
Abstract
Despite exhibiting functional impairments in a number of key domains, children with attention-deficit hyperactivity disorder (ADHD) tend to overestimate their own competence more than their peers without ADHD. In this review, we describe the evidence in support of a self-enhancement bias (SEB) in children with ADHD and factors that are associated with the presence of this bias. We discuss possible explanations for a SEB and the extent to which these inaccurate self-appraisals are adaptive or impairing. We conclude with implications for practice and further research. There is considerable evidence that the SEB exists in a substantial proportion of children with ADHD in several domains and likely persists into adolescence and adulthood. In treatment, clinicians may need to determine if any observed SEB is adaptive or maladaptive for the individual and act accordingly.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder that initially manifests in childhood and is characterized by symptoms of inattention, hyperactivity, and impulsivity [1]. Compared to their typically developing peers, children and adolescents with ADHD obtain lower scores on standardized achievement tests, have lower grade point averages, and are less likely to complete secondary school and pursue postsecondary education [2, 3]. Children with ADHD are also more apt than other children to be rejected by peers and adolescents and associate with deviant peers [4]. Adolescents with ADHD also experience more conflict with their parents [5]. Given their challenges with executive functioning, academic achievement, and social interaction, it is not surprising that adults with ADHD also have challenges with obtaining stable employment [3].
The focus of the current review is self-knowledge in individuals with ADHD. Self-knowledge is described as “…people’s awareness of their patterns of thinking, feeling, and behaving as well as awareness of their reputation” [6, p174]. Understanding of self is important in clinical populations because inadequate or inaccurate knowledge of self may interfere with life satisfaction [7] as well as treatment seeking or adherence to treatment [8]. Self-evaluation requires an individual to appraise their skills, abilities, or traits and relies in part on self-perceptions, which reflect “the ability to detect and acquire accurate information using various cues about one’s person or behavior” [6. p174]. Considerable research indicates that children with ADHD exhibit overly positive views of their abilities when rating their competencies in various domains (see [9] for a review). Early work by Hoza and colleagues examining self-perceptions in children with ADHD described this overestimation as a “positive illusory bias” (PIB) [10]. In this article, however, we use the term “self-enhancement bias” (SEB) as perceptions in individuals may be imprecise [11] rather than reflect illusory or completely unrealistic estimations of competence. In this review, we describe the evidence in support of a SEB in children with ADHD and factors that are associated with the presence of this bias. We discuss possible explanations for a SEB and the extent to which these inaccurate self-appraisals are adaptive (e.g., they may protect against mood disorders) or impairing (e.g., associated with aggression). We conclude with implications for practice and further research.
Evidence for a Self-Enhancement Bias in Individuals with ADHD
Despite exhibiting functional impairments in a number of key domains, children with ADHD tend to report overly positive views of their own competence relative to other reports of their competence (e.g., by a parent) or an objective assessment [9]. Furthermore, the magnitude of the bias between an external indicator of performance and self-reported competence is significantly greater in children with ADHD than in typically developing children [10]. This bias also appears to be maladaptive in that it is not associated with some of the more positive motivational elements that often characterize children who perceive themselves as somewhat better than they are [12]. Such findings are consistent with the general observation by Baumeister [13] that there is “an optimal margin of illusion” (p176); that is, markedly inaccurate perceptions give rise to negative outcomes such as persisting at tasks when there is little chance of success given one’s level of ability or experiencing negative thoughts that may be associated with depressed mood.
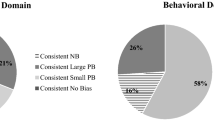
Since Hoza’s initial studies on the PIB in the first years of the twenty-first century, there have been approximately 18 studies that have demonstrated that children, adolescents, or adults with ADHD have a SEB (see [9, 14] for systematic reviews of this literature). A key question addressed in recent investigations is whether a SEB is a characteristic of ADHD or confined to a specific subgroup of children with ADHD. Recent studies indicate that approximately 30 % of children with ADHD present with a SEB [15•, 16]. While the characteristics of this specific subgroup of children exhibiting a SEB are still unclear, there are some internal and external characteristics than appear to influence the extent to which children with ADHD overestimate their abilities.
Characteristics Associated with a Self-Enhancement Bias in Individuals with ADHD
Age
The study of self-enhancement in individuals with ADHD has primarily focused on children [9]. Cross-sectional studies with adults with ADHD suggest that a SEB is also evident in adults with ADHD in domains such as parenting and driving behavior [14, 17]. For example, parents who reported high levels of hyperactive/impulsive symptoms also reported engaging in significantly more positive parenting behaviors than were actually observed in families with and without children diagnosed with ADHD [18•]. A recent longitudinal study, however, demonstrated that the magnitude of the SEB declines as children with ADHD progress into adolescence/young adulthood [19]. Further longitudinal work is needed to better understand the developmental trajectory of the SEB in individuals with ADHD and its association with symptom severity, treatment adherence, and well-being.
Gender
Few studies of the SEB in children with ADHD have focused on females [9]. However, recent studies have documented a SEB in females with ADHD in domains such as scholastic competence, social acceptance, and behavioral conduct [12, 20]. Given that gender differences in bias are evident in typically developing children and youth [21], this is an important area for future exploration. A focus on gender differences seems particularly important when examining social domains of competence (e.g., peer acceptance) as different findings are obtained depending on whether same- or opposite-gender peers are used to provide information for purposes of comparison [21, 22].
ADHD Symptom Dimensions
It is possible that overly positive beliefs of competence are most related to a particular ADHD symptom dimension. Although a recent study showed that ADHD subtype was not related to the magnitude of the SEB among girls with ADHD [20], evidence suggests that the ADHD symptom dimension is important to consider. Recent findings indicate that hyperactive/impulsive symptoms are more strongly related to a SEB than inattentive symptoms in both children [23] and adults [18•]. One limitation of the former study, however, is that comorbid aggression or oppositional behavior was not controlled in the analyses [24••].
Comorbidity
Studies examining the influence of comorbid disorders on the self-enhancement bias in children with ADHD have focused largely on co-occurring depressive and aggressive symptoms. Findings indicate that children with ADHD who display more depressive symptoms are less likely to overestimate their competence than children with ADHD without depressive symptoms [12]. On the other hand, aggressive or externalizing symptoms are related to greater overestimation of competence in children with ADHD [25]. Despite this association, the unique relation between ADHD and self-enhancement is present even when controlling for comorbid oppositional behavior (see review by Jiang & Johnston [24••]).
Domains of Functioning
One important question is whether there are aspects or areas that are prone to overestimation in individuals with ADHD. In general, an overly positive perception of ability in children with ADHD has been demonstrated a number of domains including academic [11], social [26], and behavioral conduct and symptoms of ADHD [27•, 28•]. A SEB is also evident in perceptions of executive functions in adolescents with ADHD [29], perceptions of parenting competence in parents who have ADHD [14, 18•], and driving behaviors in adults with ADHD [17]. The SEB in ADHD appears to be most evident in the domain of functioning that is most impairing [9]. For example, children with ADHD and comorbid conduct problems overestimate their competence particularly in the behavioral conduct domain [30, 31]. Estimations also vary depending on the specificity of the behavior or trait under consideration. Young adults with ADHD appear to be more accurate when judging a task or ability that is narrow and specific and less accurate when ratings are more global and require them to draw upon working memory or to integrate information [32].
Source of Information to Assess “Actual” Ability
Researchers often use informants (e.g., parents, teachers) to provide data on the actual competence of the children or youth with ADHD [9]. Sometimes, however, objective performance-based assessments are also used (e.g., social interaction task [15•]). One challenge with using informants to provide information on actual competence is that children’s appraisals of their ability are in part the result of their perceptions of how others view their ability [33]. Family is one of the principal influences on the construction of an individual’s self-concept and self-appraisals [34]. Children who perceive negative appraisals of their abilities by parents may provide overrate their ability as a means of self-protection. Emeh and Mikami [27•], for example, reported that high levels of negative parenting behaviors, such as criticism and pathological control, were associated with higher levels of self-enhancement in children with ADHD, whereas parental reports of warmth were associated with less inflated self-perceptions. This influence of context has been demonstrated in studies using observations of parent-child interactions in a laboratory [27•] and through children’s perceptions of parenting styles via self-report [35]. This family influence leads to the possibility that an enduring pattern of negative appraisals by parents may have long-term effects on the maintenance of a SEB in populations of children with ADHD.
Explanations for and Implications of Self-Enhancement in Individuals with ADHD
The underlying reasons for the SEB in children with ADHD are not clear. Four theoretical explanations have been put forth: (a) self-protective hypothesis, (b) ignorance of incompetence, (c) neuropsychological deficits, and (d) the cognitive immaturity hypothesis [9]. To date, there is considerable support for the self-protection hypothesis [27•, 36, 37]. For example, one study conducted in a laboratory setting found that children with ADHD who engaged in a cooperative task along with a confederate child adjusted their self-appraisals to become more realistic when told that the peer liked them [36]. In addition, Emeh and Mikami [27•] found that children with ADHD whose parents criticized them were also those who reported a higher SEB. Evidence indicating that a SEB occurs in the domain of greatest impairment is also consistent with a self-protection hypothesis as one is most likely to want to protect one’s self-concept in the area where one shows the greatest challenges [9].
There are also studies that support the neuropsychological deficit and cognitive-immaturity hypothesis for the SEB. First, there is some evidence that children and youth with ADHD who demonstrate more severe executive function impairments also show more self-enhancement in self-reports of ability [11, 26]. Moreover, although support for the cognitive-immaturity hypothesis is less robust than for the self-protection hypothesis [9], findings indicate that the SEB is lower [19] in adolescents than has been reported in studies with children. These results are consistent with the cognitive immaturity hypothesis and possibly associated with development of executive functions in adolescence.
In general, it is likely that more than one of the current theoretical perspectives on self-enhancement of competence in individuals with ADHD will explain the phenomenon better than any single existing theory. It is also likely that there are interactions among these theoretical perspectives. Research is needed that integrates potential contributors to the SEB in a developmentally sensitive design.
Discrimination Versus Bias
Much of the research examining self-perceptions in individuals with ADHD has focused on bias, the extent to which an individual’s report of their competence is overestimated or underestimated relative to an external indicator [9]. The second aspect of self-knowledge is discrimination, which “indexes the correlation between predicted behavior and actual behavior” [38, p642]. It is possible for an individual to be a better predictor of his or her own behavior (e.g., level of actual achievement; discrimination) than another informant but still report overly positive views of achievement relative to another informant (bias) who may, in turn, also have a biased view of the individual’s behavior [39, 40]. Although relatively few studies have examined discrimination in children with ADHD, it is important to consider as it has implications for understanding the usefulness of self-report in predicting actual behavior or later outcomes [11]. This argument is consistent with that of Swanson et al. [20] who noted the need for researchers to examine both components of the scores giving rise to bias estimations (e.g., child and teacher ratings) when trying to identify predictors of later outcomes.
Short- and Long-Term Consequences
It is important to study self-knowledge in individuals with ADHD to understand whether overly positive (or negative) self-perceptions have undesirable short- and long-term consequences. Studies assessing the long-term outcomes of overestimations of competence have reported discrepant results. On one hand, Mikami and Hinshaw [41] reported that positive self-perceived scholastic competence in childhood was associated with resilient adolescent functioning. On the other hand, a reduction in self-perceived social acceptance over time was associated with increased depression symptoms in children with ADHD [42]. Despite these seemingly positive outcomes, McQuade and colleagues [43•] also reported that higher self-perceived social acceptance was a risk factor for increased aggression and conduct problems for children with ADHD. In addition, studies indicate that overly positive estimations of ability are associated with long-term negative outcomes such as behavioral problems [19], less prosocial behavior [15•], and risky driving behaviors (higher frequency of driving illegally, of traffic violations for risky driving, and of having ones’ license or permit revoked or suspended) in young adulthood [44•] in individuals with ADHD.
Implications for Practice
There are several tentative implications of the research on SEB in individuals with ADHD for assessment and intervention. Although the research on the SEB has mainly been confined to children and there is some indication that self-enhancement is reduced in adolescence and adulthood, there is also evidence that it persists in terms of self-appraisals of parenting [14, 18•], driving behavior [17], executive function [29], and ADHD and oppositional symptom ratings when standardized rating scales are used [45]. Parents and teachers are typically consulted when clinicians are doing assessments of children with ADHD. As children move into adolescence, however, they typically have several teachers who are less familiar with them than teachers of children in elementary school [46]. Parents may spend less time with their teens and be less aware of their behaviors than parents of younger children. Consequently, clinicians may have to rely on self-reports, which makes the diagnostic process challenging. As suggested by Prevatt and colleagues [32], concrete descriptions of behaviors possibly using picture stimuli to depict symptoms of ADHD and frequently co-occurring behaviors may be helpful [28•, 47].
Children with ADHD typically engage in treatment due to the initiative of their parents. Because of their parents’ monitoring, they are typically compliant with regard to taking medication. Furthermore, evidence-based psychosocial interventions for children with ADHD typically have parent or teacher mediators [48, 49]. Adolescents, on the other hand, who have an overly positive view of their abilities may not see the need for treatment and, as a result, may not adhere to pharmacological or psychosocial interventions [50]. The onus then falls on parents and teachers to sensitively help them acquire insight into strengths and needs. For those adolescents who are willing to engage in treatment, interventions that focus on awareness and acceptance, such as mindfulness interventions, may be helpful as an adjunct to other treatments [51, 52].
The findings showing that childhood aggression, as well as parental criticism and power assertive parenting, is related to a SEB has implications for parenting interventions. As with adolescents, in addition to teaching positive parenting strategies, it might be fruitful to explore whether mindfulness interventions are beneficial. Such interventions may help parents, including those parents who themselves have ADHD become more aware of their own parenting behaviors and accept the behaviors of their children [51, 52]. This might facilitate the use of authoritative parenting practices.
Conclusion
In spite of the methodological issues identified by Jiang and Johnston [24••] and Owens et al. [9] in their reviews of the research, the evidence is strong that the SEB exists in a substantial proportion of children with ADHD in several domains and likely persists into adolescence and adulthood. Notwithstanding the implications for practice outlined above, to a large extent, the importance of this bias in individuals with ADHD rests on whether it is maladaptive or adaptive. With regard to the decision to consider the SEB in treatment, clinicians may need to determine whether it is adaptive or maladaptive for the individual and proceed accordingly.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington: Author; 2013.
Frazier TW, Youngstrom EA, Glutting JJ, Watkins MW. ADHD and achievement: meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. J Learn Disabil. 2007;40:49–65.
Kuriyan AB, Pelham Jr WE, Molina BSG, Waschbusch DA, Gnagy EM, Sibley MH, et al. Young adult educational and vocational outcomes of children diagnosed with ADHD. J Abnorm Child Psych. 2013;41:27–41.
Becker SP, Luebbe AM, Langberg JM. Co-occurring mental health problems and peer functioning among youth with attention-deficit/hyperactivity disorder: a review and recommendations for future research. Clin Child Fam Psych. 2012;15:279–302.
Markel C, Wiener J. Attribution processes in parent-adolescent conflict in families with adolescents with and without ADHD. Can J Beh Sci. 2014. doi:https://doi.org/10.1037/a0029854.
Carlson E. Overcoming the barriers to self-knowledge: mindfulness as a path to seeing yourself as you really are. Perspect Psychol Sci. 2013;8:173–86.
Proctor C, Tsukayama E, Wood AM, Maltby J, Eades JF, Linley PA. Strengths gym: the impact of a character strengths-based intervention on the life satisfaction and well-being of adolescents. J Posit Psychol. 2011;6:377–88.
Chacko A, Newcorn JH, Feirsen N, Uderman JZ. Improving medication adherence in chronic pediatric health conditions: a focus on ADHD in youth. Curr Pharm Design. 2010;16:2416–23.
Owens JS, Goldfine ME, Evangelista NM, Hoza B, Kaiser NM. A critical review of self-perceptions and the positive illusory bias in children with ADHD. Clin Child Fam Psychol Rev. 2007;10(4):335–51.
Hoza B, Pelham Jr WE, Dobbs J, Owens JS, Pillow DR. Do boys with attention deficit/hyperactivity disorder have positive illusory self-concepts? J Abnorm Psychol. 2002;111:268–78.
Chan T, Martinussen R. Positive illusions? The accuracy of academic self-appraisals in adolescents with ADHD. J Pediatr Psychol. (accepted).
Ohan JL, Johnston C. Positive illusions of social competence in girls with and without ADHD. J Abnorm Child Psychol. 2011;39(4):527–39.
Baumeister RF. The optimal margin of illusion. J Soc Clin Psychol. 1989;8:176–89.
Jiang Y, Johnston C. The relationship between ADHD symptoms and competence as reported by both self and others. J Atten Disord. 2012;16:418–26.
Linnea K, Hoza B, Tomb M, Kaiser N. Does a positive bias relate to social behavior in children with ADHD? Behav Ther. 2012;43:862–75. Positive bias in the social domain is not adaptive as children with ADHD whose self-reports of their social skills were overly positive displayed significantly less prosocial behavior in a laboratory-based dyadic social interaction task than did ADHD and non ADHD children without such a bias.
Rizzo P, Steinhausen H-C, Drechsler R. Self-perceptions of self-regulatory skills in children aged 8 to 10 years: development and evaluation of a new self-rating scale. Aust Educ Dev Psychol. 2010;10:123–43.
Knouse LE, Bagwell CL, Barkley BA, Murphy KR. Accuracy of self-evaluation in adults with ADHD: evidence from a driving study. J Atten Disord. 2005;8:221–34.
Lui JH, Johnston C, Lee CM, Lee-Flynn SC. Parental ADHD symptoms and self-reports of positive parenting. J Consult Clin Psychol. 2013;81:988–98. Parents with higher levels of hyperactive/impulsive symptoms self-reported engaging in significantly more positive parenting behaviors than were actually observed in a laboratory task where parents interacted with their child. Findings are consistent with self-enhancement bias.
Hoza B, Murray-Close D, Arnold LE, Hinshaw SP, Hechtman L, the MTA Cooperative Group. Time-dependent changes in positively biased self-perceptions of children with attention-deficit/hyperactivity disorder: a developmental psychopathology perspective. Dev Psychopathol. 2010;22:375–90.
Swanson EN, Owens EB, Hinshaw SP. Is the positive illusory bias illusory? Examining discrepant self-perceptions of competence in girls with ADHD. J Abnorm Child Psychol. 2012;40:987–98.
Smith SD, Van Gessel CA, David-Ferdon C, Kistner JA. Sex differences in children’s discrepant perceptions of peer acceptance. J Appl Dev Psychol. 2013;34:101–7.
Putarek V, Keresteš G. Self-perceived popularity in early adolescence. Accuracy, associations with loneliness, and gender differences. J Soc Pers Relat. 2015. doi:https://doi.org/10.1177/0265407515574465.
Owens JS, Hoza B. The role of inattention and hyperactivity/impulsivity in the positive illusory bias. J Consult Clin Psychol. 2003;71:680–91.
Jiang Y, Johnston C. Co-occurring aggressive and depressive symptoms as related to overestimations of competence in children with attention- deficit/hyperactivity disorder. Clin Child Fam Psychol Rev. 2014;17:157–72. This paper reviews studies of overestimations of competence among children with ADHD and examines the extent to which comorbid aggressive or depressive symptoms may be influencing these estimates.
Kaiser NM, Hoza B, Pelham WE, Gnagy E, Greiner AR. ADHD status and degree of positive illusions moderational and mediational relations with actual behavior. J Atten Disord. 2008;12:227–38.
McQuade JD, Tomb M, Hoza B, Waschbusch DA, Hurt EA, Vaughn AJ. Cognitive deficits and positively biased self-perceptions in children with ADHD. J Abnorm Child Psychol. 2011;39:307–19.
Emeh CC, Mikami AY. The influence of parent behaviors on positive illusory bias in children with ADHD. J Atten Disord. 2014;18:456–65. These authors found a relationship between parent criticism and an SEB in the social domain in children with ADHD which suggests that greater levels of criticism by parents may lead to ego protection, while warmth may lower the need for children with ADHD to engage in self-protection and provide more accurate self-ratings of their social competence.
Wiener J, Malone M, Varma A, Markel C, Biondic D, Tannock R, et al. Children’s perceptions of their ADHD symptoms: positive illusions, attributions, and stigma. Can J Sch Psychol. 2012;27(3):217–42. Children with ADHD have a SEB for their ADHD symptoms as they reporting demonstrating fewer symptoms relative to parent ratings.
Steward KA, Tan A, Delgaty L, Gonzales MM, Bunner M. Self-awareness of executive functioning deficits in adolescents with ADHD. J Atten Disord. 2014.
Haas SM, Waschbusch DA, King S, Walsh TM. Examining the role of callous-unemotional traits in the attributional styles and self-competence evaluations of children with conduct problems and ADHD. J Psychopathol Behav Assess. 2015;37:196–206.
Hoza B, Gerdes AC, Hinshaw SP, Arnold LE, Pelham WE, Molina BSG, et al. Self-perceptions of competence in children with ADHD and comparison children. J Consult Clin Psychol. 2004;72:382–91.
Prevatt F, Proctor B, Best L, Baker L, Walker JV, Taylor NW. The positive illusory bias: does it explain self-evaluations in college students with ADHD? J Atten Disord. 2012;16:235–43.
Freiberger V, Steinmayr R, Spinath B. Students’ competence beliefs and their perceived teachers’ ability evaluations—how do both contribute to students’ intrinsic motivation and achievement in math? Learn Individ Differ. 2012;22:518–22.
Harter S. The construction of the self. New York: Wiley; 1999.
Molina MF. Perceived parenting style and self-perception in children with attention deficit/hyperactivity disorder. Int J Psychol Res. 2015;8:61–74.
Diener MB, Milich R. Effects of positive feedback on the social interactions of boys with attention deficit hyperactivity disorder: a test of the self-protective hypothesis. J Clin Child Psychol. 1997;26:256–65.
Ohan JL, Johnston C. Are the performance overestimates given by boys with ADHD self-protective? J Clin Child Adolesc Psychol. 2002;31:230–41.
Epley N, Dunning D. The mixed blessings of self-knowledge in behavioral prediction: enhanced discrimination but exacerbated bias. Pers Soc Psychol B. 2006;32:641–55.
Abikoff H, Courtney M, Pelham Jr WE, Koplewicz HS. Teachers’ ratings of disruptive behaviors: the influence of halo effects. J Abnorm Child Psychol. 1993;21:519–33.
Ready DD, Wright DL. Accuracy and inaccuracy in teachers’ perceptions of young children’s cognitive abilities: the role of child background and classroom context. Am Educ Res J. 2011;48:335–60.
Mikami AY, Hinshaw SP. Resilient adolescent adjustment among girls: buffers of childhood peer rejection and attention-deficit/hyperactivity disorder. J Abnorm Child Psych. 2006;34:823–37.
McQuade JD, Hoza B, Waschbusch DA, Murray-Close D, Owens JS. Changes in self-perceptions in children with ADHD: a longitudinal study of depressive symptoms and attributional style. Behav Ther. 2011;42:170–82.
Hoza B, McQuade JD, Murray-Close D, Shoulberg E, Molina BSG, Arnold LE, et al. Does childhood positive self-perceptual bias mediate adolescent risky behavior in youth from the MTA study. J Consult Clin Psychol. 2013;81:846–858. In this study, an overly positive bias regarding behavioral conduct mediated the relationship between having childhood ADHD and risky driving behavior during adolescence or young adulthood. These findings suggest that early evidence of a SEB in children with ADHD may be an indicator for engagement in risky behaviors in adolescence or young adulthood.
McQuade JD, Vaughn AJ, Hoza B, Murray-Close D, Molina BSG, Arnold LE, et al. Perceived social acceptance and peer status differentially predict adjustment in youth with and without ADHD. J Atten Disord. 2014;18:31–43. In ADHD children, higher perceived social acceptance was protective against increases in depression symptoms for those with lower peer preference scores. In contrast, higher perceive social acceptance predicted greater aggression/conduct problems for those with higher peer preference.
Varma A. Self-perceptions of adolescents with ADHD for their problem behaviors (Doctoral dissertation). 2014.
Evans SW, Allen J, Moore S, Strauss V. Measuring symptoms and functioning of youth with ADHD in middle schools. J Abnorm Child Psychol. 2005;33:695–706.
Valla JP, Bergeron L, Smolla N. The Dominic-R: a pictorial interview for 6- to 11-year old children. J Am Acad Child Adolesc Psychiatry. 2000;39:85–93.
Chronis AM, Jones HA, Raggi VL. Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Clin Psychol Rev. 2006;26:486–502.
Kaiser NM, Pfiffner LJ. Evidence-based psychosocial treatments for childhood ADHD. Psychiatr Ann. 2011;41(1):9–15.
Charach A, Yeung E, Volpe T, Goodale T, dos Reis S. Exploring stimulant treatment in ADHD: narratives of young adolescents and their parents. BMC Psychiatry. 2014;14:110.
Cassone AR. Mindfulness training as an adjunct to evidence-based treatment for ADHD within families. J Atten Disord. 2015;19(2):147–57.
Haydicky J, Shecter C, Wiener J, Ducharme JM. Evaluation of MBCT for adolescents with ADHD and their parents: impact on individual and family functioning. J Child Fam Stud. 2015;24:76–94.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Carla Colomer, Rhonda Martinussen, and Judith Wiener declare that they have no conflict of interest
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on ADHD
Rights and permissions
About this article

Cite this article
Colomer, C., Martinussen, R. & Wiener, J. The Self-Enhancement Bias in Attention Deficit/Hyperactivity Disorder: Origin, Nature, and Consequences. Curr Dev Disord Rep 3, 1–6 (2016). https://doi.org/10.1007/s40474-016-0073-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40474-016-0073-y