
Abstract
Background
Osteoarthritis (OA) is a degenerative joint disease and a leading cause of adult disability. There is no cure for OA and there is no effective treatment to stop its progression. Current pharmacologic treatments such as analgesics and non-steroidal anti-inflammatory drugs may improve the pain and offer some relief but they do not affect the progression of the disease. The chronic intake of these drugs may result in severe adverse events. The aim of this review is to revise the effects of nutrition on cartilage metabolism and OA progression.
Methods
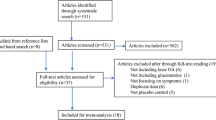
A systematic literature search was performed including those related to macro- and micro-nutrients’ actions on cartilage and OA outcome. We selected peer-reviewed articles reporting the results of human clinical trials.
Results
Glucosamine and chondroitin sulfate have shown to delay OA knee progression in several clinical trials. The effectiveness of some products considered nutraceuticals has been widely reviewed in the literature. This article presents a general description of the effectiveness and mechanism of action of nutrients, vitamins, antioxidants and other natural components considered as part of the normal diet. Many in vitro studies indicate the efficacy of specific nutrients in cartilage metabolism and its involvement in OA. However, rigorous clinical studies needed to evaluate the efficacy of these compounds in humans are still missing. The influence of nutrients and diet on the metabolism of cartilage and OA could represent a long-term coadjuvant alternative in the management of patients with OA. Effects of diet modifications on lipid and cholesterol profiles, adequate vitamin levels and weight reduction in obese patients could influence the course of the disease.
Conclusion
This review demonstrates that nutrition can improve the symptoms of OA. Glucosamine and chondroitin sulfate have shown robustly to delay the progression of knee OA in several well-designed studies, however more controlled clinical trials are needed to conclude that nutritional changes slow down the progression of the disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Articular cartilage is a specialized type of hyaline tissue that covers the surface of the bones in the synovial joints, favoring the sliding of the joint surfaces and improving friction during movements. This avascular and aneural tissue is nourished by synovial fluid and subchondral bone, and its physical properties include resistance to stress and compression forces, as well as the ability to adapt to pressure [1].
Chondrocytes are the only type of cell present in the cartilage and represent 1–5% of the cartilage and are embedded in an amorphic extracellular matrix composed mainly by collagen which is responsible for force tension and proteoglycans that provide compression resistance to cartilage [2].
OA is the most prevalent form of joint disease and a growing cause of disability worldwide. Globally, 18% of women and 9.6% of men aged over 60 years have symptomatic OA with a quarter of these individuals unable to perform routine daily activities. By 2050, a projected number of 130 million people will suffer from OA, constituting a societal burden [3, 4].
The natural products used by patients to relieve symptoms are now globally available and can be helpful in maintaining bone and joint health. Nutraceuticals, food or food products that provide medical health benefits, including prevention and/or treatment of diseases, offer not only a safe alternative to the current pharmacological therapies, but they can also modify the symptoms in OA [5, 6].
This review will focus mainly on the nutrients that usually conform to a normal diet, but also nutraceuticals such as glucosamine, chondroitin and avocado/soybean unsaponifiables for the OA.
The efficacy of certain nutraceuticals such as glucosamine sulfate, chondroitin sulfate and avocado/soybean unsaponifiables for the OA is widely reviewed in the literature and are considered as slow-acting drugs for osteoarthritis (SYSADOAs) with robust evidence on OA symptoms and disease-modifying effects in the long term for some of these products [7,8,9,10].
Multiple formulations for glucosamine and chondroitin are available, in some countries they are in a condition of sale under medical prescription and in others as over-the-counter products, but the latter may include different amounts of glucosamine and chondroitin, or in the case of glucosamine is composed of a different substance, mainly as glucosamine hydrochloride, with a different efficacy profile [11].
The efficacy of products for prescription-grade glucosamine and chondroitin have proven efficacy in controlled and properly designed clinical trials and have been subject to strict regulatory control. Over-the-counter products usually lack controlled clinical trials and may differ in the pharmaceutical formulation or molecular form and purity [5, 11]. The recommendation to use only pharmaceutical-grade preparations for glucosamine sulfate (pCGS) and chondroitin sulfate is clearly supported by the recent guidelines [5].
Forty-seven percent of adults use alternative medications non-prescribed for the management of OA. Several reports and reviews analyze the potential protective effects of nutrients on cartilage metabolism and the development of OA such as antioxidants (epicatechin, epigallocatechin 3-gallate EGCG, resveratrol), vitamin D, E and C, curcumin, pomegranate extracts, omega 3 fatty acid, and Psidium guajava (guava) [12,13,14]. However, in some trials, the quality of these products is poorly regulated and their efficacy, toxicity and mechanisms of action are largely unknown.
Interestingly, green-lipped mussel extract (GLM, Perna canaliculus) and glucosamine sulfate reduced OA symptoms and induced changes in the microbiota profile, with a reduction in the Clostridia sp. in a clinical study being the most notable. This finding suggests that nutritional supplements such as both used in this study may influence some of the metabolic and immunological activities of the gastrointestinal tract microbiota. This fact was consistent with a decrease in inflammation and improved OA symptoms. Microbiota may be important in the first-pass metabolism of these nutraceuticals [15].
How does cartilage nourish?
Articular cartilage is avascular and is nourished by synovial fluid and subchondral vessels [1]. Experimental evidence from animal models has shown that immature cartilage can be nourished in both ways, but in mature animals, the predominant source is synovial fluid due to the dense calcified barrier of subchondral bone that could limit the diffusion of fluid and soluble substances through the vascular channels [1, 16].
Subchondral mechanism has been debated [17, 18]; however, it has been reported that subchondral bone’s blood vessels may expand and penetrate the adjacent calcified cartilage through channels and the nutrients may reach the cartilage through these perforations. This theory supports the importance of this pathway for cartilage nourishment. It was postulated that 50% of glucose requirements, oxygen and water are given by perfusion from subchondral vessels [2, 19].
Subchondral bone vascularization development correlates with stress distribution and compressive forces acting on the cartilage and subchondral bone [19]. It has been reported in animal models that calcified cartilage was permeable to the diffusion of low-molecular weight solutes and cyclic changes in the joint might favor the diffusion of large molecules to the cartilage [20]. Signal molecules to maintain the communication and functional association between calcified cartilage and subchondral bone (Osteochondral Unit) may also reach cartilage and bone through subchondral vessels and the osteocyte lacuna-canalicular network of bone [21].
Proteins, amino acids and lipids in cartilage and osteoarthritis
Glucose is the main source of energy for chondrocytes, but lipids in cartilage are also needed as an energy source for these cells; additionally, they are incorporated as structural components and signaling molecules and they represent about 1% of the dry weight of the cartilage. The cartilage is also a tissue in which eicosanoids—derived from arachidonic acid—are actively produced [22, 23].
Amino acids (AA), in addition to being involved in the formation of proteins, are also precursors of a series of low-molecular weight molecules such as serotonin, dopamine, glucosamine, creatine, nitric oxide and others with important activities and functions [24, 25].
Metabolomics analysis could quantitatively detect many small-molecule metabolites in a sample (body fluids, cell, tissues), and it has been used to investigate the metabolic changes and biomarkers in OA [25, 26]. Amino acids’ profile alterations have been identified in serum, synovial fluid and urine samples from OA patients [25]. The finding that most serum AA levels were altered, suggest that metabolism and profiles of AA are also involved in the pathogenesis of OA [24].
Among the lipids, cholesterol and fatty acids are the most involved in the pathophysiology of articular cartilage. Lipids may be available for chondrocytes directly from synovial fluid or by “de novo” synthesis, because these cells contain the proteins necessary for the metabolism of fatty acids and the synthesis of cholesterol [23].
The cellular membrane of the chondrocytes has a high cholesterol content which emphasizes its structural importance; in addition the mature cartilage contains a high amount of saturated fatty acids, linoleic acid, oleic acid and palmitic acid [23, 27]. The total composition of the fatty acids in the cartilage can be modulated by the intake of fatty acids with the diet. In animal models, it has been shown that diets containing high levels of omega 3 (ω-3), and fatty acids may decrease the content of arachidonic and linoleic acid, and decreasing proteoglycan synthesis may damage articular cartilage [27, 28].
It is considered that the most important role of fatty acids in cartilage is its conversion to eicosanoids; and ω-3 and ω-6 fatty acids are substrates for the cyclooxygenase and lipoxygenase enzymes that synthesize prostaglandins and leukotrienes, the former with anti-inflammatory properties and the latter with proinflammatory and prothrombotic actions [29].
The osteoarthritic cartilage has high amounts of fatty acids and an increased expression of metalloproteinases (MMPs), and cyclooxygenase and lipoxygenase-derived eicosanoids, which can contribute to the pathogenesis of OA [22, 28].
The effect of lipids on OA is still a matter of debate; fatty acids could alter the cartilage destruction process, but the individual effects of each fatty acid appear to be different. Linoleic acid has a proinflammatory effect, while oleic acid and palmitic acid seem to inhibit cartilage destruction and inflammation [30].
Wang found a correlation between the intake of ω-6 fatty acids and the development of bone marrow lesions but without volume loss in the cartilage [31]. In asymptomatic women without clinical evidence of knee OA, elevated levels of cholesterol and triglycerides were associated with the development of incidental bone marrow lesions during a 2-year follow-up period [32]. However, Dorée found that HDL cholesterol was associated with a decrease in the size and resolution of bone marrow lesions and rather seemed to have a protective effect against incidental bone marrow lesions [33].
Some authors also pointed the benefits of olive oil and the Mediterranean diet in ameliorating the progression of cartilage degeneration, lowering the risk of pain worsening and symptoms in patients with knee OA [34, 35].
The Western-type diet rich in red meat, high-fat dairy products and refined grains has been associated with higher levels of CRP and IL-6 (proinflammatory diet), in contrast with Mediterranean diet, which is rich in fish and high in whole grains, green vegetables and fruits, and is thus associated with lower levels of inflammation [35, 36]. Veronese in a longitudinal cohort study with a follow-up period of 4 years demonstrated that higher adherence to Mediterranean diet is associated with a lower risk of pain worsening and symptomatic forms of knee OA [37].
Role of vitamins and micronutrients in cartilage and osteoarthritis
Vitamins with antioxidant properties retard or inhibit the oxidation of substrates susceptible to attack by reactive oxygen species (ROS); its protective role has been evaluated in different chronic diseases.
There are important methodological issues when analyzing the association between vitamins and micronutrients with the onset, progression or control of symptoms of osteoarthritis that make it difficult to draw definite conclusions. Among the problems are the enough number of participants in the clinical trials, the lack of adequate control groups and the chemical, source and nature of the evaluated vitamin or micronutrient [38].
Ethnicity can probably influence some dietary preferences, pain disparities, and the poor absorption of certain vitamins such as vitamin D for the skin in people with dark skin, but also in the prevalence and the requirement of major procedures as total knee arthroplasty in osteoarthritis [39,40,41].
Some vitamins with antioxidant properties such as tocopherol (vitamin E), precursors of vitamin A, carotenoids and ascorbate (vitamin C) may provide some protection against cellular injury when intracellular antioxidant enzymes have been overwhelmed; since these micronutrients are obtained from the diet, it is postulated that a high intake could have a protective effect against diseases related to aging [13]. MacAllindon did not find a significant association between the intake of antioxidant micronutrients including vitamin C, E and carotene with the incidence of OA of the knees, but subjects in the higher tertile intake of vitamin C had a reduced risk of developing knee pain [12]. After controlling the confounding variables, Peregoy found that vitamin C supplementation may be beneficial in preventing incident OA of the knees in the Clearwater Osteoarthritis Study [42].
Some clinical studies have shown contradictory results, one study found that patients with knee OA who consumed vitamin C and E in the highest tertile had an increased risk of knee OA compared with those in the lower tertile [43]. In other studies, the association is contradictory or even negative [44, 45]. In rural Japanese inhabitants, the mean tertile of alpha-tocopherol intake had a lower risk of OA, but did not find this association in the superior tertile [46].
Chin suggests that high levels of antioxidants such as vitamin E may act as pro-oxidants and cause articular cartilage damage, so there could be a U-shaped relationship between vitamin E and joint health, which would be beneficial at low concentrations and harmful at high concentrations. Finally, the different isoforms of vitamin E may have different biological effects, but most studies have focused on alpha-tocopherol [47]. However, the available information is not conclusive about a beneficial effect of antioxidant vitamin supplements to recommend their intake beyond a healthy diet that includes adequate amounts of these nutrients [48].
Vitamin K is involved in the mineralization of bone and cartilage, and the association with OA has been evaluated in different studies, particularly focused on vitamin K1 (phylloquinone). Some cross-sectional studies have shown that decreased serum vitamin K1 levels are associated with a higher prevalence of OA of the knees and hands [49, 50]. In longitudinal studies, subclinical vitamin K deficiency was associated with an increased risk of developing radiological changes of knee OA and cartilage lesions on MRI [51], and in subjects with very low levels of vitamin K, a greater progression of articular cartilage and meniscus damage was observed [52].
However; a randomized clinical trial in which the effect of vitamin K1 was compared with placebo, found no effect on radiographic OA of the hands. Only subjects who were deficient in this vitamin at baseline and who reached enough concentrations during follow-up had a benefit in joint space narrowing at the end of the study [53].
In another clinical study in older adults, the elevated status of vitamin K1 was associated with better scores of physical performances at baseline, although the longitudinal data was less consistent, the authors suggest that this vitamin is important in maintaining function but does not alter the functional decline rate [54].
The role of vitamin D in the risk of developing OA is controversial and Heidari found significantly decreased levels of vitamin D in subjects under 60 years old with OA of the knees in relation to controls, consistent with the onset of early OA [55], and Chaganti reported that men deficient in vitamin D were twice as likely to develop radiological hip OA [56].
Other clinical trials and meta-analysis have tried to assess vitamin D status and the risk of progression of OA; Bergink found that low vitamin D intake increased the progression of radiological OA of the knees [57]. Felson found no association between decreased levels of vitamin D and the risk of increased loss of joint cartilage in OA [58]; however, Zhang reported that vitamin D deficiency was associated with an increased risk of radiological progression of knee OA [59].
Finally, different studies have analyzed the effect of vitamin D supplements on the symptoms and progression of OA. McAlindon found that vitamin D supplementation at the right dose raised the plasma levels of vitamin D to 36 ng/mL or more but it did not reduce pain or loss of joint volume in patients with symptomatic knee OA [60]. Jin reported that vitamin D supplementation for 2 years did not prevent the loss of articular cartilage and did not improve the pain in subjects with symptomatic knee OA [61]. On the contrary, Sanghi reported a small benefit of vitamin D supplementation in reducing pain and improving function in patients with OA [62]. Zheng, in a post hoc analysis of the VIDEO study, found small benefit in slowing the loss of joint cartilage, reducing joint inflammation and improving physical function in subjects with OA [63].
Despite the available evidence, it would be premature to make any conclusion or recommendation about the efficacy of vitamins in reducing the development or progression of OA, and it is clear that more research is needed to clarify this topic.
Among minerals, magnesium is the second most abundant intracellular cation and one of the most important micronutrients for human health and is strongly associated with immune responses. Some evidence shows a probable relationship between magnesium and OA. Decreased levels of magnesium and calcium have been found in endemic areas of OA, and in a study of twin women with OA, reduced levels of serum magnesium were found [64, 65].
It is postulated that magnesium deficiency might cause an uncontrolled growth of crystals with high calcium content in the cartilage causing damage to this tissue. In addition, magnesium seems to promote the differentiation and viability of chondrocytes [66]. Animal models have shown that magnesium may also play a role in pain by altering cytosine and neurotransmitter levels [67]. Additionally, magnesium has been linked to the immune response, and reduced levels of magnesium in the diet have been associated with elevated C-reactive protein and other inflammatory markers, suggesting a role in low-grade inflammation that could participate in the initiation and progression of OA [68, 69].
A cross-sectional study found a modest but significant inverse relationship between magnesium intake and the radiographic incidence of knee OA in white participants, but not in black subjects [70], and a prospective cohort study in patients with radiological OA of the knees found that low magnesium intake was associated with greater pain and poorer outcomes in functional tests in patients with OA with low dietary fiber intake [71].
Selenium is an essential micronutrient for different biological functions and is associated with different organic molecules among which are the selenocysteines, required for the function of the selenoproteins involved in the regulation of the differentiation of the growth epiphyseal plate, and also fulfill antioxidant functions. In animal models, it has been demonstrated that by generating selenium deficiency in osteochondral osteoprogenitor cells, alterations in skeletal growth, delayed ossification, alteration in subchondral bone formation and severe chondronecrosis may develop [72, 73]. Although with some controversy, selenium supplementation has been shown to be effective in the primary prevention and treatment of Kashin–Beck disease in children [74, 75].
The role of other nutrients in the metabolism of cartilage and OA is still under study; zinc is a structural component of different proteins and together with its transporter molecules appears to intervene in the regulation of enzymes that degrade the articular cartilage matrix as metalloproteinases [76, 77]. The excessive accumulation of iron in obese guinea has been associated with the development of knee OA [78].
Conclusion
Among nutraceuticals, prescription-grade glucosamine and chondroitin sulfate have robust evidence on improving OA symptoms and disease-modifying effects in the long term and offer the possibility to reduce non-steroidal anti-inflammatory and analgesic doses and avoid the adverse events associated with the use of these medications.
The list of nutrients whose effect on articular cartilage or OA has been evaluated is long, but in the future, information from longitudinal and controlled studies may provide more information on this interesting topic. Finally, the influence of nutrients and diet on the cartilage metabolism and OA could represent a coadjutant long-term alternative that contributes to the management of patients with OA. The effects of diet modifications on lipids and cholesterol profiles, adequate vitamins levels and weight reductions in obese patients could influence the course of the disease.
References
Wang B, Zhou X, Price C et al (2013) Quantifying load-induced solute transport and solute-matrix interaction within the osteocyte lacunar-canalicular system. J Bone Miner Res 28:1075–1086
Madry H, Niek van Dijk C, Mueller-Gerbl M (2010) The basic science of the subchondral bone. Knee Surg Sports Traumatol Arthrosc 18:419–433
Maiese K (2016) Picking a bone with WISP1 (CCN4): new strategies against degenerative joint disease. J Transl Sci 1:83–85
Leong D, Choudhury M, Hirsh D et al (2013) Nutraceuticals: potential for chondroprotection and molecular targeting of osteoarthritis. Int J Mol Sci 14:23063–23085
Bruyère O, Cooper C, Al-Daghri NM et al (2018) Inappropriate claims from non-equivalent medications in osteoarthritis: a position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Aging Clin Exp Res 30:111–117
Akhtar N, Haqqi TM (2012) Current nutraceuticals in the management of osteoarthritis: a review. Ther Adv Musculoskelet Dis 4:181–207
Reginster JY, Deroisy R, Rovati LC et al (2001) Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. Lancet 357:251–256
Pavelká K, Gatterová J, Olejarová M et al (2002) Glucosamine sulfate use and delay of progression of knee osteoarthritis: a 3-year, randomized, placebo-controlled, double-blind study. Arch Intern Med 162:2113–2123
Kahan A, Uebelhart D, De Vathaire F et al (2009) Long-term effects of chondroitins 4 and 6 sulfate on knee osteoarthritis: the study on osteoarthritis progression prevention, a two-year, randomized, double-blind, placebo-controlled trial. Arthritis Rheum 60:524–533
Maheu E, Cadet C, Marty M et al (2014) Randomised, controlled trial of avocado–soybean unsaponifiable (piascledine) effect on structure modification in hip osteoarthritis: the ERADIAS study. Ann Rheum Dis 73:376–384
Cutolo M, Berenbaum F, Hochberg M et al (2015) Commentary on recent therapeutic guidelines for osteoarthritis. Semin Arthritis Rheum 44:611–617
McAlindon TE, Jacques P, Zhang Y et al (1996) Do antioxidant micronutrients protect against the development and progression of knee osteoarthritis? Arthritis Rheumatol 39:648–656
McAlindon T, Felson D (1997) Nutrition: risk factors for osteoarthritis. Ann Rheum Dis 56:397–402
Kakuo S, Fushimi T, Kawasaki K et al (2018) Effects of Psidium guajava Linn. leaf extract in Japanese subjects with knee pain: a randomized, double-blind, placebo-controlled, parallel pilot study. Aging Clin Exp Res 30:1391–1398
Coulson S, Butt H, Vecchio P (2013) Green-lipped mussel extract (Perna canaliculus) and glucosamine sulphate in patients with knee osteoarthritis: therapeutic efficacy and effects on gastrointestinal microbiota profiles. Inflammopharmacology 21:79–90
Hodge JA, McKibbin B (1969) The nutrition of mature and immature cartilage in rabbits: an autoradiographic study. J Bone Jt Surg Br 51:140–147
Clark JM (1990) The structure of vascular channels in the subchondral plate. J Anat 171:105–115
Malinin T, Ouellette EA (2000) Articular cartilage nutrition is mediated by subchondral bone: a long-term autograft study in baboons. Osteoarthr Cartil 8:483–491
Imhof H, Breitenseher M, Kainberger F et al (1999) Importance of subchondral bone to articular cartilage in health and disease. Top Magn Reson Imaging 10:180–192
Arkill KP, Winlove CP (2008) Solute transport in the deep and calcified zones of articular cartilage. Osteoarthr Cartil 16:708–714
Oláh T, Mandry H (2018) The osteochondral unit: the importance of the underlying subchondral bone. In: Farr J, Gomoll AH (eds) Cartilage restoration. Practical clinical applications, 2nd edn. Spriger International Publishing, Amsterdam, pp 13–22
Attur M, Dave M, Abramson SB et al (2012) Activation of diverse eicosanoid pathways in osteoarthritic cartilage: a lipidomic and genomic analysis. Bull NYU Hosp Jt Dis 70:99
Villalvilla A, Gómez R, Largo R et al (2013) Lipid transport and metabolism in healthy and osteoarthritic cartilage. Int J Mol Sci 14:20793–20808
Li Y, Xiao W, Luo W et al (2016) Alterations of amino acid metabolism in osteoarthritis: its implications for nutrition and health. Amino Acids 48:907–914
Chen R, Han S, Liu X et al (2018) Perturbations in amino acids and metabolic pathways in osteoarthritis patients determined by targeted metabolomics analysis. J Chromatogr B 1085:54–62
Lamers RJAN, Van Nesselrooij JHJ, Kraus VB et al (2005) Identification of an urinary metabolite profile associated with osteoarthritis. Osteoarthr Cartil 13:762–768
Sekar S, Crawford R, Xiao Y et al (2017) Dietary fats and osteoarthritis: insights, evidences, and new horizons. J Cell Biochem 118:453–463
Lippiello L, Fienhold M, Grandjean C (1990) Metabolic and ultrastructural changes in articular cartilage of rats fed dietary supplements of omega-3 fatty acids. Arthritis Rheum 33:1029–1036
Lopez HL (2012) Nutritional interventions to prevent and treat osteoarthritis. Part I: focus on fatty acids and macronutrients. PM&R 4:S145–S154
Bastiaansen-Jenniskens YM, Siawash M, van de Lest CHA et al (2013) Monounsaturated and saturated, but not n-6 polyunsaturated fatty acids decrease cartilage destruction under inflammatory conditions: a preliminary study. Cartilage 4:321–328
Wang Y, Wluka AE, Hodge AM et al (2008) Effect of fatty acids on bone marrow lesions and knee cartilage in healthy, middle-aged subjects without clinical knee osteoarthritis. Osteoarthr Cartil 16:579–583
Davies-Tuck ML, Hanna F, Davis SR et al (2009) Total cholesterol and triglycerides are associated with the development of new bone marrow lesions in asymptomatic middle-aged women—a prospective cohort study. Arthritis Res Ther 11:R181
Doré D, de Hoog J, Giles G et al (2012) A longitudinal study of the association between dietary factors, serum lipids, and bone marrow lesions of the knee. Arthritis Res Ther 14:R13
Ravalli S, Szychlinska MA, Leonardi RM et al (2018) Recently highlighted nutraceuticals for preventive management of osteoarthritis. World J Ortop 9:255
Veronese N, Stubbs B, Noale M et al (2017) Adherence to a Mediterranean diet is associated with lower prevalence of osteoarthritis: data from the osteoarthritis initiative. Clin Nutr 36:1609–1614
Veronese N, Shivappa N, Stubb B, Smith T, Hébert JR, Cooper C et al (2017) The relationship between the dietary inflammatory index and prevalence of radiographic symptomatic osteoarthritis: data from the osteoarthritis initiative. Eur J Nutrition. https://doi.org/10.1007/s00394-017-1589-6
Veronese N, Koyanagi A, Stubbs B et al (2018) Mediterranean diet and knee osteoarthritis outcomes: a longitudinal cohort study. Clin Nutr. https://doi.org/10.1016/j.clnu.2018.11.032
Brien S, Lewith G, Walker A (2004) Bromelain as a treatment for osteoarthritis: a review of clinical studies. Evid Based Compl Alt 1:251–257
Cruz-Almeida Y, Sibille KT, Goodin BR et al (2014) Racial and ethnic differences in older adults with knee osteoarthritis. Arthritis Rheumatol 66:1800–1810
Glover TL, Goodin BR, Horgas AL et al (2012) Vitamin D, race, and experimental pain sensitivity in older adults with knee osteoarthritis. Arthritis Rheumatol 64:3926–3935
Collins JE, Deshpand BR, Katz JN et al (2016) Race-and sex-specific incidence rates and predictors of total knee arthroplasty: seven-year data from the osteoarthritis initiative. Arthritis Care Res 68:965–973
Peregoy J, Wilder FV (2011) The effects of vitamin C supplementation on incident and progressive knee osteoarthritis: a longitudinal study. Public Health Nutr 14:709–715
Chaganti RK, Tolstykh I, Javaid MK et al (2014) High plasma levels of vitamin C and E are associated with incident radiographic knee osteoarthritis. Osteoarthr Cartil 22:190–196
Jordan JM, De Roos AJ, Renner JB et al (2004) A case-control study of serum tocopherol levels and the alpha- to- gamma-tocopherol ratio in radiographic knee osteoarthritis: the Johnston County Osteoarthritis Project. Am J Epidemiol 159:968–977
Wluka AE, Stuckey S, Brand C et al (2002) Supplementary vitamin E does not affect the loss of cartilage volume in knee osteoarthritis: a 2 year double blind randomized placebo controlled study. J Rheumatol 29:2585–2591
Seki T, Hasegawa Y, Yamaguchi J et al (2010) Association of serum carotenoids, retinol, and tocopherols with radiographic knee osteoarthritis: possible risk factors in rural Japanese inhabitants. J Orthop Sci 15:477–484
Chin KY, Chin KY, Ima-Nirwana S (2018) The role of vitamin E in preventing and treating osteoarthritis—a review of the current evidence. Front Pharmacol 9:946
Thomas S, Browne H, Mobasheri A et al (2018) What is the evidence for a role for diet and nutrition in osteoarthritis? Rheumatology 57:iv61–iv74
Neogi T, Booth SL, Zhang YQ et al (2006) Low vitamin K status is associated with osteoarthritis in the hand and knee. Arthritis Rheum 54:125561
Oka H, Akune T, Muraki S et al (2009) Association of low dietary vitamin K intake with radiographic knee osteoarthritis in the Japanese elderly population: dietary survey in a population-based cohort of the ROAD study. J Orthop Sci 14:687–692
Misra D, Booth SL, Tolstykh I et al (2013) Vitamin K deficiency is associated with incident knee osteoarthritis. Am J Med 126:243–248
Shea MK, Kritchevsky SB, Hsu FC et al (2015) The association between vitamin K status and knee osteoarthritis features in older adults: the health, aging and body composition study. Osteoarthr Cartil 23:370–378
Neogi T, Felson DT, Sarno R et al (2008) Vitamin K and hand osteoarthritis: results from a randomised controlled trial. Ann Rheum Dis 67:1570–1573
Shea MK, Loeser RF, Hsu FC et al (2016) Vitamin K status and lower extremity function in older adults: the health aging and body composition study. J Gerontol A Biol Sci Med Sci 71:1348–1355
Heidari B, Heidari P, Hajian-Tilaki K (2011) Association between serum vitamin D deficiency and knee osteoarthritis. Int Orthop 35:1627–1631
Chaganti RK, Parimi N, Cawthon P et al (2010) Association of 25-hydroxyvitamin D with prevalent osteoarthritis of the hip in elderly men: the osteoporotic fractures in men study. Arthritis Rheumatol 62:511–514
Bergink AP, Uitterlinden AG, Van Leeuwen JP et al (2009) Vitamin D status, bone mineral density, and the development of radiographic osteoarthritis of the knee: the Rotterdam Study. J Clin Rheumatol 15:230–237
Felson DT, Niu J, Clancy M et al (2007) Low levels of vitamin D and worsening of knee osteoarthritis: results of two longitudinal studies. Arthritis Rheumatol 56:129–136
Zhang FF, Driban JB, Lo GH et al (2014) Vitamin D deficiency is associated with progression of knee osteoarthritis. J Nutr 144:2002–2008
McAlindon T, LaValley M, Schneider E et al (2013) Effect of vitamin D supplementation on progression of knee pain and cartilage volume loss in patients with symptomatic osteoarthritis: a randomized controlled trial. JAMA 309:155–162
Jin X, Jones G, Cicuttini F et al (2016) Effect of vitamin D supplementation on tibial cartilage volume and knee pain among patients with symptomatic knee osteoarthritis: a randomized clinical trial. JAMA 315:1005–1013
Sanghi D, Mishra A, Sharma AC et al (2013) Does vitamin D improve osteoarthritis of the knee: a randomized controlled pilot trial. Clin Orthop Rel Res 471:3556–3562
Zheng S, Jin X, Cicuttini F et al (2017) Maintaining vitamin D sufficiency is associated with improved structural and symptomatic outcomes in knee osteoarthritis. Am J Med 130:1211–1218
Fincham JE, Hough FS, Taljaard JJ et al (1986) Mseleni joint disease. Part II. Low serum calcium and magnesium levels in women. S Afr Med J 70:740–742
Hunter DJ, Hart D, Snieder H et al (2003) Evidence of altered bone turnover, vitamin D and calcium regulation with knee osteoarthritis in female twins. Rheumatology 42:1311–1316
Zhang Y, Xu J, Qin L et al (2016) Magnesium and osteoarthritis: from a new perspective. Ann Joint. https://doi.org/10.21037/aoj.2016.11.04
Weglicki WB, Phillips TM (1992) Pathobiology of magnesium deficiency: a cytokine/neurogenic inflammation hypothesis. Am J Physiol 263:R734–R737
Song Y, Manson JE, Cook NR et al (2005) Dietary magnesium intake and risk of cardiovascular disease among women. Am J Cardiol 96:1135–1141
Zeng C, Li H, Wei J et al (2015) Association between dietary magnesium intake and radiographic knee osteoarthritis. PLoS One 10:e0127666
Qin B, Shi X, Samai PS et al (2012) Association of dietary magnesium intake with radiographic knee osteoarthritis: results from a population-based study. Arthritis Care Res 64:1306–1311
Shmagel A, Onizuka N, Langsetmo L et al (2018) Low magnesium intake is associated with increased knee pain in subjects with radiographic knee osteoarthritis: data from the osteoarthritis initiative. Osteoarthr Cartil 26:651–658
Downey CM, Horton CR, Carlson BA et al (2009) Osteo-chondroprogenitor-specific deletion of the selenocysteine tRNA gene, Trsp, leads to chondronecrosis and abnormal skeletal development: a putative model for Kashin-Beck disease. PLoS Genet 5:e1000616
Li S, Xiao T, Zheng B (2012) Medical geology of arsenic, selenium and thallium in China. Sci Total Environ 421:31–40
Zou K, Liu G, Wu T et al (2009) Selenium for preventing Kashin-Beck osteoarthropathy in children: a meta-analysis. Osteoarthr Cartil 17:144–151
Xie D, Liao Y, Yue J et al (2018) Effects of five types of selenium supplementation for treatment of Kashin-Beck disease in children: a systematic review and network meta-analysis. BMJ Open 8:e017883
Kim JH, Jeon J, Shin M et al (2014) Regulation of the catabolic cascade in osteoarthritis by the zinc-ZIP8-MTF1 axis. Cell 156:730–743
Vinatier C, Merceron C, Guicheux J (2016) Osteoarthritis: from pathogenic mechanisms and recent clinical developments to novel prospective therapeutic options. Drug Discov Today 21:1932–1937
Radakovich LB, Marolf AJ, Santangelo KS (2017) ‘Iron accumulation’ gene expression profile in obese Hartley guinea pig knee joints is associated with more severe osteoarthritis. Osteoarthr Cartil 25:S169
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Author Osvaldo Daniel Messina has received honoraria for speaking from Pfizer, Eli Lilly and American Health Foundation. Author Maritza Vidal Wilman has received financial support for attending symposia from PeruLab. Author Luis F Vidal Neira has received honoraria for speaking from Expanscience, Menarini, MSD, PeruLab, Sanofi, Eli Lilly and American Health Foundation.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Messina, O.D., Vidal Wilman, M. & Vidal Neira, L.F. Nutrition, osteoarthritis and cartilage metabolism. Aging Clin Exp Res 31, 807–813 (2019). https://doi.org/10.1007/s40520-019-01191-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-019-01191-w