associations (OR = 0.9, 95% CI 0.4–2.1 for 80th vs. 20th percentile) [19]. Ambient cadmium exposure during pregnancy or infancy was evaluated by four case-control studies [19, 20, 21••, 68]. Both Windham et al. (2006) and Roberts et al. (2013) reported approximated 50% increase in odds for children born in areas with the highest percentile air cadmium concentrations compared to those in the lowest percentile [20, 21••]. Of the four studies of ambient chromium air concentrations, increase in odds of ASD ranged from 12 to 52%, with no statistical significance [19, 20, 21••, 68]. Lead exposure also frequently occurs through inhalation of ambient air, but only two of the six studies investigating ambient air concentrations during pregnancy or infancy reported significant increases in odds (OR = 1.6, 95% CI 1.1–2.3 for highest vs. lowest quintile) [21••] and prevalence [prevalence ratio (PR) = 1.36, 95% CI 1.18–1.57 for highest vs. lowest quartile] [67]. Additionally, Roberts et al. (2013) was the only study out of five with ambient manganese air concentrations to report a significant association between birth residence in areas with the highest quintile of ambient manganese concentrations compared to those with the lowest quintile exposure (OR = 1.5, 95% CI 1.1, 2.2) [21••]. Most notable is results reported for the five studies of ambient nickel concentrations in the USA [19, 20, 21••, 68, 69], with three of these reporting significantly increased risk of ASD in children born in area with greater air nickel concentrations [20, 21••, 69].
Two of the studies investigating ambient metal concentrations reported on sex-stratified analyses of metals concentrations and ASD [19, 21••]. Kalkbrenner et al. (2010) reported that point estimates were not consistently higher for either sex in their stratified analysis, but some differences were seen in mercury compounds [19]. The most extensive and thorough report of sex differences was seen in Roberts et al. (2013), who also reported a prominent difference in significance of the relationship between highest quintile concentrations versus lowest quintile concentrations of overall metals exposure in boys that was not seen in girls (OR = 1.7, 95% CI 1.1, 2.6 in boys and OR = 0.8, 95% CI 0.2, 2.4 in girls) [21••]. Additionally, they found positive associations for ASD in boys for individual metals, including antimony (OR = 1.7, 95% CI 1.1, 2.7), cadmium (OR = 1.6, 95% CI 1.1, 2.4), lead (OR = 1.7, 95% CI 1.2, 2.6), manganese (OR = 1.5, 95% CI 1.0, 2.3), mercury (OR = 1.6, 95% CI 1.0, 2.4), and nickel (OR = 1.9, 95% CI 1.2, 2.9) [21••]. Interestingly, in girls all associations were null, with inverse ORs seen for cadmium, lead, mercury, and nickel [21••].
Discussion
Sex Difference in Metals Exposures and ASD
During our literature search, we were only able to find three studies of ASD and metal exposures that reported potential effect modification due to sex differences [19, 21••, 34]. A study of hair metals concentrations found positive associations between ASD in boys, with particularly higher lithium and cadmium concentrations in stratified analyses [34]. Two studies of ambient metals concentrations and ASD reported on sex differences, with one reporting no statistically significant sex differences [19]. However, the study utilizing responses from the Nurses’ Health Study found effect modification by sex in the investigation of ASD and ambient concentrations of all metals combined, as well as some metals independently [21••].
Metals are broadly distributed in the environment with various sources and routes of exposure. Each is processed, stored, and metabolized at its own rate, but most can accumulate in the food we ingest and in our own tissues. For example, exposure to chromium is predominantly via occupational inhalation. However, the primary source of exposure to aluminum and beryllium is food consumption, and both are generally ubiquitous in the environment and inhaled in small amounts each day [70, 71]. Although both aluminum and beryllium can be absorbed in blood, most is expelled in feces and urine [70, 71]. In contrast, the most common exposure to arsenic and antimony is through drinking water, which makes exposure to them particularly modifiable [70, 72]. Furthermore, cadmium and nickel can settle in surface water and be absorbed into leafy greens, root vegetables, and grains [73]. The most knowingly detrimental metal presented in this review is lead, which can deposit in normally calcium-rich tissues, including bones, then release slowly into the blood over decades [74]. This endogenous exposure can result in high levels of lead during bodily processes that increase bone resorption, such as pregnancy and lactation [75, 76].
It is important to note that most of the exposure measures in the studies included in this review, such as hair, urine, and blood, reflect relatively short-term exposures and were collected after ASD status was determined. Thus, with the exception of air and teeth concentrations, no temporal association can be assumed and the reported results may actually be an indicator of exposures due to differing diets, behaviors, or ability to process and metabolize toxicants. The one study of teeth measures of metals reported null results, but several results from the studies of ambient air metal concentrations showed positive associations with ASD.
Sex Differences in Metabolism and Storage of Metals
Metals such as lead interact heavily with calcium in the body [77], and a recent study looking at metal interactions via calcium pathways showed broader differences in body stores of metals in children during puberty [78]. Several metals, including lead, cadmium, arsenic, thallium, and copper, can also affect levels of free testosterone and estradiol [79,80,81], Differential levels of sex hormones also result in sex-specific variation in development of the brain. Studies have reported sex differences in prenatal testosterone levels and later development of behavioral disorders [82]. Furthermore, individuals with ASD had been shown to have increased levels of testosterone, dehydroepiandrosterone, and androstenedione [83]. Thus, it is plausible that sex-specific differences in hormone levels could be a risk factor for ASD before birth and during infancy by further complicating the interaction of hormones with metals, as accumulation and subsequent biological measures for certain metals can be impacted by disruptions and differences in storage and metabolism.
With diet being a common source of metals exposure, the body burden of metals may be inversely impacted by the uptake of nutritionally essential metals [84, 85], with differing sex-dependent nutritional needs typically arising during different ages and increasing absorption and remobilization from storage sites in the body [76, 86,87,88]. Sex differences in absorption, metabolism, and accumulation from dietary sources are well-established [89,90,91]. Additionally, general environmental exposure levels can be dependent upon sex and gender-specific behaviors (i.e., wearing jewelry, cosmetics, nail polish, and personal care products), even in children.
Regarding storage, metals such as lead interact heavily with calcium in the body [77]. A recent study looking at strontium, which also interacts with the body via calcium pathways, showed that this effect might translate into further differences in body stores of metals in children based on puberty status [78]. Puberty would initiate many processes that play a role in both the storage of metals, such as increased bone formation, and their action in the body. Cadmium has also been shown to interact with sex hormones and cause an increase in testosterone production in women [81]. Another study showed that several metals, including cadmium, arsenic, thallium, and copper, have an impact on sexual maturation and hormone levels [79]. Additionally, lead is well known to affect hormone levels of free testosterone and estradiol [79, 80]. This further complicates the interaction of hormones with metals, as accumulation and biomarkers for certain metals can be affected by disruptions in storage and metabolism of other metals.
Sex-Specific Genetic Risk
There is also evidence of hereditary factors and sex-specific genetic effects, which could lead to sex differences in metabolism or accumulation of metals. Potential effect modification by genes involved in toxic metal metabolism is particularly interesting considering that studies have shown differences in overall exposure levels, disposition, immunotoxicity, and exposure-borne disease prevalence of arsenic, nickel, cadmium, lead, and methyl mercury for males versus females [90]. Genes involved in hormone regulation, including metabolism, transport, and synthesis, have been linked to exhibition of ASD symptomology [92]. Additionally, research has shown that genes more frequently expressed in males are also those involved in development of neurological disorders, such as ASD [93]. Hence, observed sex differences in ASD may also be due to sex-specific locations of genetic mutations during transcription on X or Y chromosomes, which may be more frequently expressed in males who only carry one of each. For example, studies have shown that males with Klinefelter syndrome, a genetic disorder resulting in an additional X chromosome (47,XXY), exhibit social and emotional deficits [94] and communication difficulties [95], and are frequently diagnosed with ASD [96, 97]. Additionally, males with 47,XYY and 48,XXYY genotypes have an increased risk of ASD [96, 98,99,100]. Females with a missing X chromosome (45,X) also have an increased rate of ASD [101] and females with and extra X chromosome (47,XXX) exhibit communication problems [96]. Thus, the addition, deletion, duplication, inactivation, or mutation of whole or parts of sex determining chromosomes could plausibly influence ASD risk either directly through susceptibility or indirectly through transcription of autosomal genes [28]. However, as these mechanisms are not well understood, sex-specific genes could either contribute to vulnerability in males or have some type of protective effect in females against de novo mutations [9, 102, 103].
Conclusion
To our knowledge, this is the first review presenting literature on associations between ASD and several toxic metals. Because ASD is a rare disease, many studies of exposures to metals are case-control studies collecting biological markers after ASD diagnosis. Considering the high correlation and co-occurring nature of many of the toxic metals presented, it is difficult to decipher which particular metal is the primary driver of any observed associations. However, previous studies have indicated that simultaneous exposure to these toxicants could potentially amplify detected effects [20, 67]. Furthermore, exposure to several toxic metals could be associated with a greater number of mutagenic effects. Sex differences further complicate an already complex picture of metal interactions in the body. Sex differences could lead to differences in uptake of metals under similar exposures, observed biomarker levels, and even toxicity in the body. Polymorphisms in transport proteins may also alter metal deposition, metabolic detoxification, and subsequent oxidative stress, influencing risk of ASD [22]. However, prior studies have overall not examined sex differences, and failure to account for these differences, not just as a confounding factor of analyses, but as an effect modifier, could lead to bias and misinterpretation of exposure-disease relationships [104]. Based on our examination of existing literature, the current evidence warrants a considerable need for evaluations of sex differences in future studies of the relationship between metals exposures and ASD.
References
Papers of particular interest, published recently, have been highlighted as: •• Of major importance
Association AP. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington: American Psychiatric Publishing, Inc.; 2013.
Association AP. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR). Washington DC: American Psychiatric Publishing, Inc.; 2000.
Christensen DL, Baio J, Van Naarden Braun K, Bilder D, Charles J, Constantino JN, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveill Summ. 2016;65(3):1–23.
Messinger DS, Young GS, Webb SJ, Ozonoff S, Bryson SE, Carter A, et al. Early sex differences are not autism-specific: a Baby Siblings Research Consortium (BSRC) study. Mol Autism. 2015;6:32.
Gillberg C, Cederlund M, Lamberg K, Zeijlon L. Brief report: “the autism epidemic”. The registered prevalence of autism in a Swedish urban area. J Autism Dev Disord. 2006;36(3):429–35.
Bourke J, de Klerk N, Smith T, Leonard H. Population-based prevalence of intellectual disability and autism spectrum disorders in western australia: a comparison with previous estimates. Medicine. 2016;95(21):e3737.
Eriksson M, Marschik PB, Tulviste T, Almgren M, Perez Pereira M, Wehberg S, et al. Differences between girls and boys in emerging language skills: evidence from 10 language communities. Br J Dev Psychol. 2012;30(Pt 2):326–43.
Rynkiewicz A, Schuller B, Marchi E, Piana S, Camurri A, Lassalle A, et al. An investigation of the ‘female camouflage effect’ in autism using a computerized ADOS-2 and a test of sex/gender differences. Mol Autism. 2016;7:10.
Polyak A, Rosenfeld JA, Girirajan S. An assessment of sex bias in neurodevelopmental disorders. Genome Med. 2015;7:94.
Bedford R, Jones EJ, Johnson MH, Pickles A, Charman T, Gliga T. Sex differences in the association between infant markers and later autistic traits. Mol Autism. 2016;7:21.
Miles JH, Hillman RE. Value of a clinical morphology examination in autism. Am J Med Genet. 2000;91(4):245–53.
Duchan E, Patel DR. Epidemiology of autism spectrum disorders. Pediatr Clin N Am. 2012;59(1):27–43. ix-x
Lyall K, Croen L, Daniels J, Fallin MD, Ladd-Acosta C, Lee BK, et al. The changing epidemiology of autism spectrum disorders. Annu Rev Public Health. 2016.
Wozniak RH, Leezenbaum NB, Northrup JB, West KL, Iverson JM. The development of autism spectrum disorders: variability and causal complexity. Wiley Interdiscip Rev Cogn Sci. 2017;8(1–2).
Tran NQV, Miyake K. Neurodevelopmental disorders and environmental toxicants: epigenetics as an underlying mechanism. Int J Genomics. 2017;2017:7526592.
Zheng W, Aschner M, Ghersi-Egea JF. Brain barrier systems: a new frontier in metal neurotoxicological research. Toxicol Appl Pharmacol. 2003;192(1):1–11.
Adams JB, Audhya T, McDonough-Means S, Rubin RA, Quig D, Geis E, et al. Toxicological status of children with autism vs. neurotypical children and the association with autism severity. Biol Trace Elem Res. 2013;151(2):171–80.
Obrenovich ME, Shamberger RJ, Lonsdale D. Altered heavy metals and transketolase found in autistic spectrum disorder. Biol Trace Elem Res. 2011;144(1–3):475–86.
Kalkbrenner AE, Daniels JL, Chen JC, Poole C, Emch M, Morrissey J. Perinatal exposure to hazardous air pollutants and autism spectrum disorders at age 8. Epidemiology. 2010;21(5):631–41.
Windham GC, Zhang L, Gunier R, Croen LA, Grether JK. Autism spectrum disorders in relation to distribution of hazardous air pollutants in the San Francisco Bay Area. Environ Health Perspect. 2006;114(9):1438–44.
•• Roberts AL, Lyall K, Hart JE, Laden F, Just AC, Bobb JF, et al. Perinatal air pollutant exposures and autism spectrum disorder in the children of Nurses’ Health Study II participants. Environ Health Perspect. 2013;121(8):978–84. This study provides a thorough and comprehensive evaluation of sex differences in associations between metals exposures and autism spectrum disorder.
Obrenovich ME, Shola D, Schroedel K, Agrahari A, Lonsdale D. The role of trace elements, thiamin (e) and transketolase in autism and autistic spectrum disorder. Front Biosci (Elite Ed). 2015;7:229–41.
Skalny AV, Simashkova NV, Klyushnik TP, Grabeklis AR, Bjorklund G, Skalnaya MG, et al. Hair toxic and essential trace elements in children with autism spectrum disorder. Metab Brain Dis. 2017;32(1):195–202.
Joubert BR, Felix JF, Yousefi P, Bakulski KM, Just AC, Breton C, et al. DNA methylation in newborns and maternal smoking in pregnancy: genome-wide consortium meta-analysis. Am J Hum Genet. 2016;98(4):680–96.
Ladd-Acosta C, Shu C, Lee BK, Gidaya N, Singer A, Schieve LA, et al. Presence of an epigenetic signature of prenatal cigarette smoke exposure in childhood. Environ Res. 2016;144(Pt A):139–48.
Rahbar MH, Samms-Vaughan M, Ma J, Bressler J, Loveland KA, Hessabi M, et al. Interaction between GSTT1 and GSTP1 allele variants as a risk modulating-factor for autism spectrum disorders. Res Autism Spectr Disord. 2015;12:1–9.
Chauhan A, Chauhan V. Oxidative stress in autism. Pathophysiology. 2006;13(3):171–81.
Schaafsma SM, Pfaff DW. Etiologies underlying sex differences in autism spectrum disorders. Front Neuroendocrinol. 2014;35(3):255–71.
Kern JK, Geier DA, Sykes LK, Haley BE, Geier MR. The relationship between mercury and autism: a comprehensive review and discussion. J Trace Elem Med Biol. 2016;37:8–24.
Yoshimasu K, Kiyohara C, Takemura S, Nakai K. A meta-analysis of the evidence on the impact of prenatal and early infancy exposures to mercury on autism and attention deficit/hyperactivity disorder in the childhood. Neurotoxicology. 2014;44:121–31.
Schultz ST. Does thimerosal or other mercury exposure increase the risk for autism? A review of current literature. Acta Neurobiol Exp. 2010;70(2):187–95.
Gil F, Hernandez AF, Marquez C, Femia P, Olmedo P, Lopez-Guarnido O, et al. Biomonitorization of cadmium, chromium, manganese, nickel and lead in whole blood, urine, axillary hair and saliva in an occupationally exposed population. Sci Total Environ. 2011;409(6):1172–80.
Mordukhovich I, Wright RO, Hu H, Amarasiriwardena C, Baccarelli A, Litonjua A, et al. Associations of toenail arsenic, cadmium, mercury, manganese, and lead with blood pressure in the normative aging study. Environ Health Perspect. 2012;120(1):98–104.
De Palma G, Catalani S, Franco A, Brighenti M, Apostoli P. Lack of correlation between metallic elements analyzed in hair by ICP-MS and autism. J Autism Dev Disord. 2012;42(3):342–53.
Mohamed Fel B, Zaky EA, El-Sayed AB, Elhossieny RM, Zahra SS, Salah Eldin W, et al. Assessment of hair aluminum, lead, and mercury in a sample of autistic Egyptian children: environmental risk factors of heavy metals in autism. Behav Neurol. 2015;545674:2015.
Al-Farsi YM, Waly MI, Al-Sharbati MM, Al-Shafaee MA, Al-Farsi OA, Al-Khaduri MM, et al. Levels of heavy metals and essential minerals in hair samples of children with autism in Oman: a case-control study. Biol Trace Elem Res. 2013;151(2):181–6.
Albizzati A, More L, Di Candia D, Saccani M, Lenti C. Normal concentrations of heavy metals in autistic spectrum disorders. Minerva Pediatr. 2012;64(1):27–31.
Blaurock-Busch E, Amin OR, Rabah T. Heavy metals and trace elements in hair and urine of a sample of Arab children with autistic spectrum disorder. Maedica (Buchar). 2011;6(4):247–57.
Adams JB, Holloway CE, George F, Quig D. Analyses of toxic metals and essential minerals in the hair of Arizona children with autism and associated conditions, and their mothers. Biol Trace Elem Res. 2006;110(3):193–209.
Al-Ayadhi LY. Heavy metals and trace elements in hair samples of autistic children in central Saudi Arabia. Neurosciences (Riyadh). 2005;10(3):213–8.
Fido A, Al-Saad S. Toxic trace elements in the hair of children with autism. Autism. 2005;9(3):290–8.
Kern JK, Grannemann BD, Trivedi MH, Adams JB. Sulfhydryl-reactive metals in autism. J Toxicol Environ Health A. 2007;70(8):715–21.
Prevention ACfCLP. Low level lead exposure harms children: a renewed call of primary prevention. Atlanta: Centers for Disease Control and Prevention (CDC); 2012. 01/04/2012. Report No
Lakshmi Priya MD, Geetha A. Level of trace elements (copper, zinc, magnesium and selenium) and toxic elements (lead and mercury) in the hair and nail of children with autism. Biol Trace Elem Res. 2011;142(2):148–58.
Skalny AV, Simashkova NV, Klyushnik TP, Grabeklis AR, Radysh IV, Skalnaya MG, et al. Analysis of hair trace elements in children with autism spectrum disorders and communication disorders. Biol Trace Elem Res. 2017;177(2):215-23.
Navas-Acien A, Umans JG, Howard BV, Goessler W, Francesconi KA, Crainiceanu CM, et al. Urine arsenic concentrations and species excretion patterns in American Indian communities over a 10-year period: the Strong Heart Study. Environ Health Perspect. 2009;117(9):1428–33.
Ishizaki M, Suwazono Y, Kido T, Nishijo M, Honda R, Kobayashi E, et al. Estimation of biological half-life of urinary cadmium in inhabitants after cessation of environmental cadmium pollution using a mixed linear model. Food Addit Contam Part A Chem Anal Control Expo Risk Assess. 2015;32(8):1273–6.
Yorbik O, Kurt I, Hasimi A, Ozturk O. Chromium, cadmium, and lead levels in urine of children with autism and typically developing controls. Biol Trace Elem Res. 2010;135(1–3):10–5.
Bradstreet J, Geier DA, Kartzinel JJ, Adams JB, Geier MR. A case-control study of mercury burden in children with autistic spectrum disorders. J Am Phys Surg. 2003;8(3):76–9.
Adams J, Howsmon DP, Kruger U, Geis E, Gehn E, Fimbres V, et al. Significant association of urinary toxic metals and autism-related symptoms-a nonlinear statistical analysis with cross validation. PLoS One. 2017;12(1):e0169526.
Heard MJ, Chamberlain AC. Uptake of Pb by human skeleton and comparative metabolism of Pb and alkaline earth elements. Health Phys. 1984;47(6):857–65.
Rahbar MH, Samms-Vaughan M, Pitcher MR, Bressler J, Hessabi M, Loveland KA, et al. Role of metabolic genes in blood aluminum concentrations of Jamaican children with and without autism spectrum disorder. Int J Environ Res Public Health. 2016;13(11). https://doi.org/10.3390/ijerph13111095.
Rahbar MH, Samms-Vaughan M, Ardjomand-Hessabi M, Loveland KA, Dickerson AS, Chen Z, et al. The role of drinking water sources, consumption of vegetables and seafood in relation to blood arsenic concentrations of Jamaican children with and without Autism Spectrum Disorders. Sci Total Environ. 2012;433:362–70.
Rahbar MH, Samms-Vaughan M, Dickerson AS, Loveland KA, Ardjomand-Hessabi M, Bressler J, et al. Role of fruits, grains, and seafood consumption in blood cadmium concentrations of Jamaican children with and without autism spectrum disorder. Res Autism Spectr Disord. 2014;8(9):1134–45.
Jory J, McGinnis WR. Red-cell trace minerals in children with autism. Am J Biochem Biotechnol. 2008;4(2):101–4.
Tian Y, Green PG, Stamova B, Hertz-Picciotto I, Pessah IN, Hansen R, et al. Correlations of gene expression with blood lead levels in children with autism compared to typically developing controls. Neurotox Res. 2011;19(1):1–13.
Rahbar MH, Samms-Vaughan M, Dickerson AS, Loveland KA, Ardjomand-Hessabi M, Bressler J, et al. Blood lead concentrations in Jamaican children with and without autism spectrum disorder. Int J Environ Res Public Health. 2014;12(1):83–105.
El-Ansary A, Bjorklund G. Relationship between selenium, lead, and mercury in red blood cells of Saudi autistic children. Metab Brain Dis. 2017;32(4):1073–80.
Rahbar MH, Samms-Vaughan M, Dickerson AS, Loveland KA, Ardjomand-Hessabi M, Bressler J, et al. Blood manganese concentrations in Jamaican children with and without autism spectrum disorders. Environ Health. 2014;13:69.
Laohaudomchok W, Lin X, Herrick RF, Fang SC, Cavallari JM, Christiani DC, et al. Toenail, blood, and urine as biomarkers of manganese exposure. J Occup Environ Med. 2011;53(5):506–10.
Shepherd TJ, Dirks W, Manmee C, Hodgson S, Banks DA, Averley P, et al. Reconstructing the life-time lead exposure in children using dentine in deciduous teeth. Sci Total Environ. 2012;425:214–22.
Adams JB, Romdalvik J, Ramanujam VM, Legator MS. Mercury, lead, and zinc in baby teeth of children with autism versus controls. J Toxicol Environ Health A. 2007;70(12):1046–51.
Abdullah MM, Ly AR, Goldberg WA, Clarke-Stewart KA, Dudgeon JV, Mull CG, et al. Heavy metal in children’s tooth enamel: related to autism and disruptive behaviors? J Autism Dev Disord. 2012;42(6):929–36.
Hertz-Picciotto I, Green PG, Delwiche L, Hansen R, Walker C, Pessah IN. Blood mercury concentrations in CHARGE Study children with and without autism. Environ Health Perspect. 2010;118(1):161–6.
Rahbar MH, Samms-Vaughan M, Loveland KA, Ardjomand-Hessabi M, Chen Z, Bressler J, et al. Seafood consumption and blood mercury concentrations in Jamaican children with and without autism spectrum disorders. Neurotox Res. 2013;23(1):22–38.
Weisskopf MG, Kioumourtzoglou MA, Roberts AL. Air pollution and autism spectrum disorders: causal or confounded? Curr Environ Health Rep. 2015;2(4):430–9.
Dickerson AS, Rahbar MH, Bakian AV, Bilder DA, Harrington RA, Pettygrove S, et al. Autism spectrum disorder prevalence and associations with air concentrations of lead, mercury, and arsenic. Environ Monit Assess. 2016;188(7):407.
Talbott EO, Marshall LP, Rager JR, Arena VC, Sharma RK, Stacy SL. Air toxics and the risk of autism spectrum disorder: the results of a population based case-control study in southwestern Pennsylvania. Environ Health. 2015;14:80.
Lewandowski TA, Bartell SM, Yager JW, Levin L. An evaluation of surrogate chemical exposure measures and autism prevalence in Texas. J Toxicol Environ Health A. 2009;72(24):1592–603.
(ATSDR) AfTSaDR. Public health statement: aluminum. Atlanta, GA: Centers for Disease Control and Prevention, Medicine DoTaE; 2008 CAS # 7429-90-5 Contract No.: CAS # 7429-90-5.
(ATSDR) AfTSaDR. Public health statement: beryllium. Atlanta, GA: Centers for Disease Control and Prevention, Toxicology Do; 2002 Contract No.: CAS#: 7440–41-7.
Beesley L, Moreno-Jimenez E, Gomez-Eyles JL. Effects of biochar and greenwaste compost amendments on mobility, bioavailability and toxicity of inorganic and organic contaminants in a multi-element polluted soil. Environ Pollut. 2010;158(6):2282–7.
Rehman K, Fatima F,Waheed I, Akash MSH. Prevalence of exposure of heavy metals and their impact on health consequences. 2017. https://doi.org/10.1002/jcb.26234.
Theppeang K, Glass TA, Bandeen-Roche K, Todd AC, Rohde CA, Links JM, et al. Associations of bone mineral density and lead levels in blood, tibia, and patella in urban-dwelling women. Environ Health Perspect. 2008;116(6):784–90.
Nie H, Sanchez BN, Wilker E, Weisskopf MG, Schwartz J, Sparrow D, et al. Bone lead and endogenous exposure in an environmentally exposed elderly population: the normative aging study. J Occup Environ Med. 2009;51(7):848–57.
Manton WI, Angle CR, Stanek KL, Kuntzelman D, Reese YR, Kuehnemann TJ. Release of lead from bone in pregnancy and lactation. Environ Res. 2003;92(2):139–51.
Pounds JG, Long GJ, Rosen JF. Cellular and molecular toxicity of lead in bone. Environ Health Perspect. 1991;91:17–32.
Specht AJ, Mostafaei F, Lin Y, Xu J, Nie LH. Measurements of strontium levels in human bone in vivo using portable X-ray fluorescence (XRF). Appl Spectrosc. 2017;71(8):1962–68.
De Craemer S, CroesK, van LarebekeN,DeHenauwS, Schoeters G, Govarts E, et al. Metals, hormones and sexual maturation in Flemish adolescents in three cross-sectional studies (2002–2015). Environ Int. 2017;102:190–99.
Wu T, Buck GM, Mendola P. Blood lead levels and sexual maturation in U.S. girls: the Third National Health and Nutrition Examination Survey, 1988-1994. Environ Health Perspect. 2003;111(5):737–41.
Nagata C, Nagao Y, Shibuya C, Kashiki Y, Shimizu H. Urinary cadmium and serum levels of estrogens and androgens in postmenopausal Japanese women. Cancer Epidemiol Biomarkers Prev. 2005;14(3):705–8.
Rutter M, Caspi A, Moffitt TE. Using sex differences in psychopathology to study causal mechanisms: unifying issues and research strategies. J Child Psychol Psychiatry. 2003;44(8):1092–115.
Geier DA, Geier MR. A prospective assessment of androgen levels in patients with autistic spectrum disorders: biochemical underpinnings and suggested therapies. Neuro Endocrinol Lett. 2007;28(5):565–73.
Barany E, Bergdahl IA, Bratteby LE, Lundh T, Samuelson G, Skerfving S, et al. Iron status influences trace element levels in human blood and serum. Environ Res. 2005;98(2):215–23.
Goyer RA. Toxic and essential metal interactions. Annu Rev Nutr. 1997;17:37–50.
Gulson BL, Mahaffey KR, Jameson CW, Mizon KJ, Korsch MJ, Cameron MA, et al. Mobilization of lead from the skeleton during the postnatal period is larger than during pregnancy. J Lab Clin Med. 1998;131(4):324–9.
Hsueh YM, Ko YF, Huang YK, Chen HW, Chiou HY, Huang YL, et al. Determinants of inorganic arsenic methylation capability among residents of the Lanyang Basin, Taiwan: arsenic and selenium exposure and alcohol consumption. Toxicol Lett. 2003;137(1–2):49–63.
Loffredo CA, Aposhian HV, Cebrian ME, Yamauchi H, Silbergeld EK. Variability in human metabolism of arsenic. Environ Res. 2003;92(2):85–91.
Lee BK, Kim Y. Sex-specific profiles of blood metal levels associated with metal-iron interactions. Saf Health Work. 2014;5(3):113–7.
Vahter M, Akesson A, Liden C, Ceccatelli S, Berglund M. Gender differences in the disposition and toxicity of metals. Environ Res. 2007;104(1):85–95.
Vahter M, Gochfeld M, Casati B, Thiruchelvam M, Falk-Filippson A, Kavlock R, et al. Implications of gender differences for human health risk assessment and toxicology. Environ Res. 2007;104(1):70–84.
Chakrabarti B, Dudbridge F, Kent L, Wheelwright S, Hill-Cawthorne G, Allison C, et al. Genes related to sex steroids, neural growth, and social-emotional behavior are associated with autistic traits, empathy, and Asperger syndrome. Autism Res. 2009;2(3):157–77.
Shi L, Zhang Z, Su B. Sex biased gene expression profiling of human brains at major developmental stages. Sci Rep. 2016;6:21181.
Tartaglia N, Cordeiro L, Howell S, Wilson R, Janusz J. The spectrum of the behavioral phenotype in boys and adolescents 47,XXY (Klinefelter syndrome). Pediatr Endocrinol Rev. 2010;8(Suppl 1):151–9.
Bishop DV, Scerif G. Klinefelter syndrome as a window on the aetiology of language and communication impairments in children: the neuroligin-neurexin hypothesis. Acta Paediatr. 2011;100(6):903–7.
Bishop DV, Jacobs PA, Lachlan K, Wellesley D, Barnicoat A, Boyd PA, et al. Autism, language and communication in children with sex chromosome trisomies. Arch Dis Child. 2011;96(10):954–9.
van Rijn S, Swaab H. Vulnerability for psychopathology in Klinefelter syndrome: age-specific and cognitive-specific risk profiles. Acta Paediatr. 2011;100(6):908–16.
Geerts M, Steyaert J, Fryns JP. The XYY syndrome: a follow-up study on 38 boys. Genet Couns. 2003;14(3):267–79.
Bruining H, Swaab H, Kas M, van Engeland H. Psychiatric characteristics in a self-selected sample of boys with Klinefelter syndrome. Pediatrics. 2009;123(5):e865–70.
Tartaglia N, Davis S, Hench A, Nimishakavi S, Beauregard R, Reynolds A, et al. A new look at XXYY syndrome: medical and psychological features. Am J Med Genet A. 2008;146a(12):1509–22.
Creswell CS, Skuse DH. Autism in association with Turner syndrome: genetic implications for male vulnerability to pervasive developmental disorders. Neurocase. 1999;5(6):511–8.
Gilman SR, Iossifov I, Levy D, Ronemus M, Wigler M, Vitkup D. Rare de novo variants associated with autism implicate a large functional network of genes involved in formation and function of synapses. Neuron. 2011;70(5):898–907.
Zhao X, Leotta A, Kustanovich V, Lajonchere C, Geschwind DH, Law K, et al. A unified genetic theory for sporadic and inherited autism. Proc Natl Acad Sci U S A. 2007;104(31):12831–6.
Vatcheva KP, Lee M, McCormick JB, Rahbar MH. The effect of ignoring statistical interactions in regression analyses conducted in epidemiologic studies: an example with survival analysis using Cox proportional hazards regression model. Epidemiology (Sunnyvale). 2015;6(1). https://doi.org/10.4172/21611165.1000216.
Acknowledgments
We are grateful for the assistance of Andrea Roberts, who provided feedback on the draft manuscript.
Funding
Aisha S. Dickerson is supported by NIH training grant NIH T32 ES007069. Vy T. Nguyen is supported by NIH training grant NIH T42 OH008416. Aaron Spect is supported under NIH grants R01ES024165 and R21ES024700.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Aisha S. Dickerson, Ran Rotem, MacKinsey A. Christian, Vy T. Nguyen, and Aaron Specht, declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any data directly collected from human or animals subjects by any of the authors.
Additional information
This article is part of the Topical Collection on Synthetic Chemicals and Health
Rights and permissions
About this article

Cite this article
Dickerson, A.S., Rotem, R.S., Christian, M.A. et al. Potential Sex Differences Relative to Autism Spectrum Disorder and Metals. Curr Envir Health Rpt 4, 405–414 (2017). https://doi.org/10.1007/s40572-017-0164-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40572-017-0164-x