
Abstract
Introduction
Normal (120-140 mm Hg) systolic peridialysis blood pressure (BP) is associated with higher mortality in hemodialysis (HD) patients.
Aim
We explored the relationship between hypertension and BP on outcomes using data collected at the interdialytic period.
Methods
This was a single-center observational cohort study with 2672 HD patients. BP was determined at inception, in mid-week, between 2 consecutive dialysis sessions. Hypertension was defined as systolic BP ≥ 140 mm Hg and/or diastolic BP ≥ 90 mm Hg. Endpoints were major CV events and all-cause mortality.
Results
During a median follow-up of 31 months, 761 patients (28%) experienced CV events and 1181 (44%) died. Hypertensive patients had lower survival free of CV than normotensive patients (P = 0.031). No difference occurred in the incidence of death between groups. Compared with the reference category of SBP ≥ 171 mmHg, the incidence of cardiovascular events was reduced in patients with SBP 101-110 (HR 0.647, 95% CI 0.455 to 0.920), 111-120 (HR 0.663, 95%CI 0.492 to 0.894), 121-130 (HR 0.747, 95%CI 0.569 to 0.981), and 131-140 (HR 0.757, 95%CI 0.596 to 0.962). On multivariate analysis, systolic and diastolic BP were not independent predictors of CV events or death. Normal interdialytic BP was not associated with mortality or CV events, and hypertension predicted an increased probability of CV complications.
Conclusions
Interdialytic BP may be preferred to guide treatment decisions, and HD patients should be treated according to guidelines for the general population until specific BP targets for this population are identified.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Hypertension is fairly common in patients on hemodialysis (HD) and often poorly controlled. Although the estimates of the prevalence may vary, most studies indicate that more than 70% of patients on dialysis have hypertension [1, 2]. Hypertension is closely related to cardiovascular events and death in the general population [3], and it is intuitive that the same will be true in patients on dialysis. However, that may not necessarily be the case and the association of blood pressure (BP) and adverse outcomes in that population remains controversial. Indeed, many studies reported no association or a U- or J- shaped relationship between blood pressure and events indicating a higher mortality at low BP, including patients with systolic BP considered normal, that is, between 120 to 140 mm Hg [4,5,6]. It has also been shown that hypertensive HD patients have a better 2 year survival than normotensives patients have [5]. Therefore, physicians in charge of hemodialysis patients may be concerned about the potential harm of BP reduction. More recently, the variable association between BP and outcomes has been attributed to the period of time when blood pressure is recorded, either peridialysis or during the interdialytic period [7], the latter, instead of the former, showing consistent increase in the incidence of death with higher pulse pressure or BP [8, 9]. Unfortunately, these and other studies had a relatively short follow-up, precluding more definitive estimation of the impact of BP on prognosis.
In 1997, we started a prospective observational investigation aimed at determining the best strategy for the detection and treatment of cardiovascular (CV) disease in patients on HD (the KiHeart cohort). Since that time, more than 2500 patients have been enrolled who underwent a comprehensive cardiovascular assessment according to a prespecified protocol that included BP determination, performed at inception, between 2 consecutive dialysis sessions. In the present study, using the KiHeart database, we intended to verify the relationship between the diagnoses of hypertension and BP levels on outcomes using data collected at the interdialytic period. Therefore, this study intend to clarify the value of BP, measured at the interdialytic period, as a predictor of outcomes using a large CKD population followed for a long period of time. We want to know if normal interdialytic BP is associated with mortality or with CV events and if hypertension is a predictor of major CV complications.
2 Methods
This was a single-center, retrospective, observational cohort study of adult patients on HD. The study was performed according to the Helsinki Declaration, and the protocol was approved by the institutional ethics committee (NCT01359722).
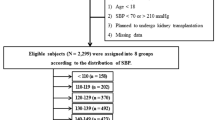
Patients had been treated by hemodialysis and were sent to our center for CV evaluation. Between August 1997 and August 2021, 2794 patients were enrolled in the cohort, 122 (9.6%) were excluded due to incomplete data, participation in another study, or were lost to follow-up, leaving 2672 subjects to be considered for inclusion.
Due to a centralized government-controlled system, hemodialysis followed a standardized routine and was performed 3 times/week, 4 hour sessions, in centers located in the São Paulo Metropolitan area. Patients were maintained on statins, aspirin, rennin-angiotensin system inhibitors, and beta-blockers, according to current guidelines for secondary prevention of CV events, independently of clinical evaluation and were seen at least 2 times per year in our service when medication and adhesion to a healthy life-style were checked and enforced. Patients had free access to medication and dialysis.
Baseline data were collected at inception, at cardiac evaluation, in mid-week, between 2 consecutive dialysis sessions, and entered into a computerized database. BP was recorded using a calibrated aneroid sphygmomanometer, with the patient in a seated position, by one of the authors or by a trained technician. The average of 2 consecutive measurements was used. Hypertension was defined as systolic BP ≥ 140 mm Hg and/or diastolic BP ≥ 90 mm Hg.
Echocardiograms (standard 2D and Doppler) were obtained with the patient in the left lateral recumbent and supine positions by using a 1.5–3.6 MHz 3S probe (Vivid I; GE Medical Systems, Sonigen, Germany) on a day between two consecutive dialysis sessions. LV internal dimensions, interventricular septum, and posterior wall thicknesses were determined. Left ventricular mass was indexed to body surface area. LV ejection fraction was measured in the apical views using the Simpson method. LV systolic dysfunction (LVSD) was defined as LV ejection fraction ≤0.50. The echocardiograms were read by experienced observers unaware that patients were part of a study.
Body mass index, tobacco use, hypertension, dyslipidemia, and diabetes were defined as previously described [10]. Previous or current cardiovascular disease included myocardial infarction, coronary intervention, stroke, heart failure, and peripheral arterial disease. Censored events were verified during clinical visits, by telephone, electronic mail, or review of hospital charts. Patients were followed until death or renal transplantation. Endpoints were the occurrence of major cardiovascular events (myocardial infarction, unstable angina, stroke, sudden death, new-onset heart failure, and acute peripheral arterial syndrome) and death by any cause.
We explored the relationship between BP and outcomes in 3 ways. First, we compared the outcomes according to a BP cutoff of 140 (systolic) and/or 90 (diastolic) mm Hg; second, according to the distribution of BP in 3 percentile groups, 130, 150, and 170 mm Hg (systolic BP) and 80, 90, and 100 mm Hg (diastolic BP). We also examined the relationship between discrete BP levels and outcomes.
2.1 Statistical Analysis
Values are expressed as means, standard deviation of the means, median, and percentages. We used a statistical software package (SPSS Statistics, version 20.0, IBM, Armonk, NY, USA) for analysis of the data. The differences among the groups were assessed with chi-square test (for categorical data), or the Student t test (for continuous data), when appropriate. Survival curves were constructed using the Kaplan-Meier method and compared by using the log-rank test. Cox proportional hazards model was used to verify the variables associated with outcomes. The variables selected for multivariate Cox model were those showing a significant association with outcomes on univariate analysis. A P value of < 0.05 was considered significant.
3 Results
Table 1 shows the demographic and clinical characteristics of the study population at inception. The mean age was 54.8 ± 10.7 years, and the majority of our patients were male, White, with a high prevalence of diabetes and associated CV disease. Their systolic and diastolic BPs were 152 ± 31 and 89 ± 16 mm Hg, respectively, and hypertension was observed in 1937 subjects (72%). Left ventricular hypertrophy was common, and the mean left ventricular systolic function was within the normal range.
Hypertensive and normotensive individuals differed in many aspects. Hypertension was associated with an increased prevalence of diabetes and with a higher left ventricular mass index, whereas smokers, concomitant CV disease, previous myocardial infarction, longer time on dialysis, and reduced left ventricular ejection fraction predominated among normotensive individuals. Of note is the very high prevalence of peripheral arterial disease in the 2 groups.
During a median follow-up of 31 months (range, 1.5–216 months) 761 patients (28%) had at least one fatal-nonfatal major cardiovascular event and 1181 (44%) died, 50% from cardiovascular causes. Figure 1 shows that hypertensive patients had a lower survival free of cardiovascular events (Log-rank = 0.031). There was no difference in the incidence of death between normotensive and hypertensive groups (Log-rank = 0.760, Figure 2). Interestingly, the mortality curves appear to diverge after 5 years of follow-up, but the small number of patients at risk beyond that point probably interfered with the statistical power.

Cardiovascular events according with hypertension

Death by any cause according with hypertension
Table 2 shows the hazard ratio of cardiovascular events and death according to systolic blood pressure percentiles. Patients at the lower percentile showed a 25% reduction in the incidence of cardiovascular events (HR 0.750, 95%CI 0.637–0.883, P = 0.001) compared with the higher percentile. There was also a trend toward a lower incidence of death that did not achieve significance in patients belonging to the lower percentile (P = 0.077). Diastolic blood pressure percentiles were not related to either cardiovascular events (HR 1.004, 95%CI 0.926–1.089, P = 0.922) or death (HR 0.955, 95%CI 0.894–1.019, P = 0.166).
Table 3 shows the hazard ratio of cardiovascular events in accordance with discrete systolic BP levels using the highest level as reference. Compared with the reference category of > 170 mm Hg, the incidence of cardiovascular events was significantly reduced in patients with SBP 101–110 (HR 0.647, 95%CI 0.455–0.920), 111-120 (HR 0.663, 95%CI 0.492–0.894), 121-130 (HR 0.747, 95%CI 0.569–0.981), and 131-140 (HR 0.757, 95%CI 0.596–0.962). Patients at lower systolic BP stratum (≤ 100 mm Hg) did not differ from reference (HR 0.765, 95%CI 0.525–1.115).
Tables 4 and 5 show the results of the multivariate analysis (Cox proportional hazards model) for combined CV events and death by any cause, respectively. The variables selected for the Cox proportional model were those showing significant association with hypertension in the univariate analysis plus age. The variables significantly associated with CV events were age (HR 1.013, 95%CI 1.003–1.022), diabetes (HR 1.874, 95%CI 1.548–2.270), pre-existing CV disease (HR 1.556, 95%CI 1.284–1.885), LV mass index (HR 1.003, 95%CI 1.001–1.005), and LV ejection fraction (HR 0.258, 95%CI 0.128–0518). Death by any cause was predicted by age (HR 1.017, 95%CI 1.009–1.025), diabetes (HR 1.571, 95%CI 1.345–1.895), associated CV disease (HR 1.442, 95%CI 1.234–1.684), LV mass index (HR 1.002, 95%CI 1.000–1.003), and LV ejection fraction (HR 0.202, 95%CI 0.144–0.359). Systolic and diastolic BP were not independently associated with events or death.
4 Discussion
The main finding of this investigation was that normotension and normal systolic interdialytic BP were not associated with an increased risk of cardiovascular events or death. Only patients with abnormally low systolic BP (< 100 mm Hg) had a hazard ratio of events not different from that in patients with uncontrolled hypertension. On the contrary, we observed that hypertension predicted an increased incidence of combined cardiovascular events. We, therefore, conclude that normal blood pressure is not harmful and that hypertension may increase the probability of future major cardiovascular complications in HD patients and must, therefore, be treated.
Contrary to the general population, BP fluctuates within a very large range in patients on dialysis due to rapid changes in extracellular volume and sodium balance during the procedure. It follows that BP may be more stable between 2 consecutive dialysis sessions so that this period should be preferred to study the associations between BP and outcomes, as we have done in our work. That is indeed the position assumed by the European Renal Association that recommends an out-of-dialysis BP measurement obtained during a pre-specified visit [7].
Observational studies consistently have reported elevated mortality in patients with normal or low BP levels. However, this finding has been attributed to BP instability when that variable is determined during the peridialysis period or caused by unmeasured confounders affecting blood pressure and mortality simultaneously. In the present work, using BP data obtained during the interdialytic period, we found that factors usually correlated with mortality like smoking, cardiovascular disease, previous myocardial infarction, longer dialysis treatment, and reduced left ventricular systolic function were indeed predominant in normotensive individuals. However, that did not reduce survival. In fact, patients with systolic BP within the normal range (101–140 mm Hg) had a reduced incidence of cardiovascular events compared with patients with systolic BP ≥ 171 mm Hg. Therefore, the results suggest that normal systolic BP does not always indicate an unfavorable prognosis even in high-risk dialysis patients, echoing observations in the general population. They also indicate that the hypothesis that the association of low-normal BP and mortality are caused by unmeasured confounders cannot be universally applied. However, when BP is very low (systolic BP < 100), the risk of outcomes does increase, as we have shown.
The majority of the available data indicate that low BP may increase the risk of death, the highest risk corresponding to a systolic BP considered normal, close to 120–140 mm Hg [11,12,13]. On the other hand, the association between higher systolic BP and mortality has been considered inconsistent [14]. However, this view has been challenged by more recent observations documenting a close association between high systolic BP and outcomes when BP was measured during the out-of-dialysis period [15,16,17]. In our work, we observed a trend to an increased incidence of death in hypertensive patients and in patients in the higher percentiles of systolic BP that did not achieve significance. It is worth noting that the Kaplan-Meier mortality curves appear to diverge after 5 years of follow-up (Figure 1). Interestingly, in a cohort of dialysis patients, higher predialysis systolic BP was associated with an increased risk of mortality only after 5 years of follow-up [18].
This work is the first confirmation of the study by Bansal et al in the CRIC cohort (16) showing that interdialytic BP may be preferred to guide treatment decisions in patients on dialysis. The present retrospective cohort is much larger (about 2500 patients) than the subpopulation of the CRIC cohort (about 400 patients) where the same BP component was analyzed. Our results are of interest for generalist as well as for physicians treating patients with advanced CKD and underscore the peculiarities of the interactions between BP and outcomes in this high-risk population.
Diastolic BP did not correlate with outcomes. The importance of diastolic BP on events received less attention in the literature compared with systolic BP. In one study, low pre- and post-dialysis diastolic BP were associated with mortality [19]. It has been suggested that this phenomenon is caused by the resultant increase in pulse pressure [8]. In our work, the changes in diastolic BP were relatively modest precluding any firm conclusion on that matter.
We did not document any significant effect of either systolic BP or diastolic BP on outcomes in the multivariate analysis. That is not really surprising considering that patients on dialysis have important risk factors that overshadow any possible additional effect exercised by BP. This means that the different risk exposure between hypertensive and normotensive patients is influenced by the greater comorbidity of hypertensives. Indeed, diabetes and LV mass index that were independent predictors of CV events and death were more frequent among hypertensive patients. The practical implication is that a proper control of BP, although important, may be not sufficient to improve prognosis.
4.1 Limitations
This was an observational unicentric study precluding conclusions on cause-effect relationships. BP was measured only at inception. Blood pressure, measured only a single point does not rule out the possibility of previous increased BP that may cause structural or functional CV alteration that persisted after control of hypertension. The list of confounding factors is not complete: we did not include information on calcium-phosphate metabolism, nutritional status, and causes of renal disease, among others. Although we checked and enforced the use of medication, changes could have been introduced by the dialysis team that were not controlled by the investigators. Patients were sent to our center because they were suspected of harboring CV disease and may not represent the whole dialysis population. On the positive side, the number of patients was large, the follow-up was long, the clinical and laboratory evaluation was prospective and obeyed a prespecified protocol, and all patients were periodically evaluated by the investigational group.
5 Conclusion
In this observational cohort study of HD patients, we did not find evidence linking normal interdialytic BP with mortality or with CV events and that hypertension was associated with an increased probability of serious cardiovascular complications. The clinical implications of our study are that interdialytic BP may be preferred to guide treatment decisions, and HD patients should be treated in accordance with the guidelines for the general population until specific BP targets for this population are identified.
Data availability
All data are available on request.
References
Agarwal R, Nissenson AR, Batlle D, Coyne DW, Trout JR, Warnock DG. Prevalence, treatment, and control of hypertension in chronic hemodialysis patients in the United States. Am J Med. 2003;115:291–7.
Agarwal R. Epidemiology of interdialytic ambulatory hypertension and the role of volume excess. Am J Nephrol. 2011;34:381–90.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13.
Zager PG, Nikolic J, Brown RH, Campbell MA, Hunt WC, Peterson D, Van Stone J, Levey A, Meyer KB, Klag MJ, Johnson HK, Clark E, Sadler JH, Teredesai P. “U” curve association of blood pressure and mortality in hemodialysis patients. Medical directors of dialysis clinic, inc. Kidney Int. 1998;54:561–9.
Salem MM. Hypertension in the haemodialysis population: any relationship to 2 years survival? Nephrol Dial Transplant. 1999;14:125–8.
Hannedouche T, Roth H, Krummel T, London GM, Jean G, Bouchet JL, Drüeke TB, Fouque D. French observatory. multiphasic effects of blood pressure on survival in hemodialysis patients. Kidney Int. 2016;90:674–84.
Sarafidis PA, Persu A, Agarwal R, Burnier M, de Leeuw P, Ferro CJ, Halimi JM, Heine G, Jadoul M, Jarraya F, Kanbay M, Mallamaci F, Mark PB, Ortiz A, Parati G, Pontremoli R, Rossignol P, Ruilope L, Van der Niepen P, Vanholder R, Verharr MC, Wiecek A, Wuerzner G, London GM, Zoccali C. Hypertension in dialysis patients: a consensus document by the European Renal and Cardiovascular Medicine (EURECA-m) working group of the European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) and the Hypertension and the Kidney working group of the European Society of Hypertension (ESH). Nephrol Dial Transplant. 2017;32:620–40.
Klassen PS, Lowrie EG, Reddan DN, DeLong ER, Coladonato JA, Szczech LA, Lazarus JM, Owen WF Jr. Association between pulse pressure and mortality in patients undergoing maintenance hemodialysis. JAMA. 2002;287:1548–55.
Agarwal R. Blood pressure and mortality among hemodialysis patients. Hypertension. 2010;55:762–8.
De Lima JJ, Gowdak LH, de Paula FJ, Muela HC, David-Neto E, Bortolotto LA. Coronary artery disease assessment and intervention in renal transplant patients: analysis from the KiHeart Cohort. Transplantation. 2016;100:1580–7.
Chang TI, Friedman GD, Cheung AK, Greene T, Desai M, Chertow GM. Systolic blood pressure and mortality in prevalent haemodialysis patients in the HEMO study. J Hum Hypertens. 2011;25:98–105.
Tozawa M, Iseki K, Iseki C, Takishita S. Pulse pressure and risk of total mortality and cardiovascular events in patients on chronic hemodialysis. Kidney Int. 2002;61:717–26.
Li Z, Lacson E Jr, Lowrie EG, Ofsthun NJ, Kuhlmann MK, Lazarus JM, Levin NW. The epidemiology of systolic blood pressure and death risk in hemodialysis patients. Am J Kidney Dis. 2006;48:606–15.
Chang TI. Systolic blood pressure and mortality in patients on hemodialysis. Curr Hypertens Rep. 2011;13:362–9.
Alborzi P, Patel N, Agarwal R. Home blood pressures are of greater prognostic value than hemodialysis unit recordings. Clin J Am Soc Nephrol. 2007;2:1228–34.
Bansal N, McCulloch CE, Rahman M, Kusek JW, Anderson AH, Xie D, Townsend RR, Lora CM, Wright J, Go AS, Ojo A, Alper A, Lustigova E, Cuevas M, Kallem R, Hsu CY. CRIC Study Investigators. Blood pressure and risk of all-cause mortality in advanced chronic kidney disease and hemodialysis: the chronic renal insufficiency cohort study. Hypertension. 2015;65:93–100.
Doulton TWR, Swift PA, Murtaza A, Dasgupta I. Uncertainties in BP management in dialysis patients. Semin Dial. 2020;33:223–35.
Mazzuchi N, Carbonell E, Fernández-Cean J. Importance of blood pressure control in hemodialysis patient survival. Kidney Int. 2000;58:2147–54.
Foley RN, Herzog CA, Collins AJ. United States Renal Data System. Blood pressure and long-term mortality in United States hemodialysis patients: USRDS Waves 3 and 4 Study. Kidney Int. 2002;62:1784–90.
Funding
There is no funding to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest to disclose.
Ethical approval
The protocol was approved by the institutional ethics committee (NCT01359722).
Informed consent
Patients signed an informed consent.
Permission to reproduce material
Not applicable.
Clinical trial registrationnot
Applicable.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
De Lima, J.J.G., Gowdak, L.H.W., Reusing Jr, J. et al. Interdialytic Blood Pressure and Risk of Cardiovascular Events and Death in Hemodialysis Patients. High Blood Press Cardiovasc Prev 30, 235–241 (2023). https://doi.org/10.1007/s40292-023-00575-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40292-023-00575-4