
Abstract
Purpose
The aim of the study was to verify whether ultrasound (US)-guided preoperative localization of breast lesions is an adequate technique for correct and safe surgical resection and to contribute positively and effectively to this topic in the literature with our results.
Methods
From June 2016 to November 2016, 155 patients with both benign and malignant breast lesions were selected from our institute to undergo US localization before surgery. The lesions included were:
-
sonographically visible and nonpalpable lesions;
-
palpable lesions for which a surgeon had requested US localization to better evaluate the site and extension;
-
sonographically visible, multifocal breast lesions, both palpable and nonpalpable.
US localization was performed using standard linear transducers (Siemens 18 L6, 5.5–8 MHz, 5.6 cm, ACUSON S2000 System, Siemens Medical Solutions). The radiologist used a skin pen to mark the site of the lesion, and the reported lesion’s depth and distance from the nipple and pectoral muscle were recorded. The lesions were completely excised by a team of breast surgeons, and the surgical specimens were sent to the Radiology Department for radiological evaluation and to the Pathology Department for histological assessment.
Results
In 155 patients who underwent to preoperative US localization, 188 lesions were found, and the location of each lesion was marked with a skin pen. A total of 181 lesions were confirmed by the final histopathologic exam (96.28%); 132 of them (72.92%) were malignant, and 124 of these (93.93%) showed free margins.
Conclusions
US-guided preoperative localization of sonographically visible breast lesions is a simple and nontraumatic procedure with high specificity and is a useful tool for obtaining accurate surgical margins.
Sommario
Obiettivo
Lo scopo dello studio è di verificare se la localizzazione preoperatoria eco-guidata delle lesioni mammarie sia una tecnica adeguata per una corretta e sicura resezione chirurgica ed è altresì quello di contribuire positivamente ed efficacemente, con i risultati ottenuti dal nostro istituto, all’approfondimento di questo argomento nella letteratura scientifica.
Metodi
Dal giugno 2016 al novembre 2016, 155 pazienti con lesioni mammarie benigne e maligne sono state selezionate dal nostro istituto per sostenere una localizzazione ecografica prima della seduta chirurgica.
Le lesioni considerate sono state:
-
lesioni ecograficamente visibili e non palpabili;
-
lesioni palpabili per le quali il chirurgo avesse richiesto una localizzazione ecografica per meglio valutarne sito ed estensione;
-
lesioni mammarie multifocali, ecograficamente visibili, sia palpabili che non palpabili.
La localizzazione ecografica è stata eseguita utilizzando trasduttori lineari standard (Siemens 18 L 6, 5.5–8 MHz, 5.6 cm, ACUSON S2000 System, Siemens Medical Solution).
Il radiologo ha utilizzato una penna per uso cutaneo per marcare il sito della lesione ed ha, dunque, calcolato e registrato profondità e distanza dal capezzolo e dal muscolo pettorale.
Le lesioni sono state completamente escisse dal team dei chirurghi mammari e i campioni chirurgici sono stati inviati al Dipartimento di Radiologia per una valutazione radiologica ed al Dipartimento di Anatomia patologica per una valutazione istologica.
Risultati
Nelle 155 pazienti, che sono state sottoposte a localizzazione ecografica pre-operatoria, sono state riscontrate 188 lesioni e il sito di ognuna di esse è stato marcato con una penna ad uso cutaneo.
Un totale di 181 lesioni è stato confermato dall’esame isto-patologico finale (96.28%); 132 di queste (72.92%) sono risultate maligne e 124 di queste ultime (93.93%) mostravano margini liberi da malattia.
Conclusioni
La localizzazione preoperatoria eco-guidata di lesioni mammarie ecograficamente visibili è una procedura semplice e non traumatica con un’elevata specificità ed è una metodica ideale per l’ottenimento di margini chirurgici indenni.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common cancer among women worldwide and is the leading cause of cancer-related death among women [1]; however, there is an excellent 5-year disease-free survival rate for node-negative breast cancer (98%) due to all the possible combination treatments [2].
Breast-conserving surgery (BCS) plus adjuvant radiotherapy has become the alternative treatment to mastectomy for early stage breast cancer because of equivalent survival [3, 4].
The rate of local recurrence after BCS and the margin status are strongly correlated [5, 6], as demonstrated by a large number of studies based on follow-up after BCS plus local radiotherapy [7, 8].
Only evident involvement of the tumor on the inked resection margins has been shown to confer a higher risk of local recurrence [9]; consequently, it is not necessary to remove a tumor with a large amount of adjacent breast tissue [9].
Therefore, resecting the mass with an appropriate disease-free margin (distance > 1 mm) is required [10].
For this purpose, many different localization techniques exist: the carbon marking technique, which is based on the injection of sterile charcoal powder into the site of a breast lesion after preoperative sonographic or stereotactic localization [11]; wire-guided localization (WGL), which consists of positioning a needle or a flexible wire into or alongside a nonpalpable breast lesion under mammographic or sonographic guidance [12]; and radio-guided occult lesion localization (ROLL), which depends on preoperative injection of radiopharmaceutical drugs into the tumor under sonographic or mammographic guidance, followed by a scintigraphy scan of the breast and localization of the tumor with a gamma probe during surgery [13, 14].
The ultrasound (US)-guided excision technique is used to localize breast lesions that are clearly visible on US using a high frequency probe. Furthermore, this technique can be performed with subsequent immediate positioning of a wire, injection of dye, skin marking, or direct calibration of the excision during surgery [15].
Some studies have demonstrated that intraoperative US localization is more accurate than wire localization and ROLL-guided surgery because it optimizes the surgeon’s ability to obtain adequate margins for nonpalpable invasive breast cancer [16,17,18,19].
Furthermore, a recent multicentric, randomized trial, named “cosmetic outcome of the breast after lumpectomy treatment” (COBALT), also reported negative margins and smaller volumes for breast resection in 97% of patients using intraoperative US-guided excision for palpable lesions [20, 21].
The aim of this study is to verify whether ultrasound-guided preoperative localization of breast lesions, performed in the Radiology Department before the surgery, is an adequate technique for correct and safe surgical resection and to contribute positively and effectively to this topic in the literature [22,23,24,25,26] with our results.
Materials and methods
From June 2016 to November 2016, breast surgeons at our institute treated 653 patients for both benign and malignant breast lesions.
Among these patients, we selected 155 patients who were referred for imaging-guided localization according to the following criteria.
Inclusion criteria:
-
sonographically visible, nonpalpable breast lesions (Figs. 1, 2);
Fig. 1 
Transverse sonogram showing a hypoechoic, nonpalpable, irregular shaped mass with spiculated margins
Fig. 2 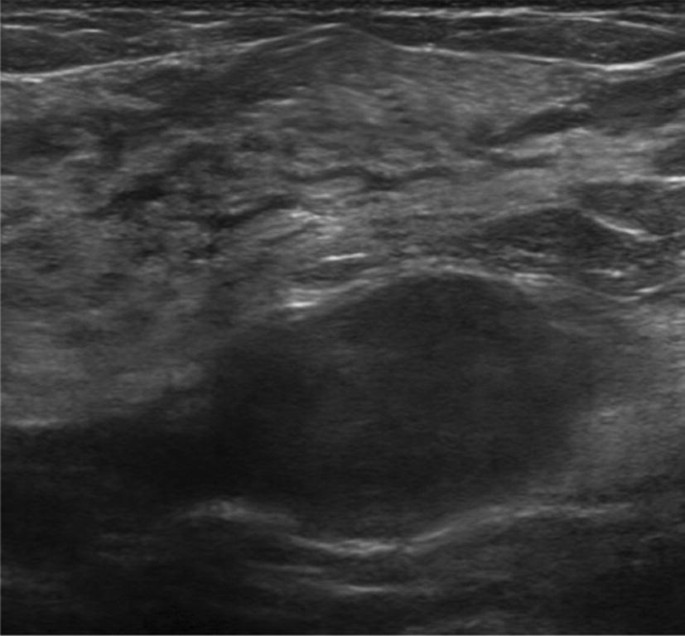
Transverse sonogram showing a hypoechoic, nonpalpable, oval shaped mass with circumscribed margins
-
palpable lesions for which a surgeon had requested US localization to better evaluate the site and extension of the lesion (Figs. 3, 4);
Fig. 3 
Transverse sonogram showing a hypoechoic, palpable, round shaped mass with microlobulated margins
Fig. 4 
Sagittal sonogram showing a hypoechoic, palpable, oval shaped mass with circumscribed margins
-
sonographically visible, multifocal breast lesions, both palpable and nonpalpable (Figs. 5, 6).
Fig. 5 
Sagittal sonogram showing hypoechoic, palpable, round shaped multifocal masses with indistinct margins
Fig. 6 
Sagittal sonogram showing hypoechoic, nonpalpable, round shaped multifocal masses with angular margins






Exclusion criteria:
-
lesions not visible by US;
-
patients referred for mastectomy;
All the lesion’s resections were followed by postoperative specimen US to verify that the resection was successful [27,28,29,30,31,32].
All the lesions had previously undergone US-guided fine-needle biopsy. We included both malignant lesions and benign lesions with suspicious radiological features [33, 34] that had increased in size or had inconclusive results on fine-needle biopsy.
US localization
All US localizations were performed in the Radiology Department, in the section of Breast Radiology, by 5 radiologists with at least 5 years of experience in breast imaging and who were acquainted with the previous exams of the patient. The exams were performed with a standard linear transducer (Siemens 18 L6 HD, 5.5–18 MHz, 5.6 cm, ACUSON S2000 System, Siemens Medical Solutions, Mountain View, CA) with the patients lying in the supine position with their arms in the same position as during the surgery.
The radiologists performed an examination of the known lesion site in the breast and placed a skin pen tattoo with a permanent pen marker to indicate the site of the lesion, reporting the depth of the tumor in relation to the skin level and its distance from the nipple and pectoral muscle. The pressure on the transducer was maintained to better determine the depth of the lesion.
The radiologists visualized the tumors at their largest diameter to achieve the optimal correspondence between the lesion and the skin markers.
The procedure was explained to all patients, who had been kindly asked not to wash the breast skin before surgery.
Surgery
Depending on the size and location of the tumor, and the size and shape of the patient’s breasts, different oncoplastic surgical techniques were used. The planned incision was marked on the skin; the patient’s breast was then prepped and draped; the incision was made, and dissection proceeded to the area of the lesion immediately under the preoperatively placed skin tattoo. The excised tissue was placed inside a transparent bag and sent to the Radiology Department for US evaluation. If the specimen included the entire lesion, the surgeon was instructed to end the procedure. Otherwise, if the lesion appeared to be close to a margin, the surgeon was told to extend the excision before considering completing the procedure. The surgical specimen was then sent to the pathologists for histological assessment.
Study of postoperative specimens
We performed sonography on the specimens to confirm the complete excision of the targeted lesions. Sonography was performed using the same transducer utilized for the US-guided preoperative localizations, and the aim was to evaluate the presence of the lesions previously localized and measure their distance from the resection margins.
Pathological examination
After sonography, the surgical specimens were sent to the pathology laboratory for macroscopic and histological assessment.
The pathologists inked the entire specimen and divided the tissue from the inferior margin to the superior margin in multiple 5-mm-thick slices. Tumor localization was the first goal of the macroscopic evaluation, while the second goal was to establish the negativity of the margins by determining the macroscopic distance of the lesion from each margin [33]. We considered margins to be disease free if they were at least 1 mm away from the lesion. In case of a positive margin, pathologists recommended the surgeon extend the excision as well as where to extend the margin to.
Results
In 155 patients who underwent preoperative US localization, the radiologists found 188 lesions, and each lesion was localized by marking the skin of the breast with a tattoo pen.
One-hundred and forty patients had nonpalpable tumors, for a total of 173 lesions; the remaining 15 patients had palpable lesions (Table 1).
Every US-guided preoperative localization required from 3 to 8 min to complete, depending on the complexity of the case, with an average time of 5 min.
All 173 lesions were visualized by sonography of the specimens.
Of the 188 lesions, 181 were confirmed at the final histopathologic exam (96.28%), while in 7 cases (3.72%), the localized lesions corresponded to pseudonodular-like parenchymal areas.
Ten patients had multifocal lesions, for a total of 26 lesions, at the histopathologic exam and all of these lesions were visualized by US localization.
Of the 181 lesions found on histopathologic exam, 132 (72.92%) were malignant and 49 were benign (27.08%) (Table 2).
Of the 132 malignant lesions, 124 (93.93%) showed margins free from neoplasia at the histopathologic exam, and 8 lesions (6.06%) presented involved margins: in 5 cases (62.5%), the involvement was due to an in situ component of ductal carcinoma, pagetoid dissemination or the presence of satellite microlesions (Table 3).
The maximum value obtained from the operative margin never exceeded 25 mm. The majority of our resections (56.6%) showed a distance from the margins ranging from 5 to 9 mm.
Out of the 49 benign lesions, 43 lesions (87.75%) were completely contained within the margins, with a minimal distance of 1 mm from the margins, while 6 lesions (12.25%), even if totally encompassed, were at a minimal distance from the surgical resection margins (Table 3).
Discussion
The complete removal of neoplasia and resection margins that are pathologically free of disease are the most important factors for reducing the rate of ipsilateral breast cancer recurrence after BCS [34,35,36]. For this purpose, it is important to obtain precise information on tumor location and extent in order to resect the pathological tissue with proper surgical margins.
We performed US-guided preoperative localization in 155 patients with 188 lesions, and each lesion was localized and marked with a breast skin tattoo.
One-hundred and forty patients had nonpalpable tumors, for a total of 173 lesions; the remaining 15 patients each had one palpable lesion. We included patients with palpable tumors whose surgeon had requested a US evaluation of the site and extent because many authors, including Krekel et al. and Moore et al. [14], recently demonstrated the efficacy of US-guided BCS in patients with palpable, invasive breast cancer.
US-guided preoperative localization was performed in the Radiology Department before the surgery and, depending on the complexity of the case, the procedure lasted approximately 3–8 min, with an average time of 5 min; a part of this time was to allow the radiologist to study the case and to make comparisons with previous examinations of the patient.
The procedure time is significantly lower than the time required for other common localization techniques. In fact, Lovrics et al. reported a mean operative time of 19 min for ROLL and 22 min for WGL [37, 38]. Instead, the extra time required for IOUS (calculated to be 21 min in a recent study) is mainly due to the presence of radiologists in the operating room, which increases the anesthesia time.
In our study, US-guided localization was performed outside the operating room, with a significant reduction in anesthesia time compared to IOUS.
In our study of 188 breast lesions, 181 were confirmed at the final histopathologic exam (95.21%) by pathologists. These results are in agreement with those reported in other studies on preoperative localization methods. Medina-Franco et al., in a study comparing ROLL versus WGL, reported that both techniques resulted in 100% retrieval of the lesions [36, 37]. Ngo et al. reported an identification of lesions in 95.7% of patients using IOUS [38]. In the literature, the rate of successful IOUS in US-visible, nonpalpable tumors varies between 95 and 100% [39,40,41,42,43].
In 7 lesions, the pathologist confirmed the presence of pseudonodular-like area of dense fibroglandular breast tissue in addition to the tumor, and the dimensions and morphology of this area corresponded to one of the two lesions we had localized.
In all the other cases of multifocal tumors, the lesions were localized by radiologists using US localization and were then confirmed by the pathologists. Overall, 10 patients had multifocal lesions, for a total of 26 lesions, which were confirmed by the histopathologic exam.
In our study, we considered both benign (Fig. 7) and malignant lesions (Fig. 8) because the localization techniques are the same between the two lesion types. The benign lesions were resected because they had doubtful or nondiagnostic biopsy results and had increased in size or because the results of fine-needle US-guided biopsy were inconclusive.

Sagittal sonogram showing a hypoechoic, nonpalpable, round shaped mass with circumscribed margins close to silicon breast prosthesis

Transverse sonogram showing a hypoechoic, palpable, round shaped mass with angular margins and intralesional coarse heterogeneous calcifications
We must remember that the primary aim of our localization method is to allow surgeons to perform BCS and remove the tumor with margins free of disease. Regarding this point, 124 of 132 malignant lesions (93.93%) showed margins free from neoplasia at the histopathologic exam, while 8 lesions (6.06%) had involved margins. These 8 patients required additional treatment such as re-excision or mastectomy.
Our results follow what is described in the literature regarding US-guided excision. In fact, some authors reported that US-guided excision of nonpalpable breast masses is practicable and even superior to needle localization excision [21]. The rate of success of IOUS in US–visible tumors varies between 95 and 100% for nonpalpable tumors.
Conversely, after WGL, positive margins are described in 10–43% of patients, with up to 40% re-excisions after the initial surgery. Moreover, Sajid et al. showed in a meta-analysis that clear margins obtained with WGL are reported to be 70.8–87.4%, while free margins reported with ROLL range from 75 to 93.5% [44]. Some studies have suggested that IOUS-guided excision can significantly lower the proportion of positive margins for breast cancer more than WGL for nonpalpable breast cancer. [39, 40].
The incidence of tumor-involved margins in BCS has been reported to reach up to 40%, but a real comparison of studies is difficult due to the use of multiple definitions for positive margins because of the absence of a clear definition of margin status. Some countries such as Germany and France have BCS guidelines that indicate that patients with margins ≤ 1 mm should undergo additional surgery. Other countries, such as the Netherlands and the United States, consider all specimens without tumor cells at the inked margins to be tumor-free margins. In the recent St. Gallen International Breast Cancer Conference 2015, the majority of the panelists agreed that the minimal acceptable surgical margin was “no inked invasive tumor” in women undergoing BCS for invasive breast cancer and proceeding to standard radiation and adjuvant systemic therapy. Furthermore, the meta-analysis of Houssami et al. concluded that the positive margins are defined as ink on invasive tumors or DCIS and are associated with an increased rate of local recurrence. Furthermore, there is a lack of evidence that margins wider than the ink line outside the tumor reduce the risk of local recurrence; thus, the routine use of re-excision to obtain larger disease-free margins is not indicated [34].
In our institute, we consider a margin free of disease if it is at least 1 mm from the neoplasia. The patients received postoperative radiotherapy and adjuvant chemotherapy depending on other pathological parameters (such as the presence of lymph nodes involvement, histotype, grading and receptor status).
In terms of our results, 5 out of 8 cases (62.5%) showed involved margins on histopathologic exam; the involvement was due to an in situ component of ductal carcinoma, pagetoid dissemination or the presence of satellite microlesions; therefore, they were not visible on US. As a result, our US-guided preoperative localization technique was able to obtain margins free from involvement in 93.93% of cases, but we must consider that it is not possible to identify the microscopic components, which would increase our margin-free percentage. Ultrasound is not normally able to view these components of a tumor, although the presence of in situ components is found to be an independent prognostic factor for re-excision by multivariate analysis for WGL [36]. In fact, some studies have shown that the presence of ductal carcinoma in situ is a factor that increases the number of cases with positive surgical margins regardless of the localization method used [45]. Moreover, it is known whether US is less sensitive in cases of intraductal carcinoma [46]. Therefore, only sonographically visible lesions can be localized using our method, and lesions that are visible by only mammography, such microcalcifications or parenchymal distortions, and not associated with sonographic signs, are not candidates for US localization [45, 47].
In addition to radical resection of the tumor, BCS also aims to obtain a good aesthetic result. Therefore, the calculated resection ratio (CRR) was introduced to indicate the excess of healthy tissue in the specimen resection. One retrospective study reported a significant difference in the CRR between ROLL and WGL, in which the amount of healthy tissue removed was higher in ROLL than WGL. However, in both techniques, the CRR indicated that a large amount of healthy tissue is resected [46]. Furthermore, Barentsz et al. showed that the total resection volumes are similar between IOUS and WGL [41]. In fact, poor cosmetic outcomes are currently observed in up to 30% of patients after BCS.
In our study, we cannot verify the volume of the excised tissue and relate it to cosmetic outcomes. Nevertheless, the maximum value obtained from the operative margin never exceeded 25 mm and the majority of our resections (56.6%) showed a distance from the margin ranging from 2 to 9 mm. Fortunato et al., in a prospective study of patients with breast tumors surgically treated and who underwent IOUS, obtained a median distance from the tumor to the closest margin of excision of 1.3 cm [43].
As stated previously, 49 lesions were benign at the histopathologic exam. In 43 cases (87.75%), the lesion was completely included in the resection, with a distance of at least 5 mm from the margins. In 6 cases (12.24%), the lesion, even if completely included in the resection, was at minimal distance from the resection margins. In a recent retrospective analysis of the margin status of patients with benign and low-grade breast neoplasms, Cowan et al. showed no statistically significant difference in the recurrence rate of patients who presented positive surgical margins (defined as < 5 mm) compared to those with disease-free surgical margins (> 5 mm) [48]. In our study, no patient had to undergo re-excision. In their study, Fortunato et al. [43] also considered benign tumors in the median distance from the tumor to the closest margins, but their results considered both benign and malignant lesions.
Our localization technique proved to be simple, rapid and safe to perform. Even if WGL and ROLL are currently the most widely used localization methods for the preoperative localization of nonpalpable breast lesions, both methods have many disadvantages such as patient discomfort at the insertion of the wire, the risk of wire migration, the possibility of vasovagal reactions, possible fragmentation of the wire, pneumothorax and perforation of the heart and aorta [13]. ROLL entails exposure to ionizing radiations and, in some cases, widespread dispersal of the isotope by accidental intraductal injection, possibly causing failure to detect the lesion [19].
Conversely, several studies have clearly demonstrated that IOUS has considerable advantages such as reduced preoperative stress and reduced discomfort for patients [12]. However, IOUS also has some limitations such as the presence of air and liquid in the wound that may create problems, thereby reducing the quality of the US images. In our study, we performed normal high frequency US localization, using a probe and a medical gel on undamaged skin; therefore, there were no artifacts due to the wound.
Our study also has some limitations, such as retrospective nature, the small number of patients and the short follow-up.
US-guided preoperative localization is a method that can be used for only sonographically visible lesions; therefore, when microcalcifications are present, it may be necessary to combine US localization with other techniques that facilitate tumor resection.
Postbiopsy hematoma can, moreover, cover the lesion itself or the biopsy marker clip; therefore, it may be necessary to combine US localization with other techniques.
Furthermore, with our method, it is not possible to achieve real-time visualization of the resection margins and to direct the surgery during the excision.
Finally, US-guided preoperative localization does have the disadvantage of being operator dependent; nevertheless, in our study, it has yielded a specificity of 96.28%.
Many authors, including Ricci et al. and Di Segni et al., recently showed that Breast Elastography and S-Detect may be used as additional diagnostic tools to improve the specificity of US-guided preoperative localization and guides in decision making for breast lesions detected on US [49, 50].
We obviously need to enlarge our number of patients in order to confirm the results obtained.
Conclusions
US-guided preoperative localization is a simple, nontraumatic procedure that is relatively fast if executed by a radiologist who is experienced in breast imaging. The success rate of US localization is similar to that of other breast lesion preoperative localization techniques.
Our technique is associated with accurate surgical margins and a very low re-excision rate for positive margins, and it has high specificity for localizing tumors, thus avoiding the unpleasant insertion of a wire.
US localization was determined to be particularly useful for the study of patients with multifocal lesions.
Radiologists can perform US-guided localization prior to surgery and patient anesthesia and they may calmly evaluate the patient’s previous exams to obtain the optimal lesion localization.
To obtain the best possible results and to achieve optimal tumor resection with a good cosmetic outcome, it is essential to have close cooperation between the radiologists, surgeons and pathologists.
References
Anderson BO, Lipscomb J, Murillo RH et al (2015) Disease Control Priorities, Third Edition (Volume 3). The International Bank for Reconstruction and Development/The World Bank, Washington (DC) (Chapter 3)
Krekel NM, Zonderhuis BM, Schreurs HW et al (2011) Ultrasound-guided breast-sparing surgery to improve cosmetic outcomes and quality of life. A prospective multicentrerandomised controlled clinical trial comparing ultrasound-guided surgery to traditional palpation-guided surgery (COBALT trial). BMC Surg 11:8. https://doi.org/10.1186/1471-2482-11-8
Fisher B, Anderson S, Bryant J et al (2002) Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 347:1233–1241
Veronesi U, Cascinelli N, Mariani L et al (2002) Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 347:1227–1232
Singletary SE (2002) Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg 184:383–393
Corsi F, Sorrentino L, Bossi D et al (2013) Preoperative localization and surgical margins in conservative breast surgery. Int J Surg Oncol 2013:793819. https://doi.org/10.1155/2013/793819 (Epub 2013 Aug 5)
Park CC, Mitsumori M, Nixon A et al (2000) Outcome at 8 years after breast-conserving surgery and radiation therapy for invasive breast cancer: influence of margin status and systemic therapy on local recurrence. J Clin Oncol 18(8):1668–1675
Peterson ME, Schultz DJ, Reynolds C, Solin LJ (1999) Outcomes in breast cancer patients relative to margin status after treatment with breast-conserving surgery and radiation therapy: the University of Pennsylvania experience. Int J Radiat Oncol Biol Phys 43(5):1029–1035
Taghian A, Mohiuddin M, Jagsi R et al (2005) Current perceptions regarding surgical margin status after breast-conserving therapy: results of a survey. Ann Surg 241:629–639
Hershman DL, Buono D, Jacobson JS et al (2009) Surgeon characteristics and use of breast conservation surgery in women with early stage breast cancer. Ann Surg 249(5):828–833. https://doi.org/10.1097/SLA.0b013e3181a38f6f
Volders JH, Haloua MH, Krekel NM et al (2016) Current status of ultrasound-guided surgery in the treatment of breast cancer. World J Clin Oncol 7(1):44–53. https://doi.org/10.5306/wjco.v7.i1.44
Rahusen FD, Bremers AJA, Fabry HFJ et al (2002) Ultrasound-guided lumpectomy of nonpalpable breast cancer versus wire-guided resection: a randomized clinical trial. Ann SurgOncol 9:994–998
Rovera F, Frattini F, Marelli M et al (2008) Radio-guided occult lesion localization versus wire-guided localization in non-palpable breast lesions. Int J Surg 6(Suppl 1):S101–S103. https://doi.org/10.1016/j.ijsu.2008.12.010 (Epub 2008 Dec 13)
Krekel NM, Haloua MH, Cardozo AML et al (2013) Intraoperative ultrasound guidance for palpable breast cancer excision: a multicentre, randomised controlled trial. Lancet Oncol 14:48–54
Bennett I, Biggar M (2011) Intraoperative ultrasonography-guided excision of nonpalpable breast lesions. World J Surg 35(8):1835–1839. https://doi.org/10.1007/s00268-011-1082-y
Snider HC, Morrison DG (1999) Intraoperative ultrasound localization of nonpalpable breast lesions. Ann Surg Oncol 6(3):308–314
Dogan BE, Whitman GJ (2011) Intraoperative breast ultrasound. Semin Roentgenol 46(4):280–284. https://doi.org/10.1053/j.ro.2011.02.009
Kaufman CS, Jacobson L, Bachman B et al (2003) Intraoperative ultrasonography guidance is accurate and efficient according to results in 100 breast cancer patients. Am J Surg 186(4):378–382
Ivanovic NS, Zdravkovic DD, Skuric Z et al (2015) Optimization of breast cancer excision by intraoperative ultrasound and marking needle—technique description and feasibility. World J Surg Oncol 18(13):153. https://doi.org/10.1186/s12957-015-0568-8
Volders JH, Haloua MH, Krekel NM et al (2017) Intraoperative ultrasound guidance in breast-conserving surgery shows superiority in oncological outcome, long-term cosmetic and patient-reported outcomes: final outcomes of a randomized controlled trial (COBALT). Eur J Surg Oncol 43(4):649–657. https://doi.org/10.1016/j.ejso.2016.11.004 (Epub 2016 Nov 23)
Karanlik H, Ozgur I, Sahin D et al (2015) Intraoperative ultrasound reduces the need for re-excision in breast-conserving surgery. World J Surg Oncol 13:321
Chan BK, Wiseberg-Firtell JA, Jois RH (2015) Localization techniques for guided surgical excision of non-palpable breast lesions. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.cd009206.pub2
Inoue T, Tamaki Y, Sato Y et al (2005) Three-dimensional ultrasound imaging of breast cancer by a real-time intraoperative navigation system. Breast Cancer 12(2):122–129
Yu CC, Chiang KC, Kuo WL et al (2013) Low re-excision rate for positive margins in patients treated with ultrasound-guided breast-conserving surgery. Breast 22(5):698–702. https://doi.org/10.1016/j.breast.2012.12.019 (Epub 2013 Jan 17)
Moore MM, Whitney LA, Cerilli L et al (2001) Intraoperative ultrasound is associated with clear lumpectomy margins for palpable infiltrating ductal breast cancer. Ann Surg 233:761–768
DeJean P, Brackstone M, Fenster A (2010) An intraoperative 3D ultrasound system for tumor margin determination in breast cancer surgery. Med Phys 37:564–570
Mesurolle B, El-Khoury M, Hori D et al (2006) Sonography of postexcision specimens of nonpalpable breast lesions: value, limitations, and description of a method. AJR Am J Roentgenol 186(4):1014–1024
Kendall T, Clarke J, Carmichael J (2008) The use of specimen ultrasound in the identification of screen-detected breast lesions. Histopathology 52(7):903–904. https://doi.org/10.1111/j.1365-2559.2008.03048.x (Epub 2008 May 6)
Ciccarelli G, Di Virgilio MR, Menna S et al (2007) Radiography of the surgical specimen in early stage breast lesions: diagnostic reliability in the analysis of the resection margins. Radiol Med 112:366–376
Lee KY, Seo BK, Yi A et al (2008) Immersion ultrasonography of excised nonpalpable breast lesion specimens after ultrasound-guided needle localization. Korean J Radiol 9(4):312–319. https://doi.org/10.3348/kjr.2008.9.4.312
Versteegden DPA, Keizer LGG, Schlooz-Vries MS et al (2017) Performance characteristics of specimen radiography for margin assessment for ductal carcinoma in situ: a systematic review. Breast Cancer Res Treat 166(3):669–679. https://doi.org/10.1007/s10549-017-4475-2 (Epub 2017 Aug 22)
Moschetta M, Telegrafo M, Introna T et al (2015) Role of specimen US for predicting resection margin status in breast conserving therapy. G Chir 36(5):201–204
Ramos M, Díaz JC, Ramos T et al (2013) Ultrasound-guided excision combined with intraoperative assessment of gross macroscopic margins decreases the rate of reoperations for non-palpable invasive breast cancer. Breast 22(4):520–524. https://doi.org/10.1016/j.breast.2012.10.006 (Epub 2012 Oct 27)
Houssami N, Macaskill P, Marinovich ML et al (2014) The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol 21:717–730
Cabioglu N, Hunt KK, Sahin AA (2007) Role for intraoperative margin assessment in patients undergoing breast-conserving surgery. Ann Surg Oncol 14(4):1458–1471
Tóth D, Varga Z, Sebő É, Török M, Kovács I (2016) Predictive factors for positive margin and the surgical learning curve in non-palpable breast cancer after wire-guided localization—prospective study of 214 consecutive patients. Pathol Oncol Res 22(1):209–215. https://doi.org/10.1007/s12253-015-9999-3 (Epub 2015 Nov 2)
Medina-Franco H, Abarca-Pérez L, García-Alvarez MN et al (2008) Radioguided occult lesion localization (ROLL) versus wire-guided lumpectomy for non-palpable breast lesions: a randomized prospective evaluation. J Surg Oncol 97(2):108–111. https://doi.org/10.1002/jso.20880
Lovrics PJ, Goldsmith CH, Hodgson N et al (2011) A multicentered, randomized, controlled trial comparing radioguided seed localization to standard wire localization for nonpalpable, invasive and in situ breast carcinomas. Ann Surg Oncol 18(12):3407–3414. https://doi.org/10.1245/s10434-011-1699-y (Epub 2011 Apr 30)
Haid A, Knauer M, Dunzinger S et al (2007) Intra-operative sonography: a valuable aid during breast-conserving surgery for occult breast cancer. Ann Surg Oncol 14:3090–3101
Ngô C, Pollet AG, Laperrelle J et al (2007) Intraoperative ultrasound localization of nonpalpable breast cancers. Ann Surg Oncol 14(9):2485–2489 (Epub 2007 May 31)
Barentsz MW, van Dalen T, Gobardhan PD et al (2012) Intraoperative ultrasound guidance for excision of non-palpable invasive breast cancer: a hospital-based series and an overview of the literature. Breast Cancer Res Treat 135(1):209–219
Monti S, Galimberti V, Trifiro G et al (2007) Occult breast lesion localization plus sentinel node biopsy (SNOLL): experience with 959 patients at the European Institute of Oncology. Ann Surg Oncol 14(10):2928–2931 (Epub 2007 Aug 1)
Fortunato L, Penteriani R, Farina M et al (2008) Intraoperative ultrasound is an effective and preferable technique to localize non-palpable breast tumors. Eur J Surg Oncol 34(12):1289–1292. https://doi.org/10.1016/j.ejso.2007.11.011 (Epub 2008 Jan 14)
Sajid MS, Parampalli U, Haider Z et al (2012) Comparison of radioguided occult lesion localization (ROLL) and wire localization for non-palpable breast cancers: a meta-analysis. J Surg Oncol 105(8):852–858. https://doi.org/10.1002/jso.23016 (Epub 2011 Dec 27)
Nagashima T, Hashimoto H, Oshida K et al (2005) Ultrasound demonstration of mammographic detected microcalcifications in patients with ductal carcinoma in situ of the breast. Breast Cancer 12:216–220
Krekel NM, Zonderhuis BM, Stockmann HB et al (2011) A comparison of three methods for nonpalpable breast cancer excision. Eur J Surg Oncol 37(2):109–115
Berg WA, Gutierrez L, NessAiver MS et al (2004) Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 233:830–849
Cowan ML, Argani P, Cimino-Mathews A (2016) Benign and low-grade fibroepithelial neoplasms of the breast have low recurrence rate after positive surgical margins. Mod Pathol 29:259–265
Ricci P, Maggini E, Mancuso E et al (2014) Clinical application of breast elastography: state of the art. Eur J Radiol 83(3):429–437. https://doi.org/10.1016/j.ejrad.2013.05.007 (Epub 2013 Jun 18)
Di Segni M, De Soccio V, Cantisani V et al (2018) Automated classification of focal breast lesions according to S-detect: validation and role as a clinical and teaching tool. J Ultrasound 21(2):105–118. https://doi.org/10.1007/s40477-018-0297-2 (Epub 2018 Apr 21)
Author information
Authors and Affiliations
Contributions
I confirm that all the authors have made a significant contribution to this manuscript, have seen and approved the final manuscript, and have agreed to its submission to “Journal of Ultrasound”.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Carlino, G., Rinaldi, P., Giuliani, M. et al. Ultrasound-guided preoperative localization of breast lesions: a good choice. J Ultrasound 22, 85–94 (2019). https://doi.org/10.1007/s40477-018-0335-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-018-0335-0