
Abstract
Background
The importance of muscular fitness (MF) in the performance of activities of daily living is unequivocal. Additionally, emerging evidence has shown MF can reduce cardiometabolic risk in children and adolescents.
Objectives
The purpose of this study was to examine and summarize the evidence regarding the relationship between MF phenotypes (i.e., maximum muscular strength/power, muscular endurance, and maximum muscular strength/power/endurance) and cardiometabolic variables (obesity, blood pressure, lipids, glucose homeostasis, inflammatory markers, and clustered cardiometabolic variables) in children and adolescents.
Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and was registered with PROSPERO, number CRD42020179273.
Data Sources
A systematic review was performed on five databases (PubMed, EMBASE, SciELO, Scopus, and Web of Knowledge) from database inception to May 2020, with complementary searches in reference lists.
Eligibility Criteria for Selecting Studies
Eligibility criteria included (1) a study sample of youth aged ≤ 19 years, (2) an assessment of MF with individual or clustered cardiometabolic variables derived from adjusted models (regardless of test/measurement adopted or direction of reported association), and (3) a report of the association between both, using observational studies. Only original articles published in peer-reviewed journals in English, Portuguese, and Spanish languages were considered. The quality of the included studies was assessed by using the National Heart, Lung, and Blood Institute checklist. The percentage of results reporting a statistically significant inverse association between each MF phenotype and cardiometabolic variables was calculated.
Results
Of the 23,686 articles initially identified, 96 were included (77 cross-sectional and 19 longitudinal), with data from children and adolescents from 35 countries. The score for the quality of evidence ranged from 0.33 to 0.92 (1.00 maximum). MF assessed by maximum muscular strength/power was inversely associated with lower obesity (64/113 total results (56.6%)) and reduction in clustered cardiometabolic risk (28/48 total results (58.3%)). When assessed by muscular endurance, an inverse association with obesity (30/44 total results (68.1%)) and cardiometabolic risk (5/8 total results (62.5%)) was identified. Most of the results for the relationship between MF phenotypes with blood pressure, lipids, glucose homeostasis, and inflammatory markers indicated a paucity of evidence for these interrelationships (percentage of results below 50.0%).
Conclusion
MF assessed by maximum muscular strength/power or muscular endurance is potentially associated with lower obesity and lower risk related to clustered cardiometabolic variables in children and adolescents. There is limited support for an inverse association between MF with blood pressure, lipids, glucose homeostasis biomarkers, and inflammatory markers in children and adolescents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Muscular fitness assessed by maximum muscular strength/power or muscular endurance is potentially associated with lower obesity in children and adolescents. When considering the assessment of maximum muscular strength/power, tests with lower limb demand (e.g., jumps), tests involving recruitment of upper limbs (e.g., handgrip strength) and results normalized for body mass, and/or a combination of tests that evaluate maximum muscular strength/power and results normalized for body mass have been shown to be more sensitive for this interrelation. |
Maximum muscular strength/power or muscular endurance are associated with a lower risk related to clustered cardiometabolic variables in children and adolescents, with no differences attributed to the muscular fitness tests/measurements adopted. |
The associations between muscular fitness and blood pressure, lipids, glucose homeostasis biomarkers, and inflammatory markers are inconsistent. |
1 Introduction
Cardiovascular disease (CVD) is the leading cause of death among adults globally [1], though the manifestations of the disease in children and adolescents are uncommon [2]. However, risk factors associated with the development of CVD begin during childhood and adolescence, and risk exposure can slowly progress towards disease [2]. Thus, the investigation and monitoring of traditional and emerging cardiometabolic disease risk variables have been routinely assessed in the clinic and primary prevention [3,4,5].
The importance of muscular fitness (i.e., incorporation of phenotypes of muscular strength, including maximum isometric and dynamic strength, muscular power, and muscular endurance) [6,7,8,9] in the performance of activities of daily living is unequivocal. Additionally, there is a growing body of evidence reporting an inverse association between muscular fitness with individual [10,11,12,13,14] and clustered cardiometabolic variables among children and adolescents [11, 13,14,15], suggesting that muscular fitness may have a mitigating effect on the development of CVD. However, the relationship between muscular fitness and cardiometabolic variables in children and adolescents is not clear, with results showing both an absence of association [16,17,18,19] and inverse associations [12, 20, 21].
The inconsistency in findings for associations between muscular fitness and cardiometabolic variables may result from the diversity of muscular fitness tests/measurements adopted by studies (e.g., evaluation of upper or lower limbs, static or moving, counter-resistance effort or use of own body) for assessing different phenotypes of muscular fitness (each one with different assessment procedures) [6, 7]. However, although tests/measurements for the assessment of muscular fitness may influence the result of the association with cardiometabolic risk indicators, there is no standardized assessment for muscular fitness in children and adolescents [22]. In addition, it is speculated that such conflicting results may also be related to the different strategies adopted by the studies to consider body size [23, 24]. This is because a portion of the studies normalized the results for body-related indexes, including body mass [10, 11, 16, 21, 25,26,27,28,29,30,31,32,33], body mass index (BMI) [28, 34], and fat-free mass [34], while others adopted absolute values [18,19,20, 35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75], muscular fitness scores obtained from the use of two or more tests (and different procedures for considering body size in each test adopted) [76,77,78,79] or mathematical models to create muscular fitness indexes uncorrelated with body mass [12, 13, 32, 66, 80, 81]. Finally, some studies described in the literature failed to control for important covariates directly associated with muscular fitness or/and cardiometabolic variables, such as age [16, 18, 39, 48, 61, 66, 82], sex [20, 28, 36, 38,39,40,41,42,43, 48, 50, 52, 56, 61, 66, 67, 77, 81,82,83,84,85,86], sexual maturation [11, 13, 18,19,20, 28, 34,35,36,37,38,39,40, 42, 45, 48,49,50,51,52, 54, 55, 57, 60, 62, 66, 77, 81,82,83, 86, 87], and physical activity [11, 13, 15, 17,18,19,20, 26, 27, 34,35,36,37,38, 41,42,43, 45, 50, 52, 54, 55, 60,61,62, 65, 66, 76, 77, 81,82,83,84, 86], which may have contributed to the divergent associations observed.
Existing reviews on this topic are available in the literature [6, 9, 88, 89], though they explored a limited number of cardiometabolic risk variables. Further, the impact or the heterogeneity of the results according to the tests/measurements adopted to assess muscular fitness across studies, or results described according to sex, were not considered [6, 9, 88, 89]. Furthermore, although adolescent boys have greater muscle mass and lower body fat compared to adolescent girls, aspects that can confound, or even mediate [77] the association between muscular fitness and cardiometabolic variables, the direction of these associations according to sex is not known [6, 9, 88, 89]. Additionally, the information compiled in the previously published reviews [6, 9, 88] was restricted to the extraction of results in which it was identified that muscular fitness was associated with better results for the investigated cardiometabolic variables, although the same studies had identified absence of association or even inverse association of muscular fitness with the cardiometabolic variable investigated depending on the investigated muscular fitness phenotype [13].
Thus, the aim of this systematic review was to examine the relationship between muscular fitness and cardiometabolic variables among children and adolescents, advancing previous reviews [6, 9, 88, 89], by comprehensively investigating the relationship between muscular fitness and several cardiometabolic risk variables, considering the heterogeneity of the results according to muscular fitness tests/measurements adopted.
2 Methods
2.1 Protocol and Registration
This systematic literature review was registered in the International Prospective Register of Systematic Reviews—PROSPERO (CRD42020179273) and described according to the items suggested by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses—PRISMA [90].
2.2 Eligibility Criteria
Eligible studies for this review included: (i) original articles in Portuguese, Spanish, or English; (ii) observational (cross-sectional, cohort, and case–control) studies; (iii) studies in which the result for the association between muscular fitness (i.e., maximum muscular strength, muscular endurance, and muscular power) and the indicator investigated was derived from adjusted models (i.e., adjusted for covariates); and (iv) studies that investigated muscular fitness (regardless of test/measurement adopted) and individual or clustered cardiometabolic variables in children and adolescents with no diseases or special clinical conditions (e.g., diabetes, kidney disease, HIV/AIDS) and age group and/or mean age ≤ 19 years [91]. The selection of the descriptors regarding included cardiometabolic variables was based on guidelines/studies described in the literature [3,4,5]. Based on this information, studies that investigated the relationship between muscular fitness with obesity indicators, blood pressure, lipids, glucose homeostasis biomarkers, and inflammatory markers were included. Studies that investigated the relationship between muscular fitness and clusters of cardiometabolic variables (i.e., two or more variables grouped) were also included in this review. Published peer-reviewed original manuscripts and in-press manuscripts were eligible for inclusion. Grey literature and conference abstracts were excluded.
2.3 Information Sources
The systematic search for potential articles for this review took place during May 2020 using five electronic databases: PubMed, EMBASE, SciELO, Scopus, and Web of Knowledge.
2.4 Search
Systematic searches were adjusted and applied to all databases based on the method elaborated for PubMed, combining different terms for muscular fitness, cardiometabolic variables, and children and adolescents. A variety of descriptors related to each of these terms was entered into each database. Further information regarding the systematic search (descriptors used, search strategy for each database and number of papers captured) can be accessed in Electronic Supplementary Material (ESM) File 1. There was no restriction on the period of publication of original articles. Manual searches were conducted in the reference lists of the included studies and in review articles in which themes similar to that investigated in this review were analyzed. Additionally, experts in the field were contacted for additional studies.
2.5 Study Selection
The procedures for searching and evaluating titles, abstracts, and full-text articles, as well as assessing the risk of bias, were completed independently by two researchers (TRL and PCM), with guidance from a senior researcher (DASS), who in addition to supervising the information-gathering process, established consensus and assisted in resolving any disputes.
2.6 Data Collection Process and Data Items
Descriptive and methodological information and results for the relationship between muscular fitness and the outcomes investigated in each study were extracted. It is necessary to emphasize the absence of a test/reference instrument to assess muscular fitness phenotypes [92]. This is because the manifestations of muscular strength encompassed by muscular fitness can manifest in a number of different ways [93], which implies different ways of measuring. Thus, in view of the use of multiple measures to assess muscular fitness (small or large muscle groups, upper or lower limbs, with the need to support or move the body, or the substantial covariance between the results identified in the measurements with parameters related to body composition) [23], results for the associations investigated in the studies were presented considering such specificities. Thus, the summarized information was described as: (i) evidence derived from studies where absolute muscular fitness was adopted in the analyses (absence of a strategy to consider parameters of the body size in the expression of muscular fitness results); (ii) evidence from studies where normalized muscular fitness was adopted in the analyses (adoption of strategy to consider body-related indexes in the expression of muscular fitness, e.g., body mass) or; (iii) evidence from studies where absolute/normalized muscular fitness (adoption of both absolute and normalized strategy, e.g., results of absolute muscular fitness from one test, and results of normalized muscular fitness from another test—used to create a composite muscular fitness score. To complement the summarized information, the results were also presented as follows: (i) absolute or normalized values for measurements of maximum muscular strength/power according to tests involving upper or lower limbs; (ii) absolute or normalized values for measurements of muscular endurance according to the need or not of support of the body itself; (iii) absolute, normalized, or absolute/normalized values for measurements of composite muscular fitness score (two or more tests/measurements) according to tests involving the evaluation of the phenotypes maximum muscular strength/power, muscular endurance, or a combination of the two described muscular fitness phenotypes—maximum muscular strength/power/endurance (e.g., muscular fitness score derived from the adoption of one test that measured maximum muscular strength/power and another test that assessed muscular endurance).
To provide further investigation regarding the quality of the evidence of the information included, all results analyzed in this review were also described according to the design (reverse-causation bias), participation rate (selection bias—internal validity), and control for confounding variables (i.e., variables that can influence both the outcome and the exposure—confounding bias). Regarding the calculation of participation rate, although a range of definition has been suggested [94, 95], which can cause disagreements when comparing different studies [96], in the present study, participation rate was defined as the number of respondents who have provided a usable response divided by the total number of initial personal invitations requesting participation [95, 96]—to provide results as a percentage (%), the final value was multiplied by 100. Regarding the control of analyses for confounding variables, although there is no consensus regarding the determining variables for the interrelation between muscular fitness and cardiometabolic variables in children and adolescents, or the number of variables needed to be inserted in the adjusted models in order to reduce confounding factors, it is necessary to somehow consider the appropriate control for confounding variables. The available evidence indicated that information related to age, sex, sexual maturation, and body size (e.g., body mass, height, fat mass, fat-free mass) is relevant in this context [24, 93, 97]. Likewise, the performance of physical activity and systematic bodily activities (e.g., engagement in sports practices—especially those in which counter-resistance efforts are necessary) was directly associated with muscular fitness [98]. Thus, results according to the number of confounding variables (0, 1, 2, ≥ 3) considered relevant (i.e., age, sex, sexual maturation, body size, and physical activity) for the association between muscular fitness and cardiometabolic variables inserted as control in the adjusted analyses were also considered in the summary of information.
Based on the summarized results regarding the relationship between muscular fitness and the investigated cardiometabolic variable of the included studies, a global percentage score for the relationship between muscular fitness and the investigated cardiometabolic variables was calculated [(number of results indicating an inverse relationship between muscular fitness and the investigated cardiometabolic variable/number of results for the relationship investigated) × 100]. For example, in the relationship between muscular fitness (assessed by maximum muscular strength/power measurements) and obesity indicators, if the study found a result indicating that higher levels of muscular fitness were associated with lower values for the investigated obesity indicator, that result was considered an inverse association.
After the data were extracted in spreadsheets designed specifically for the review, the outcome variable(s) of each study were classified based on available evidence [3,4,5] and grouped into six broad categories: (i) general (BMI) and central obesity (waist circumference, WC) indicators; (ii) blood pressure (hypertension/high blood pressure, mean arterial pressure, systolic and diastolic blood pressure); (iii) lipids (total cholesterol, HDL-cholesterol, triglycerides, HDL-cholesterol/total cholesterol ratio, total cholesterol/HDL-cholesterol ratio, [(Triglycerides) – (HDL-cholesterol)]/2, triglycerides/HDL-cholesterol ratio, non-HDL-cholesterol, atherogenic index of plasma); (iv) glucose homeostasis biomarkers [2-h glucose, fasting blood glucose, insulin, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), Homeostatic Model Assessment of B-cell function (HOMA-B), quantitative insulinsensitivity check index (QUICKI), glycated hemoglobin (HbA1c)]; (v) inflammatory markers [C-reactive protein (CRP), complement factor C3, complement factor C4, ceruplasmin, adiponectin, leptin, white blood cells, interleukin-6 (IL-6), tumor necrosis factor alpha (TNF-α)]; and (vi) clustered cardiometabolic variables.
2.7 Risk of Bias in Individual Studies
Quality appraisal was based on the National Heart, Lung, and Blood Institute checklist for observational cohort/cross-sectional studies [99]. This instrument is based on the evaluation of 14 items that comprise methodological aspects according to the design of the study. For cross-sectional studies, items 7 (“Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?”) and 13 (“Was loss to follow-up after baseline 20% or less?”) were recorded as not applicable. With regard to exposure measures and assessment (item 9), muscular fitness tests/measurements obtained from physical test batteries and/or validated for the population (children and adolescents) were considered valid and reliable measures [22]. Regarding outcome measures (item 11), measured and non-self-reported information for anthropometric indicators of obesity, blood pressure levels, and blood (lipids, glucose homeostasis biomarkers, inflammatory markers) were considered valid and reliable measures. Adjustment for confounding (item 14) was considered sufficient if studies adjusted for at least three relevant variables for the interrelationship between muscular fitness and cardiometabolic variables in children and adolescents (i.e., age, sex, sexual maturation, body size, and physical activity) [24, 93, 97, 98]. For each criterion, a score of + 1 is assigned when the answer is positive (yes), while a score of zero (0) is assigned otherwise (that is, a "no," "not applicable," "answer not reported," or "cannot be determined”). The specific global score of the study ranges from zero to 14 and a quality score is determined by: number of questions with positive score “+ 1”/number of questions with a score of zero “0” (ESM File 2). Thus, scores ranging from 0.0 (low methodological quality/high risk of bias) to 1.0 (high methodological quality/low risk of bias) could be assigned to the articles inserted/analyzed in this review. For cases of disagreement between the two researchers assigned to assess the risk of bias (TRL & PCM), a third researcher (DASS) with experience in this type of study was consulted through a consensus meeting.
2.8 Synthesis of Results
Meta-analyses were planned if data could be meaningfully pooled (i.e., if sufficiently homogeneous in terms of statistical, clinical, and methodological characteristics). Narrative syntheses structured around the results for the association between muscular fitness phenotypes (e.g., maximum muscular strength/power, muscular endurance, combination of maximum muscular strength/power/endurance phenotypes) and the cardiometabolic variables were conducted if meta-analyses were not possible.
3 Results
3.1 Overview of Studies
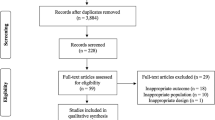
After systematic search of articles in the databases, exclusion of duplicate information, application of inclusion and exclusion criteria, and incorporation of additional articles (after additional readings – references of included studies) 96 articles were included (Fig. 1).

Results of database searches and criteria used in the selection of studies included to identify the relationship between muscular fitness and cardiometabolic variables among children and adolescents
The studies included in this review gathered information from children and adolescents from 35 countries. Of this total, 77 were cross-sectional [20, 25,26,27,28,29,30,31, 33, 37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64, 67,68,69,70,71,72,73,74,75,76,77,78,79, 81,82,83,84,85,86,87, 100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118] and 19 were longitudinal [10,11,12,13,14,15,16, 18, 19, 21, 32, 34,35,36, 65, 66, 80, 119, 120]. With regard to the quality of the longitudinal information investigated, in 63.1% of the studies [10, 11, 14, 15, 18, 19, 34,35,36, 66, 119, 120] the baseline value of the analyzed outcome was added to the adjusted models when investigating the possible effect attributed to the exposure variable on the outcome longitudinally. Of the total number of studies included, in 22 [21, 27, 29, 30, 36,37,38, 41, 46, 50, 51, 53, 57, 60, 62, 65, 72, 79, 81, 82, 105, 118] the described frequency rate (or calculated based on the information available in these studies) was ≥ 80.0%. Additionally, a frequency rate ≥ 50.0% was verified/calculated in ten studies [12, 16, 18, 40, 61, 79, 87, 102, 116, 120], while in another 31 studies [10, 11, 13,14,15, 19, 26, 32, 33, 35, 39, 66, 67, 74,75,76, 78, 80, 84, 85, 101, 103, 104, 107, 108, 110, 111, 114, 115, 117, 119] such values were less than 50.0%. It is noteworthy that in 33 studies [20, 25, 28, 31, 34, 42,43,44,45, 47,48,49, 52, 54,55,56, 58, 59, 63, 64, 68,69,70,71, 73, 77, 83, 86, 100, 106, 109, 112, 113], values referring to frequency rate were not described or the information necessary for the calculation of this indicator was not available. With regard to the number of participants included in the studies, only three trials [37, 47, 62] (which supported the results of the interrelationship of muscular fitness and obesity) were conducted with a sample of less than 100 evaluated. In addition, in approximately 50% of the studies (n = 45) [10, 11, 13, 15, 19, 26, 27, 30,31,32,33,34, 49, 51, 56, 57, 65, 67, 68, 70,71,72,73,74,75,76, 78,79,80, 87, 100, 102,103,104,105,106,107, 109, 110, 113, 115, 116, 119, 120] a high number of variables likely to confound the interrelationship of muscular fitness and cardiometabolic variables were considered in the analysis models (≥ 3 variables). Further details regarding the characteristics, muscular fitness tests/measurements and adjustment variables adopted by the included studies in this review are available in ESM Tables S1–S3.
3.2 Risk of Bias
The methodological quality assessment of each of the included studies in this review can be accessed in ESM Table S4. Briefly, values for the methodological quality/risk of bias score ranged from 0.67 to 0.92 for longitudinal studies and from 0.33 to 0.82 for cross-sectional studies.
3.3 Association Between Muscular Fitness and Investigated Outcomes
3.3.1 Muscular Fitness and Obesity Indicators
3.3.1.1 Maximum Muscular Strength/Power and Obesity Indicators
The relationship between maximum muscular strength/power and obesity indicators (BMI and WC) has been investigated in 43 studies; seven studies with a longitudinal design [11, 15, 18, 19, 34, 65, 66] and 36 studies with a cross-sectional design [20, 25,26,27,28, 37,38,39,40,41, 44, 45, 47, 48, 51, 52, 54,55,56,57,58,59,60,61,62,63,64, 67, 76, 77, 81,82,83,84, 86, 87] (ESM Table S5). Considering all the information available in the studies (Table 1, ESM Tables 6 and 7), 56.6% of the evidence indicated that maximum muscular strength/power was inversely associated with obesity indicators in children and adolescents. In this context, tests where maximum muscular strength/power was evaluated by jumps (78.1%; 34/43 results), upper limbs and values normalized for body-related indexes (93.7%; 15/16 results) and/or a combination of tests that evaluated maximum muscular strength/power and results normalized for body related indexes (88.9%; 8/9 results) presented a greater number of results indicating an inverse relationship of maximum muscular strength/power with obesity indicators. However, it is necessary to highlight that evidence from 19 studies, 28.7% of the evidence [20, 34, 37, 40, 41, 44, 51, 52, 54, 56, 57, 60, 61, 63, 64, 66, 83, 86, 87], identified a direct relationship between muscular fitness and obesity indicators (32.1%—BMI; 19.3%—WC). Such associations were predominantly identified when maximum muscular strength/power was measured by handgrip strength, or tests in which body-related indexes were not considered in determining the results obtained. When muscular fitness was normalized for body size, no direct association with obesity was identified. Additional information for the association between maximum muscular strength/power and obesity indicators is available in the ESM (Tables S8–S11).
3.3.1.2 Muscular Endurance and Obesity Indicators
The evidence available in the literature regarding the association of muscular endurance and obesity indicators is based on two longitudinal studies [35, 36] and 19 cross-sectional studies [25, 37,38,39, 41,42,43, 46, 48,49,50, 53, 55, 58, 61, 64, 82, 83, 87] (ESM Table S5). Of the total information analyzed (ESM Tables S6 and S7), 68.1% of the evidence indicated that muscular endurance was inversely associated with obesity indicators (Table 2). In addition, similar results regarding the inverse relationship between muscular endurance and obesity indicators were verified for boys (61.5%) and girls (64.3%) (Table 1). With regard to each obesity indicator investigated, although tests requiring body support (e.g., pull-ups, push-ups) have generally been inversely associated with BMI, longitudinal evidence consistently indicated no association for this interrelationship (muscular endurance and BMI) [35, 36]. Additionally, regardless of how muscular fitness was measured (e.g., sit-ups, curl-ups, push-ups), muscular endurance was inversely associated with WC (evidence derived exclusively from cross-sectional studies [25, 53, 61]). Detailed information regarding the association between muscular endurance and obesity indicators according to design and tests/measurements can be found in ESM Tables S8–S11.
3.3.1.3 Maximum Muscular Strength/Power/Endurance and Obesity Indicators
The longitudinal evidence for the association between the combination of maximum muscular strength/power/endurance phenotypes and obesity [13] (ESM Table S5) indicated that higher values of the score derived from assessments of maximum muscular strength/power/endurance phenotypes was inversely associated with obesity (1/1 results; Table 3 and ESM Table S7). General and specific information for this association is available in ESM Tables S9 and S11.
3.3.2 Muscular Fitness and Blood Pressure
3.3.2.1 Maximum Muscular Strength/Power and Blood Pressure
The relationship between maximum muscular strength/power and blood pressure (hypertension, high blood pressure, mean arterial pressure, systolic and diastolic blood pressure) was investigated in 23 studies, ten with a longitudinal design [11,12,13,14,15,16, 19, 21, 65, 120] and 13 with a cross-sectional design [25, 26, 30, 31, 61, 68,69,70,71, 76, 77, 82, 84] (ESM Table S5). In view of the results described in each investigated study (Table 1, ESM Tables S6 and S7), the overall percentage of results for the inverse association between maximum muscular strength/power and blood pressure was 25.7%. When considering sex in this interrelationship, the percentage for the inverse association among boys was 13.3% and among girls was 35.7% (Table 1). Additionally, 16.7% of the evidence (derived from seven studies [12, 21, 26, 29, 65, 70, 71]), indicated that maximum muscular strength/power was directly associated with blood pressure. Such results were mostly identified when absolute muscular fitness values were analyzed [12, 65, 70, 71]. Detailed information according to the study design and tests/measurements adopted by the studies are available in ESM Tables S12–S19.
3.3.2.2 Muscular Endurance and Blood Pressure
Evidence regarding the association between muscular endurance and blood pressure derived from one longitudinal study [12] and four cross-sectional studies [25, 29, 61, 82] (ESM Table S5). None of the evidence available in the literature and analyzed in this review (Table 2, ESM Tables S6 and S7) reported an inverse association between muscular endurance and blood pressure (including longitudinal and cross-sectional evidence). Lack of statistical significance [12, 25, 61, 82] and direct association [12] were identified for 90.0% (9/10 results) and 10.0% (1/10 results) of the evidence, respectively. Additional information for the interrelationship between muscular endurance and blood pressure can be found in ESM Tables S15–S19.
3.3.2.3 Maximum Muscular Strength/Power/Endurance and Blood Pressure
The results for the relationship between the combination of maximum muscular strength/power/endurance phenotypes and blood pressure derived from one longitudinal study [13] (ESM Tables S5, S14, and S15), the results of which indicated a global percentage for the inverse association of 50.0% (Table 3, ESM Tables S7, S18, and S19).
3.3.3 Muscular Fitness and Lipids
3.3.3.1 Maximum Muscular Strength/Power and Lipids
Information from 15 studies described in the literature—six longitudinal [11, 12, 14,15,16, 19] and nine cross-sectional [25,26,27, 30, 61, 69, 77, 82, 84]—underpin the relationship between maximum muscular strength/power and lipids in children and adolescents (ESM Table S5). In view of the results described according to the tests/measurements for muscular fitness (ESM Tables S6 and S7), the global percentage for the inverse relationship between maximum muscular strength/power and lipids was 25.4% (Table 1). Additionally, the global percentage for the inverse association among boys was 35.3%, whereas among girls the percentage was 23.5% (Table 1). It is noteworthy that the results for this inverse interrelationship (considering all analyzed results, or according to sex) were consistent regardless of the lipid analyzed, test adopted to assess maximum muscular strength/power, or whether the results were normalized for body size or not. Detailed information regarding the relationship between maximum muscular strength/power and lipids is available in ESM Tables S20–S37.
3.3.3.2 Muscular Endurance and Lipids
One longitudinal study [12] and four cross-sectional studies [25, 61, 82, 115] referring to the association between muscular endurance and lipid markers have been identified in the literature (ESM Table S5). Based on the results synthesized according to the tests/measurements (ESM Tables S6 and S7), the global percentage for the inverse relationship between muscular endurance and lipids was 38.5%. When considering sex, the percentage identified for boys was 66.7%. For girls, this percentage was 0.0% (Table 2). Results for the association between muscular endurance and individual lipid indicators, according to the design and tests/measurements are available in ESM Tables S20–S37.
3.3.3.3 Maximum Muscular Strength/Power/Endurance and Lipids
The evidence supporting the relationship between the combination of maximum muscular strength/power/endurance phenotypes and lipids in children and adolescents was derived from one longitudinal study [13] (ESM Table S5). Based on the summary of results (ESM Table S7), the global percentage for the inverse relationship for this association was 100.0% (2/2 results, Table 3).
3.3.4 Muscular Fitness and Glucose Homeostasis Biomarkers
3.3.4.1 Maximum Muscular Strength/Power and Glucose Homeostasis Biomarkers
Eight longitudinal studies [10,11,12, 14, 15, 19, 32, 80] and ten cross-sectional studies [26, 30, 61, 72, 77, 78, 82, 84, 100, 104] investigated the relationship between maximum muscular strength/power and glucose homeostasis biomarkers in children and adolescents (ESM Table S5). According to the summarized findings (ESM Tables S6 and S7), the global percentage for the inverse relationship between maximum muscular strength/power and glucose homeostasis biomarkers was 31.6% (Table 1). Additionally, 67.1% of the evidence indicated an absence of association, while one study (1.3% of the evidence analyzed) [32] identified that maximum muscular strength/power (assessed by lower limb test—standing long jump) was directly associated with glucose homeostasis biomarkers (fasting blood glucose). The calculated percentages for the inverse relationship between maximum muscular strength/power and glucose homeostasis biomarkers according to sex were 33.3% for boys and 16.7% for girls. Additional information for this interrelation can be found in ESM Tables S38–S51.
3.3.4.2 Muscular Endurance and Glucose Homeostasis Biomarkers
The relationship between muscular endurance and glucose homeostasis biomarkers has been investigated in four studies; two studies with a longitudinal design [12, 80] and two studies with a cross-sectional design [61, 82] (ESM Table S5). Considering general (ESM Tables S38–S51) and specific information (ESM Tables S6 and S7), the global percentage for the inverse association between muscular endurance and glucose homeostasis biomarkers was 40.0%—4/10 results (Table 2). Regarding the summary of evidence according to the evaluated glucose homeostasis biomarker, consistent results (100.0%) pointed to an inverse association between muscular endurance (assessed by push-up or trunk extension) with insulin, HOMA-IR and HOMA-B [12, 80].
3.3.5 Muscular Fitness and Inflammatory Markers
3.3.5.1 Maximum Muscular Strength/Power and Inflammatory Markers
One longitudinal study [12] and 11 cross-sectional studies [30, 61, 73,74,75, 79, 103, 105, 107, 113, 118] investigated the relationship between maximum muscular strength/power and inflammatory markers in children and adolescents (ESM Table S5). In view of the general (ESM Tables S52–S60) and specific results (ESM Tables S61–S69), in addition to the evidence analyzed according to tests adopted by the studies (ESM Tables S6 and S7), the global percentage for the inverse relationship between maximum muscular strength/power and inflammatory markers was 47.2% (Table 1). Although less than half of the evidence analyzed identified an inverse association between maximum muscular strength/power and inflammatory markers, results according to each inflammatory marker analyzed indicated that muscular fitness (maximum muscular strength/power) was consistently inversely associated with leptin (100.0% – 5/5 results) [75, 79, 103, 105, 113], regardless of the test used to assess muscular fitness or strategy adopted to consider body size (absolute or normalized results). Furthermore, in 55.5% of the evidence, maximum muscular strength/power was inversely associated with CRP [12, 30, 73, 74, 113].
3.3.5.2 Muscular Endurance and Inflammatory Markers
The results described in this review regarding the interrelationship between muscular endurance and inflammatory markers derived children and adolescents. Of the from three studies; one study with longitudinal design [12] and two cross-sectional studies [61, 118] (ESM Table S5). According to the results summarized—essentially derived from studies investigating the association between muscular endurance and CRP (ESM Tables S6 and S7; Supplementary Tables S52–S69), the percentage for the inverse relationship between muscular endurance and inflammatory markers was 50.0% (2/4 results) (Table 2).
3.3.5.3 Maximum Muscular Strength/Power/Endurance and Inflammatory Markers
Two cross-sectional studies [79, 105] that reported results for the association between the combination of maximum muscular strength/power/endurance phenotypes and inflammatory markers were included in this review (ESM Table S5). Based on the results described by the studies (ESM Tables S6 and S7, and S52–S69), the percentage for the inverse relationship between the combination of maximum muscular strength/power/endurance phenotypes and inflammatory markers was 100.0% (3/3 results—Table 3). These results were verified regardless of the inclusion or not of body size as an adjustment in the expression of muscular fitness values.
3.3.6 Muscular Fitness and Clustered Cardiometabolic Variables
3.3.6.1 Maximum Muscular Strength/Power and Clustered Cardiometabolic Variables
According to the findings described in the literature, 24 studies aimed to investigate the relationship between maximum muscular strength/power and clustered cardiometabolic variables in children and adolescents. Of the total number of studies, seven were longitudinal [11, 13,14,15,16, 19, 119] and 17 were cross-sectional [25, 26, 30, 33, 75, 77, 82, 84, 85, 102, 106, 108, 110,111,112,113,114] (ESM Table S5). Based on the evidence summarized in this review (ESM Tables S6 and S7) and available in Table 1, the percentage for the inverse relationship between maximum muscular strength/power and clustered cardiometabolic variables in children and adolescents was 58.3%. When considering the results according to sex, the overall percentage for the inverse association between boys was 45.4%, while for girls a percentage of 54.5% was identified. It is noteworthy that the results obtained by normalized handgrip strength [14, 15, 26, 30, 33, 82, 84, 85, 108, 110, 111, 113] indicated a percentage for the inverse association between maximum muscular strength/power and clustered cardiometabolic variables of 78.2%, suggesting that this test/procedure may be superior to the others when investigating the relationship between muscular fitness (maximum muscular strength/power) and clustered cardiometabolic variables in children and adolescents. Detailed information for the described results can be found in ESM Tables S70 and S71.
3.3.6.2 Muscular Endurance and Clustered Cardiometabolic Variables
One longitudinal study [13] and six cross-sectional studies [25, 43, 82, 109, 116, 117] that investigated the relationship between muscular endurance and clustered cardiometabolic variables in children and adolescents were identified in the literature and included in this review (ESM Table S5). Based on the analyzed (ESM Tables S70 and S71) and summarized (ESM Tables S6 and S7) results, the global percentage for the inverse relationship between muscular endurance and clustered cardiometabolic variables in children and adolescents was 62.5%—although the only longitudinal study analyzed [13] reported no significant association for this interrelationship (push-up and clustered cardiometabolic variables) (Table 2, ESM Tables S70 and S71).
3.3.6.3 Maximum Muscular Strength/Power/Endurance and Clustered Cardiometabolic Variables
Three studies evaluated the relationship between the combination of maximum muscular strength/power/endurance phenotypes and clustered cardiometabolic variables; one longitudinal study [13] and two cross-sectional studies [79, 101] (ESM Table S5). Finally, according to the results analyzed (ESM Tables S6, S7, S70, and S71), the global percentage for the inverse relationship between the combination of maximum muscular strength/power/endurance and clustered cardiometabolic variables in children and adolescents was 50.0% (Table 3).
4 Discussion
This systematic review synthesized evidence from 96 studies of which the objective was to verify the association between muscular fitness and cardiometabolic variables in children and adolescents. The included studies mainly consisted of cross-sectional (79.8%) studies that involved participants from 35 countries. This systematic review showed that maximum muscular strength/power and muscular endurance phenotypes were inversely associated with obesity indicators and clustered cardiometabolic variables among children and adolescents.
This study found that muscular fitness investigated by maximum muscular strength/power was associated with lower obesity indicators in 56.6% of the evidence, whereas when investigated by muscular endurance, the calculated percentage was 68.1%. However, it is necessary to emphasize that important factors, such as age [16, 18, 39, 48, 61, 66, 82], sex [20, 28, 36, 38,39,40,41,42,43, 48, 50, 52, 56, 61, 66, 67, 77, 81,82,83,84,85,86], sexual maturation [11, 13, 18,19,20, 28, 34,35,36,37,38,39,40, 42, 45, 48,49,50,51,52, 54, 55, 57, 60, 62, 66, 77, 81,82,83, 86, 87], body size [11, 15, 17, 18, 20, 27, 28, 34,35,36,37,38,39,40,41, 43, 45, 48,49,50,51, 54,55,56, 60,61,62, 67, 76, 81, 83, 84, 86], physical activity [11, 13, 15, 17,18,19,20, 26, 27, 34,35,36,37,38, 41,42,43, 45, 50, 52, 54, 55, 60,61,62, 65, 66, 76, 77, 81,82,83,84, 86], or cardiorespiratory fitness [17,18,19,20, 26,27,28, 34,35,36,37,38,39,40,41,42,43, 45, 48, 50,51,52, 54,55,56,57, 60,61,62, 65, 67, 76, 77, 81, 83, 84, 86, 87] were not considered by the studies, which may have contributed to an overestimation of significant results. When considering the results according to the study design, the body of evidence from longitudinal studies suggested a low (maximum muscular strength/power) or even no association (muscular endurance) of muscular fitness with these indicators (BMI and WC). Regarding the assessment of maximum muscular strength/power, lower limb tests (e.g., jumps), tests involving recruitment of upper limbs (e.g., handgrip strength) and results normalized for body mass, and/or a combination of tests that evaluate maximum strength/power and results obtained normalized for body mass have been shown to be more sensitive tests/measurements to identify associations with obesity (although identifying an association is not always positive if the association is not causal). Although body mass (body-related index predominantly adopted by the included studies to consider body size) is a determinant for muscular fitness, this interrelation can be mediated by other body-related indexes, such as body fat [121]. Thus, the adoption of techniques that consider the effect of body fat/body size, such as the use of maximum muscular strength/power tests evaluated by jumps, or the normalization (or standard ratio) of results by body mass appear to be appropriate strategies to investigate the interrelationship between maximum muscular strength/power and obesity indicators. However, it is worth noting that in addition to impacting muscular fitness levels, body fat is directly related to adverse prognoses in relation to cardiometabolic variables [122], where the hypothesis that muscular fitness may be a mediator in the relationship between adiposity with these variables cannot be ruled out (especially in subgroups with high body fat) [77]. While considering body mass as a strategy for reducing differences in the mass of non-skeletal muscle tissues (such as fat, organ, and bone) can be a good strategy, it also introduces statistical problems since muscle mass is part of both the numerator and denominator (i.e., muscle mass is a fraction of body mass) [123, 124]. Additionally, when considering adding body mass in the expression of results, it must be understood that the level of body adiposity can negatively influence this interrelation, since the ratio of muscular fitness to body mass will decrease as the fat percentage increases [124]. Thus, considering the existing limitations when normalizing muscular fitness for body mass, the adoption of additional strategies such as the use of muscular fitness indexes not correlated with body mass, generated from the use of residuals derived from regression analysis (including absolute values of muscular fitness as outcome and body mass as exposure variable) [13, 32, 66, 80, 81], or adoption of allometric parameters [15, 25, 65], was described, suggesting other possibilities for considering body size when determining muscular fitness values in children and adolescents. Also, based on the premise that adolescence is a period of changes in body structures [125], and that muscle mass plays an important role in maintenance of growth development [126], it is speculated that the expression of the values of muscular fitness according to height allows inclusion of such development in the structure and body composition, and that the use of this technique can result in more reliable muscular fitness values. Such an assumption is based on the fact that an increase in fat-free mass throughout puberty occurs similarly to an increase in height—at least in the shape of the growth curve [126]. Finally, given that the magnitude of the relationship between muscular fitness and body size tends to grow concomitantly with the increase in body dimensions—possibly due to the increase in muscular cross-sectional area (proportional to height and body mass) [23]— consideration of height and body mass simultaneously in the expression of muscular fitness values can contribute to the determination of muscular quality (rather than muscular quantity). Thus, in addition to the need for a greater body of evidence derived from longitudinal studies with rigorous control of confounding factors in order to confirm the results identified in this review, it is suggested that future studies should consider height, or height and body mass simultaneously, in the expression of muscular fitness values (especially when the goal is to investigate maximum muscular strength or muscular power), since it is possible that the identified associations and conclusions assumed by the studies vary depending on the inclusion or not of these parameters in the muscular fitness values.
Considering the results described in the literature and included in this review, which reported mostly an inverse association between maximum muscular strength/power and muscular endurance with clustered cardiometabolic variables regardless of the variables investigated or number of clustered indicators analyzed, these muscular fitness phenotypes were associated with better results related to clustered cardiometabolic variables. The plausibility for the aforementioned relationship has been related to the potential effect of muscular fitness in reducing the harmful health impact of each of the cardiometabolic variables when grouped [6, 9, 88]. However, findings described in this present systematic review indicated that maximum muscular strength/power and muscular endurance was associated with lower values of some specific cardiometabolic variables and not for all of these variables, suggesting additional aspects are involved in this association. It is noteworthy that although the results for the inverse association between maximum muscular strength/power and clustered cardiometabolic variables are based on a large number of longitudinal and cross-sectional evidence, the same is not true for muscular endurance, which is based on cross-sectional studies [25, 43, 82, 109, 116, 117] and one single longitudinal study [13], of which the result differs from those summarized by cross-sectional evidence. With regard to this single longitudinal study [13], the hypothesis raised by the authors to justify the absence of association would be related to a minor role of muscular endurance in children and adolescents on clustered cardiometabolic variables, or the possible greater measurement error of tests for muscular endurance compared to tests for maximum muscular strength/power [22]. Thus, although the synthesis of evidence (regardless of design) points to an inverse association between muscular fitness and clustered cardiometabolic variables, longitudinal evidence for the interrelationship of muscular endurance/clustered cardiometabolic variables is needed to confirm the identified findings.
Due to the small amount of evidence (≥ 50.0%) that identified that muscular fitness was associated with lower blood pressure, lipids, glucose homeostasis biomarkers, and inflammatory markers, the adoption of muscular fitness as a marker for these cardiometabolic indicators is still largely unknown. The aforementioned absence of an association occurred independently of the muscular fitness phenotypes or tests/measurements adopted. It is noteworthy that the direction of evidence derived from longitudinal and cross-sectional studies was similar with regard to the lack of association of muscular fitness (measured by maximum muscular strength/power or muscular endurance) with blood pressure and blood variables, although a very small amount of information regarding the relationship between muscular endurance with blood pressure, lipids, glucose homeostasis, biomarkers, and inflammatory markers has been derived from longitudinal studies [12, 80], or from studies in which multiple confounding factors likely to change the direction of associations have been considered (including age, sex, sexual maturation, body size, or physical activity) [80, 115, 118]. Greater muscular fitness and muscle mass are both associated with better vascular and endothelial function, lower central arterial stiffness [127, 128], prevention of abnormalities attributed to lipids [124], and glucose homeostasis control in children and adolescents [124]. Regarding the relationship between muscular fitness and inflammatory markers, it has been linked to improved insulin sensitivity by muscles and a reduction of the adverse impact attributed to body fat (seen in individuals with higher levels of muscular fitness), which contributes to the reduction/attenuation of inflammatory substances [75, 121, 129, 130]. However, it is hypothesized that the underlying hormonal effect in these interrelationships may moderate the magnitude of the associations [124, 131, 132]. Thus, it is possible that the lack of consideration of the effect of sexual maturation by a significant portion of the studies analyzed [10,11,12,13,14,15,16, 19, 25, 29, 31, 32, 65, 68, 72, 77, 80, 82, 115] may have contributed to the lack of common direction for the results reported. Another aspect that could justify the inconsistent results is related to the adoption of strategies to consider body size in the obtained muscular fitness values [11, 13, 14, 16, 25, 26, 30, 33, 75, 77, 79, 82, 84, 85, 102, 108, 110, 111, 113, 114, 119].
Results for the relationship between muscular fitness – investigated by the combination of maximum muscular strength/power/endurance phenotypes (evaluated by different tests, of which the resulting values were aggregated and used as a muscular fitness score) – and cardiometabolic variables in children and adolescents were also extracted from the identified studies [13, 79, 101, 105]. Evidence from these studies indicated that the combination of maximum muscular strength/power/endurance phenotypes was inversely related to obesity indicators, lipids, and inflammatory markers. However, caveats must be considered for the reported results, including the fact that only one longitudinal study [13] was responsible for all the evidence for the association between maximum muscular strength/power/endurance phenotypes with obesity, blood pressure, and lipids. Thus, considering the absence of longitudinal evidence for the interrelationship between maximum strength/power/endurance phenotypes and inflammatory markers, and the small number of studies for which confounding factors have been adequately controlled, a larger body of evidence to confirm the direction of these associations is needed.
Although muscular fitness is determined to a large extent by genetic factors (30.0–95.0% of the variability, according to the type of contraction, contraction speed, or test/predominant muscle group evaluated) [133, 134], the rest of the variability arises from behavioral factors, with physical activity being the main modifiable component associated with muscular fitness [92]. This issue is especially important to address, considering that in addition to directly impacting muscular fitness (especially vigorous physical activity or participation in sports) [98], physical activity has been directly associated with better prognosis regarding cardiometabolic variables in adolescents [135]. Another variable known to be associated with muscular fitness and inversely associated with cardiometabolic risk factors [10, 102] in children and adolescents, is cardiorespiratory fitness. The relationship between these health-related physical fitness components seems to be even more relevant considering that although the mechanisms responsible for the inverse association with cardiometabolic variables are different depending on the physical fitness component [121, 136], some improvements are partially mediated by similar pathways, including the reduction of visceral adipose tissue [67] and improved insulin sensitivity [10]. In this sense, although studies have identified an association of muscular fitness with cardiometabolic variables in young people regardless of physical activity [67] or cardiorespiratory fitness [10, 102], disregard for the possible effect attributed to these variables when investigating the association between muscular fitness and cardiometabolic variables may lead to different interpretations regarding obtained results. Thus, in addition to muscular fitness, it seems appropriate that studies measure physical activity and cardiorespiratory fitness, and consider adjusted models with and without the inclusion of these variables in order to remove the confounding, and thus provide a better interpretation of the results obtained. Additionally, it is suggested that when the inclusion/adjustment of associations for such variables is not possible, the authors of the studies must acknowledge the possible limitations that the absence of control for the analyses for physical activity and cardiorespiratory fitness may result, whether in the results obtained in their own studies, or when citing the results identified in other studies or comparing their own results with others described in the literature.
In addition to a large number of databases and information analyzed/reviewed, the analysis of all available information according to the muscular fitness tests/measurements adopted by the studies and the presentation of results according to sex, design, and number of variables for the control of confounding are considered strengths of this review. Conversely, important limitations of this review should be reported, such as the small number of studies that aimed to investigate the association between muscular fitness and lipids, glucose markers and inflammatory markers, which reduces the possibility of conclusive establishment for these associations. Although rigorous methodological control was adopted in the search for information, publication bias cannot be disregarded. However, the global percentage for the inverse association of muscular fitness with cardiometabolic variables below 50.0% identified in most of the results indicates a reduced possibility of this bias in the summarized of evidence. Additionally, although evidence according to sex reported by the studies indicated a similar direction compared to those analyzed in general, information according to sex for most of the investigated associations is not available in the literature. Another aspect that must be stated concerns the quality of conduct of the analyzed longitudinal studies. Approximately three out of ten studies analyzed did not include outcome values measured at baseline as a covariate in the adjusted longitudinal analyses. The inclusion of measured outcome values at baseline can lead to different scenarios with regard to the direction of associations, which can be important for understanding the tested associations. Not adjusting analysis results to baseline outcome values will indicate the total longitudinal effect of exposure on the outcome, whereas adjusting the analyses for the baseline outcome values will essentially indicate the direct effect of exposure on the longitudinal outcome [137]. Finally, the evidence mainly derives from cross-sectional studies that preclude inferences about causality and directionality. Properly controlled longitudinal studies for confounding and mechanistic studies are needed to better understand the role of muscular fitness in the cardiometabolic health of children and adolescents and possible differences based on sex. In this same sense, Mendelian randomization studies could provide valuable contributions regarding the causality of these associations.
5 Conclusions
In view of the studies included in this systematic review regarding the relationship between muscular fitness and cardiometabolic variables in children and adolescents, it can be concluded that:
-
1.
Muscular fitness assessed by maximum muscular strength/power or muscular endurance is potentially associated with lower obesity. When considering the assessment of maximum muscular strength/power, tests with lower limb demand (e.g., jumps), tests involving recruitment of upper limbs (e.g., handgrip strength) and results normalized for body mass, and/or a combination of tests that evaluate maximum muscular strength/power and results normalized for body mass have been shown to be more sensitive for this interrelationship.
-
2.
Maximum muscular strength/power or muscular endurance are associated with a lower risk related to clustered cardiometabolic variables, with no differences attributed to the muscular fitness tests/measurements adopted.
-
3.
The associations between muscular fitness and blood pressure, lipids, glucose homeostasis biomarkers, and inflammatory markers are inconsistent.
References
Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. https://doi.org/10.1016/j.jacc.2017.04.052.
National Heart Lung and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. 2011;128(Suppl 5):S213–56. https://doi.org/10.1542/peds.2009-2107c.
Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;74(10):e177–232. https://doi.org/10.1161/CIR.0000000000000678.
Leiter LA, Fitchett DH, Gilbert RE, Gupta M, Mancini GJ, McFarlane PA, et al. Cardiometabolic risk in Canada: a detailed analysis and position paper by the cardiometabolic risk working group. Can J Cardiol. 2011;27(2):e1–33. https://doi.org/10.1016/j.cjca.2010.12.054.
Eckel RH, Cornier MAJB. Update on the NCEP ATP-III emerging cardiometabolic risk factors. BMC Med. 2014;12(1):115. https://doi.org/10.1186/1741-7015-12-115.
Smith JJ, Eather N, Morgan PJ, Plotnikoff RC, Faigenbaum AD, Lubans DR. The health benefits of muscular fitness for children and adolescents: a systematic review and meta-analysis. Sports Med. 2014;44(9):1209–23. https://doi.org/10.1007/s40279-014-0196-4.
American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. Baltimore: Lippincott Williams & Wilkins; 2013.
Ortega FB, Ruiz JR, Castillo MJ, Sjöström M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. 2008;32(1):1–11. https://doi.org/10.1038/sj.ijo.0803774.
de Lima TR, Martins PC, Guerra PH, Silva DAS. Muscular fitness and cardiovascular risk factors in children and adolescents: a systematic review. J Strength Cond Res. 2020;34(8):2394–406. https://doi.org/10.1519/jsc.0000000000002840.
Grontved A, Ried-Larsen M, Ekelund U, Froberg K, Brage S, Andersen LB. Independent and combined association of muscle strength and cardiorespiratory fitness in youth with insulin resistance and beta-cell function in young adulthood: the European Youth Heart Study. Diabetes Care. 2013;36(9):2575–81. https://doi.org/10.2337/dc12-2252.
Grøntved A, Ried-Larsen M, Møller NC, Kristensen PL, Froberg K, Brage S, et al. Muscle strength in youth and cardiovascular risk in young adulthood (the European Youth Heart Study). Br J Sports Med. 2015;49(2):90–4. https://doi.org/10.1136/bjsports-2012-091907.
Demmer DL, Beilin LJ, Hands B, Burrows S, Cox KL, Straker LM, et al. Effects of muscle strength and endurance on blood pressure and related cardiometabolic risk factors from childhood to adolescence. J Hypertens. 2016;34(12):2365–75. https://doi.org/10.1097/hjh.0000000000001116.
Fraser BJ, Huynh QL, Schmidt MD, Dwyer T, Venn AJ, Magnussen CG. Childhood muscular fitness phenotypes and adult metabolic syndrome. Med Sci Sports Exerc. 2016;48(9):1715–22. https://doi.org/10.1249/mss.0000000000000955.
Castro-Piñero J, Perez-Bey A, Cuenca-Garcia M, Cabanas-Sanchez V, Gómez-Martínez S, Veiga OL, et al. Muscle fitness cut points for early assessment of cardiovascular risk in children and adolescents. J Pediatr. 2019;206:134-41.e3. https://doi.org/10.1016/j.jpeds.2018.10.026.
Tarp J, Bugge A, Moller NC, Klakk H, Rexen CT, Grontved A, et al. Muscle fitness changes during childhood associates with improvements in cardiometabolic risk factors: a prospective study. J Phys Act Health. 2019;16(2):108–15. https://doi.org/10.1123/jpah.2017-0678.
Hasselstrom H, Hansen SE, Froberg K, Andersen LB. Physical fitness and physical activity during adolescence as predictors of cardiovascular disease risk in young adulthood. Danish Youth and Sports Study. An eight-year follow-up study. Int J Sports Med. 2002;23(Suppl 1):S27-31. https://doi.org/10.1055/s-2002-28458.
Benson A, Torode ME, Singh MF. The effect of high-intensity progressive resistance training on adiposity in children: a randomized controlled trial. Int J Obes. 2008. https://doi.org/10.1038/ijo.2008.5.
Cooper R, Hardy R, Bann D, Sayer AA, Ward KA, Adams JE, et al. Body mass index from age 15 years onwards and muscle mass, strength, and quality in early old age: findings from the MRC national survey of health and development. J Gerontol A Biol Sci Med Sci. 2014;69(10):1253–9. https://doi.org/10.1093/gerona/glu039.
Zaqout M, Michels N, Bammann K, Ahrens W, Sprengeler O, Molnar D, et al. Influence of physical fitness on cardio-metabolic risk factors in European children. The IDEFICS study. Int J Obes. 2016;40(7):1119–25. https://doi.org/10.1038/ijo.2016.22.
Heroux M, Onywera V, Tremblay MS, Adamo KB, Lopez Taylor J, Jauregui Ulloa E, et al. The relation between aerobic fitness, muscular fitness, and obesity in children from three countries at different stages of the physical activity transition. ISRN Obes. 2013;2013:e.1-10. https://doi.org/10.1155/2013/134835.
Crump C, Sundquist J, Winkleby MA, Sundquist K. Aerobic fitness, muscular strength and obesity in relation to risk of heart failure. Heart. 2017;103(22):1780–7. https://doi.org/10.1136/heartjnl-2016-310716.
Castro-Piñero J, Artero EG, España-Romero V, Ortega FB, Sjöström M, Suni J, et al. Criterion-related validity of field-based fitness tests in youth: a systematic review. Br J Sports Med. 2010;44(13):934–43. https://doi.org/10.1136/bjsm.2009.058321.
Jaric S. Muscle strength testing. Sports Med. 2002;32(10):615–31. https://doi.org/10.2165/00007256-200232100-00002.
Croix MDS. Advances in paediatric strength assessment: changing our perspective on strength development. J Sports Sci Med. 2007;6(3):292–304.
Magnussen CG, Schmidt MD, Dwyer T, Venn A. Muscular fitness and clustered cardiovascular disease risk in Australian youth. Eur J Appl Physiol. 2012;112(8):3167–71. https://doi.org/10.1007/s00421-011-2286-4.
Barker AR, Gracia-Marco L, Ruiz JR, Castillo MJ, Aparicio-Ugarriza R, González-Gross M, et al. Physical activity, sedentary time, TV viewing, physical fitness and cardiovascular disease risk in adolescents: the HELENA study. Int J Cardiol. 2018;254:303–9. https://doi.org/10.1016/j.ijcard.2017.11.080.
Blakeley CE, Van Rompay MI, Schultz NS, Sacheck JM. Relationship between muscle strength and dyslipidemia, serum 25(OH)D, and weight status among diverse schoolchildren: a cross-sectional analysis. BMC Pediatr. 2018;18(1):23. https://doi.org/10.1186/s12887-018-0998-x.
Palacio-Agüero A, Díaz-Torrente X, Dourado DQS. Relative handgrip strength, nutritional status and abdominal obesity in Chilean adolescents. PLoS ONE. 2020. https://doi.org/10.1371/journal.pone.0234316.
Dong B, Wang Z, Arnold L, Song Y, Wang HJ, Ma J. The association between blood pressure and grip strength in adolescents: Does body mass index matter. Hypertens Res. 2016;39(12):919–25. https://doi.org/10.1038/hr.2016.84.
Cohen DD, Gomez-Arbelaez D, Camacho PA, Pinzon S, Hormiga C, Trejos-Suarez J, et al. Low muscle strength is associated with metabolic risk factors in Colombian children: the ACFIES study. PLoS ONE. 2014;9(4): e93150. https://doi.org/10.1371/journal.pone.0093150.
Cohen DD, López-Jaramillo P, Fernández-Santos JR, Castro-Piñero J, Sandercock GRH. Muscle strength is associated with lower diastolic blood pressure in schoolchildren. Prev Med. 2017;95:1–6. https://doi.org/10.1016/j.ypmed.2016.11.006.
Fraser BJ, Blizzard L, Schmidt MD, Dwyer T, Venn AJ, Magnussen CG. The association between muscular power from childhood to adulthood and adult measures of glucose homeostasis. Scand J Med Sci Sports. 2019;29(12):1909–16. https://doi.org/10.1111/sms.13529.
Peterson MD, Saltarelli WA, Visich PS, Gordon PM. Strength capacity and cardiometabolic risk clustering in adolescents. Pediatrics. 2014;133(4):e896-903. https://doi.org/10.1542/peds.2013-3169.
Henriksson P, Leppänen MH, Henriksson H, Delisle Nyström C, Cadenas-Sanchez C, Ek A, et al. Physical fitness in relation to later body composition in pre-school children. J Sci Med Sport. 2019;22(5):574–9. https://doi.org/10.1016/j.jsams.2018.11.024.
Kim J, Must A, Fitzmaurice GM, Gillman MW, Chomitz V, Kramer E, et al. Relationship of physical fitness to prevalence and incidence of overweight among schoolchildren. Obes Res. 2005;13(7):1246–54. https://doi.org/10.1038/oby.2005.148.
Hruby A, Chomitz VR, Arsenault LN, Must A, Economos CD, McGowan RJ, et al. Predicting maintenance or achievement of healthy weight in children: the impact of changes in physical fitness. Obesity. 2012;20(8):1710–7. https://doi.org/10.1038/oby.2012.13.
Butterfield SA, Lehnhard RA, Coladarci T. Age, sex, and body mass index in performance of selected locomotor and fitness tasks by children in grades K-2. Percept Mot Ski. 2002;94(1):80–6. https://doi.org/10.2466/pms.2002.94.1.80.
Tokmakidis SP, Kasambalis A, Christodoulos AD. Fitness levels of Greek primary schoolchildren in relationship to overweight and obesity. Eur J Pediatr. 2006;165(12):867–74. https://doi.org/10.1007/s00431-006-0176-2.
Fogelholm M, Stigman S, Huisman T, Metsämuuronen J. Physical fitness in adolescents with normal weight and overweight. Scand J Med Sci Sports. 2008;18(2):162–70. https://doi.org/10.1111/j.1600-0838.2007.00685.x.
Ara I, Sanchez-Villegas A, Vicente-Rodriguez G, Moreno LA, Leiva MT, Martinez-Gonzalez MA, et al. Physical fitness and obesity are associated in a dose-dependent manner in children. Ann Nutr Metab. 2010;57(3–4):251–9. https://doi.org/10.1159/000322577.
Artero EG, Espana-Romero V, Ortega FB, Jimenez-Pavon D, Ruiz JR, Vicente-Rodriguez G, et al. Health-related fitness in adolescents: underweight, and not only overweight, as an influencing factor The AVENA study. Scand J Med Sci Sports. 2010;20(3):418–27. https://doi.org/10.1111/j.1600-0838.2009.00959.x.
Mak KK, Ho SY, Lo WS, Thomas GN, McManus AM, Day JR, et al. Health-related physical fitness and weight status in Hong Kong adolescents. BMC Public Health. 2010;23(10):88. https://doi.org/10.1186/1471-2458-10-88.
Mota J, Vale S, Martins C, Gaya A, Moreira C, Santos R, et al. Influence of muscle fitness test performance on metabolic risk factors among adolescent girls. Diabetol Metab Syndr. 2010;23(2):42. https://doi.org/10.1186/1758-5996-2-42.
Pino-Ortega J, De la Cruz-Sánchez E, Martínez-Santos R. Health-related fitness in school children: compliance with physical activity recommendations and its relationship with body mass index and diet quality. Arch Latinoam Nutr. 2010;60(4):374–9.
Gonzalez-Suarez CB, Grimmer-Somers K. The association of physical activity and physical fitness with pre-adolescent obesity: an observational study in Metromanila, Philippines. J Phys Act Health. 2011;8(6):804–10. https://doi.org/10.1123/jpah.8.6.804.
Joshi P, Bryan C, Howat H. Relationship of body mass index and fitness levels among schoolchildren. J Strength Cond Res. 2012;26(4):1006–14. https://doi.org/10.1519/jsc.0b013e31822dd3ac.
Pathare N, Haskvitz EM, Selleck M. Comparison of measures of physical performance among young children who are healthy weight, overweight, or obese. Pediatr Phys Ther. 2013;25(3):291–6. https://doi.org/10.1097/pep.0b013e31829846bd.
Cieśla E, Mleczko E, Bergier J, Markowska M, Nowak-Starz G. Health-related physical fitness, BMI, physical activity and time spent at a computer screen in 6 and 7-year-old children from rural areas in Poland. Ann Agric Environ Med. 2014;21(3):617–21. https://doi.org/10.5604/12321966.1120613.
Silva DAS, Gonçalves ECA, Grigollo LR, Petroski EL. Factors associated with low levels of lumbar strength in adolescents in Southern Brazil. Revista Paul Pediatr. 2014;32(4):360–6. https://doi.org/10.1016/s2359-3482(15)30071-3.
Casonatto J, Fernandes RA, Batista MB, Cyrino ES, Coelho-e-Silva MJ, de Arruda M, et al. Association between health-related physical fitness and body mass index status in children. J Child Health Care. 2016;20(3):294–303. https://doi.org/10.1177/1367493515598645.
Henriksson P, Cadenas-Sanchez C, Leppänen MH, Delisle Nyström C, Ortega FB, Pomeroy J, et al. Associations of fat mass and fat-free mass with physical fitness in 4-year-old children: results from the MINISTOP Trial. Nutrients. 2016;8(8):473. https://doi.org/10.3390/nu8080473.
Martinez-Tellez B, Sanchez-Delgado G, Cadenas-Sanchez C, Mora-Gonzalez J, Martín-Matillas M, Löf M, et al. Health-related physical fitness is associated with total and central body fat in preschool children aged 3 to 5 years. Pediatr Obes. 2016;11(6):468–74. https://doi.org/10.1038/hr.2016.84.
Pereira TA, Bergmann MLDA, Bergmann GG. Factors associated with low physical fitness in adolescents. Rev Bras Med Esporte. 2016;22(3):176–81. https://doi.org/10.1590/1517-869220162203144162.
Latorre Román P, López DM, Aguayo BB, Fuentes AR, García-Pinillos F, Redondo MM. Handgrip strength is associated with anthropometrics variables and sex in preschool children: a cross sectional study providing reference values. Phys Ther Sport. 2017;26:1–6. https://doi.org/10.1016/j.ptsp.2017.04.002.
Nkwana MR, Monyeki KD, Matshipi M, Sekgala MD, Ramoshaba NE, Mashiane TMJ. The relationship between strength measurements and anthropometric indicators (BMI and skinfold thickness) in Ellisras rural adolescents aged 9–15 Years: Ellisras Longitudinal Study. Hum Mov. 2017;18(1):11–8. https://doi.org/10.1515/humo-2017-0003.
Silva DAS, Pelegrini A, de Castro JAC, de Lima TR, de Sousa GR, de Lima Silva JMF, et al. Low handgrip strength levels among adolescents in a city in southern Brazil. J Bodyw Mov Ther. 2017;21(4):884–9. https://doi.org/10.1016/j.jbmt.2017.03.004.
Riso EM, Toplaan L, Viira P, Vaiksaar S, Jürimäe J. Physical fitness and physical activity of 6–7-year-old children according to weight status and sports participation. PLoS ONE. 2018;14(6): e0218901. https://doi.org/10.1371/journal.pone.0218901.
Toriola A, Ajayi-Vincent O, Oyeniyi P, Akindutire I, Adeagbo D, Konwea P, et al. Relationship between body composition and musculoskeletal fitness in Nigerian children. Asian J Sci Res. 2018;11(2):169–76. https://doi.org/10.3923/ajsr.2018.169.176.
Garcia-Hermoso A, Correa-Bautista JE, Olloquequi J, Ramirez-Velez R. Health-related physical fitness and weight status in 13-to 15-year-old Latino adolescents. A pooled analysis. J Pediatr (Rio J). 2019;95(4):435–42. https://doi.org/10.1016/j.jped.2018.04.002.
He HJ, Pan L, Dui JW, Liu F, Jin YM, Ma JG, et al. Muscle fitness and its association with body mass index in children and adolescents aged 7–18 years in China: a cross-sectional study. BMC Pediatr. 2019;19:101. https://doi.org/10.1186/s12887-019-1477-8.
Lang JJ, Larouche R, Tremblay MS. The association between physical fitness and health in a nationally representative sample of Canadian children and youth aged 6 to 17 years. Health Promot Chronic Dis Prev Can. 2019;39(3):104–11. https://doi.org/10.24095/hpcdp.39.3.02.
Weston KL, Pasecinic N, Basterfield L. A preliminary study of physical fitness in 8-to 10-year-old primary school children from north east England in comparison with national and international data. Pediatr Exerc Sci. 2019;31(2):229–37. https://doi.org/10.1123/pes.2018-0135.
Fiori F, Bravo G, Parpinel M, Messina G, Malavolta R, Lazzer S. Relationship between body mass index and physical fitness in Italian prepubertal schoolchildren. PLoS ONE. 2020;15(5): e0233362. https://doi.org/10.1371/journal.pone.0233362.
Xu Y, Mei M, Wang H, Yan Q, He G. Association between weight status and physical fitness in chinese mainland children and adolescents: a cross-sectional study. Int J Environ Res Public Health. 2020;17(7):2468. https://doi.org/10.3390/ijerph17072468.
Janz K, Dawson J, Mahoney L. Increases in physical fitness during childhood improve cardiovascular health during adolescence: the Muscatine Study. Int J Sports Med. 2002;23(S1):15–21. https://doi.org/10.1055/s-2002-28456.
Fraser BJ, Blizzard L, Cleland V, Schmidt MD, Smith KJ, Gall SL, et al. Factors associated with persistently high muscular power from childhood to adulthood. Med Sci Sports Exerc. 2020;52(1):49–55. https://doi.org/10.1249/mss.0000000000002108.
Moliner-Urdiales D, Ruiz JR, Vicente-Rodriguez G, Ortega FB, Rey-Lopez JP, España-Romero V, et al. Associations of muscular and cardiorespiratory fitness with total and central body fat in adolescents: The HELENA study. Br J Sports Med. 2011;45(2):101–8. https://doi.org/10.1136/bjsm.2009.062430.
Garcia-Hermoso A, Vegas-Heredia ED, Fernandez-Vergara O, Ceballos-Ceballos R, Andrade-Schnettler R, Arellano-Ruiz P, et al. Independent and combined effects of handgrip strength and adherence to a Mediterranean diet on blood pressure in Chilean children. Nutrition. 2019;60:170–4. https://doi.org/10.1016/j.nut.2018.08.019.
Hoekstra T, Boreham CA, Murray LJ, Twisk JW. Associations between aerobic and muscular fitness and cardiovascular disease risk: the northern Ireland young hearts study. J Phys Act Health. 2008;5(6):815–29. https://doi.org/10.1123/jpah.5.6.815.
Nunes HEG, Alves CAS, Gonçalves ECA, Silva DAS. What physical fitness component is most closely associated with adolescents’ blood pressure? Percept Mot Ski. 2017;124(6):1107–20. https://doi.org/10.1177/0031512517730414.
Zhang R, Li CW, Liu TT, Zheng LQ, Li SX. Handgrip strength and blood pressure in children and adolescents: evidence from NHANES 2011 to 2014. Am J Hypertens. 2018;31(7):792–6. https://doi.org/10.1093/ajh/hpy032.
Li S, Zhang R, Pan G, Zheng L, Li C. Handgrip strength is associated with insulin resistance and glucose metabolism in adolescents: Evidence from National Health and Nutrition Examination Survey 2011 to 2014. Pediatr Diabetes. 2018;19(3):375–80. https://doi.org/10.1111/pedi.12596.
Ruiz JR, Ortega FB, Warnberg J, Moreno LA, Carrero JJ, Gonzalez-Gross M, et al. Inflammatory proteins and muscle strength in adolescents: the Avena study. Arch Pediatr Adolesc Med. 2008;162(5):462–8. https://doi.org/10.1001/archpedi.162.5.462.
Martinez-Gomez D, Gomez-Martinez S, Ruiz JR, Diaz LE, Ortega FB, Widhalm K, et al. Objectively-measured and self-reported physical activity and fitness in relation to inflammatory markers in European adolescents: the HELENA Study. Atherosclerosis. 2012;221(1):260–7. https://doi.org/10.1016/j.atherosclerosis.2011.12.032.
Artero EG, Espana-Romero V, Jimenez-Pavon D, Martinez-Gomez D, Warnberg J, Gomez-Martinez S, et al. Muscular fitness, fatness and inflammatory biomarkers in adolescents. Pediatr Obes. 2014;9(5):391–400. https://doi.org/10.1111/j.2047-6310.2013.00186.x.
Rodríguez Valero FJ, Gualteros JA, Torres JA, Umbarila Espinosa LM, Ramírez-Velez R. Association between muscular fitness and physical health status among children and adolescents from bogotá, colombia. Nutr Hosp. 2015;32(4):1559–66. https://doi.org/10.3305/nh.2015.32.4.9310.
Diez-Fernandez A, Sanchez-Lopez M, Gulias-Gonzalez R, Notario-Pacheco B, García-Prieto JC, Arias-Palencia N, et al. BMI as a mediator of the relationship between muscular fitness and cardiometabolic risk in children: a mediation analysis. PLoS ONE. 2015;10(1): e0116506. https://doi.org/10.1371/journal.pone.0116506.
Agostinis-Sobrinho CA, Ramirez-Velez R, García-Hermoso A, Moreira C, Lopes L, Oliveira-Santos J, et al. Low-grade inflammation and muscular fitness on insulin resistance in adolescents: Results from LabMed Physical Activity Study. Pediatr Diabetes. 2018;19(3):429–35. https://doi.org/10.1111/pedi.12607.
Steene-Johannessen J, Anderssen SA, Kolle E, Andersen LB. Low muscle fitness is associated with metabolic risk in youth. Med Sci Sports Exerc. 2009;41(7):1361–7. https://doi.org/10.1249/mss.0b013e31819aaae5.
Fraser BJ, Blizzard L, Schmidt MD, Juonala M, Dwyer T, Venn AJ, et al. Childhood cardiorespiratory fitness, muscular fitness and adult measures of glucose homeostasis. J Sci Med Sport. 2018;21(9):935–40. https://doi.org/10.1016/j.jsams.2018.02.002.
Fraser BJ, Blizzard L, Cleland V, Schmidt MD, Smith KJ, Gall SL, et al. Factors associated with muscular fitness phenotypes in Australian children: A cross-sectional study. J Sports Sci. 2020;38(1):38–45. https://doi.org/10.1080/02640414.2019.1679575.
Morikawa SY, Fujihara K, Hatta M, Osawa T, Ishizawa M, Yamamoto M, et al. Relationships among cardiorespiratory fitness, muscular fitness, and cardiometabolic risk factors in Japanese adolescents: Niigata screening for and preventing the development of non-communicable disease study-Agano (NICE EVIDENCE Study-Agano) 2. Pediatr Diabetes. 2018;19(4):593–602. https://doi.org/10.1111/pedi.12623.
Malina RM, Reyes MEP, Tan SK, Little BB. Physical fitness of normal, stunted and overweight children 6–13 years in Oaxaca, Mexico. Eur J Clin Nutr. 2011;65(7):826–34. https://doi.org/10.1038/ejcn.2011.44.
Ramirez-Velez R, Tordecilla-Sanders A, Correa-Bautista JE, Peterson MD, Garcia-Hermoso A. Handgrip Strength and ideal cardiovascular health among Colombian Children and Adolescents. J Pediatr. 2016;179:82–9. https://doi.org/10.1016/j.jpeds.2016.08.099.
Castro-Piñero J, Laurson KR, Artero EG, Ortega FB, Labayen I, Ruperez AI, et al. Muscle strength field-based tests to identify European adolescents at risk of metabolic syndrome: the HELENA study. J Sci Med Sport. 2019;22(8):929–34. https://doi.org/10.1016/j.jsams.2019.04.008.
Lopez-Gil JF, Brazo-Sayavera J, Lucas JLY, Cavichiolli FR. Weight status is related to health-related physical fitness and physical activity but not to sedentary behaviour in children. Int J Environ Res Public Health. 2020;17(12):4518. https://doi.org/10.3390/ijerph17124518.
Edelson LR, Mathias KC, Fulgoni VL 3rd, Karagounis LG. Screen-based sedentary behavior and associations with functional strength in 6–15 year-old children in the United States. BMC Public Health. 2016;4(16):116. https://doi.org/10.1186/s12889-016-2791-9.
de Lima TR, Martins PC, Torre GL, Mannocci A, Samara Siva K, Santos Silva DA. Association between muscle strength and risk factors for metabolic syndrome in children and adolescents: a systematic review. J Pediatr Endocrinol Metab. 2020. https://doi.org/10.1515/jpem-2020-0135(ahead of print)
García-Hermoso A, Ramírez-Campillo R, Izquierdo M. Is muscular fitness associated with future health benefits in children and adolescents? A systematic review and meta-analysis of longitudinal studies. Sports Med. 2019;49(7):1079–94. https://doi.org/10.1007/s40279-019-01098-6.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–34. https://doi.org/10.7326/0003-4819-151-4-200908180-00136.
World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach (World Health Organization, 2016).
Artero EG, Lee D-C, Lavie CJ, España-Romero V, Sui X, Church TS, et al. Effects of muscular strength on cardiovascular risk factors and prognosis. J Cardiopulm Rehabil Prev. 2012;32(6):351–8. https://doi.org/10.1097/hcr.0b013e3182642688.
Enoka RM. Muscle strength and its development. Sports Med. 1988;6(3):146–68. https://doi.org/10.2165/00007256-198806030-00003.
Keeble C, Baxter P, Barber S, Law G. Participation rates In epidemiology studies and surveys: a review 2005–2007. Internet J Epidemiol. 2016;14(1):1–14. https://doi.org/10.1016/j.annepidem.2007.03.013.
American Association for Public Opinion Research. Standard definitions: final dispositions of case codes and outcome rates for surveys. 9th ed. Lenexa: American Association for Public Opinion Research; 2016.
Morton LM, Cahill J, Hartge P. Reporting participation in epidemiologic studies: a survey of practice. Am J Epidemiol. 2006;163(3):197–203. https://doi.org/10.1093/aje/kwj036.
Beunen G, Thomis M. Muscular strength development in children and adolescents. Pediatr Exerc Sci. 2000;12(2):174–97. https://doi.org/10.1123/pes.12.2.174.
Smith JJ, Eather N, Weaver RG, Riley N, Beets MW, Lubans DR. Behavioral correlates of muscular fitness in children and adolescents: a systematic review. Sports Med. 2019;49(6):887–904. https://doi.org/10.1007/s40279-019-01089-7.
National Heart Lung Blood Institute. Quality assessment tool for observational cohort and cross-sectional studies. National Institutes of Health, Department of Health Human Services; 2014.
Benson AC, Torode ME, Fiatarone Singh MA. Muscular strength and cardiorespiratory fitness is associated with higher insulin sensitivity in children and adolescents. Int J Pediatr Obes. 2006;1(4):222–31. https://doi.org/10.1080/17477160600962864.
Garcia-Artero E, Ortega FB, Ruiz JR, Mesa JL, Delgado M, Gonzalez-Gross M, et al. Lipid and metabolic profiles in adolescents are affected more by physical fitness than physical activity (AVENA study). Rev Esp Cardiol. 2007;60(6):581–8. https://doi.org/10.1157/13107114.
Artero EG, Ruiz JR, Ortega FB, Espana-Romero V, Vicente-Rodriguez G, Molnar D, et al. Muscular and cardiorespiratory fitness are independently associated with metabolic risk in adolescents: the HELENA study. Pediatr Diabetes. 2011;12(8):704–12. https://doi.org/10.1111/j.1399-5448.2011.00769.x.
Jiménez-Pavón D, Ortega FB, Artero EG, Labayen I, Vicente-Rodriguez G, Huybrechts I, et al. Physical activity, fitness, and serum leptin concentrations in adolescents. J Pediatr. 2012;160(4):598–603. https://doi.org/10.1016/j.jpeds.2011.09.058.
Jiménez-Pavón D, Ortega FB, Valtueña J, Castro-Piñero J, Gómez-Martínez S, Zaccaria M, et al. Muscular strength and markers of insulin resistance in European adolescents: The HELENA Study. Eur J Appl Physiol. 2012;112(7):2455–65. https://doi.org/10.1007/s00421-011-2216-5.
Martinez-Gomez D, Eisenmann JC, Gomez-Martinez S, Veses A, Romeo J, Veiga OL, et al. Associations of physical activity and fitness with adipocytokines in adolescents: the AFINOS study. Nutr Metab Cardiovasc Dis. 2012;22(3):252–9. https://doi.org/10.1016/j.numecd.2010.07.010.
Buchan DS, Boddy LM, Young JD, Cooper SM, Noakes TD, Mahoney C, et al. Relationships between cardiorespiratory and muscular fitness with cardiometabolic risk in adolescents. Res Sports Med. 2015;23(3):227–39. https://doi.org/10.1080/15438627.2015.1040914.
Agostinis-Sobrinho C, Santos R, Moreira C, Abreu S, Lopes L, Oliveira-Santos J, et al. Association between serum adiponectin levels and muscular fitness in Portuguese adolescents: LabMed Physical Activity Study. Nutr Metab Cardiovasc Dis. 2016;26(6):517–24. https://doi.org/10.1016/j.numecd.2016.02.011.
Peterson MD, Zhang P, Saltarelli WA, Visich PS, Gordon PM. Low muscle strength thresholds for the detection of cardiometabolic risk in adolescents. Am J Prev Med. 2016;50(5):593–9. https://doi.org/10.1016/j.amepre.2015.09.019.
Agostinis-Sobrinho C, Abreu S, Moreira C, Lopes L, García-Hermoso A, Ramírez-Vélez R, et al. Muscular fitness, adherence to the Southern European Atlantic Diet and cardiometabolic risk factors in adolescents. Nutr Metab Cardiovasc Dis. 2017;27(8):695–702. https://doi.org/10.1080/17461391.2017.1394368.
Agostinis-Sobrinho CA, Moreira C, Abreu S, Lopes L, Sardinha LB, Oliveira-Santos J, et al. Muscular fitness and metabolic and inflammatory biomarkers in adolescents: Results from LabMed Physical Activity Study. Scand J Med Sci Sports. 2017;27(12):1873–80. https://doi.org/10.1111/sms.12805.
Gomes TN, dos Santos FK, Katzmarzyk PT, Maia J. Active and strong: physical activity, muscular strength, and metabolic risk in children. Am J Hum Biol. 2017;29(1):e.22904. https://doi.org/10.1002/ajhb.22904.
Rioux BV, Kuwornu P, Sharma A, Tremblay MS, McGavock JM, Senechal M. Association between handgrip muscle strength and cardiometabolic z-score in children 6 to 19 years of age: results from the Canadian Health Measures Survey. Metab Syndr Relat Disord. 2017;15(7):379–84. https://doi.org/10.1089/met.2016.0147.
Delgado-Alfonso A, Perez-Bey A, Conde-Caveda J, Izquierdo-Gomez R, Esteban-Cornejo I, Gomez-Martinez S, et al. Independent and combined associations of physical fitness components with inflammatory biomarkers in children and adolescents. Pediatr Res. 2018;84(5):704–12. https://doi.org/10.1038/s41390-018-0150-5.
Pérez-Bey A, Segura-Jiménez V, Fernández-Santos JDR, Esteban-Cornejo I, Gómez-Martínez S, Veiga OL, et al. The role of adiposity in the association between muscular fitness and cardiovascular disease. J Pediatr. 2018;199:178-85.e4. https://doi.org/10.1016/j.jpeds.2018.03.071.
Agostinis-Sobrinho C, Dias AF, Brand C, Norkiene S, Abreu S, Gaya ACA, et al. Adherence to Southern European Atlantic Diet and physical fitness on the atherogenic index of plasma in adolescents. Cad Saúde Pública. 2019;35(12): e00200418. https://doi.org/10.1590/0102-311x00200418.
Lee HS, Jeong WW, Choi YJ, Seo YG, Noh HM, Song HJ, et al. Association between physical fitness and cardiometabolic risk of children and adolescents in Korea. Korean J Fam Med. 2019;40(3):159–64. https://doi.org/10.4082/kjfm.17.0085.
Saldanha N, Reuter CP, Renner JDP, Barbian CD, Silveira JFD, Schneiders LD, et al. Low levels of cardiorespiratory fitness and abdominal resistance are associated with metabolic risk in schoolchildren. J Pediatr Endocrinol Metab. 2019;32(5):455–60. https://doi.org/10.1515/jpem-2018-0236.
Agostinis-Sobrinho C, Brand C, Moreira C, Lopes L, Oliveira-Santos J, Silva P, et al. Muscular fitness, Southern European Atlantic Diet and inflammation in adolescents. Azorean Physical Activity and Health Study II. Eur J Sport Sci. 2018;18(1):104–11. https://doi.org/10.1080/17461391.2017.1394368.
Agostinis-Sobrinho C, García-Hermoso A, Ramírez-Vélez R, Moreira C, Lopes L, Oliveira-Santos J, et al. Longitudinal association between ideal cardiovascular health status and muscular fitness in adolescents: the LabMed Physical Activity Study. Nutr Metab Cardiovasc Dis. 2018;28(9):892–9. https://doi.org/10.1016/j.numecd.2018.05.012.
Agostinis-Sobrinho C, Ruiz JR, Moreira C, Lopes L, Ramirez-Velez R, Garcia-Hermoso A, et al. Changes in muscular fitness and its association with blood pressure in adolescents. Eur J Pediatr. 2018;177(7):1101–9. https://doi.org/10.1007/s00431-018-3164-4.
Wolfe RR. The underappreciated role of muscle in health and disease. Am J Clin Nutr. 2006;84(3):475–82. https://doi.org/10.1093/ajcn/84.3.475.
Cali AM, Caprio S. Obesity in children and adolescents. J Clin Endocrinol Metab. 2008;93(11_supplement_1):s31–6.
Wells JC. Toward body composition reference data for infants, children, and adolescents. Adv Nutr. 2014;5(3):320S-S329. https://doi.org/10.3945/an.113.005371.
Orsso CE, Tibaes JR, Rubin DA, Field CJ, Heymsfield SB, Prado CM, et al. Metabolic implications of low muscle mass in the pediatric population: a critical review. Metab Clin Exp. 2019;99:102–12. https://doi.org/10.1016/j.metabol.2019.153949.
Tanner JM. Growth at adolescence. Oxford: Blackwell; 1962.
Sayer AA, Syddall H, Martin H, Patel H, Baylis D, Cooper C. The developmental origins of sarcopenia. J Nutr Health Aging. 2008;12(7):427–32.
Fahs C, Heffernen K, Ranadive S, Jae S, Fernhall B. Muscular strength is inversely associated with aortic stiffness in young men. Med Sci Sports Exerc. 2010;42(9):1619–24. https://doi.org/10.1249/mss.0b013e3181d8d834.
Loenneke JP, Fahs CA, Heffernan KS, Rossow LM, Thiebaud RS, Bemben MG. Relationship between thigh muscle mass and augmented pressure from wave reflections in healthy adults. Eur J Appl Physiol. 2013;113(2):395–401. https://doi.org/10.1007/s00421-012-2449-y.
Hosick PA, McMurray RG, Hackney A, Battaglini CL, Combs TP, Harrell JS. Resting IL-6 and TNF-α level in children of different weight and fitness status. Pediatr Exerc Sci. 2013;25(2):238–47. https://doi.org/10.1123/pes.25.2.238.
Stump CS, Henriksen EJ, Wei Y, Sowers JR. The metabolic syndrome: role of skeletal muscle metabolism. Ann Med. 2006;38(6):389–402. https://doi.org/10.1080/07853890600888413.
Marlatt KL, Steinberger J, Dengel DR, Sinaiko A, Moran A, Chow LS, et al. Impact of pubertal development on endothelial function and arterial elasticity. J Pediatr. 2013;163(5):1432–6. https://doi.org/10.1016/j.jpeds.2013.07.002.
Armstrong N, Barker AR, McManus AM. Muscle metabolism changes with age and maturation: How do they relate to youth sport performance? Br J Sports Med. 2015;49(13):860–4. https://doi.org/10.1136/bjsports-2014-094491.
Loos R, Thomis M, Maes H, Beunen G, Claessens A, Derom C, et al. Gender-specific regional changes in genetic structure of muscularity in early adolescence. J Appl Physiol. 1997;82(6):1802–10. https://doi.org/10.1152/jappl.1997.82.6.1802.
Thomis M, Beunen G, Leemputte MV, Maes H, Blimkie C, Claessens A, et al. Inheritance of static and dynamic arm strength and some of its determinants. Acta Physiol Scand. 1998;163(1):59–71. https://doi.org/10.1046/j.1365-201x.1998.00344.x.
Tarp J, Child A, White T, Westgate K, Bugge A, Grøntved A, et al. Physical activity intensity, bout-duration, and cardiometabolic risk markers in children and adolescents. Int J Obes. 2018;42(9):1639–50. https://doi.org/10.1038/s41366-018-0152-8.
Boreham C, Riddoch C. The physical activity, fitness and health of children. J Sports Sci. 2001;19(12):915–29. https://doi.org/10.1080/026404101317108426.
Glymour MM, Weuve J, Berkman LF, Kawachi I, Robins JM. When is baseline adjustment useful in analyses of change? An example with education and cognitive change. Am J Epidemiol. 2005;162(3):267–78.
Acknowledgements
The authors would like to thank the team of the Clinical Analysis Laboratory of the University Hospital “Professor Polydoro Ernani de São Thiago” at Federal University of Santa Catarina, Florianópolis, Brazil, for assisting the research. Dr. Silva was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001 and Dr. Silva is supported in part by CNPq (302028/2018-8).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The authors declare that they have not received funding for this article.
Conflict of interest
Tiago Rodrigues de Lima, Priscila Custódio Martins, Yara Maria Franco Moreno, Jean-Philippe Chaput, Mark Tremblay, Xuemei Sui and Diego Augusto Santos Silva declare that they have no conflicts of interest relevant to the content of this review.
Authorship contributions
TRL conceived the review, wrote and edited significant sections of the manuscript, carried out the literature search, screened all identifed studies based on title and abstract, and assisted with the full text screening, the risk-of-bias assessment, and the data extraction process. PCM assisted with the title and abstract screening, the full text screening, and the risk-of-bias assessment. YMFM wrote and edited significant sections of the manuscript. JPC wrote and edited significant sections of the manuscript. MST wrote and edited significant sections of the manuscript. XS revised and edited significant sections of the manuscript and assisted with the risk-of-bias assessment. DASS revised and edited significant sections of the manuscript and assisted with the risk-of-bias assessment. All authors reviewed and approved the final manuscript.
Data availability statement
The material analyzed in this study (including the strategies and descriptors used in each database, the detailed risk-of-bias assessment, and the totality of information analyzed) are available in the Electronic Supplementary Materials.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
de Lima, T.R., Martins, P.C., Moreno, Y.M.F. et al. Muscular Fitness and Cardiometabolic Variables in Children and Adolescents: A Systematic Review. Sports Med 52, 1555–1575 (2022). https://doi.org/10.1007/s40279-021-01631-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-021-01631-6