
Abstract
Background and Objectives
A new once-daily formulation of tacrolimus (Envarsus®) has recently been developed, with alleged different pharmacokinetics from previous tacrolimus formulations. The objectives of this study were to develop population pharmacokinetic models and Bayesian estimators based on limited sampling strategies for Envarsus® in kidney and liver transplant recipients.
Materials and Methods
Full tacrolimus concentration-time profiles (13 samples) were drawn from 57 liver (113 profiles) and 49 kidney (97 profiles) graft recipients transplanted for at least 6 months and switched from Prograf® to Envarsus®. The two databases were split into a development (75%) and a validation (25%) dataset. Pharmacokinetic models characterised by a single compartment with first-order elimination and absorption in two phases described by a sum of two gamma distributions were developed using non-parametric (Pmetrics) and parametric (ITSIM) approaches in parallel. The best limited sampling strategy for each patient group was determined using the multiple model optimal algorithm. The performance of the models and derived Bayesian estimators was evaluated in the validation set.
Results
The best limited sampling strategy was 0, 8 and 12 h post-dose, leading to a relative bias ± standard deviation (root-mean-square error) between observed and modelled inter-dose area under the curve in the validation dataset of: 0.32 ± 6.86% (6.87%) for ITSIM and 3.4 ± 13.4% (13.2%) for Pmetrics in kidney transplantation; and 0.89 ± 7.32% (7.38%) for ITSIM and −2.62 ± 8.65% (8.89%) for Pmetrics in liver transplantation.
Conclusion
Population pharmacokinetic models and Bayesian estimators for Envarsus® in kidney and liver transplantation were developed and are now available online for area under the curve-based tacrolimus dose adjustment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
This is the first study describing the population pharmacokinetics of Envarsus®, a new tacrolimus formulation, in kidney and liver transplant patients. |
Two modelling methods were used in parallel (a parametric and a non-parametric). |
Two Bayesian estimators were developed enabling area under the curve determination using three samples performed at 0, 8 and 12 h post-dose. |
1 Introduction
Tacrolimus is the most employed first-line immunosuppressant in the prevention and treatment of allograft rejection in solid organ transplantation. As this drug has a narrow therapeutic index and significant inter-individual variability, therapeutic drug monitoring is essential to avoid under- or over-exposure [1]. Tacrolimus monitoring is routinely based on trough level measurement [2], while the average inter-dose exposure measured as the area under the curve (AUC) has been consensually recommended as the best marker for tacrolimus dose adjustment [3]. However, routine measurement of inter-dose AUC is difficult using conventional non-compartmental methods owing to the need for a large number of samples, and even more so for once-daily formulations. The a posteriori Bayesian estimation method allows estimation of the inter-dose AUC using population pharmacokinetic (POPPK) models associated with a limited number of blood samples, and sometimes demographic characteristics as covariates, in individual patients. Most of the POPPK algorithms available involve a parametric approach, based on the hypothesis of a normal or log-normal distribution of the pharmacokinetic (PK) parameters.
Pmetrics, the R interface for NPAG (Non-Parametric Adaptive Grid) proposes a non-parametric approach with no a priori hypothesis regarding the distribution of PK parameters and, while it is harder to conceptualise, it can theoretically catch outliers better than the parametric approach [4]. While the pharmacokinetics of the previously approved twice-daily (Tac BID, Prograf® Astellas Pharma Inc., Tokyo, Japan) or once-daily (Tac OD, Advagraf® Astellas Pharma Inc., Tokyo, Japan) tacrolimus formulations has been well established [5, 6], less is known about Envarsus® (Chiesi Farmaceutici S.p.A., Parma, Italy), another tacrolimus prolonged-release once-daily formulation (Tac OD) more recently developed by Veloxis, using their patented technology MeltDose® (Veloxis Pharmaceuticals, Hørsholm, Denmark).
The registered clinical trials conducted with Envarsus® showed increased bioavailability, lower blood peak levels [maximum concentration (C max)] and less peak-to-trough fluctuation at a lower total daily dose compared with Prograf® and Advagraf®, both in kidney and liver transplant recipients [7–9]. Envarsus® was approved in October 2014 in Europe for “the prevention of allograft rejection in adult renal or hepatic transplant patients” and for “the treatment of allograft rejection resistant to other immunosuppressive drugs in adult patients”.
In 2005, we launched the ImmunoSuppressant Bayesian dose Adjustment website, dedicated to the estimation of inter-dose AUC and dose adjustment of immunosuppressive drugs (calcineurin inhibitors, mammalian target of rapamycin inhibitors and mycophenolate mofetil) using Bayesian estimators (BE). Since then, more than 9200 requests for tacrolimus AUC estimation and individual dose adjustment have been received from over 64 different transplantation centres worldwide, leading to better knowledge of the drug’s PK behaviour in the process [10]. Currently, no PK model or BE has been reported for the new Envarsus® formulation, available in Europe for both kidney and liver transplantation while, as discussed above, PK differences are expected with respect to the Advagraf® and Prograf® formulations.
The objectives of this study were to exploit PK data of Envarsus® phase II studies in kidney and liver transplant recipients to develop POPPK models and BEs based on limited sampling strategies (LSSs) using two independent modelling approaches, to be used as tools for PK-driven dose adjustment, as was previously done with the other formulations.
2 Materials and Methods
2.1 Patients
Veloxis Pharmaceuticals provided us with the individual tacrolimus blood concentration vs. time data from two phase II, open-label, multicentre prospective US clinical trials they conducted in stable adult kidney and liver transplant patients, who were converted from Prograf® capsules twice daily to Envarsus® (so-called LCP-Tacro at the time) tablets once daily [7, 8]. These trials complied with the Declaration of Helsinki amended in Tokyo and all the patients enrolled gave their written informed consent. Data from 57 liver (113 PK profiles) and 49 kidney (97 PK profiles) graft recipients transplanted for at least 6 months and receiving oral maintenance immunosuppression with Prograf® were included in this PK study. After a first PK assessment on Prograf® (7 days after enrolment), they were switched to Envarsus® on day 8 and had two other PK assessments on days 14 and 21. At both Envarsus® PK periods, 13 blood samples were collected in ethylenediamine tetraacetic acid tubes at pre-dose and 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12, 16, 20 and 24 h after dosing. The blood samples were shipped to a central laboratory for drug measurement using a validated, liquid chromatography-tandem mass spectrometry method with a lower limit of quantitation of 0.2 ng/mL.
2.2 Pharmacokinetic Modelling
Modelling was performed using in parallel two independent approaches, involving parametric (ITSIM) and non-parametric (Pmetrics) algorithms, respectively. Data were split into a development dataset (n = 73 for kidney and n = 85 for liver) and a validation dataset (n = 24 and n = 28, respectively). Inter-occasion variability was not explored and the randomisation between development and validation datasets was based on PK profiles, considered to be all independent from the others. A previously published structural model made of a single compartment with first-order elimination and one or two absorption phases described by a sum of two gamma distributions [11] that finely fitted tacrolimus profiles in renal transplantation [12, 13] was employed.
Briefly, the PK curves are described by a Gamma absorption model involving one or two absorption phases. The absorption rate at time t is described by a sum of Gamma distributions:
with:
where F denotes the bioavailability factor, D is the administered dose, Γ is the Gamma function, a i and b i are the parameters of the distributions, r i is the dose fraction absorbed by the ith way (r 1 + r 2 + ··· + r m = 1) and m is the number of absorption phases.
The disposition kinetics, which corresponds to the impulse response I(t) of the system, is described by a sum of exponentials:
This function represents the drug concentration at time t after intravenous administration of a unit dose D 0; p represents the number of compartments (one to three).
The convolution of functions vabs and I yields the following expression:
where C(t) denotes the concentration at time t, C 0 is the residual concentration for a unit dose (1000 mg for tacrolimus) and P denotes the incomplete Gamma function as follows:
A mixed (proportional and additive) error model was used with both modelling approaches. An additive (lambda) or proportional residual error (gamma) weighting the analytical error model was also investigated with Pmetrics models. Associations between the individual PK parameters and covariates (age, sex, haematocrit, and time between the transplantation and inclusion in the study) were then screened using linear regression and graphical examination in the development dataset. When significant (p < 0.01), the covariates were introduced in the model using linear, exponential or power relationships and the relevance of each covariate in the final model was assessed using its likelihood [Bayesian Information Criteria (BIC)and Akaike Information Criteria (AIC)]. Diagnostic plots were drawn for the final models with individual predictions vs. observed concentrations and weighted residues vs. observed concentrations. The final model underwent internal evaluation using the visual predictive checks. One thousand Monte-Carlo simulations were performed for a typical patient taking the median dose, and the observations were normalised by this median dose (division of concentrations by patient dose*median dose).
2.3 Development of Bayesian Estimators
Using the population PK models obtained in the development datasets, the best LSS among all the combinations of three sampling times was determined using the multiple model optimal sampling function weighted on the AUC, provided in Pmetrics. This algorithm finds the collection times of a specified number of samples that minimise the risk of misrepresenting the patient as the wrong set of support points in the model, i.e. estimating the wrong set of PK parameters for the patient [14].
Then, the predictive performance of the BEs developed using the best LSS was evaluated in the validation groups by comparison of the AUC from time zero to 24 h (AUC0–24h) obtained using the best three-point LSS to the reference AUC0–24h obtained using the linear trapezoidal method applied to the full profiles. A calculation of the root-mean-square error (RMSE), relative bias and number of profiles from the ±20% interval compared with the reference AUC was performed. Finally, the AUCs obtained using both PK modelling approaches were compared using a Bland–Altman graph.
3 Results
3.1 Patients
Patient characteristics from the two phase II trials are described in Table 1. The PK profiles obtained using this new formulation exhibit comparable inter-individual variability with the one reported for Prograf® in the original study reports [7, 8].
Observation of PK profiles showed that some exhibited one absorption phase and others two absorption phases. Based on AIC criteria, the model with two gamma distributions for description of double-phase absorption was retained (liver: AIC for single absorption −11,085, AIC for double-phase absorption −11,116; kidney: AIC for single absorption −9397, AIC for double absorption −9425).
3.2 Model Development
A structural single-compartment model with first-order elimination and two absorption phases described by a sum of two gamma distributions was employed, together with a combined analytical error model of (0.001 mg/L + concentration × 0.1). No weighting factor (lambda or gamma) was retained with the final models, as they degraded the precision of concentration and AUC estimates. The population PK parameters of the final models obtained with the two approaches in liver and kidney transplantation, as well as the model-estimated C max and time to C max are presented in Table 2. Interestingly, the C max and time to C max values were very similar whatever the type of transplantation and the POPPK approaches with values of about 12 µg/L and 5 h, respectively. The marginal densities of the PK parameters of the non-parametric models in kidney and liver transplantation are presented in Online Resource 1. The haematocrit was significantly associated with the scale of the second gamma law b 2 = 27.7 − 0.48 × haematocrit, p = 0.00182) in liver transplant patients, but its introduction in the model increased the BIC and AIC by 100 and 95, respectively, showing degradation rather than improvement. In kidney graft recipients, sex had a significant influence on the shape of the second gamma law a 2 = 28.9 − 6.49 × sex (1 or 2), p = 0.00074), but again its introduction in the model increased the BIC and AIC, by 55 and 50, respectively. None of the other covariates tested was significantly associated with any PK parameter, whatever the modelling approach used. The scatter plots of individually predicted vs. observed concentrations showed no major bias, whatever the PK approach, and the weighted residuals were homogeneously distributed over the concentration range for both (Fig. 1). The relative bias ± standard deviation (RMSE) between observed concentrations and concentrations estimated using the final model were: −0.33 ± 6.05% (6.05%) for ITSIM and 0.34 ± 9.22% (9.22%) for Pmetrics in liver transplantation; −0.57 ± 7.38% (7.40%) and 0.64 ± 9.46% (9.48%) in kidney transplantation, respectively. The model was then evaluated using the visual predictive checks. The observed data normalised to a dose of 4 mg (median) overlaid adequately the 90% prediction intervals of the simulations for both kidney and liver transplantation groups and both POPPK approaches (Fig. 2).

Diagnostic plots: individual predicted concentrations for ITSIM and Pmetrics as function of observed concentrations in kidney transplant patients (a, b, respectively) and in liver transplant patients (c, d, respectively); and weighted residuals with ITSIM and Pmetrics as function of observed concentrations in kidney transplant patients (e, f, respectively) and in liver transplant patients (g, h, respectively)

Visual predictive check based on a normalised dose of 5 mg in kidney transplant recipients for ITSIM (a) and Pmetrics (b) and in liver transplant recipients for ITSIM (c) and Pmetrics (d)
3.3 Bayesian Estimators
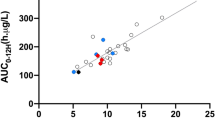
The optimal sampling times proposed by the multiple model optimal algorithm were 0, 8 and 12 h post-dose for both kidney and liver transplant groups. The BEs derived from each of the POPPK models and based on this 0, 8 and 12-h sampling schedule yielded accurate estimation of tacrolimus AUC0–24h in the validation dataset (Table 3). Random examples of profiles modelled using each method in kidney and liver transplantation are presented in Fig. 3. The bias and RMSE were always lower with ITSIM, as was the number of poorly estimated AUCs. Finally, the Bland–Altman plots of the differences between the three-point AUC estimates obtained with Pmetrics and ITSIM are presented in Fig. 4, separately for liver and kidney transplant patients, showing up to 50% difference in a few cases [mean difference ± standard deviation (minimum; maximum): kidney = −0.005 ± 0.038 (−0.112; 0.0802) mg*h/L; and liver = 0.008 ± 0.020 (−0.015; 0.095) mg*h/L] It corresponded to one difference out of the 95% confidence interval in liver transplant patients and two in kidney transplant patients (one above the upper limit and one below the lower limit of the 95% confidence interval).

Random examples of individual profiles for ITSIM and Pmetrics, in kidney transplant patients (a, b, respectively) and in liver transplant patients (c, d, respectively). The black lines are the model predicted curve and the grey lines are the observed data

Bland–Altman plot of the differences between the three-point area under the curve (AUC) estimates obtained using ITSIM and Pmetrics. SD standard deviation
4 Discussion
In this study ancillary to two phase II clinical trials of the new once-daily, prolonged-release tacrolimus formulation Envarsus®, one in liver and one in kidney stable adult transplant recipients, we developed POPPK models and BEs with their corresponding best LSS, to accurately estimate tacrolimus AUC0–24h using only three blood samples. These models and estimators were developed using in parallel two independent POPPK approaches, one parametric developed in-house and used for the expert system ImmunoSuppressant Bayesian dose Adjustment (https://pharmaco.chu-limoges.fr), and the other a shareware characterised by its non-parametric approach (http://www.lapk.org/pmetrics.php).
As expected, the coefficients of variation of the PK parameters obtained using the non-parametric approaches were wider, which is consistent with the fact that non-parametric modelling is based on the discrete probability of each parameter rather than on the assumption of their normal distribution [15, 16]. Similarly, the individual prediction vs. observed concentration graph showed three outliers with ITSIM that were not observed with Pmetrics. Two of them corresponded to the highest concentrations observed at the peak in a single kidney transplant recipient. Although the parametric model underestimated in some patients the first peak, the AUCs were well estimated in most cases, with only a few patients from the ±20% interval when comparing estimated and reference AUCs. However, in this study, the bias and RMSE of AUC estimates obtained with ITSIM were smaller than those with Pmetrics, especially in kidney transplant recipients. The AUC differences between the two approaches were generally acceptable, although they reached almost 50% in a few cases (Fig. 4). However, combining two independent modelling approaches may allow a decrease in the error in AUC estimation, especially in the case of discordant results as previously shown for mycophenolate mofetil in heart transplant patients [17] or cyclosporine in haematopoietic stem cell transplant patients [18].
Very interestingly, the PK parameters obtained here using ITSIM in kidney transplant patients are significantly different (t-test) compared with those previously obtained using exactly the same model in another population of kidney transplant recipients for the other once-daily tacrolimus formulation Advagraf® [13]. As a consequence, while we were able to propose a convenient and efficient LSS within the first 3 h post-dose (0, 1 and 3 h) for Advagraf®, all the convenient LSSs for Envarsus® included later sampling times, the best being 0, 8 and 12 h. This LSS is more difficult to apply in routine practice, but dried blood spot sampling by patients at home is increasingly employed [19], which should render this LSS and AUC0–24h BE feasible. Of note, population pharmacokinetics and BE are flexible with respect to sampling times, meaning that even if samples are taken at (slightly) different times than those scheduled and on condition that the exact times are known, the inter-dose AUC can still be estimated accurately.
This study has however some limitations. First, it was a switch study that was performed in stable kidney and liver transplant recipients more than 6 months after transplantation. Owing to the changes in tacrolimus clearance, the model and LSS developed here may not be applicable in patients receiving tacrolimus-Envarsus® de novo. Second, only a few covariates and especially no pharmacogenetic data were available [in particular for the cytochrome P450 (CYP)3A5 and CYP3A4 genotypes]. The influence of CYP3A5 on tacrolimus clearance and trough level is well established [20]. However, covariates are most useful in cases of simulation, or for estimating the first dose to be given to individual patients, i.e. only when no a posteriori data are available. In the case of BE using a LSS, most of the information is carried by the a posteriori data (i.e. concentrations) themselves if they are in sufficient number (i.e. a CYP3A5 expressor will have lower concentrations than a non-expressor). In this case, covariates will lead to an increase in the number of parameters to estimate, which may be of limited benefit in terms of accuracy, as is obviously the case here.
5 Conclusion
POPPK models and BEs for Envarsus® in adult kidney or liver transplant patients will help clinicians individualise the drug dose. The tools developed with ITSIM are now available on the ImmunoSuppressant Bayesian dose Adjustment website (https://pharmaco.chu-limoges.fr), while those developed with Pmetrics can be provided for research purposes upon request.
References
Venkataramanan R, Swaminathan A, Prasad T, et al. Clinical pharmacokinetics of tacrolimus. Clin Pharmacokinet. 1995;29:404–30.
Laskow DA, Vincenti F, Neylan JF, et al. An open-label, concentration-ranging trial of FK506 in primary kidney transplantation: a report of the United States Multicenter FK506 Kidney Transplant Group. Transplantation. 1996;62:900–5.
Wallemacq P, Armstrong VW, Brunet M, et al. Opportunities to optimize tacrolimus therapy in solid organ transplantation: report of the European consensus conference. Ther Drug Monit. 2009;31:139–52.
Neely MN, van Guilder MG, Yamada WM, et al. Accurate detection of outliers and subpopulations with Pmetrics, a nonparametric and parametric pharmacometric modeling and simulation package for R. Ther Drug Monit. 2012;34:467–76.
Staatz CE, Willis C, Taylor PJ, Tett SE. Population pharmacokinetics of tacrolimus in adult kidney transplant recipients. Clin Pharmacol Ther. 2002;72:660–9.
Staatz CE, Tett SE. Clinical pharmacokinetics of once-daily tacrolimus in solid-organ transplant patients. Clin Pharmacokinet. 2015;54:993–1025.
Gaber AO, Alloway RR, Bodziak K, et al. Conversion from twice-daily tacrolimus capsules to once-daily extended-release tacrolimus (LCPT): a phase 2 trial of stable renal transplant recipients. Transplantation. 2013;96:191–7.
Alloway RR, Eckhoff DE, Washburn WK, Teperman LW. Conversion from twice daily tacrolimus capsules to once daily extended-release tacrolimus (LCP-Tacro): phase 2 trial of stable liver transplant recipients. Liver Transpl. 2014;20:564–75.
Tremblay S, Nigro V, Weinberg J, et al. A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (Tacrolimus) Formulations (ASTCOFF): an open-label, prospective, randomized, two-arm, three-period crossover study. Am J Transplant. 2017;17(2):432–42.
Saint-Marcoux F, Woillard J-B, Jurado C, Marquet P. Lessons from routine dose adjustment of tacrolimus in renal transplant patients based on global exposure. Ther Drug Monit. 2013;35:322–7.
Prémaud A, Debord J, Rousseau A, et al. A double absorption-phase model adequately describes mycophenolic acid plasma profiles in de novo renal transplant recipients given oral mycophenolate mofetil. Clin Pharmacokinet. 2005;44:837–47.
Saint-Marcoux F, Knoop C, Debord J, et al. Pharmacokinetic study of tacrolimus in cystic fibrosis and non-cystic fibrosis lung transplant patients and design of Bayesian estimators using limited sampling strategies. Clin Pharmacokinet. 2005;44:1317–28.
Saint-Marcoux F, Debord J, Undre N, et al. Pharmacokinetic modeling and development of Bayesian estimators in kidney transplant patients receiving the tacrolimus once-daily formulation. Ther Drug Monit. 2010;32:129–35.
Bayard DS, Neely M. Experiment design for nonparametric models based on minimizing Bayes Risk: application to voriconazole. J Pharmacokinet Pharmacodyn. 2016. doi:10.1007/s10928-016-9498-5
Bustad A, Terziivanov D, Leary R, et al. Parametric and nonparametric population methods: their comparative performance in analysing a clinical dataset and two Monte Carlo simulation studies. Clin Pharmacokinet. 2006;45:365–83.
Prémaud A, Weber LT, Tönshoff B, et al. Population pharmacokinetics of mycophenolic acid in pediatric renal transplant patients using parametric and nonparametric approaches. Pharmacol Res. 2011;63:216–24.
Woillard J-B, Saint-Marcoux F, Monchaud C, et al. Mycophenolic mofetil optimized pharmacokinetic modelling, and exposure-effect associations in adult heart transplant recipients. Pharmacol Res. 2015;99:308–15.
Woillard J-B, Lebreton V, Neely M, et al. Pharmacokinetic tools for the dose adjustment of ciclosporin in haematopoietic stem cell transplant patients. Br J Clin Pharmacol. 2014;78:836–46.
Koop DR, Bleyle LA, Munar M, et al. Analysis of tacrolimus and creatinine from a single dried blood spot using liquid chromatography tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci. 2013;926:54–61.
Hesselink DA, Bouamar R, Elens L, et al. The role of pharmacogenetics in the disposition of and response to tacrolimus in solid organ transplantation. Clin Pharmacokinet. 2014;53:123–39.
Acknowledgements
The authors gratefully thank Mrs. Karen Poole for manuscript editing, and Veloxis and Chiesi for providing the phase II pharmacokinetic data and for funding this pharmacokinetic analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J.-B. Woillard have no conflict of interest. J. Debord have no conflict of interest. C. Monchaud have no conflict of interest. F. S. Marcoux have no conflict of interest. Pierre Marquet has been a member of scientific boards for, and received funding for this study from, Chiesi France.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Woillard, JB., Debord, J., Monchaud, C. et al. Population Pharmacokinetics and Bayesian Estimators for Refined Dose Adjustment of a New Tacrolimus Formulation in Kidney and Liver Transplant Patients. Clin Pharmacokinet 56, 1491–1498 (2017). https://doi.org/10.1007/s40262-017-0533-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-017-0533-5