
Abstract
Purpose
To (1) assess dietary intakes of pregnant women with previous bariatric surgery in comparison with Dietary Reference Intakes (DRIs); (2) compare their dietary intakes as well as their diet quality with a control group of pregnant women with no history of bariatric surgery.
Methods
Twenty-eight (28) pregnant women with previous surgery (sleeve gastrectomy, n = 7 and biliopancreatic diversion with duodenal switch, n = 21) were matched for pre-pregnancy body mass index with 28 pregnant women with no history of bariatric surgery. In at least one trimester, participants completed a minimum of 2 Web-based 24-h dietary recalls from which energy, macro- and micronutrient intakes as well as the Canadian Healthy Eating Index (C-HEI) were derived.
Results
No differences were observed for energy intake between groups. All women had protein intakes within the recommended range, but most women with previous surgery had carbohydrate (67%) and dietary fiber intakes (98%) below recommendations. In both groups, mean total fat, saturated fatty acids, free sugars and sodium intakes were above recommendations, as opposed to mean vitamin D, folic acid and iron dietary intakes below recommendations for most women. Compared with the control group, pregnant women with previous bariatric surgery had lower overall C-HEI scores.
Conclusion
These results suggest that pregnant women with previous bariatric surgery would benefit from a nutritional follow-up throughout their pregnancy.
Level of evidence
III: Evidence obtained from well-designed cohort or case–control analytic studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
An increasing number of childbearing age women with severe obesity now undergo bariatric surgery [1]. Weight loss surgeries, especially those with a malabsorptive component such as biliopancreatic diversion with duodenal switch (BPD) and Roux-en-Y gastric bypass (RYGB), are associated with improvements in maternal and fetal pregnancy outcomes [2]. However, it is also associated with insufficient gestational weight gain and delivery of small for gestational age neonates [3, 4].
To ensure optimal fetal development and sustain the mother`s physiological changes, the requirements for energy and specific nutrients are increased during pregnancy [5]. For pregnant women who underwent bariatric surgery, nutrition may be more challenging. Stomach volume reduction following some bariatric procedures can reduce food intake, whereas malabsorption associated with mixed restrictive and malabsorptive surgeries can exacerbate the risk of nutritional deficiencies [6]. Moreover, gastrointestinal symptoms, food intolerances and aversions sometimes developed following weight loss surgeries can increase malnutrition risk during pregnancy [7, 8].
Despite the importance of diet during pregnancy, very few studies have characterized dietary intakes in pregnant women with previous bariatric surgery. Studies have mostly focused on micronutrient supplementation and serum concentrations rather than dietary intakes [6, 9]. However, some authors suggested that in pregnant women with previous bariatric surgery, macronutrient intakes, especially protein, as well as micronutrient intakes, like folate and vitamin B12, do not meet nutritional requirements during pregnancy and that diet quality is poor, irrespective of the type of surgery [10, 11]. Literature on the diet adopted by pregnant women with previous bariatric surgery is scarce and a better understanding of it would help target interventions that aim at improving maternal and fetal outcomes.
In this study conducted in pregnant women with previous bariatric surgery (BPD or sleeve gastrectomy), the objectives were to: (1) assess their dietary intakes at each trimester in comparison with the Dietary Reference Intakes (DRIs); and (2) compare their dietary intakes as well as the diet quality with a control group of pregnant women with no history of bariatric surgery.
Materials and methods
Study population
Forty (40) pregnant women who underwent bariatric surgery were recruited from May 2017 to August 2020 at the CHU de Québec-Université Laval (Québec City, Qc, Canada). Exclusion criteria were twin pregnancy, severe medical condition (i.e., type 1 or type 2 diabetes, renal disease, inflammatory and autoimmune disorders), gestational age greater than 24 weeks at enrollment and being younger than 18 years. Twelve (12) participants were excluded due to miscarriage (n = 4) or lack of time to devote to the project (n = 8). Our final sample includes 28 women for whom nutritional data was available for at least one trimester. Each participant was individually matched (1:1) for pre-pregnancy body mass index (BMI) (± 0.3 kg/m2) with a pregnant woman from the ANGE (Apports Nutritionnels Durant la GrossessE) cohort (control group), a prospective study that aimed to characterize the dietary intakes of pregnant women with no history of bariatric surgery [12]. This study was performed in line with the principles of the Declaration of Helsinki. The Institutional Ethics Committee approved the project (Reference number: MP-20-2017-3217) and all participants gave their informed written consent.
The automated web-based 24-h recall (R24W)
Within 21 days, participants were asked to complete two to three Web-based 24-h dietary recalls during at least one trimester, using the R24W (Rappel de 24 h Web) platform. The R24W has been validated in the general as well as in a pregnant population [13,14,15]. The R24W database is linked to the 2015 Canadian Nutrient File, allowing for an automatic assessment of the nutrient values for all food items reported in a 24-h period. Data on energy intake, macronutrients and some micronutrients of interest such as vitamin D, iron, folate, vitamin B12, calcium and sodium, originating from food intake, not supplements, were analyzed and compared to the DRIs.
Canadian healthy eating index
At each trimester, diet quality was assessed using the Canadian Healthy Eating Index (C-HEI) [16, 17]. The HEI score has been used by many authors to assess diet quality in the general population as well as in pregnant women [16, 18]. The total C-HEI score, which ranges from 0 to 100 points, represents the degree to which diet meets the 2007 Canada’s Food Guide recommendations, which were in effect at the beginning of the study. The total score is divided into eight adequacy components and three moderation components with scores varying between 0, 5, 10 or 20 points based on the scoring criteria.
Other web questionnaires
Web-based questionnaires were completed to collect information on medical history, medication, tobacco use, eating habits, education and household income.
Statistical analyses
Based on recommendations that suggest delaying pregnancy for 12–18 months after bariatric surgery [19, 20], analyses of variance (ANOVA) were used to compare energy intake according to surgery-to-conception interval (≤ 18, 19–60, > 60 months) in women with previous surgery. Tukey’s honestly significant difference (HSD) post-hoc test was used to account for multiple comparisons. Macronutrients as percentage of energy were compared with the acceptable macronutrient distribution range (AMDR) and the proportion of women with values below or above the AMDR were calculated [21]. The percentage of participants who had micronutrient intakes below the estimated average intakes (EARs) or above the upper intake limit (UL), as applicable, were also calculated [21]. Continuous and categorical variables were compared using paired t-tests and chi-squared tests, respectively. P-values ≤ 0.05 were considered significant. All statistical analyses were performed using JMP, version 14 (SAS Institute Inc., Cary, NC, USA).
Results
Participants’ characteristics
Mean pre-surgery BMI of women who underwent surgery was 49.1 ± 6.9 kg/m2, 75% had BPD and half of them had a surgery-to-conception interval greater than 60 months (Table 1). The mean pre-pregnancy BMI of women with and without surgery was 31.6 ± 5.6 kg/m2 and 31.3 ± 5.9 kg/m2 respectively, and despite the surgery, 60% of women had a pre-pregnancy BMI ≥ 30 kg/m2. Both groups were similar in age, parity, household income and frequency of dining-out. However, women with previous surgery had a significantly lower education level compared to the control group.
Regarding completion of the dietary recalls, in the first trimester (range: 9.0–13.0 weeks), among women with previous bariatric surgery, 35% (n = 6) had completed two recalls, while 65% (n = 11) had completed three. Those percentages were 29% (n = 6) and 71% (n = 15) in the second trimester (range: 21.6–27.0 weeks), and 31% (n = 5) and 69% (n = 11) in the third trimester (range: 31.7–37.7 weeks). All women in the control group completed three recalls per trimester (ranges: 9.0–13.3, 21.9–26.3, 32.7–36.1 weeks).
Energy and macronutrients
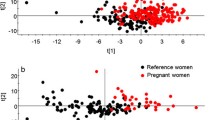
Mean energy intake did not differ between women with and without surgery (Table 2). Energy intakes measured during the second trimester were significantly higher in women with a longer surgery-to-conception interval (Fig. 1). Similar trends were observed in the first and third trimesters. Percentage of energy from protein was within the AMDR for all participants (Table 2). However, in the third trimester, women with previous surgery consumed a significantly higher percentage of energy from protein compared to the control group. Carbohydrate as a percentage of energy intake as well as fiber intake were significantly lower in women with previous surgery compared to the control group. Carbohydrate and fiber intakes were below recommendations for most women in both groups, but this trend was more pronounced in women with a history of surgery. Mean percentage of energy from free sugars did not differ between groups and was above the 10% recommended limit [22]. Energy intake from fat as well as from saturated fatty acids exceeded recommendations for most women in both groups.

Total energy intakes according to surgical-to-conception interval for the first (a), second (b) and third (c) trimesters
Micronutrients
Micronutrient intakes were similar between groups (data not shown). Suboptimal dietary intakes of vitamin D, folate and iron and excessive sodium intake were reported by most women from both groups at each trimester (data not shown).
Diet quality
In the first and second trimesters, total C-HEI scores were significantly lower in pregnant women with previous surgery compared to the control group, while this difference was not significant in the third trimester (Table 3). Women with previous surgery also had significantly lower scores for the following components: fruits and vegetables, whole fruits, dark green and orange vegetables, total grain products and whole grains.
Discussion
To our knowledge, this is the first study to precisely characterize trimester-specific dietary intakes as well as diet quality in pregnant women with previous bariatric surgery. Energy intake did not differ significantly between groups. However, in women with previous surgery, there was a trend for energy intake to be higher with longer surgery-to-conception interval. During the third trimester, women with previous surgery consumed a significantly higher proportion of proteins than the control group. Conversely, carbohydrate as well as dietary fiber intakes for most women with previous surgery were below the recommendations and were significantly lower compared to the control group. Overall, women with previous surgery had a poorer diet quality compared to the control group.
Energy intakes did not differ significantly between women with and without bariatric surgery. This could be explained by the surgery-to-conception interval, which was greater than 18 months for 82% of the participants. The procedure associated with BPD and SG does involve a significant resection of the stomach volume and, consequently, a reduction in food intake, but mostly during the first months after the procedure. It is why it is generally recommended that women wait at least 12 months after a SG and 18 months after a BPD before conceiving [19, 20]. The lack of difference in energy intakes is similar to the findings of Jans et al., who noted no significant difference in energy intake (measured in the first and third trimesters) between women who became pregnant on average 45.6 months after surgery (mainly RYGB) and pregnant women without history of surgery [23]. In addition, in the present study, women with previous surgery tended to have higher energy intakes with increasing surgery-to-conception interval. As energy intakes appear to be influenced by the surgery-to-conception interval, healthcare professionals should consider this factor in nutritional monitoring of pregnant women with previous surgery.
In the third trimester, women with previous surgery reported a significantly greater proportion of energy intake from protein compared to the control group. Women with previous surgery may have been encouraged by health professionals to consume more protein-rich foods toward the end of their pregnancy, which could explain the difference observed between groups. Currently, there are no guidelines for specific macro- and micronutrient consumption for pregnant women with a history of surgery except for an unendorsed recommendation of a minimum daily protein intake of 60 g, regardless of the surgical procedure [20, 24]. In the present study, women with previous surgery had protein intakes that were well above this recommendation. In contrast, daily protein intakes below 60 g have been reported by Coupaye et al. in pregnant women with previous SG or RYGB, while barely higher intakes were reported by Dias et al. in pregnant women with previous RYGB [25, 26]. The difference between their results and ours may be related to the type of surgery. Most women from our study had a BPD, a procedure known to induce a more pronounced protein deficiency than SG or RYGB, due to the short common limb [27]. Evaluating optimal protein requirements is a significant challenge for clinicians working with this population and the type of procedure should be considered in the elaboration of recommendations.
Carbohydrate and dietary fiber intakes of women with previous surgery were significantly lower than the control group and well below the DRI’s. Similar results were reported in Belgian pregnant women who had laparoscopic adjustable gastric banding (LAGB) or RYGB before pregnancy as well as in the non-pregnant bariatric populations [10, 28]. These results could be explained by the following: in the first post-surgery months, patients may have difficulty tolerating some complex carbohydrates and/or dietary fiber rich foods like bread, rice, pasta, vegetables and fruit skins [28]. Intolerances can persist for a few years after the procedure and may even cause food aversions [28]. Additionally, surgery can alter dietary preferences, which may also influence the patients’ food choices [29]. It is also of common practice to recommend that patients prioritize protein and micronutrient over starch intake after surgery [8, 24]. To date, the effects of a suboptimal carbohydrate intake on pregnancy outcomes in that population are under-studied.
Overall, diet quality of women with surgery was significantly lower than the control group in the first and second trimester. It is possible that food intolerances or aversions in women who had surgery influence dietary choices and therefore the overall diet quality [8]. Since the significant differences were observed for the adequacy components of the C-HEI, it could be hypothesized that food intolerances or aversions are more likely to affect ‘healthy’ foods. Indeed, the only components that differed significantly between groups were foods rich in complex carbohydrates or dietary fiber such as grain products and fruits and vegetables. According to some authors, being a younger and less educated woman is associated with a lower diet quality during pregnancy [30, 31]. In our study, women with previous surgery had a significantly lower level of education than the control group. Indeed, education level may explain in part the differences observed between the groups. Thus, food intolerances or aversions as well as education level of pregnant women with previous surgery should be considered when monitoring their diet quality.
Strength and limits
The use of a validated Web-based dietary assessment tool resulted in precise nutritional data at each trimester and the matched pairs design of the study considered the participants' pre-pregnancy BMI. Some limitations must be recognized including the small sample size and the large proportion of participants who did not complete the questionnaires at each trimester. Furthermore, the two types of surgery were not equally represented, which limits the generalization of our results and comparison between those surgeries. Missing data regarding education prevented us from adequately adjusting our results for this factor. Moreover, supplement use was not assessed, which did not allow us to evaluate the real risks of micronutrients deficiencies. Furthermore, only a small proportion of women did complete the physical acidity questionnaire, thus this variable was not considered. We did not have access to all medical records, which prevented us from assessing the association between diet and pregnancy outcomes. Finally, our study did not include questions about food intolerances or aversions developed following the operation.
Conclusion
Although weight loss surgery improves many pregnancy outcomes, it may increase the risk of nutritional deficiencies. Our results showed that dietary intakes of pregnant women after bariatric surgery were suboptimal in terms of macronutrient and micronutrient intakes and their overall diet quality required improvement. Women with previous surgery had a poorer diet quality mainly explained by lower intakes of fruits, vegetables and grain products, which translated into a significantly lower carbohydrate and dietary fiber intake. Reasons underlying the observed eating habits as well as the repercussions on maternal and fetal health are poorly documented. As nutrition is a major modifiable health variable, it is imperative that women with previous bariatric surgery benefit from continuous nutritional monitoring throughout pregnancy.
What is already known on this subject?
Pregnant women with previous bariatric surgery are at greater risk of nutritional deficiencies but no study precisely characterized their eating habits at each trimester of pregnancy.
What this study adds?
This study showed that dietary intakes of pregnant women with bariatric surgery are suboptimal in terms of nutrient intakes and overall diet quality.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
No software application or custom code were used for these analyses.
References
Welbourn R et al (2019) Bariatric surgery worldwide: baseline demographic description and one-year outcomes from the Fourth IFSO Global Registry Report 2018. Obes Surg 29(3):782–795
Carreau AM et al (2017) Pregnancy after bariatric surgery: balancing risks and benefits. Can J Diabetes 41(4):432–438
Balestrin B et al (2019) Pregnancy after bariatric surgery: a comparative study of post-bariatric pregnant women versus non-bariatric obese pregnant women. Obes Surg 29(10):3142–3148
Grandfils S et al (2019) Impact of gestational weight gain on perinatal outcomes after a bariatric surgery. J Gynecol Obstet Hum Reprod 48(6):401–405
Tsakiridis I et al (2020) Nutrition in pregnancy: a comparative review of major guidelines. Obstet Gynecol Surv 75(11):692–702
Devlieger R, et al (2014) Micronutrient levels and supplement intake in pregnancy after bariatric surgery: a prospective cohort study. PLoS ONE 9(12):e114192.
Boerlage TCC et al (2019) Gastrointestinal symptoms before and after laparoscopic Roux-en-Y gastric bypass: a longitudinal assessment. Surg Obes Relat Dis 15(6):871–877
Freeman RA et al (2014) Food tolerance and diet quality following adjustable gastric banding, sleeve gastrectomy and Roux-en-Y gastric bypass. Obes Res Clin Pract 8(2):e115-200
Rottenstreich A et al (2019) Maternal nutritional status and related pregnancy outcomes following bariatric surgery: a systematic review. Surg Obes Relat Dis 15(2):324–332
Guelinckx I et al (2012) Lifestyle after bariatric surgery: a multicenter, prospective cohort study in pregnant women. Obes Surg 22(9):1456–1464
Maslin K, et al (2019) What is known about the nutritional intake of women during pregnancy following bariatric surgery? A scoping review. Nutrients 11(9).
Savard C, et al (2018) Trimester-specific dietary intakes in a sample of french-canadian pregnant women in comparison with national nutritional guidelines. Nutrients 10(6).
Jacques S, et al (2016) Development of a web-based 24-h dietary recall for a French-Canadian population. Nutrients 8(11).
Lafrenière J et al (2018) Assessing the relative validity of a new, web-based, self-administered 24 h dietary recall in a French-Canadian population. Public Health Nutr 21(15):2744–2752
Savard C et al (2018) Validation of a self-administered web-based 24-hour dietary recall among pregnant women. BMC Pregnancy Childbirth 18(1):112
Garriguet D (2009) Diet quality in Canada. Health Rep 20(3):41–52
Kennedy ET et al (1995) The Healthy Eating Index: design and applications. J Am Diet Assoc 95(10):1103–1108
Moran LJ et al (2013) A decrease in diet quality occurs during pregnancy in overweight and obese women which is maintained post-partum. Int J Obes (Lond) 37(5):704–711
Bebber FE et al (2011) Pregnancy after bariatric surgery: 39 pregnancies follow-up in a multidisciplinary team. Obes Surg 21(10):1546–1551
Ciangura C et al (2019) Clinical practice guidelines for childbearing female candidates for bariatric surgery, pregnancy, and post-partum management after bariatric surgery. Obes Surg 29(11):3722–3734
Institute of Medicine (US) Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. DRI Dietary Reference Intakes: Applications in Dietary Assessment. Washington (DC): National Academies Press (US); 2000.
World Health Organization (2015) Guideline: sugars intake for adults and children. World Health Organization, Geneva
Jans G et al (2018) Depression and anxiety: lack of associations with an inadequate diet in a sample of pregnant women with a history of bariatric surgery-a multicenter prospective controlled cohort study. Obes Surg 28(6):1629–1635
Shawe J et al (2019) Pregnancy after bariatric surgery: consensus recommendations for periconception, antenatal and postnatal care. Obes Rev 20(11):1507–1522
Coupaye M et al (2018) Impact of Roux-en-Y gastric bypass and sleeve gastrectomy on fetal growth and relationship with maternal nutritional status. Surg Obes Relat Dis 14(10):1488–1494
Dias MC et al (2009) Body weight changes and outcome of pregnancy after gastroplasty for morbid obesity. Clin Nutr 28(2):169–172
De Carolis S et al (2018) Influence of biliopancreatic diversion on pregnancy outcomes in comparison to other bariatric surgery procedures. Obes Surg 28(10):3284–3292
Zarshenas N et al (2020) The relationship between bariatric surgery and diet quality: a systematic review. Obes Surg 30(5):1768–1792
Nance K, Acevedo MB, Pepino MY (2020) Changes in taste function and ingestive behavior following bariatric surgery. Appetite 146:104423
Doyle IM et al (2017) Determinants of dietary patterns and diet quality during pregnancy: a systematic review with narrative synthesis. Public Health Nutr 20(6):1009–1028
Savard C, et al (2019) Trimester-specific assessment of diet quality in a sample of Canadian pregnant women. Int J Environ Res Public Health 16(3)
Acknowledgements
We would like to acknowledge the valuable collaboration of Suzie Laroche and Mélanie Nadeau as well as the bariatric surgeons and clinical team at IUCPQ who contributed to the recruitment of participants. We thank Anaïs Desaulniers who participated in this project. We would also like to acknowledge the research team that developed the R24W platform and all the participants without whom the realization of this study would not have been possible. We finally recognize the help provided by Inès Auclair Mangliar for the linguistic revision of the manuscript.
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the conception and design of the manuscript, and all critically revised a first draft of the manuscript for important intellectual content. All authors participated in the interpretation of data. All authors gave their approval of the manuscript’s final version to be published and therefore take public responsibility for the content of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
We confirm that all procedures performed in the studies were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration.
Informed consent
Informed consent was also obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gagnon, G., Carreau, AM., Plante, AS. et al. Dietary intakes in pregnant women with previous bariatric surgery. Eat Weight Disord 27, 2063–2071 (2022). https://doi.org/10.1007/s40519-021-01333-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-021-01333-y