
Abstract
Background
The use of intraoperative ultrasonography (US) to localize and guide excision of nonpalpable breast lesions has advantages over other techniques. It avoids the need for additional resources and minimizes patient morbidity.
Methods and results
The technique of surgeon-performed US-guided excision as described in this report is straightforward and safe, easily reproducible, and suitable for teaching.
Conclusions
The US-guided breast excision technique is predictable and accurate, minimizes costs, and is advocated as an appropriate method for US-visible lesions requiring surgical excision. With appropriate training, breast surgeons can easily acquire the necessary skills to incorporate the use of US in their surgical practice.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In recent years, particularly with the advent of new, smaller, portable, high-quality ultrasonography (US) machines, there has been a growing trend for surgeons to utilize US in both the office and the operating theater. Breast surgeons in particular are increasingly incorporating this tool into their everyday practice [1–3].
Surgeon-performed US-guided breast biopsy is a reliable and invaluable means of assessing breast lesions as an office-based procedure [3]. The natural extension of office-based US is its application in the operating theater. US-guided excision of impalpable breast lesions is a highly useful, readily acquired skill that many breast surgeons have been able to adopt [4–7]. However, training and accreditation in surgeon-performed US is important as part of this process to ensure that patients are offered high quality care. It has been demonstrated that dedicated US workshops are an effective means of educating surgeons and surgical trainees in attaining the necessary skills [8]. Moreover, practical in-house training and supervision can be undertaken by surgeons who are experienced in US techniques in both the outpatient setting and in theater.
Since the advent of mammographic breast screening and the more liberal use of US, atypical breast lesions and early breast cancers are increasingly being detected in a nonpalpable growth phase. Options for localization of the nonpalpable breast lesions requiring open surgical excision have traditionally included preoperative hookwire placement [9–11], the carbon injection technique [12] and radio-guided occult lesion localization (ROLL) [13]. More recently with a larger number of breast surgeons gaining competence in the use of US in their clinical practice, the technique of intraoperative US (IOUS) localization is increasingly being utilized and recognized as an appropriate and safe technique [4–7]. The advantages of surgeon-performed IOUS-guided excision of nonpalpable breast lesions over the other techniques include the following: (1) reduced patient anxiety and discomfort preoperatively; (2) avoidance of the need for day-of-surgery organizational requirements to coordinate placement of the hookwire by a radiologist and for obtaining confirmation that the specimen contains all of the offending lesion with good margins; (3) avoidance of the potential complications of hookwire use, including inadvertent displacement and the risk of pneumothorax; and (4) reduced operating time as on-table sonography of the specimen provides immediate confirmation of lesion removal. IOUS guidance has also been demonstrated to be associated with improved margins of clearance for neoplastic lesions at the first surgical procedure, thereby reducing the need for patients to return to the theater for reexcision [5–7].
The experience of this technique in the practice of a single surgeon (I.B.) has been previously described [4]. More recently this method has achieved broader utilization, with a number of authors reporting the use of IOUS to guide excision of benign and malignant lesions [5–7, 14–16]. There are a variety of approaches to this technique. This article describes the methodology utilized by the primary author (I.B.) for performing US-guided excision of a nonpalpable breast lesion, highlighting the features that make it a successful and preferred technique.
Methods
The most important criterion for selection of patients is that they have a breast lesion that is readily visible on US imaging preoperatively. Ideally, this can be checked in the surgeon’s office during the preoperative consultation, utilizing the same or similar equipment as will be used in theater. The surgeon undertaking the procedure must be appropriately trained in breast US, having fulfilled local accreditation requirements.
The US equipment required in the operating room can be either a portable device or a larger upright unit, but the essential requirements are a high-frequency small parts probe preferably in the range 10–15 MHz. As US probes should not be autoclaved, for the purposes of sterility the use of a sterile sleeve placed over the probe is the most practical approach.
The breast is prepared and draped, and the US probe is placed in the sterile plastic sleeve containing US gel. Although sterile US gel can be utilized as the conductor between the sleeved probe and the skin, we have found povidine-iodine solution to be a useful conductive agent when placed on the outside of the sleeve. It enables the operative field to remain free of gel while allowing good US transmission. The US probe is placed on the breast; and once the lesion is identified a marking pen is used to mark the skin in two axis planes: at right angles to each other, directly overlying the lesion (Fig. 1). A skin incision is made over the lesion, and the subcutaneous fat is divided.

Lesion is identified and marked in two planes (a, b)
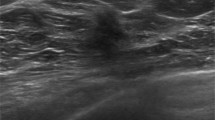
The US probe is then placed into the wound to confirm the position of the lesion. Then, under US guidance and in a fashion similar to performing a needle biopsy, straight mosquito forceps or toothed Kocher forceps are directed toward the lesion in the breast under the long axis of the probe (Fig. 2). The tip of the forceps is advanced, under US guidance, until it immediately abuts the lesion, usually over its anterior aspect (Fig. 3). The jaws of the forceps are then opened to grasp the tissue immediately adjacent to the lesion, localizing its position. The area of tissue thus localized by the Kocher forceps is then grasped with Moynihan forceps to facilitate retraction (Fig. 4). The breast tissue around the Moynihan/Kocher forceps is excised using a combination of diathermy and sharp dissection, removing the lesion with an adequate margin. US may be used to check the adequacy of the excision during its execution (Fig. 5).

Straight, toothed Kocher forceps

Under ultrasonography (US) guidance, straight forceps are advanced to grasp tissue immediately adjacent to the lesion

Moynihan forceps grasp the tissue identified with US guidance, and mosquito forceps are used to guide the excision and facilitate retraction of the specimen

Obtaining US confirmation of the presence of the lesion in the tissues being excised
On completion of the excision, the specimen is marked with orientation sutures. US is then performed on the specimen to confirm that the lesion is contained within the excised tissues (Fig. 6). If the margins are questionable, additional tissue can be excised to reduce the odds of the patient requiring a subsequent surgical intervention. The US probe may be placed back in the breast cavity to ensure that there is no persisting lesion. After confirming that the lesion has been completely excised, the wound is closed in the usual fashion with absorbable sutures.

US examination of the specimen is performed to confirm excision of the lesion and to check the adequacy of the margins
Discussion
The utilization of IOUS to localize nonpalpable breast lesions has significant benefits over other methods, not the least of which is the fact that the patient does not have to endure an additional procedure preoperatively, thus minimizing patient morbidity. It is well documented that preoperative hookwire localization, which is the commonest alternative method, can be associated with significant complications, such as wire displacement, wire amputation, pain, hematoma, and pneumothorax. The presence of the wire also places the surgeon at risk of needle stick injury. The US technique avoids the need to inject carbon, radiotracer, or dye into the lesion, which may spread through tissues and lead to confusion regarding the extent of resection required [12, 17, 18]. Additionally, the presence of the lesion in the excised specimen can be checked in the operating room, obviating the need for sending the specimen to the radiology department, which takes more time.
Various methods have been described for US-guided excision of nonpalpable breast lesions, but compared to others the technique outlined here is simple and has been proven to be effective [4]. Some authors have described placing a hookwire needle into the lesion intraoperatively prior to commencing surgery. This method adds cost to the operation, can be associated with wire amputation and needle-stick injury, and the needle may become dislodged during the procedure [17, 19]. With the technique we described, additional expensive equipment, such as electrosurgical loop devices utilized in other reports, are not required [20]. Furthermore, a radiographer or radiologist need not be present as a proficient and accredited surgeon is working with US [5, 17].
Another application described in other reports involves utilizing IOUS to guide the excision of sonographically occult lesions, such as ductal carcinoma in situ, that have been marked preoperatively with a US-visible marker during stereotactic biopsy [6, 21]. The technique described above could also be adapted to such a setting.
Most surgeons initially acquire familiarization with US techniques in the office or outpatient setting under the supervision of a US-experienced surgeon or a radiologist and in conjunction with participation in training workshops. Office-based US techniques are readily translated to use in the operating theater. Once the sugeon has acquired the necessary skills, this technique can be performed independently of the radiology department with portable US equipment being based in the operating theater. This represents a substantial time and cost saving for the hospital.
Accreditation and regular re-credentialing are vital to maintaining satisfactory standards in the application of US to the breast whether it is in the office or the operating theater. The Royal Australian College of Surgeons together with the Australian Society for Ultrasound in Medicine (ASUM) have recently developed guidelines for accreditation of breast surgeons who wish to utilize US in their practices [22]. Structured workshops with a set syllabus are considered an important aspect of the training. The ASUM guidelines require candidates to have attended 6 h of accredited theory and practical workshops and to have performed 100 ultrasound examinations and 20 supervised needle biopsies. Maintaining a logbook is therefore essential for documenting skill acquisition. Similarly, The American College of Surgeons (ACS) has developed a US educational program for surgeons and surgical residents [23]. The intent of that program is to provide surgeons and surgical residents with a basic understanding of clinical US and knowledge of advanced clinical applications tailored to suit surgeons’ specific clinical practice. The ACS program was developed in cooperation with the Committee on Emerging Surgical Technologies and Education and the National Ultrasound Faculty (NUF) [24]. The NUF has approved a series of US courses to be offered at the annual ACS Clinical Congress and to be made available for export to other venues. These organizations emphasize the need for ongoing education and accreditation.
Conclusions
Intraoperative US has clear advantages in breast surgery. The technique described in this report is simple, safe, accurate, and minimizes additional costs. Its use is advocated in the management US-visible lesions that require surgical excision. It is important that breast surgeons have an appropriate level of competence in US techniques as determined by local accreditation and proficiency standards. Ultimately, the evolving utilization of US by breast surgeons in clinical practice will lead to enhanced provision of care for women with breast disease.
References
Rubio IT, Henry-Tillman R, Klimberg VS (2003) Surgical use of breast ultrasound. Surg Clin N Am 83:771–788
Thompson M, Klimberg VS (2007) Use of ultrasound in breast surgery. Surg Clin N Am 87:469–484
Fine RE, Staren ED (2004) Updates in breast ultrasound. Surg Clin N Am 84:1001–1034
Bennett IC, Greenslade J, Chiam H (2005) Intraoperative ultrasound-guided excision of nonpalpable breast lesions. World J Surg 29:369–374
Rahusen FD, Bremers AJA, Fabry HF et al (2002) Ultrasound-guided lumpectomy of nonpalpable breast cancer versus wire-guided resection: a randomized clinical trial. Ann Surg Oncol 9:994–998
James TA, Harlow S, Sheehey-Jones J et al (2009) Intraoperative ultrasound versus mammographic needle localization for ductal carcinoma in situ. Ann Surg Oncol 16:1164–1169
Ngo C, Pollett AG, Laperrelle J et al (2007) Intraoperative ultrasound localization of nonpalpable breast cancers. Ann Surg Oncol 14:2485–2489
Law MT, Bennett IC (2010) Structured ultrasonography workshop for breast surgeons: is it an effective training tool? World J Surg 34:549–554
Chadwick DR, Shorthouse AJ (1997) Wire directed localization biopsy of the breast: an audit of results and analysis of factors influencing therapeutic value in the treatment of breast cancer. Eur J Surg Oncol 23:128–133
Kelly P, Winslow EH (1996) Needle wire localization for non-palpable breast lesions: sensations, anxiety levels, and informational needs. Oncol Nurs Forum 23:639–645
Homer MJ, Smith TJ, Safaii H (1992) Prebiopsy needle localization: methods, problems, and expected results. Radiol Clin North Am 30:139–153
Canavese G, Catturich A, Vecchio C et al (1995) Preoperative localization of nonpalpable lesions in breast cancer by charcoal suspension. Eur J Surg Oncol 21:47–49
Paganelli G, Veronesi V (2002) Innovation in early breast cancer surgery: radio-guided occult lesion localization and sentinel node biopsy. Nucl Med Commun 23:625–627
Smith LF, Rubio IT, Henry-Tillman R et al (2000) Intraoperative ultrasound-guided breast biopsy. Am J Surg 180:419–423
Fortunato L, Penteriani R, Farina M et al (2008) Intraoperative ultrasound is an effective and preferable technique to localize non-palpable breast tumors. EJSO 24:1289–1292
La Pinta M, Ascarelli A, Testa V et al (2009) Intraoperative ultrasound in excision of breast nonpalpable lesions: The experience of the breast unit of San Giovanni Hospital in Rome. Breast J 15:546–548
Kaufman CS, Jacobson L, Bachman B et al (2002) Intraoperative ultrasound facilitates surgery for early breast cancer. Ann Surg Oncol 9:988–993
Kim J, Chung D, Spillane A (2004) Combined radioguided occult lesion and sentinel node localization for breast cancer. ANZ J Surg 74:550–553
Buman SJ, Da Clark (2005) Breast intraoperative ultrasound: prospective study in 112 patients with impalpable lesions. ANZ J Surg 75:124–127
Fine RE, Swalke MA, James VP et al (2009) A novel ultrasound-guided electrosurgical loop device for intra-operative excision of breast lesions; an improvement in surgical technique. Am J Surg 198:283–286
Gittleman MA (2003) Single-step ultrasound localization of breast lesions and lumpectomy procedure. Am J Surg 186:386–390
Anonymous (2010) Australian Society for Ultrasound in Medicine website: http://www.asum.au/site/index.php Qualifications; CCPU Certificate in Clinician Performed Ultrasound
Conflicts of interest
There are no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bennett, I., Biggar, M. Intraoperative Ultrasonography-Guided Excision of Nonpalpable Breast Lesions. World J Surg 35, 1835–1839 (2011). https://doi.org/10.1007/s00268-011-1082-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-011-1082-y