
Abstract
Introduction
Rheumatoid arthritis (RA) has a complex component induced by several genes that interact together with environmental and hormonal factors. We aimed to investigate the association of miR-196a2 rs11614913 (C/T) and miR-499a rs3746444 (A/G) polymorphisms and their combination with RA susceptibility and disease activity in an Egyptian population, and to evaluate their impact on methotrexate drug response and toxicity.
Materials and Methods
Bioinformatics databases were searched to select potential micro RNA (miRNA)–messenger RNA (mRNA) interactions involved in RA pathogenesis. Ninety-five RA patients diagnosed according to the American College of Rheumatology and 200 healthy controls were genotyped using real-time polymerase chain reaction technology.
Results
In overall and stratified analysis, miR-499a, but not miR-196a2, was associated with RA risk. Heterozygote carriers with rs3746444*A/G displayed protection against developing RA (p = 0.005) with an odds ratio of 0.2 (95 % confidence interval 0.17–0.62). The carriage of the combinations (miR499a*AG + miR196a2*CC) and (miR499a*AA + miR196a2*TT) were 3 and 7.5 times more likely to develop RA, respectively, while the combinations (miR499a*GG + miR196a2*CC), (miR499a*AG + miR196a2*TT) and (miR499a*AA + miR196a2*CT) show less susceptibility to have RA disease (all p < 0.05). rs3746444*AA genotype had a higher disease activity score (DAS28) [p = 0.023], tender joint count (TJC) (p = 0.007), and methotrexate-induced gastrointestinal toxicity (p = 0.043) compared with both AG/GG genotypes. rs11614913*C carriers were associated with higher DAS28 activity (p = 0.021). Homozygote male patients (CC and TT) had higher TJC (p = 0.046) and higher rheumatoid factor levels (p = 0.026), whereas, TT homozygote females had higher levels of ALT (p = 0.022).
Conclusions
Different genotypes of miR-499a rs3746444 single nucleotide polymorphisms (SNPs) are associated with RA risk, disease activity, and methotrexate toxicity in our population. In combination with specific miR-196a2 rs11614913 genotypes, this risk could increase or decrease according to the type of combination. Further functional analysis of the SNP and its impact on mRNA targets is required to confirm the relationship between genotype and phenotype.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
miR-499a rs3746444 genotypes, but not miR-196a2 rs11614913, were associated with rheumatoid arthritis (RA) risk and drug toxicity. |
Combined (miR499a*AG + miR196a2*CC) and (miR499a*AA + miR196a2*TT) genotypes were 3 and 7.5 times more likely to develop RA, respectively. |
miR-499a rs3746444*AA genotype had a higher disease activity score, tender joint count, and methotrexate-induced gastrointestinal toxicity compared with both AG/GG genotypes. |
Both of the study SNPs showed gender-specific association with disease activity and inflammatory markers. |
1 Introduction
Rheumatoid arthritis (RA) is a highly prevalent chronic immune-mediated inflammatory disease with articular and systemic effects, leading to joint destruction, deformity, and functional disability, with heterogeneous manifestations and multiple comorbidities [1]. RA is approximately three times as common in women as in men, and affects 0.5–2.0 % of the human population worldwide [2]. Although the mechanisms involved in disease initiation and progression has not been fully elucidated, numerous studies have demonstrated that RA has a complex component induced by several genes that interact together with environmental, hormonal, and stochastic factors [3]. Disease initiation takes place in peripheral lymphoid organs where dendritic cells present self-antigens to autoreactive T cells, which in turn activate autoreactive B cells through numerous cytokines and co-stimulatory molecules. This results in the production of autoantibodies followed by the deposition of immune complexes in the joint and other organs [4]. Synovial cell hyperplasia and endothelial cell activation are early events in the pathologic process that progresses to uncontrolled inflammatory cell infiltration, extensive angiogenesis, and consequent cartilage and bone destruction [5]. Abnormal production of numerous cytokines, chemokines, and other inflammatory mediators, such as tumor necrosis factor (TNF)-α, interleukin (IL)-1, -2, -6, -8, -10, and -17, transforming growth factor (TGF)-β, fibroblast growth factor (FGF), and platelet-derived growth factor (PDGF), are key modulators in the pathogenesis of RA [6]. As the disease progresses, the resident cells in rheumatoid joints, such as synovial fibroblasts, are activated, releasing collagenases, matrix metalloproteinases (MMPs), and adhesion molecules, which leads to destruction of matrix tissues. The net result of these activities is pannus formation with articular cartilage invasion, periarticular erosions and osteoporosis, and joint swelling with destruction of periarticular structures [2].
In the last decade, many therapies have been developed to target specific components of the inflammatory and autoimmune response in RA. Unfortunately, the response to these drugs is variable and the outcome cannot be predicted before starting the therapy [7]. Thus, a full understanding of the role of genetic and epigenetic regulation in RA signaling pathways might lead to a novel effective targeted treatment [5]. Recently, many groups have focused their attention on the role of micro RNAs (miRNAs) in the pathogenesis of RA, as well as a potential biomarker to monitor RA [2]. miRNAs are small (19–24 nucleotides long) non-coding RNAs that influence gene expression at the post-transcriptional level [8]. They are first transcribed from their corresponding gene loci as a primary transcript (pri-miRNA), spliced in the nucleus by the Drosha enzyme into a precursor hairpin loop (pre-miRNA), and exported to the cytoplasm to be cleaved by the Dicer enzyme forming an miRNA–miRNA* duplex (a guide strand and a passenger strand) [9]. Depending on the thermodynamics of a given duplex, its loading on to the miRNA binding pocket of the Argonaute (Ago) protein in the RNA-induced silencing complex (RISC) will select recruitment of one mature strand and ejection of the other passenger strand [2]. Mature miRNA bound to the Ago complex can recognize and bind target messenger RNAs (mRNAs) at the 3′-untranslated region (UTR), 5′-UTR, or protein coding sequence, resulting in their translational repression and/or degradation [8]. Thus, a single miRNA could virtually bind to hundreds of mRNA targets, and hence it is estimated that miRNAs influence the expression of approximately 60 % of all human genes [10]. miRNA has been shown to be one of the major regulators in a variety of biological processes such as cell cycle, apoptosis, cell differentiation, immune function, stress resistance, and metabolism. Aberrant expression of miRNA has been implicated in the pathogenesis of human diseases [2]. Dysregulation of miRNAs in peripheral blood mononuclear cell, T lymphocytes, synovial fibroblasts and osteoclasts as examples of key effector cells of joint destruction was shown to contribute to inflammation, degradation of the extracellular matrix (ECM), and invasive behavior of resident cells [1]. Literature screening of 80 studies, including 24 review articles, demonstrated overexpression of miR-142, miR-146a, miR-155, miR-203a, miR-214, miR-221/222, miR-223, and miR-323, and downregulation of miR-19b, miR-22, miR-23b, miR-30a, miR-34a, miR-124a, miR-363, and miR-498a in RA patients compared with healthy controls [5, 11]. They have been demonstrated to play an important role in inflammatory responses, cell proliferation of synoviocytes, and MMP production in rheumatoid joints [5].
In human diseases, the altered expression profile could be caused by genetic variations in DNA sequences of miRNA-coding genes [12]. These single nucleotide polymorphisms (SNPs) may influence miRNA processing, maturation, and/or miRNA–mRNA interactions, resulting in different functional events which may play a crucial role in the development and progression of a wide range of diseases [13]. Two common variants, miR-196a2 (rs11614913; C/T) and miR-499a (rs3746444; A/G), existing within the precursor miRNA gene loci were found to be involved in inflammatory conditions with autoimmune components [14–18]. MiR-196a2 is expressed from an intergenic region in HOX gene clusters, at chromosome 12q13.13 (110 nucleotides long, coordinates at 53991738–53991847 bp, positive strand). The non-coding transcript variant rs11614913 is located at nucleotide 78 (GRCh38 coordinates 12:53991815) at the passenger strand near the processing site. MiR-196a2 expression was only reported to be deregulated in RA synovial fibroblasts (RASF) [19] with no previous association study of its variants with RA susceptibility. The miR-499a gene is 122-base long, existing within the intron of myosin heavy chain 7 (MYH7B) gene clusters at chromosome 20q11.22 from position 34,990,376–34,990,497 bp. The rs3746444 SNP is located at nucleotide 73 (20:34990448) within the seed region of the mature miR-499 sequence [13, 20]. With the comprehensive literature review, some evidences showed this later SNP was associated with various aspects of RA [21–23]; however, few studies were conducted to validate the association between the selected study variants with RA susceptibility, activity, and drug toxicity in our population, especially in the case of miR-196a2. As miRNAs could have potential implications as biomarkers or therapeutic targets, we performed this current preliminary association study to determine whether the rs11614913 and rs3746444 polymorphisms, or their combination, were associated with RA risk, activity, methotrexate treatment response and toxicity in an Egyptian population.
2 Materials and Methods
2.1 Study Participants
A total of 295 subjects (95 cases of unrelated RA and 200 age- and gender-matched controls) were enrolled in the current study. RA patients were diagnosed according to the 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) classification criteria of RA and had been treated with methotrexate for at least 6 months. Patients were attending the outpatient Rheumatology and Orthopedic Clinics, Suez Canal University Hospitals. Patients’ disease activity status at the start of methotrexate therapy was evaluated using the disease activity score [DAS28 C-reactive protein (CRP); a validated composite outcome measure consisting of the 28 tender joint counts (TJC28) representing the number of joints that are tender (first through fifth metacarpophalangeal joints and the interphalangeal joint of the thumb, and the second through fifth proximal interphalangeal joint, elbows, shoulders and knees), the 28 swollen joint count (SJC 28), CRP and global health parameter representing the patient’s self-assessment of disease activity on a scale of 0–100, where 100 indicates maximal disease activity] [24]. Participants underwent pretreatment clinical assessment, physical examination, routine laboratory measurements, including complete blood counts, liver function tests, screening of hepatitis C and B, serum CRP and erythrocyte sedimentation rate (ESR), kidney function test, and chest X-ray. RA patients were re-evaluated at 4 weeks then every 4–8 weeks [25]. We initiated methotrexate at a dose between 7.5 and 10 mg once weekly depending upon the degree of disease activity and the presence of comorbidities. Then the dose was increased as tolerated 2.5 mg weekly. In patients who exceeded 15mg/week, we shifted from oral administration to an intramuscular injection up to a maximum dose 25 mg/week. Folic acid 10 mg/week was administered in the morning the day after the methotrexate administartion [26]. Starting from a dose of 15 mg, we shifted our patients from oral to intramuscular injection [27]. Methotrexate was administered with non-steroidal anti-inflammatory drugs (NSAIDs) on and off. For clinical improvement evaluation, the patient was classified as a good responder to treatment when the DAS28 was ≤2.6 at 3 months, low disease activity if the DAS28 was ≥2.6 to ≤3.2, moderate disease activity if the DAS28 was >3.2 and ≤5.1, and high disease activity when the DAS28 was >5.1 [24]. The second group of ‘poor responders’ included patients with active disease despite at least 3 months of therapy. Toxicity for methotrexate was assessed by reviewing medical records, recording the patients’ history, and by measuring routine laboratory parameters. Toxicity was graded as mild (requiring dose reduction by 2.5 mg/week or a change in the route of administration), moderate (requiring temporary stoppage of methotrexate), or severe (requiring permanent stoppage of methotrexate) [27].
The control group included 200 unrelated healthy blood donors with no past or family history of RA or associated autoimmune disease. The study was conducted in accordance with the guidelines of the Declaration of Helsinki.
2.2 Biochemical and Immunochemical Analysis
Blood samples were drawn from all subjects after overnight fasting, and ESR was evaluated using the traditional method after 1 and 2 h. Serum CRP and immunoglobulin M (IgM) rheumatoid factor (RF) using the immunoturbidimetric method [28], serum creatinine and serum alanine transaminase were measured using a Cobas Integra 400 analyzer (Roche Diagnostics, Mannheim, Germany) according to the manufacturer’s instructions. RF values of ≥20 IU/mL were considered positive [29].
2.3 Single Nucleotide Polymorphism Identification
Genomic DNA was extracted from venous blood using a QIAamp DNA Blood Mini kit (Catalog No. 51104; Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Extracted DNA concentration and purity were measured using a NanoDrop ND-1000 (NanoDrop Technologies, Inc. Wilmington, DE, USA). DNA samples of patients and controls were genotyped for the hsa-miR-196a2 and hsa-miR-499a polymorphisms. Polymerase chain reaction (PCR) was performed in a 25-µL reaction volume containing genomic DNA (20 ng) diluted to 11.25 μL with DNase–RNase-free water, 12.5 μl Taqman® Universal PCR Master Mix, No AmpErase UNG (2×) and 1.25 µl 20× TaqMan® SNP Genotyping Assay Mix (assay ID C_31185852_10 for rs11614913 and C_2142612_30 for rs3746444; Applied Biosystems, Foster City, CA, USA). Genotyping was performed blinded to the case/control status, and appropriate negative controls were used. Real-time PCR amplification was performed using the StepOne™ Real-Time PCR System (Applied Biosystems) using the following conditions: two initial holds (50 °C for 2 min and 95 °C for 10 min) followed by a 40-cycle two-step PCR (95 °C denaturation for 15 s and annealing/extension 60 °C for 1 min). Allelic discrimination was called by the SDS software version 1.3.1 (Applied Biosystems). The overall genotype call rate using the TaqMan allelic discrimination assays were 100 %, and the genotyping reproducibility was 100 % in 32 (10 %) randomized samples genotyped in duplicate.
2.4 Identifications of the Predicted Target Gene Set
Multiple online computational tools were used to identify predicted target genes (in the coding sequence (CDS), 3′untranslated region (3′UTR), or 5′UTR regions) for the studied miRNAs, such as DIANA-microT-CDS v5.0 (http://www.microrna.gr/microT-CDS), miRTarBase v 20 (http://mirtarbase.mbc.nctu.edu.tw/) [30], TargetScanHuman v6.2 (http://www.targetscan.org/), PicTar (http://pictar.mdc-berlin.de/), and miRDB (http://mirdb.org).
2.5 Exploring Micro DNA Disease Interaction
The predicted miRNA target genes were analyzed for functional annotation clustering and Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment pathways [31] using the DIANA-miRPath v2.0 web-server with default settings [32]. In addition, the physical interaction relationships and biological functions of both miR-196a2 and miR-499 with genes of the rheumatoid arthritis-related KEGG pathway were analyzed using the miRTar.Human tool (http://miRTar.mbc.nctu.edu.tw/). Moreover, the miRPub database (http://www.microrna.gr/mirpub/), used for searching miRNA publications, was used to link the studied miRNAs to autoimmune and inflammatory diseases [33]. The Gene Expression Omnibus (GEO) Database (http://www.ncbi.nlm.nih.gov/sites/GDSbrowser) and the MalaCards Human Disease Database (http://www.malacards.org/) were used to detect genes deregulated in RA joints compared with controls.
2.6 Predicted Functional Effect of rs11614913 and rs3746444 Polymorphisms
The predicted functional impact of miR-196a* (5′-CGGCAACAAGAAACUGC[C/U]UGAG-3′) and miR-499a* (5′AAC[A/G]UCACAGCAAGUCUGUGCU-3′) polymorphisms at the 3p arm was performed using miRmut2Go (http://compbio.uthsc.edu/miR2GO), a web-based platform for comparative functional analysis of mutations in miRNAs based on the enriched functional annotations of reference and derived target gene sets [34]. Selected parameter settings included combining both the TargetScan and miRanda methods for miRNA target prediction, the p value threshold for functional enrichment set as <0.01, and medium Gene Ontology hierarchical filtering level.
2.7 Statistical Analyses
All statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 20 (IBM Corporation, Armonk, NY, USA), and the test for normality was performed using the Shapiro–Wilk test. For quantitative variables, the one-way analysis of variance (ANOVA) test for parametric data, as well as the Mann–Whitney and Kruskal–Wallis tests, were used for non-parametric variables. For qualitative variables, the Chi square test was used. We applied the Bonferroni method to adjust for multiple comparisons. The allele frequency within each group was determined as the number of occurrences of an individual allele divided by the total number of alleles. The Hardy–Weinberg equilibrium (HWE) for each SNP was tested by using a goodness-of-fit Chi square test with a degree of freedom equal to 1 via the Online Encyclopedia for Genetic Epidemiology (OEGE) software (http://www.oege.org/software/hwe-mr-calc.shtml). The associations of the rs11614913 and rs3746444 genotypes, and susceptibility to RA, were estimated by computing odds ratios (ORs) and their 95 % confidence intervals (CIs) from unconditional logistic regression analysis with the adjustment for possible confounders. A p value <0.05 was considered statistically significant, and all statistical tests were two-sided. The statistical power was estimated using Quanto software version 1.2.4; (http://biostats.usc.edu/software, University of Southern California). Calculations showed that sample size, together with the specified study design, allele frequencies, and allowable error rates under a dominant model, can give as high as 80 % power.
3 Results
3.1 Characteristics of Study Subjects
The baseline characteristics of RA cases and controls are shown in electronic supplementary Table S1. Age and gender were matched adequately. Similarly, there were no statistically significant differences in smoking status and family history of RA between the case and control groups.
3.2 Association of Pre-miRNA Variants with Rheumatoid Arthritis Risk
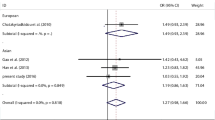
The frequency distribution of miR-196a2 and miR-499a polymorphisms in RA patients and healthy subjects are demonstrated in Table 1. miR-196a2 genotypes were in agreement with those expected by the HWE in RA patients and controls (p = 0.186 and 0.083, respectively), while miR-499a genotypes showed a deviation from this equilibrium (p < 0.05) in both study groups due to increased minor allele frequency (MAF) being more than expected. MAFs were 0.23 and 0.27 for rs11614913*T, and 0.39 and 0.42 for rs3746444*G in patients and controls, respectively. A significant difference was found between patients and control groups with regard to rs3746444 genotypes (p = 0.005), but not with the rs11614913 polymorphism (p = 0.106). Carrying both alleles, rs3746444*A/G displayed protection against developing the RA disease (15.8 and 34 % in patients and controls, respectively) with an OR of 0.2 (95 % CI 0.17–0.62) under the co-dominant genetic model. Stratified analysis by gender and age showed that the AG genotype of the miR-499a variant rendered protection against RA in women (p = 0.003) and young patients (p = 0.014) (Fig. 1); however, combined genotype analysis revealed a differential effect of miR-499a genotypes when existing with certain miR-196a2 genotypes. The carriage of combinations (miR499a*AG + miR196a2*CC) and (miR499a*AA + miR196a2*TT) were 3 and 7.5 times more likely to develop RA, respectively, while the combinations (miR499a*GG + miR196a2*CC), (miR499a*AG + miR196a2*TT), and (miR499a*AA + miR196a2*CT) showed less susceptibility to having RA disease (all p < 0.05) (Fig. 2).

Genotype frequencies of a hsa-miR-196a2 (rs11614913: C/T) and b hsa-miR-499a (rs3746444: A/G) polymorphisms in rheumatoid arthritis patients and controls according to gender and age

Association of hsa-miR-196a2 (rs11614913: C/T) and hsa-miR-499a (rs3746444: A/G) genotype combinations with rheumatoid arthritis risk. Gray bars indicate controls, black bars indicate patients. Significant ORs (95 % CI) are written above the bars; red OR indicates risk, blue OR shows protection. OR odds ratio, CI confidence interval
3.3 Relation Between Pre-miRNA Variants and the Clinical and Laboratory Data of RA Patients
With regard to rs11614913, a significant association was observed between C-variant patients with CC and CT genotypes and degree of DAS28 activity (p = 0.021) [electronic supplementary Table S2]. Stratification analysis by gender also showed differential association with disease activity and inflammatory markers among different genotypes (Figs. 3, 4). Male RA patients with homozygote genotypes (CC and TT) had a higher TJC than heterozygotes (p = 0.046), and higher levels of RF compared with the heterozygote CT patients (p = 0.026). In contrast, homozygote women with the TT genotype had significantly higher levels of ALT in the blood (p = 0.022). Interestingly, early-onset RA patients with the CT/TT genotypes had a significantly higher frequency of positive family history compared with CC carriers (p = 0.035; data not shown).

Gender-specific association of hsa-miR-196a2 (rs11614913: C/T) and hsa-miR-499a (rs3746444: A/G) genotypes with rheumatoid arthritis activity. Data are represented as medians. The box defines upper and lower quartiles (25 and 75 %, respectively) and the error bars indicate upper and lower adjacent limits. The Kruskal–Wallis and Mann–Whitney U tests were used. Statistical significance at p < 0.05 is illustrated

Gender-specific association of hsa-miR-196a2 (rs11614913: C/T) and hsa-miR-499a (rs3746444: A/G) genotypes with inflammatory markers. Data are represented as medians. The box defines upper and lower quartiles (25 and 75 %, respectively) and the error bars indicate upper and lower adjacent limits. The Kruskal–Wallis test was used. Statistical significance at p < 0.05 is illustrated
For the rs3746444 SNP, the AA genotype was associated with lower levels of body mass index (BMI) [p = 0.003; electronic supplementary Table S3]; however, it showed higher DAS28 activity (p = 0.023), elevated TJC (p = 0.007), and more frequent methotrexate-induced gastrointestinal toxicity (p = 0.043) compared with both AG/GG genotypes. In affected women, although the same genotype (AA) was associated with lower disease duration (<5 years), they also presented with higher degrees of DAS28 activity (p = 0.031) and TJC (0.024) (Fig. 3). No significant association was observed between the rs3746444 SNP and the levels of inflammatory markers, such as CRP, ESR, RF, or ALT (all p > 0.05) (Fig. 4). In addition, overall and stratified analysis by gender, age at onset, and disease duration did not show significant differences in genotype combinations with disease activity, drug response, or toxicity.
3.4 Predicted Target Gene Lists
Human miR-196a2 and miR-499a genes are 121 and 122 base pairs in length, respectively. During the biogenesis process, precursor hairpin transcripts undergo two cleavage processes. Each stem loop produces two different mature forms from the 5p and 3p arms. Hundreds of genes were predicted to be targeted by miR-196a2 and miR-499a (Fig. 5; electronic supplementary Table S4).

Predicted target genes of hsa-miR-196a2 and hsa-miR-499a. a Hairpin structure of the hsa-mir-196a2 stem loop. Mature forms at the 5p and 3p arms are illustrated in red and blue, respectively. The studied single nucleotide polymorphism rs11614913 C > T at the 3′ end of miR-196a2-3p is highlighted in green and is indicated by the arrow. b Hairpin structure of the hsa-mir-499a stem loop. Mature forms at the 5p and 3p arms are illustrated in red and blue, respectively. The studied single nucleotide polymorphism rs3746444 A > G in the seed region of miR-499a-3p is highlighted in green and is indicated by the arrow [data source: miRBase release 21 (http://www.mirbase.org/) and miRNAMap version 2.0 (http://miRNAMap.mbc.nctu.edu. tw/)]. c Intersection between predicted target genes of the mature forms of both miR-196a2 and miR-499a. A detailed gene list is mentioned in electronic supplementary Table S4. d Differential predicted target genes of miR-499a according to the rs3746444: A > G SNP [data source: PolymiRTS Database 3.0 (http://compbio.uthsc.edu/miRSNP/)]
3.5 Functional Annotation Clustering and miRNA Disease Interaction
Enriched KEGG pathway analyses of predicted and validated targets using the DIANA-miRPath v2.0 web-server (at a threshold of 0.7) and the miRTar.Human tool (http://miRTar.mbc.nctu.edu.tw/) showed that the targeted genes regulated by mir-196a2 and miR-499a were involved in critical cell functions and various immune processes (Fig. 6). Some of these signaling pathways are responsible for the overall mRNA processing and degradation, such as mRNA surveillance, RNA transport, and RNA degradation, while others are related to the inflammatory process, such as TGFβ and mitogen-activated protein kinase (MAPK) signaling pathways, focal adhesion, ECM-receptor interaction, Fc gamma R-mediated phagocytosis, leukocyte transendothelial migration, and chemokine signaling pathway. In addition, the studied miRNA can regulate gene expression in glycosaminoglycans biosynthesis and degradation. Specifically, miR-499a-5p binds to CD28 and IL23 genes involved in the pathogenesis of the rheumatoid arthritis pathway (KEGG 05323) (Fig. 7). The MalaCards Human Diseases Database and GEO database reported 57 genes differentially expressed in cartilage tissues of RA patients versus healthy controls, six of which (DDX3Y, ADCY2, NFIL3, FABP4, ATF3, and TCF7L2) are predicted targets of miR-499a, and three (MAOA, TOX3, and TRHDE) are targeted by miR-196a2. All were downregulated more than threefold.

Functional clustering annotation of hsa-miR-196a2 and hsa-miR-499a predicted targets. a Enrichment pathway analysis. Heat map showing targeted pathways for mature forms of both hsa-miR-196a2 and hsa-miR-499a with p values <0.05 and microT-coding sequence (CDS) threshold of 0.5. A total of 50 pathways have target genes (in the CDS or 3′-UTR regions): 10 for miR-196a2-5p, 12 for miR-196a2-3p, with only one intersecting pathway responsible for the mRNA surveillance pathway targeted by both mature miRNAs. On the other hand, 31 pathways were targeted by miR-499a-5p, and 22 pathways were targeted by miR-499a-3p, with 13 common pathways. The degree of color is based on the significant p values of the predicted algorithm using the DIANA tools; red has the highest score of statistical significance. b miR-196a2 and miR-99a regulate multiple rheumatoid arthritis-related inflammatory KEGG pathways [data source: DIANA-miRPath v2.0 and miRTar.Human web-server]. mRNA messenger RNA, miRNA micro RNA, KEGG Kyoto Encyclopedia of Genes and Genomes, TGF transforming growth factor receptor, MAPK mitogen-activated protein kinase

Human miR-499a regulates target genes in the rheumatoid arthritis pathway. a Rheumatoid arthritis pathway (KEGG ID: 05323). White boxes indicate genes and proteins involved in the pathogenesis of rheumatoid arthritis disease, cells are shown in red, the targeted genes are shown in the orange box, and the pathological process is shown in the yellow boxes. b Alignment of miR-499a and predicted target genes [data source: microRNA.org]. Ag Antigen, Ang1 angiopoietin 1, CCL C-C motif chemokine, CD cluster of differentiation, CTGA4 cytotoxic T-lymphocyte-associated protein 4, CTSK cathepsin K, CTSL cathepsin L, CXCL C-X motif chemokine, FLT1 FMS-like tyrosine kinase 1, GMCSF granulocyte-macrophage colony-stimulating factor, IFN interferon, IGg immunoglobulin G, IL interleukin, KEGG Kyoto Encyclopedia of Genes and Genomes, LTB lymphotoxin beta, MHCII major histocompatibility complex class II, MMP1/3 matrix metalloproteinase-1/3, RANKL receptor activator of nuclear factor kappa-B ligand, TCR T-cell receptor, TGF transforming growth factor, Th cells T helper cells, Tie endothelial-specific receptor tyrosine kinase, TNF tumor necrosis factor, TRAP tartrate-resistant acid phosphatase, VEGF vascular endothelial growth factor
3.6 Functional Impact of miR-196a2 and miR-499a Variants
Both studied common variants exist in the passenger strand; rs11614913 SNP of the miR-196a2* gene at the 3′ end, and rs3746444 SNP of the miR-499a gene at the 5′ end, inside the ‘seed region’, which is essential for the miRNA-mediated silencing mechanism (Fig. 5). Comparative functional analysis using the miRmut2Go server reveals no functional consequence of rs11614913 polymorphism on the predicted target gene sets, with a complete similarity score for molecular function, biological process, and cellular components, while the rs3746444 polymorphism causes disruption of 667 targets and the creation of 744 new gene targets. Within the seed region of miR-499a, another nearby SNP (rs150018420; C > T) is present at nucleotide 77, which might be in linkage disequilibrium with the rs3746444 SNP at nucleotide 73 and may cause alteration of the miRNA target gene set (PolymiRTS Database 3.0).
4 Discussion
In this preliminary study, we investigated for the first time the combined genotype effects of miRNA-196a2 rs11614913 and miR-499a rs3746444 polymorphisms with RA susceptibility and activity in an Egyptian population sample. The rs3746444 SNP was revealed to be associated with an increased risk of RA and drug toxicity; however, it showed a differential effect when combined with various rs11614913 genotypes. Both SNPs showed a gender-specific association with disease activity and inflammatory markers. Among the whole study population, MAF of the pre-miRNA variants were 25 % for miR-196a2*T and 40.5 % for miR-499a*G. These allele frequencies were different from those reported by the 1000 Genome Project (electronic supplementary Fig. 1). Egypt has unique geographic sectors with intra-population cultural and environmental differences. In addition, throughout history, the Arabs, Romans, Greeks, Turks, French, and British have all ruled Egypt, especially the Suez Canal area (from which our population have been selected) [35]. Thus, there is a considerable genetic admixture in the Egyptian population, which might explain our unique genetic signature. This could also contribute to deviation from the HWE (p < 0.05) in the case of miRNA-499a genotyping in the current study. As genotype frequencies differ from those we would expect under equilibrium, we can assume that one or more of the model’s assumptions of the HWE has been violated. In our case, the gene flow between populations, from migration or transfer of gametes, could be the cause [36].
In the current study, a positive association between miR-499a genotypes and susceptibility to RA disease was identified. Heterozygote individuals carrying both A and G alleles of rs3746444 conferred protection against developing RA in our adult Egyptian population. This protection was significantly evident in female patients but not in males. However, we should mention that great care should be taken with interpretation and comparison of the current reported result as the female participants were approximately 88.5 % of the current study population, which could overestimate the gender difference. Similarly, in a prior Egyptian study conducted in a different geographic area (in the Nile Delta region), miRNA-499a was also an independent factor of RA risk, but the frequency of the AG genotype was significantly higher in RA patients compared with controls [37]. Two previous meta-analysis studies conducted on Caucasians, Asians, and Mediterranean populations also revealed an association between miR-499a polymorphism and RA risk [16, 38]. In addition, the miR-499a rs3746444 SNP has been previously associated with other autoimmune and inflammatory diseases. The homozygote AA genotype exhibited a significantly higher risk of Behcet’s disease in Turks [18] and chronic obstructive pulmonary disease (COPD) in Chinese patients [39]. The GG genotype was associated with primary tuberculosis in Tibetan and Chinese patients [14], as well as in schizophrenia [40] and hepatitis B virus-related hepatocellular carcinoma [41], whereas, the heterozygote AG genotype had an association with ulcerative colitis in Japanese patients [15] and idiopathic recurrent spontaneous abortion in Korean women [42]. In contrast, no association was found in Chinese patients with systemic lupus erythematosis [43], asthma [44], and coal workers’ pneumoconiosis [45]; thus, miR-499a appears to be a key player in RA initiation as it may regulate CD28 and IL-23a, which are important in T-cell maturation and development in the RA pathway [KEGG 05323] (Fig. 7). T-cell-specific surface glycoprotein CD28 is essential for T-cell proliferation and survival, cytokine production, and T-helper type 2 development. IL-23a stimulates the production of interferon-γ, activates the Jak-Stat signaling cascade, stimulates memory rather than naive T cells, promotes production of proinflammatory cytokines, and induces autoimmune inflammation (Genecards.org). Our in silico analysis showed the miR-499a rs3746444 polymorphism to be located within the stem region of the miR-499 gene, and results in an A:U to G:U mismatch in the stem structure of the miR-499 precursor (Fig. 5). The SNP is in the seed region (the first eight nucleotides) at the 5′ end of the mature miR-499a-3p, which is essential for miRNA– mRNA binding, and thus results in the disruption and creation of gene targets (http://compbio.uthsc.edu/miR2GO). Homozygote individuals (AA or GG) can produce two mature forms (miR-499a and miR-499a*A or *G, respectively), each with its own distinct set of target genes. Therefore, the AG heterozygosity is the only state that can have three mature forms (miR-499a, miR-499a*A, miR-499a*G), with target genes comprising all three subsets.
For the rs11614913 polymorphism, no significant difference was found in the present study between patients and controls under all tested genetic models. Similar insignificant results were previously reported in asthmatic Chinese patients [46] and coal workers’ pneumoconiosis [45]. In contrast, the TT genotype of miR-196a2 showed a higher risk of refractory phenotype of ulcerative colitis [15] and higher degree of mononuclear cell infiltration in gastric cancer in the Japanese population [47], whereas the CC genotype and C allele showed association with higher risk of COPD among Chinese patients [39] and idiopathic recurrent spontaneous abortion in Korean women [42, 48]. Combined genotype analysis revealed two unfavorable and three favorable combinations in our study population. When combined with miR196a2*TT, the miR499a*AG carriers showed a similar protected effect reported earlier in single SNP analysis, but when combined with the other homozygote, the miR196a2*CC genotype showed threefold more susceptibility to develop RA disease, while the homozygote miR499a*AA was considered a possible risk factor when combined with miR196a2*TT but not with miR196a2*CT genotypes. This combined effect was also reported in several prior studies. The carriage of combinations (miR-196a2CC/miR-499AG) represented possible independent risk factors for idiopathic recurrent spontaneous abortion in Korean women [42] and more severe multiple sclerosis course in Russians, especially in women patients [49]. The regulation and synergistic interaction of different target genes by heterozygote compared with homozygotes for miR-196a2 and miR-499a genotypes may explain differential susceptibility in human disease.
RA is characterized by persistent joint synovial tissue inflammation. Over time, destruction of cartilage, bone erosion, and complete loss of joint integrity can occur. Eventually, multiple organ systems may be affected [50]. In the current study, the rs11614913*C variant (CC and CT) was associated with higher disease activity in RA patients, based on the DAS28 score. Homozygote male patients (CC or TT) had more TJC and higher levels of serum RF compared with corresponding heterozygotes, while TT female patients had significantly higher levels of ALT. Hu et al. demonstrated that rs11614913 in the pre-miRNA-196a was associated with an increase in mature miRNA expression [51]. In vitro, Hoffman et al. also reported an increased expression of mature miR-196a2 in breast cancer cells transfected with pre-miR-196a-C vector compared with cells transfected with pre-miR-196a-T, but did not observe the differential expression of the pre-miRNA, suggesting that miR-196a2 genotypes may result in altered processing of the precursor hairpin loop into mature forms [52]. Enrichment pathway analysis revealed that miR-196a2 could play an important role in disease progression, neovascularization, pannus formation, and bone resorption. It can target nine genes in toll-like receptor signaling pathways (TRAF6, TLR5, PIK3CA, NFKB1, MAPK3, MAP2K6, MAP2K3, IKBKE, AKT1) [miRTar.Human], which result in the activation of cells of the innate immune system in RA as monocytes, macrophages, and dendritic cells, leading to the rapid expression of pro-inflammatory cytokines, such as TNFα, and chemokines, such as IL-8 and CCL2 [53]. In addition, miR-196a2 could also regulate the expression of PRKCA, RAF1, MAPK3, PPP3CC, NFATC4, and PIK3CA, which are regulators of the vascular endothelial growth factor (VEGF) signaling pathway (DIANA-miRPath v2.0). This pathway is responsible for neovascularization of the inflamed synovium in RA, with further leukocyte recruitment, tissue remodeling, and joint swelling [54]. The results of this study provided the first evidence that the SNP rs11614913 in pre-miR-196a2 could affect the inflammatory reaction in patients with RA. Positive RF with high titer and the presence of high ALT are predictors of poor outcomes in RA as these parameters indicate the development of extra-articular systemic inflammation [55]. In addition, elevated ALT usually occurs in patients receiving methotrexate, thus providing another possible mechanism [56].
For the rs3746444 SNP, the AA genotype was associated with lower levels of BMI, higher DAS28 activity, elevated TJC, and more frequent methotrexate-induced gastrointestinal toxicity compared with both AG/GG genotypes. These associations also showed gender specificity as disease activity was not significant in men and substantially reinforced in women. The observed gender difference may result from the interaction between the genotype and sexual hormones during disease development. Gender-dependent associations have been shown in other case–control studies involving immune entities [37, 57]. Our in silico approaches highlighted the important role of miR-499a in normal immune function at different levels. They can control many immune processes, including T-cell development and maturation, T- and B-cell receptor signaling, toll-like receptor signaling cascade, and chemokine signaling pathway. Moreover, they can regulate glycosaminoglycans biosynthesis and degradation essential for cartilage hemostasis. In addition, miR-499a regulates various rheumatoid arthritis-associated pathogenic pathways, including MAPK, VEGF and TGF-β signaling pathways involved in osteoblast differentiation, cytokine production, leukocyte infiltration, and synovial angiogenesis (DIANA-miRPath v2.0).
It is worthwhile to mention that although the current study first demonstrated the combined genotype effect of miR-196a2 rs11614913 (C/T) and miR-499a rs3746444 (A/G) variants on RA susceptibility, disease activity, and their impact on methotrexate drug response and toxicity in our population, there are some limitations in the present study. The sample of patients in our preliminary study was relatively small, therefore the results observed need to be confirmed using a large sample size and should include other distinct geographic areas. In addition, the lack of consideration of combined genetic factors, together with environmental exposures and other treatment modalities also need to be confirmed. Future studies will be needed in order for all these issues to be clarified.
5 Conclusions
The results of the current study suggest that SNP rs3746444 (A/G) may have a role, especially in a gender-specific pattern, in RA risk, disease activity, and methotrexate toxicity in our population. In combination with SNP rs11614913 (C/T), this association could be modified according to the type of combination. These findings are significant in that they might contribute to the clinical assessment of RA susceptibility and activity, which in turn may influence therapeutic decision making. Further functional studies will be required to clarify the mechanism of how these two SNPs and their combined genotypes affect the inflammation of RA and response to treatment.
References
Murata K, Furu M, Yoshitomi H, Ishikawa M, Shibuy H, Hashimoto M, et al. Comprehensive microRNA analysis identifies miR-24 and miR-125a-5p as plasma biomarkers for rheumatoid arthritis. PLoS One. 2013;8:e69118.
Chen XM, Huang QC, Yang SL, Chu YL, Yan YH, Han L, et al. Role of micro RNAs in the pathogenesis of rheumatoid arthritis: novel perspectives based on review of the literature. Medicine (Baltimore). 2015;94:e1326.
Wang X, Xia S, Fu B. RNA-seq analysis of synovial fibroblasts in human rheumatoid arthritis. Mol Med Rep. 2014;10:241–7.
Bolon B. Cellular and molecular mechanisms of autoimmune disease. Toxicol Pathol. 2012;40:216–29.
Song YJ, Li G, He JH, Guo Y, Yang L. Bioinformatics-based identification of microRNA-regulated and rheumatoid arthritis-associated genes. PLoS One. 2015;10:e0137551.
Choy E. Understanding the dynamics: pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology. 2012;51:v3–11.
Ceribelli A, Nahid MA, Satoh M, Chan EK. MicroRNAs in rheumatoid arthritis. FEBS Lett. 2011;585:3667–74.
Toraih EA, Mohammed EA, Farrag S, Ramsis N, Hosny S. Pilot study of serum microRNA-21 as a diagnostic and prognostic biomarker in Egyptian breast cancer patients. Mol Diagn Ther. 2015;19:179–90.
Kishore A, Borucka J, Petrkova J, Petrek M. Novel insights into miRNA in lung and heart inflammatory diseases. Mediators Inflamm. 2014;2014:259131.
Li Q, Chen L, Chen D, Wu X, Chen M. Influence of microRNA-related polymorphisms on clinical outcomes in coronary artery disease. Am J Transl Res. 2015;7:393–400.
Duroux-Richard I, Jorgensen C, Apparailly F. What do microRNAs mean for rheumatoid arthritis? Arthritis Rheum. 2012;64:11–20.
Cammaerts S, Strazisar M, De Rijk P, Del Favero J. Genetic variants in microRNA genes: impact on microRNA expression, function, and disease. Front Genet. 2015;6:186.
Chen C, Yang S, Chaugai S, Wang Y, Wang DW. Meta-analysis of Hsa-mir-499 polymorphism (rs3746444) for cancer risk: evidence from 31 case-control studies. BMC Med Genet. 2014;15:126.
Li D, Wang T, Song X, Qucuo M, Yang B, Zhang J, et al. Genetic study of two single nucleotide polymorphisms within corresponding microRNAs and susceptibility to tuberculosis in a Chinese Tibetan and Han population. Hum Immunol. 2011;72:598–602.
Okubo M, Tahara T, Shibata T, Yamashita H, Nakamura M, Yoshioka D, et al. Association study of common genetic variants in pre-microRNAs in patients with ulcerative colitis. J Clin Immunol. 2011;31:69–73.
Lu L, Tu Y, Liu L, Qi J, He L. MicroRNA-499 rs3746444 polymorphism and autoimmune diseases risk: a meta-analysis. Mol Diagn Ther. 2014;18:237–42.
Yang Y, Zhang K, Zhou R. Meta-analysis of pre-miRNA polymorphisms association with susceptibility to autoimmune diseases. Immunol Invest. 2014;43:13–27.
Oner T, Yenmis G, Tombulturk K, Cam C, Kucuk OS, Yakicier MC, et al. Association of pre-miRNA-499 rs3746444 and pre-miRNA-146a rs2910164 polymorphisms and susceptibility to Behcet’s disease. Genet Test Mol Biomark. 2015;19:424–30.
Filkova M, Trenkmann M, Stanczyk J, et al. MiR-196a is an important regulator of synovial fibroblasts in the pathogenesis of rheumatoid arthritis [abstract]. Arthritis Rheum. 2011;63(Suppl 10):2519.
McFarland AP, Horner SM, Jarret A, Joslyn RC, Bindewald E, Shapiro BA, et al. The favorable IFNL3 genotype escapes mRNA decay mediated by AU-rich elements and hepatitis C virus-induced microRNAs. Nat Immunol. 2014;15:72–9.
Hashemi M, Eskandari-Nasab E, Zakeri Z, Atabaki M, Bahari G, Jahantigh M, et al. Association of pre-miRNA-146a rs2910164 and pre-miRNA-499 rs3746444 polymorphisms and susceptibility to rheumatoid arthritis. Mol Med Rep. 2013;7(1):287–91.
Song GG, Bae SC, Seo YH, Kim JH, Choi SJ, Ji JD, et al. The association between susceptibility to inflammatory arthritis and miR-146a, miR-499 and IRAK1 polymorphisms. A meta-analysis. Z Rheumatol. 2015;74(7):637–45.
Fu L, Jin L, Yan L, Shi J, Wang H, Zhou B, et al. Comprehensive review of genetic association studies and meta-analysis on miRNA polymorphisms and rheumatoid arthritis and systemic lupus erythematosus susceptibility. Hum Immunol. 2016;77(1):1–6.
Aletaha D, Ward MM, Machold KP, Nell VP, Stamm T, Smolen JS. Remission and active disease in rheumatoid arthritis: defining criteria for disease activity states. Arthritis Rheum. 2005;52:2625–36.
Singh JA, Saag KG, Bridges SL Jr, Akl EA, Bannuru RR, Sullivan MC, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26.
Dhir V, Sandhu A, Kaur J, et al. Comparison of two different folic acid doses with methotrexate: a randomized controlled trial (FOLVARI Study). Arthritis Res Ther. 2015;17(1):156.
Wessels JA, de Vries-Bouwstra JK, Heijmans BT, Slagboom PE, Goekoop-Ruiterman YP, Allaart CF, et al. Efficacy and toxicity of methotrexate in early rheumatoid arthritis are associated with single-nucleotide polymorphisms in genes coding for folate pathway enzymes. Arthritis Rheum. 2006;54:1087–95.
Sánchez A, Mirabel JL, Barrenechea E, Eugui J, Puelles A, Castañeda A. Evaluation of an improved immunoturbidimetic assay for serum C-reactive protein on a COBAS INTEGRA 400 Analyzer. Clin Lab. 2002;48:313–7.
Knijff-Dutmer E, Drossaers-Bakker W, Verhoeven A, van der Sluijs Veer G, Boers M, van der Linden S, et al. Rheumatoid factor measured by fluoroimmunoassay: a responsive measure of rheumatoid arthritis disease activity that is associated with joint damage. Ann Rheum Dis. 2002;61:603–7.
Hsu SD, Tseng YT, Shrestha S, Lin YL, Khaleel A, Chou CH, et al. miRTarBase update 2014: an information resource for experimentally validated miRNA-target interactions. Nucleic Acids Res. 2014;42(Database issue):D78–85.
Kanehisa M, Goto S, Kawashima S, Okuno Y, Hattori M. The KEGG resource for deciphering the genome. Nucleic Acids Res. 2004;32(Database issue):D277–80.
Vlachos IS, Paraskevopoulou MD, Karagkouni D, Georgakilas G, Vergoulis T, Kanellos I, et al. DIANA-TarBase v7.0: indexing more than half a million experimentally supported miRNA:mRNA interactions. Nucleic Acids Res. 2015;43(Database issue):D153–9.
Vergoulis T, Kanellos I, Kostoulas N, Georgakilas G, Sellis T, Hatzigeorgiou A, et al. mirPub: a database for searching microRNA publications. Bioinformatics. 2015;31(9):1502–4.
Bhattacharya A, Cui Y. miR2GO: comparative functional analysis for microRNAs. Bioinformatics. 2015;31:2403–5.
Hamdy SI, Hiratsuka M, Narahara K, Endo N, El-Enany M, Moursi N, et al. Genotype and allele frequencies of TPMT, NAT2, GST, SULT1A1 and MDR-1 in the Egyptian population. Br J Clin Pharmacol. 2003;55:560–9.
Campbell NA. Biology. Menlo Park: Benjamin/Cummings Publishing Co; 1996.
El-Shal AS, Aly NM, Galil SM, Moustafa MA, Kandel WA. Association of microRNAs genes polymorphisms with rheumatoid arthritis in Egyptian female patients. Joint Bone Spine. 2013;80:626–31.
Li K, Tie H, Hu N, Chen H, Yin X, Peng C, et al. Association of two polymorphisms rs2910164 in miRNA-146a and rs3746444 in miRNA-499 with rheumatoid arthritis: a meta-analysis. Hum Immunol. 2014;75:602–8.
Li LJ, Gao LB, Lv ML, Dong W, Su XW, Liang WB, et al. Association between SNPs in pre-miRNA and risk of chronic obstructive pulmonary disease. Clin Biochem. 2011;44:813–6.
Zou M, Li D, Lv R, Zhou Y, Wang T, Liu J, et al. Association between two single nucleotide polymorphisms at corresponding microRNA and schizophrenia in a Chinese population. Mol Biol Rep. 2012;39:3385–91.
Xiang Y, Fan S, Cao J, Huang S, Zhang LP. Association of the microRNA-499 variants with susceptibility to hepatocellular carcinoma in a Chinese population. Mol Biol Rep. 2012;39:7019–23.
Jeon YJ, Choi YS, Rah H, Kim SY, Choi DH, Cha SH, et al. Association study of microRNA polymorphisms with risk of idiopathic recurrent spontaneous abortion in Korean women. Gene. 2012;494:168–73.
Zhang J, Yang B, Ying B, Li D, Shi Y, Song X, et al. Association of pre-microRNAs genetic variants with susceptibility in systemic lupus erythematosus. Mol Biol Rep. 2011;38:1463–8.
Wolters HH, Heistermann HP, Stöppeler S, Hierlemann H, Spiegel HU, Palmes D. A new technique for ureteral defect lesion reconstruction using an autologous vein graft and a biodegradable endoluminal stent. J Urol. 2010;184:1197–203.
Wang M, Ye Y, Qian H, Song Z, Jia X, Zhang Z, et al. Common genetic variants in pre-microRNAs are associated with risk of coal workers’ pneumoconiosis. J Hum Genet. 2010;55:13–7.
Su XW, Yang Y, Lv ML, Li LJ, Dong W, Miao-Liao, et al. Association between single-nucleotide polymorphisms in pre-miRNAs and the risk of asthma in a Chinese population. DNA Cell Biol. 2011;30:919–23.
Okubo M, Tahara T, Shibata T, Yamashita H, Nakamura M, Yoshioka D, et al. Association between common genetic variants in pre-microRNAs and gastric cancer risk in Japanese population. Helicobacter. 2010;15:524–31.
Jeon YJ, Kim SY, Rah H, Choi DH, Cha SH, Yoon TK, et al. Association of the miR-146a C > G, miR-149 T > C, miR-196a2 T > C, and miR-499 A > G polymorphisms with risk of spontaneously aborted fetuses. Am J Reprod Immunol. 2012;68:408–17.
Kiselev I, Bashinskaya V, Kulakova O, Baulina N, Popova E, Boyko A, et al. Variants of microRNA genes: gender-specific associations with multiple sclerosis risk and severity. Int J Mol Sci. 2015;16:20067–81.
Rindfleisch JA, Muller D. Diagnosis and management of rheumatoid arthritis. Am Fam Physician. 2005;72:1037–47.
Hu Z, Liang J, Wang Z, Tian T, Zhou X, Chen J, et al. Common genetic variants in pre-micro- sRNAs were associated with increased risk of breast cancer in Chinese women. Hum Mutat. 2009;30:79–84.
Hoffman AE, Zheng T, Yi C, Leaderer D, Weidhaas J, Slack F, et al. microRNA miR-196a-2 and breast cancer: a genetic and epigenetic association study and functional analysis. Cancer Res. 2009;69:5970–7.
Huang QQ, Pope RM. The role of toll-like receptors in rheumatoid arthritis. Curr Rheumatol Rep. 2009;11:357–64.
Paleolog EM. The vasculature in rheumatoid arthritis: cause or consequence? Int J Exp Pathol. 2009;90:249–61.
Heidari B. Rheumatoid arthritis: early diagnosis and treatment outcomes. Caspian J Intern Med. 2011;2:161–70.
Curtis JR, Beukelman T, Onofrei A, Cassell S, Greenberg JD, Kavanaugh A, et al. Elevated liver enzyme tests among patients with rheumatoid arthritis or psoriatic arthritis treated with methotrexate and/or leflunomide. Ann Rheum Dis. 2010;69:43–7.
Kiselev I, Bashinskaya V, Kulakova O, Baulina N, Popova E, Boyko A, et al. Variants of microRNA genes: gender-specific associations with multiple sclerosis risk and severity. Int J Mol Sci. 2015;16(8):20067–81.
Acknowledgments
The authors would like to thank the Oncology Diagnostic Unit, Suez Canal University, Egypt, for providing the facilities for pursuing the research work at the unit.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
Eman A. Toraih, Nesreen M. Ismail, Ahmed A. Toraih, Mohammad H. Hussein and Manal S. Fawzy declare that they have no competing interests.
Ethical approval and informed consent
All patients declared informed consent and the study was approved by the local Ethics Committee of the Faculty of Medicine, Suez Canal University (approval no. 2629).
Funding
No sources of funding were used for this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Toraih, E.A., Ismail, N.M., Toraih, A.A. et al. Precursor miR-499a Variant but not miR-196a2 is Associated with Rheumatoid Arthritis Susceptibility in an Egyptian Population. Mol Diagn Ther 20, 279–295 (2016). https://doi.org/10.1007/s40291-016-0194-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40291-016-0194-3