
Abstract
Purpose
This study investigated effects of 1α,25-dihydroxyvitamin D3 [1,25(OH)2D3] on biodistribution and pharmacokinetics of L-carnitine and creatinine as organic cation/carnitine transporter 2 (OCTN2) and organic cation transporter 2 (OCT2) biomarkers, respectively, together with mRNA expressional changes.
Methods
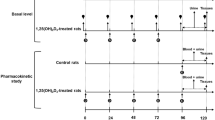
After four consecutive days of pretreatment with 1,25(OH)2D3 (2.56 nmol/kg/day), plasma, urine, and tissues were collected for analysis of endogenous L-carnitine and creatinine basal levels, or rats were intravenously administered exogenous L-carnitine (50 mg/kg). The selected tissues were subjected to analysis of rOCTN2 and rOCT2 gene expression using real-time quantitative polymerase chain reaction. The quantification of L-carnitine and creatinine was performed with liquid chromatography-tandem mass spectrometry.
Results
1,25(OH)2D3-treated rats exhibited decreased rOCTN2 mRNA expression in the liver, kidney, spleen, and brain, and decreased rOCT2 mRNA expression in the kidney. L-carnitine levels indicated that basal plasma abundance in the 1,25(OH)2D3-treated group elevated, whereas the tissue-plasma partition coefficient dropped in all tissues and the urine level also reduced. Exogenous L-carnitine pharmacokinetics were consistent with the endogenous level, with a significant rise in area under the curve and significant decreases in renal clearance and volume of distribution at steady state in the group treated with 1,25(OH)2D3. Additionally, the significant increase in plasma levels and decrease in renal clearance of creatinine were likely due to decreased OCT2 function.
Conclusion
Our observations suggest the risk of co-administering 1,25(OH)2D3 with OCT2 and/or OCTN2 substrates. Moreover, this study confirmed that L-carnitine and creatinine are sensitive endogenous biomarkers of OCTN2- and OCT2-mediated drug-drug interactions, respectively.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Membrane transporters are crucial for the uptake, distribution, metabolism and excretion of both endogenous and exogenous substances (Giacomini and Huang 2013; Lin et al. 2015). Expressional and/or functional changes in drug transporters are among the most important factors that significantly influence the pharmacokinetic and pharmacodynamic properties of drug substrates (Lin et al. 2015; Czuba et al. 2018). To ensure safety during polypharmacy in clinical practice, it is necessary to evaluate transporter-mediated drug-drug interactions (DDIs) during new drug development (Giacomini and Huang 2013). The potential risk associated with a drug candidate as a human transporter inhibitor was evaluated in in vitro transporter inhibition studies (Volpe 2016). While in vitro data are commonly employed to assess the potential for DDI in patients, it is important to acknowledge many limitations. These limitations encompass significant heterogeneity between different experimental systems and laboratories, as well as a lack of trust in extrapolating findings from in vitro to in vivo (Elsby et al. 2022). Thus, regulatory agencies, such as the United States Food and Drug Administration (US FDA), mandate that sponsors of new drug applications conduct clinical pharmacokinetic DDI studies to determine the impact of new drug candidates on concurrently administered drugs as well as the reciprocal effect of these drugs on the new candidates. This requirement is particularly applicable when the new drug candidates demonstrate evident DDI potential in vitro. Regulatory guidance documents are cautious regarding the prevention of false-negative data and require additional clinical DDI studies (Katz 2004).
Over the past several years, various endogenous substrates of transporters have been identified as possible biomarkers for predicting functional changes in drug transporters and possible DDIs that may arise during the early stage of pharmaceutical development (Chu et al. 2018). Analyzing the effects of transporter inhibitors on the exposure of these endogenous biomarkers in human plasma or urine is considered as an alternate method to evaluate the DDIs possibility of new drug candidates in vivo. These biomarker-driven DDI studies have been implemented in both preclinical and clinical research, with the expectation that they can be considered as predictive techniques for prospective DDI studies (Chu et al. 2017; Müller et al. 2018; Li et al. 2021). Therefore, the identification of endogenous biomarkers in plasma and urine is gaining interest due to their potential utility as early predictors of transporter-mediated DDIs (Giacomini and Huang 2013; Chu et al. 2018; Mochizuki et al. 2021).
Fat-soluble vitamin D3 is essential for calcium absorption and proper bone development (Robien et al. 2013; Choi et al. 2020). It is involved in cell division, cellular differentiation, and the regulation of inflammatory responses (Guillot et al. 2010; Wang et al. 2012). Additionally, it is used to treat various autoimmune disorders (Schoindre et al. 2012). The active form of vitamin D3 is 1α,25-dihydroxyvitamin D3 (1,25(OH)2D3, commonly known as calcitriol), which acts as a ligand for the vitamin D receptor (VDR) (Haussler et al. 1998). Owing to its beneficial effects, vitamin D3 or 1,25(OH)2D3 is frequently used as medicines and/or supplements. Consequently, their interactions with other medications have gained significant attention. Upon binding to VDR, 1,25(OH)2D3 regulates the expression of various transporters, receptors, and metabolic enzymes via transcriptional regulation of target genes (Wang et al. 2012; Gui et al. 2017; Doan et al. 2020; Lee et al. 2022). Our previous studies have demonstrated that 1,25(OH)2D3 alters the expression levels of several drug transporters, thereby altering the pharmacokinetics of drug substrates. For instance, administration of 1,25(OH)2D3 decreases the expression of organic anion transporters (rOAT1/OAT3) in rat kidneys, resulting in a significant reduction in cefadroxil and cefdinir renal clearance (Kim et al. 2014). In addition, 1,25(OH)2D3, which is responsible for downregulating the mRNA/protein expression of rat organic cation transporter 2 (OCT2), and rat multidrug and toxin extrusion (MATE) proteins, decreases the renal clearance of an OCT2 substrate (procainamide hydrochloride) in rats (Balla et al. 2021). Moreover, we recently investigated the effects of 1,25(OH)2D3 on mRNA expression and function of rat organic cation/carnitine transporter 1 (rOCTN1) using ergothioneine (an OCTN1 biomarker) (Vo et al. 2022). The pharmacokinetics and biodistribution of ergothioneine exhibited notable alterations in rats treated with 1,25(OH)2D3 as compared to the control group. These changes included elevated plasma concentrations of ergothioneine, increased area under the concentration-time curve (AUC), reduced total clearance (CL), and decreased volume of distribution at steady state (Vss). Additionally, a substantial reduction in the tissue-plasma partition coefficient (Kp) of ergothioneine was observed across most tissues. However, the effects of 1,25(OH)2D3 on rat organic cation/carnitine transporter 2 (rOCTN2) remain unclear.
Similar to OCTN1, OCTN2 is a member of the solute carrier family that was initially cloned from human kidneys in 1998 (Tamai et al. 1998). It is primarily localized in the kidney, skeletal muscle, lung, liver, brain, and heart. OCTN2 is primarily responsible for transporting L-carnitine (β-hydroxy-γ-trimethylaminobutyric acid) (Fig. 1A), a fundamental cofactor of fatty acid metabolism (Goa and Brogden 1987), into cells and plays a central role in the pharmacokinetics of L-carnitine (Evans and Fornasini 2003; Koepsell and Endou 2004; Kato et al. 2006). L-carnitine transforms long fatty acids into acylcarnitines, which are carried into the mitochondrial matrix and β-oxidized to create acetyl coA for energy through the Krebs cycle (Evans and Fornasini 2003; Longo et al. 2006). Owing to its usefulness as a nutritional supplement and therapeutic agent, L-carnitine has recently gained increasing interest. In addition, OCTN2 mutations decrease carnitine uptake, causing primary carnitine deficiency (Walter 1996; Tang et al. 1999). Systemic carnitine deficiency can cause encephalopathy, cardiomyopathy, and muscle weakness, leading to heart failure and death (Pauly and Pepine 2003). Given that OCTN2 plays a significant role in carnitine absorption by mouse intestinal epithelial cells, this transporter may represent a good target for examining oral OCTN2 substrates (Kato et al. 2006). In addition, human OCTN2 transports L-carnitine into adipocytes and facilitates its reabsorption into the renal proximal tubule (Evans and Fornasini 2003; Koepsell and Endou 2004). A recent study revealed that OCTN2 expression in patients with breast cancer can be used as a prognostic biomarker (Dinarvand et al. 2023). Patients with a partial OCTN2 deficiency should take carnitine or avoid OCTN2-interacting drugs (Evans and Fornasini 2003). Thus, multiple studies have recommended exogenous L-carnitine for treating carnitine insufficiency and its associated diseases (York et al. 1983; Evans and Fornasini 2003; Pauly and Pepine 2003).

Chemical structures of L-carnitine (A) and creatinine (B)
Creatinine (Fig. 1B) is produced via the non-enzymatic conversion of creatine as a byproduct of muscle metabolism (Wyss and Kaddurah-Daouk 2000). It is continuously produced and excreted in urine as the creatine level in the body remains steady. Conventional determination of creatinine levels in plasma and urine enables the calculation of endogenous creatinine clearance, which provides an estimation of glomerular filtration rate, a marker of renal function in clinical practice (Müller et al. 2018). However, inhibition of the secretion of organic cations (OCT2/MATE) in the renal tubules is often linked to a reduction in creatinine clearance or an elevation in creatinine level in plasma; therefore, plasma creatinine has been suggested as a biomarker for DDI potential during the administration of OCT2/MATE inhibitors (Urakami et al. 2004; Kimura et al. 2005; Imamura et al. 2011; Minematsu and Gaicomini 2011; Giacomini and Huang 2013; Chu et al. 2016; Zhao et al. 2016; Türk et al. 2022). Although it was previously reported that renal OCT2 expression is significantly downregulated by 1,25(OH)2D3 (Balla et al. 2021), the effect of 1,25(OH)2D3 on OCT2 function and creatinine levels has not been studied.
In the current study, we investigated the effects of 1,25(OH)2D3 on the expression and function of rOCTN2, including the biodistribution of its primary substrate, L-carnitine, as an endogenous biomarker of OCTN2. Several articles have mentioned the potential role of L-carnitine as a biomarker for OCTN2-mediated DDIs; however, limited in vivo data have been published to date (Kido et al. 2001; Li et al. 2021; McCann et al. 2021; Dinarvand et al. 2023). In addition, considering the downregulatory effect of 1,25(OH)2D3 on renal OCT2 (Balla et al. 2021), concomitant administration of 1,25(OH)2D3 and OCT2 substrates may lead to potential DDIs during renal excretion. Thus, another aim of this investigation was to examine the impact of 1,25(OH)2D3 on the biodistribution and renal excretion of endogenous creatinine, a potential OCT2 biomarker.
Materials and methods
Materials and reagents
The reagents listed below were acquired from Sigma-Aldrich (St Louis, MO, USA): 1,25(OH)2D3, isotope-labeled d3-1,25(OH)2D3, L-carnitine, creatinine, 4-phenyl-1,2,4-triazoline-3,5-dione (PTAD), metformin, formic acid, and maize oil. Acetonitrile at high-performance liquid chromatography (HPLC) grade was provided by Honeywell Burdick & Jackson (Muskegon, Michigan, USA). Additional analytical grade reagents were employed in the experiment without any subsequent purification steps.
1,25(OH)2D3 pretreatment in rats
Male Sprague-Dawley rats (7–8 weeks old, Nara Biotech, South Korea) with an average weight of 250–300 g were used in this study. Animals were acclimated to the laboratory environment for 1 week, during which they were provided with unrestricted access to both food and water and subjected to a light-dark cycle of 12 h each. The pretreatment with 1,25(OH)2D3 was conducted by the methodology described in prior studies (Maeng et al. 2011, 2019; Kim et al. 2014; Yoon et al. 2015; Balla et al. 2021; Vo et al. 2022). Briefly, two groups (1,25(OH)2D3-treated and control) were randomly divided for this study. A mixture of ethanol (2.26 µL) and filtered maize oil (5 mL) served as the injection vehicle for the control group, while a solution of 1,25(OH)2D3 in ethanol (2.26 µL) and 5 mL of filtered maize oil (1,25(OH)2D3 2.56 nmol/mL) were used for the treatment group. Rats were given intraperitoneal injections (1 mL/kg) at the same time for four days. Pharmacokinetic experiments were conducted on the fifth day (Maeng et al. 2011, 2019; Kim et al. 2014; Vo et al. 2022).
Determination of 1,25(OH)2D3 levels in rat plasma during 1,25(OH)2D3 pretreatment
1,25(OH)2D3 determination was carried out using liquid-liquid extraction (LLE), followed by a derivatization method obtained from previously published articles with slight modifications (Ding et al. 2010; Hedman et al. 2014; Fu et al. 2019). The PTAD was activated by adding acetonitrile at a concentration of 1 mg/mL. The color of the solution transformed to deep red after approximately 5 min, indicating the activation of PTAD. The activated PTAD solution was used immediately or kept on ice for no more than 30 min after activation (Hedman et al. 2014). Proteins were precipitated by adding 100 µL of working internal standard (IS) acetonitrile solution to 50 µL of rat plasma, followed by vortexing and centrifugation at 2360×g for 10 min. The supernatant was transferred to a fresh tube and the volume was reduced using a vacuum evaporator. LLE was performed by adding 250 µL ethyl acetate to the residual solution (50 µL). After vigorously shaking the samples for 10 min, they were centrifuged (590×g, 20 min) and the upper layer was separated into another tube. After completely evaporating the solvent under a stream of nitrogen, 150 µL (1 mg/mL) of activated PTAD in acetonitrile was added to the residue, vortexed, and allowed at room temperature for 1 h to complete the reaction. The sample was then transferred to another tube, evaporated using an evaporation machine, and reconstituted in 40 µL acetonitrile. For analysis, each sample was transferred to an amber-colored glass vial with a glass insert.
Real-time quantitative polymerase chain reaction
Real-time quantitative polymerase chain reaction (qPCR) was used to evaluate rOCTN2 and rOCT2 expression in selected organs. Kidney, liver, spleen, brain, muscle, lung, and heart tissues were examined, and results were normalized to glyceraldehyde 3-phosphate dehydrogenase (GAPDH) expression. After 1,25(OH)2D3 pretreatment, rats were intraperitoneally anesthetized and subsequently slaughtered to collect tissues, which were then stored at − 80 °C until analysis. The isolation of total RNA was conducted using 100 mg homogenated tissue with TRIzol® (Invitrogen, Carlsbad, CA, USA). Total RNA concentration was measured by a Thermo Scientific Nanodrop 2000c spectrophotometer (Waltham, MA, USA) at wavelengths of 260–280 nm. The synthesis of the first-strand cDNA, qPCR assays, and relative mRNA quantification were performed following methods described in previous publications (Kim et al. 2014; Yoon et al. 2015; Maeng et al. 2019; Vo et al. 2022). The employed qPCR primer sets were listed in Supplemental Table S1.
Determination of basal levels of endogenous L-carnitine and creatinine by in vivo pharmacokinetic study
The mean basal levels of L-carnitine and creatinine in plasma, urine, and tissues were determined for the control and 1,25(OH)2D3-treated rats during the entire 1,25(OH)2D3 treatment. Blood samples were obtained 30 min after injection of 1,25(OH)2D3 like the schedule of a previously published study (Vo et al. 2022). Briefly, during each sampling interval, blood sample (0.35 mL) was collected from the tail vein. Subsequently, the collected blood samples were subjected to centrifugation (4 °C, 14,000 rpm, 15 min). This centrifugation process was performed to obtain plasma samples. Urine samples were obtained within 24 h spanning from the fifth to the sixth day. On the sixth day, a collection of tissues was obtained, encompassing the kidney, liver, spleen, brain, muscle, lung and heart. Tissues were maintained at − 20 °C until further process of analysis (Vo et al. 2022).
In addition, a pharmacokinetic investigation was conducted on exogenous L-carnitine in rats, as previous articles (Kim et al. 2014; Yoon et al. 2015; Maeng et al. 2019; Balla et al. 2021; Vo et al. 2022; Lee et al. 2023). Briefly, rats were first anesthetized, then polyethylene tubing filled with 20 IU/mL heparinized saline was used to cannulate the femoral vein and artery for drug administration and blood sampling, respectively. A solution of L-carnitine in water (50 mg/mL) was prepared for injection. Rats in both the 1,25(OH)2D3 treatment and control groups were intravenously administered exogenous L-carnitine with a dose of 50 mg/kg (1 mL/kg). About 220 µL of blood samples were collected at 0, 1, 5, 15, 30, 60, 120, 240, 360, 480 and 1,440 min after drug administration. To compensate for fluid loss, equivalent quantities of 20 IU/mL heparinized normal saline were administered. Subsequently, the plasma was isolated and stored until it was ready for analysis, as described by (Vo et al. 2022). Urine samples were simultaneously collected over a 24 h period, divided into three intervals: 0–4 h, 4–8 h, and 8–24 h. Following the final blood sampling time point, the rats were promptly euthanized, and targeted tissues (as listed above) were collected. Preceding weighing and transferring to homogenate collection containers, tissues were rinsed with 0.9% w/v of NaCl to eliminate any excess blood. Upon determining their wet weights, tissues were preserved at − 80 °C.
Plasma, urine, and tissue sample preparation for analysis
Master stock solutions (50 mg/mL) of L-carnitine and creatinine were prepared in water, and then serials of standard working stock solutions were diluted in acetonitrile. To prepare the IS, a concentrated solution of metformin in dimethyl sulfoxide (1 mg/mL) was diluted with acetonitrile to obtain a working IS solution of 100 ng/mL.
The preparation of standards for biological samples (plasma, urine, and tissues) involved the addition of 10 µL of working stock solutions to 90 µL of a 2% bovine serum albumin (BSA) solution in phosphate-buffered saline (PBS), using a previously established protocol (Vo et al. 2022). The concentration range of L-carnitine and creatinine for the calibration curve were 2–5000 ng/mL, and 10–5000 ng/mL, respectively. Each sample was treated with 200 µL of the IS solution, which was subsequently vortexed (30 s) before being centrifuged (4 °C, 14,000 rpm, 15 min). A volume of 80 µL of the supernatant was obtained for liquid chromatography-tandem mass spectrometry (LC-MS/MS) analysis.
For basal L-carnitine levels quantifying, the plasma samples underwent a dilution of 10-fold, whereas the urine sample underwent a dilution of 50-fold using a 2% BSA solution. The tissue samples underwent homogenization using a two-fold volume of PBS, followed by dilution with 2% BSA. The kidney, liver, muscle and heart samples were diluted 50-fold, while the lung and spleen samples were diluted 20-fold, and the brain samples were diluted 10-fold. In the study of exogenous L-carnitine pharmacokinetics, the plasma and urine samples underwent dilution with 2% BSA at a ratio of 50-fold and 100-fold, respectively. Tissue samples were diluted with different dilution factors: the kidney and liver (1000-fold), the spleen (500-fold), and the muscle, lung, brain, and heart (100-fold). The diluted sample (100 µL) was combined with 200 µL of IS solution. The resulting mixture was subjected to vortex mixing and subsequent centrifugation to obtain the supernatant, which was then utilized for analysis using LC-MS/MS (Jin et al. 2013; Kim et al. 2014).
Quantitative LC-MS/MS analysis of L-carnitine and creatinine
Both L-carnitine and creatinine concentrations were measured by a 6490 QQQ mass spectrometer coupled with a 1290 Infinity HPLC system using an electrospray ionization (ESI+) Jet Stream ion source (Agilent Technologies, Santa Clara, CA, USA). The separation of L-carnitine, creatinine, and IS from the biological matrices was achieved by utilizing a Synergi™ 4 μm polar-RP 80 A column (Phenomenex, Torrance, CA, USA) protected by SecurityGuard™, 4.0 × 3.0 mm guard column. An isocratic condition of mobile phase including 0.1% formic acid and acetonitrile at a flow rate of 200 µL/min was used. The mobile phase ratio for each compound is shown in Supplemental Table S2. The column and autosampler had respective temperatures of 25 °C and 4 °C and the injection volume was 2 µL. The pressure of the nitrogen sheath gas was adjusted to 50 psi, while the flow rate of the gas was set to 12 L/min to nebulize the sample. The capillary voltage was adjusted to a value of 3000 V, while the gas temperature was carefully controlled and kept at a constant level of 350 °C. LC-MS/MS conditions for each compound are summarized in Supplemental Table S2. The data collection and processing were performed using Agilent Mass Hunter software (version A.06.00).
Calibration curves were determined using 1/x weighted least-squares linear regression approach to plot the target/IS peak area ratios against the target concentration. The analytical methods for L-carnitine, creatinine, and 1,25(OH)2D3-PTAD were validated in terms of selectivity and linearity as previously described (Yoon et al. 2020; Nguyen et al. 2021; Le et al. 2023) (Supplemental Figs. S1–S6).
Data analysis
Pharmacokinetic parameters, including area under the plasma concentration versus time curve from zero to infinity (AUC∞), area under the plasma concentration versus time curve from zero to the last time point (AUClast or AUC0− 24), the elimination half-life (t1/2), the mean residence time (MRT), Vss, CL, non-renal clearance (CLNR) and renal clearance (CLR), were determined using WinNonlin® 8.3 software (Pharsight Co., Mountain View, CA, USA) through the application of non-compartmental analysis.
Area under the plasma concentration-time curve ratio (AUCR), determined as the AUC ratio of the victim drug in the presence and absence of the perpetrator drug (1,25(OH)2D3) for transporters inhibition following the US FDA DDI guideline (US-FDA 2020), was calculated using Eq. (1):
Upon determining the cumulative amounts of exogenous L-carnitine in the urine for up to 24 h (Ae, ∞, i.v.), the CLR of exogenous L-carnitine was calculated using the following equation:
Renal clearance of basal L-carnitine and creatinine was calculated using Lars Jacobsson’s method for calculating renal clearance based on a solitary plasma sample, as given by the following equation:
where Q(t) is the excreted amount of tracer (i.e., basal L-carnitine and creatinine) per unit of time, and C(t) is the tracer concentration in the plasma (Jacobsson 1983).
A statistical analysis was conducted using the Student’s t-test (two-tailed) to compare the means of the control and experimental groups. A p-value < 0.05 was considered statistically significant diference. Data are presented in the form of means ± standard deviations (SDs).
Results
1,25(OH)2D3 plasma level and mRNA expressional changes of rOCTN2 and rOCT2 in 1,25(OH)2D3-treated rats
Prior to the determination of mRNA expression changes involving rOCTN2 and rOCT2 in 1,25(OH)2D3-treated rats, plasma concentration levels of 1,25(OH)2D3 were compared between control and 1,25(OH)2D3-treated rats (Fig. 2A). Thirty minutes after the first intraperitoneal injection of 1,25(OH)2D3, the plasma concentration of 1,25(OH)2D3 in the treated rats reached approximately 262.69 ± 82.92 pg/mL and subsequently returned to normal levels after 24 h. On the second day of pretreatment, comparable results were observed. However, the plasma level of 1,25(OH)2D3 after 30 min of the third injection dropped dramatically, reaching 38.83 ± 17.10 pg/mL after 30 min of the last injection (the fourth). Under normal conditions, the concentration of 1,25(OH)2D3 in rat plasma of the control group was below the lower limit of quantification (LLOQ, 10 pg/mL) of our LC-MS/MS bioanalytical method.

1,25(OH)2D3 plasma levels (A) and mRNA expressional changes involving rOCTN2 (B) and rOCT2 (C) in control and 1,25(OH)2D3-treated rats (n = 3–5). Open and closed circles/bars represent the control and 1,25(OH)2D3-treated rats, respectively. Data are presented as means ± SDs. *p < 0.05 and ** p < 0.01 compared to the control group
Using qPCR (Fig. 2B), the mRNA expression level of rOCTN2 was found to be significantly decreased in the liver, kidney, spleen, and brain of 1,25(OH)2D3-treated rats (by 56%, 53%, 77%, and 33%, respectively) (p < 0.05), whereas it was considerably increased in muscle (by 112%). Additionally, the expression levels of rOCTN2 in the lung of 1,25(OH)2D3-treated rats were lower than those in the control group, although no significant differences were observed. Given that rOCT2 mRNA is expressed at high levels in the kidney and very low levels in other tissues (Okuda et al. 1996; Slitt et al. 2002), we only investigated the expression level of rOCT2 mRNA in the kidney in the current study. qPCR results (Fig. 2C) revealed that the mRNA expression level of rOCT2 in the kidney of rats treated with 1,25(OH)2D3 was substantially reduced (by 64%) (p < 0.05) compared to that in the kidney of control rats. This result agrees with our previous observations (Balla et al. 2021).
Effects of 1,25(OH)2D3 on basal level of endogenous L-carnitine in plasma, urine, and tissues
During multiple doses of 1,25(OH)2D3 administered to rats, the basal level of endogenous L-carnitine as a rOCTN2 biomarker in plasma was investigated (Fig. 3A). The plasma level of endogenous L-carnitine in the 1,25(OH)2D3-treated group was significantly higher than that in the control group after 24 h from the first 1,25(OH)2D3 injection, and this trend was maintained until 24 h after the last injection (120 h).

Basal levels in plasma (A), cumulative amount in urine (B), renal clearance (C) and basal levels in tissues (D) of endogenous L-carnitine in control and 1,25(OH)2D3-treated rats (n = 5–6). Open and closed circles/bars represent the control and 1,25(OH)2D3-treated rats, respectively. Data are presented as means ± SDs. *p < 0.05, **p < 0.01 and *** p < 0.001 compared to the control group
In addition, both the cumulative urinary amount of L-carnitine for up to 24 h and the renal clearance of L-carnitine in 1,25(OH)2D3-treated rats decreased by 45.9% (p < 0.05) and 51.4% (p < 0.01), respectively, compared to those in the control rats (Fig. 3B and C).
Based on the concentration of L-carnitine in each tissue (Fig. 3D), endogenous L-carnitine was predominantly distributed in the heart, followed by skeletal muscle and kidney. The heart contained approximately 20-fold more L-carnitine than the brain, consistent with previous reports, which indicate that the concentration of carnitine is highest in the heart (Pearson and Tubbs 1967; Brooks and Mcintosh 1975). We hypothesized that changes in the plasma level of L-carnitine are significantly associated with the distribution and accumulation of L-carnitine in tissues expressing rOCTN2. Indeed, the Kp value of all seven tissues was found to be significantly lower after pretreatment with 1,25(OH)2D3 (Table 1), which was likely due to lower rOCTN2 expression in most tissues.
Effects of 1,25(OH)2D3 on intravenous pharmacokinetics of L-carnitine hydrochloride
We further investigated the pharmacokinetic profile of an intravenous bolus of exogenous L-carnitine in the presence of 1,25(OH)2D3 after four consecutive days of pretreatment. The plasma concentration-time profiles of L-carnitine hydrochloride following intravenous administration of 50 mg/kg in control and 1,25(OH)2D3-treated rats are presented in Fig. 4A. The plasma profile of control rats was consistent with that of a previous study, in which plasma L-carnitine concentrations declined to basal levels within 24 h after the administration of a single dose (Rebouche 2004). Notably, significantly higher plasma L-carnitine levels were observed in the 1,25(OH)2D3-treated group than in the control group. At 24 h after exogenous L-carnitine administration, the plasma level of L-carnitine in the 1,25(OH)2D3-treated group was still slightly higher than that in the control group, but no statistically significant difference was found.

Pharmacokinetic studies of L-carnitine after 50 mg/kg IV administration in control and 1,25(OH)2D3-treated rats (n = 6–7). Plasma concentration-time profiles (A), cumulative urine recovery (B), tissue levels (C) of L-carnitine. Open and closed circles/bars represent the control and 1,25(OH)2D3-treated rats, respectively. Data are presented as means ± SDs. *p < 0.05 compared to the control group
The calculated pharmacokinetic parameters (Table 2) illustrated that the AUClast and AUC∞ of L-carnitine in 1,25(OH)2D3-treated rats increased by 72.9% and 48.2%, respectively, compared to those of the control group. In addition, there was a 37.4% decrease in CL and a 35.1% decrease in CLR in 1,25(OH)2D3-treated rats compared to control rats. In addition, the volume of distribution at the Vss was significantly reduced by 50.7%. However, CLNR, t1/2, and MRT remained unaltered between two groups. In addition, the cumulative urinary recovery (% dose) of L-carnitine (Fig. 4B) remained unchanged in 1,25(OH)2D3-treated rats.
For biodistribution studies, the tissue concentration and Kp of L-carnitine in the liver, kidney, spleen, heart, lung, brain, and skeletal muscle 24 h after the administration of exogenous L-carnitine to rats are shown in Fig. 4C; Table 3, respectively. Interestingly, although L-carnitine concentration levels were observed to be only significantly decreased in the spleen and heart (Fig. 4C), significant decreases in Kp values were observed in all seven analyzed tissues (Table 3), consistent with the results for endogenous L-carnitine (Table 1).
Effects of 1,25(OH)2D3 on the basal level of endogenous creatinine in plasma, urine and tissues
The effects of 1,25(OH)2D3 on the basal level of endogenous creatinine as a rOCT2 biomarker were investigated in the same manner as that for endogenous L-carnitine. A significantly increased plasma concentration of creatinine in 1,25(OH)2D3-treated rats compared to that in control rats was observed 48 h after the first injection of 1,25(OH)2D3 (Fig. 5A). The marked elevation in plasma creatinine level for up to 24 h sampling demonstrated the effects of 1,25(OH)2D3 on the fifth day (Fig. 5B). The literature findings indicated that the concentrations of creatinine in rat plasma were approximately 20–25 µmol/L (equivalent to 2260–2830 ng/mL) (Lysne et al. 2015), which aligns with the creatinine concentrations in the control groups of our study (2420–3700 ng/mL). In addition, the creatinine clearance of rats from control group (3.05 ± 0.88 mL/min/kg) is also similar to a value reported from the previous literature (2.83 ± 0.09 mL/min/kg) (Deguchi et al. 2005). The cumulative urinary creatinine and calculated renal clearance in the 1,25(OH)2D3-treated group were significantly decreased by 27.2% (p < 0.01) and 37.7% (p < 0.05), respectively, compared to those in the control group (Fig. 5C and D). In the tissue distribution study, creatinine concentration levels were significantly decreased in the kidney and brain of the 1,25(OH)2D3-treated group compared to those in the control group (Fig. 5E), whereas Kp was significantly decreased not only in the kidney and brain, but also in the liver, heart and muscle (Table 4).

Endogenous creatinine levels in plasma collected during four consecutive days of pretreatment with 1,25(OH)2D3 (A), creatinine levels in plasma collected on the fifth day (B), cumulative urinary amount (C), renal clearance (D) and tissues levels (E) of creatinine in control and 1,25(OH)2D3-treated rats (n = 6). Open and closed circles/bars represent the control and 1,25(OH)2D3-treated rats, respectively. Data are presented as means ± SDs. *p < 0.05, **p < 0.01 and *** p < 0.001 compared to the control group
Discussion
Vitamin D3 analogs, including 1,25(OH)2D3, have been widely used as therapeutic agents or supplements in multiple-drug therapies, especially in cancer treatment. Among the membrane transporters that are highly relevant to human pathophysiology, OCTN2 and OCT2 are recognized as primary transporters for many specific first-line chemotherapeutic organic cationic drugs, such as etoposide, cisplatin and oxaliplatin (Taieb et al. 2020; Zhou et al. 2020). However, the effect of 1,25(OH)2D3 on OCTN2 and OCT2 function and their endogenous biomarkers, L-carnitine and creatinine, respectively, have not been investigated.
In the current study, to clarify the effects of 1,25(OH)2D3 on the 1,25(OH)2D3-treated and control groups, the plasma concentrations of 1,25(OH)2D3, rOCTN2 mRNA levels in seven selected tissues, and rOCT2 mRNA levels in kidney were evaluated (Fig. 2). Plasma levels of 1,25(OH)2D3 in the treated group were considerably higher than those in the control group during pretreatment. However, the concentration of 1,25(OH)2D3 gradually decreased after repeated injections, consistent with a previous publication (Brożyna et al. 2014), which revealed that elevated CYP24A1 levels via VDR activation caused a decrease in 1,25(OH)2D3 levels in the plasma. Subsequently, C24-hydroxylation, C23-hydroxylation, and C3-epimerization proceed via CYP24A1 to convert 1,25(OH)2D3 into metabolites including calcitroic acid, 1,25R(OH)2D3-26,23 S-lactone, and 3-epi-1,25(OH)2D3 (Hurst et al. 2020). Furthermore, these metabolites bind to the VDR, imitating the activity of 1,25(OH)2D3 (Shepard and Deluca 1980). Regarding mRNA expressional changes of rOCTN2 and rOCT2, rOCTN2 gene expression was noticeably affected by 1,25(OH)2D3 administration, especially in the kidney, liver, brain, spleen, and skeletal muscle. The expression of rOCT2 was also downregulated in the kidney. These changes may alter the distribution of L-carnitine and creatinine in these tissues and their systemic clearance, thereby affecting their pharmacokinetics.
Overall, the effect of 1,25(OH)2D3 on the pharmacokinetics of L-carnitine in plasma, urine, and tissue was strongly consistent between the endogenous and exogenous levels (Figs. 3, 4 and Tables 1 and 3). The increase in plasma levels (AUClast and AUC∞) of L-carnitine may be due to reduced renal clearance and tissue distribution in 1,25(OH)2D3-treated rats (Tables 1, 2 and 3; Figs. 3A, 4A). Considering that renal rOCTN2 functions as a dual-purpose transporter, facilitating both reabsorption and active secretion of L-carnitine and that a high intravenous dose of L-carnitine increases active secretion and decreases reabsorption in the kidney (Rebouche and Engel 1984; Rebouche et al. 1993; Rebouche 2004), the lower renal clearance of L-carnitine in 1,25(OH)2D3-treated rats is likely due to decreased rOCTN2 in the kidney (Fig. 2B).
When exogenous L-carnitine was administered intravenously, a substantial decrease in the Vss of L-carnitine was observed in 1,25(OH)2D3-treated rats. The significant decrease in L-carnitine distribution (i.e., Kp ratio) in all investigated organs (Tables 1 and 3) could explain the reduced Vss in the 1,25(OH)2D3-treated group. Notably, among seven analyzed tissues, the heart showed the highest percentage change in Kp (79% decrease), followed by the brain with a 72% decrease (Table 3). Interestingly, endogenous L-carnitine levels were higher in the heart than in other tissues (Fig. 3D), suggesting the potential importance of L-carnitine in the heart. Indeed, it has been reported that OCTN2 expressed in the cardiac sarcolemma is responsible for the majority of carnitine transport into the heart (Iwata et al. 2008). Additional evidence strongly suggests that a decrease in carnitine levels in cardiac muscle cells caused by OCTN2 deficiency or suppression of OCTN2 could lead to cardiomyopathy or death from heart failure (Miyagawa et al. 1995; Kuwajima et al. 1998). OCTN2 is expressed not only in the brain but also in the blood-brain barrier (BBB) and numerous parts of the central nervous system (CNS). It plays a crucial role in the CNS and belongs to the four essential enzymes for fatty acid oxidation (carnitine palmitoyltransferase 1 (CPT1), carnitine palmitoyltransferase 2 (CPT2) and two acyl-CoA dehydrogenases specialized for either long- or medium-chain acyl-CoAs) (Jernberg et al. 2017). A case study conducted in 2018 found that high-dose L-carnitine alleviated attention-deficit/hyperactivity disorder (ADHD) symptoms in a patient with OCTN2 deficiency (Lamhonwah et al. 2018). Another study revealed that carnitine supplementation is associated with an improvement in non-dysmorphic autism, which may be related to a deletion in exon 2 of the gene encoding 6-N-trimethyllysine dioxygenase, the initial enzyme in the carnitine biosynthesis process (Celestino-Soper et al. 2012). Therefore, the administration of 1,25(OH)2D3 may reduce the levels of L-carnitine accumulated in various tissues, especially in the heart and brain, resulting in side effects in these organs. However, the administration of 1,25(OH)2D3 resulted in a substantial elevation in the mRNA expression levels of rOCTN2 in the muscle (Fig. 2B). Nevertheless, the Kp value of L-carnitine in the muscle of the rats treated with 1,25(OH)2D3 exhibited a notable decrease (Fig. 3D; Tables 1 and 3). The underlying cause of this discrepancy has yet to be fully elucidated in this study. Additional research should be undertaken to provide further clarification on the outcomes of this phenomenon in relation to muscle.
In addition, the effect of 1,25(OH)2D3 on creatinine, the endogenous biomarker of OCT2, was examined. The downregulation of renal rOCT2 mRNA expression levels (Fig. 2C), consistent with a previous observation (Balla et al. 2021), might cause reduced creatinine renal clearance (Fig. 5D), consequently leading to a dramatic increase in creatinine plasma levels (Fig. 5A and B) and a decrease in tissue accumulation (Fig. 5E; Table 4) in 1,25(OH)2D3-treated rats. The increase in plasma creatinine levels in the 1,25(OH)2D3-treated group was consistent with a previous study, in which short-term VDR activation increased serum creatinine levels (Agarwal et al. 2011).
In comparison with our previous report that revealed the impact of 1,25(OH)2D3 treatment on rOCT2 function and its substrate, procainamide (Balla et al. 2021), the present study demonstrated the feasibility of using creatinine as an OCT2 biomarker in 1,25(OH)2D3-treated rats. In terms of DDIs, by calculating AUCR value, we found that the AUCR of procainamide and creatinine was 1.422 and 1.488, respectively, suggesting that the effect of 1,25(OH)2D3 on creatinine is quite similar to that of 1,25(OH)2D3 on procainamide, a well-known substrate of OCT2. In other words, our findings strongly confirm that creatinine is a sensitive biomarker for OCT2-mediated DDIs.
There was a fluctuation in creatinine plasma level for 24 h sampling (Fig. 5B), likely due to the circadian rhythm of creatinine in vivo (Thorpe et al. 2012). In fact, creatinine levels varied over the light-dark cycle and were significantly higher around the dark phase, likely related to changes in muscular activity, drinking and urination. As creatinine is a byproduct of creatine in the process of muscle metabolism, the significant decrease in creatinine accumulation in skeletal muscles in the 1,25(OH)2D3-treated group (Table 4) supports the hypothesis that VDR activation prevents muscle atrophy (Bertoli et al. 1990; Weir 2011). The results regarding muscles also implied the importance of dose control of vitamin D3 analogs, since an appropriate dose can prevent muscle loss (Bertoli et al. 1990; Weir 2011) whereas overdose administration can lead to muscle weakness due to vitamin D toxicity (Jones 2008).
Recently, the use of cocktails of drugs in polypharmacy for patients with cancer has received increasing attention. Vitamin D3 analogs are usually prescribed in combination with numerous therapeutic agents such as cisplatin and oxaliplatin. Cisplatin is associated with excessive urinary loss of L-carnitine, which is dependent on the renal tubular uptake of cisplatin by Oct2 in mice and is related to the downregulation of the luminal carnitine transporter Octn2 (Lancaster et al. 2010). Oxaliplatin, another platinum-based chemotherapeutic agent used to treat carcinoma of the rectum or stage III colon cancer, is a well-known substrate for both OCT2 and OCTN2 (Jong et al. 2011; Motohashi and Inui 2013). This evidence in animal models is useful for linking the relative activities of the OCT2 and OCTN2 transporters, which may also be applicable to humans. In this study, we determined the effect of 1,25(OH)2D3 on the pharmacokinetics of the endogenous biomarkers creatinine (rOCT2) and L-carnitine (rOCTN2). Based on these results using biomarkers of OCT2 and OCTN2, it could be expected that the pharmacokinetics of OCT2 and OCTN2 substrates (i.e., cisplatin and oxaliplatin) may be altered in the presence of 1,25(OH)2D3. Therefore, to improve their effectiveness and safety surveillance, it is worth considering dosing regimen adjustment and therapeutic drug monitoring of anticancer agents co-administered with 1,25(OH)2D3 in humans.
Conclusion
This is the first study to examine the biodistribution and pharmacokinetics of L-carnitine, a known biomarker of the OCTN2 transporter, in the presence of 1,25(OH)2D3 in rats. 1,25(OH)2D3 treatment demonstrated decreased rOCTN2 expression and functional activity, resulting in higher plasma L-carnitine levels, decreased renal clearance, and decreased L-carnitine tissue distribution. In addition, we investigated the downregulation of rOCT2 gene expression and function by 1,25(OH)2D3 to increase serum creatinine levels, lower renal clearance of creatinine and reduce creatinine distribution in the kidney and other tissues. The present study, which uses biomarkers, may attract attention due to the prevalent use of vitamin D3 in combination with other pharmaceuticals for therapeutic purposes, necessitating future human investigations when vitamin D3 and OCTN2- or OCT2-targeted medications are provided simultaneously. Moreover, L-carnitine and creatinine levels in plasma and urine can be used as biomarkers to predict the DDI possibility on OCTN2 and OCT2 during drug discovery and early new drug development.
References
Agarwal R, Hynson JE, Hecht TJ, Light RP, Sinha AD (2011) Short-term vitamin D receptor activation increases serum creatinine due to increased production with no effect on the glomerular filtration rate. Kidney Int 80:1073–1079
Balla A, Jeong YS, Kim HJ, Lee YJ, Chung SJ, Chae YJ, Maeng HJ (2021) Effects of 1α,25-dihydroxyvitamin D(3) on the pharmacokinetics of procainamide and its metabolite N-acetylprocainamide, organic cation transporter substrates, in rats with PBPK modeling approach. Pharmaceutics 13:1133
Bertoli M, Luisetto G, Ruffatti A, Urso M, Romagnoli G (1990) Renal function during calcitriol therapy in chronic renal failure. Clin Nephrol 33:98–102
Brooks DE, Mcintosh JE (1975) Turnover of carnitine by rat tissues. Biochem J 148:439–445
Brożyna AA, Jochymski C, Janjetovic Z, Jóźwicki W, Tuckey RC, Slominski AT (2014) CYP24A1 expression inversely correlates with Melanoma progression: clinic-pathological studies. Int J Mol Sci 15:19000–19017
Celestino-Soper PB, Violante S, Crawford EL, Luo R, Lionel AC, Delaby E, Cai G, Sadikovic B, Lee K, Lo C, Gao K, Person RE, Moss TJ, German JR, Huang N, Shinawi M, Treadwell-Deering D, Szatmari P, Roberts W, Fernandez B, Schroer RJ, Stevenson RE, Buxbaum JD, Betancur C, Scherer SW, Sanders SJ, Geschwind DH, Sutcliffe JS, Hurles ME, Wanders RJ, Shaw CA, Leal SM, Cook EH Jr, Goin-Kochel RP, Vaz FM, Beaudet AL (2012) A common X-linked inborn error of carnitine biosynthesis may be a risk factor for nondysmorphic autism. Proc Natl Acad Sci USA 109:7974–7981
Choi MS, Kim YC, Maeng HJ (2020) Therapeutic targets of vitamin D receptor ligands and their pharmacokinetic effects by modulation of transporters and metabolic enzymes. J Pharm Invest 50:1–16
Chu X, Bleasby K, Chan GH, Nunes I, Evers R (2016) The complexities of interpreting reversible elevated serum creatinine levels in drug development: does a correlation with inhibition of renal transporters exist? Drug Metab Dispos 44:1498–1509
Chu X, Chan GH, Evers R (2017) Identification of endogenous biomarkers to predict the propensity of drug candidates to cause hepatic or renal transporter-mediated drug-drug interactions. J Pharm Sci 106:2357–2367
Chu X, Liao M, Shen H, Yoshida K, Zur AA, Arya V, Galetin A, Giacomini KM, Hanna I, Kusuhara H, Lai Y, Rodrigues D, Sugiyama Y, Zamek-Gliszczynski MJ, Zhang L (2018) Clinical probes and endogenous biomarkers as substrates for transporter drug-drug interaction evaluation: perspectives from the international transporter consortium. Clin Pharmacol Ther 104:836–864
Czuba LC, Hillgren KM, Swaan PW (2018) Post-translational modifications of transporters. Pharmacol Ther 192:88–99
Deguchi T, Takemoto M, Uehara N, Lindup WE, Suenaga A, Otagiri M (2005) Renal clearance of endogenous hippurate correlates with expression levels of renal organic anion transporters in uremic rats. J Pharmacol Exp Ther 314:932–938
Dinarvand N, Karimi F, Azizi R, Rastaghi S, Sheikhi A, Pourfarzam M (2023) Evaluation of the gene encoding carnitine transporter (OCTN2/SLC22A5) expression in human Breast cancer and its association with clinicopathological characteristics. Mol Biol Rep 50:2061–2066
Ding S, Schoenmakers I, Jones K, Koulman A, Prentice A, Volmer DA (2010) Quantitative determination of vitamin D metabolites in plasma using UHPLC-MS/MS. Anal Bioanal Chem 398:779–789
Doan TNK, Vo DK, Kim H, Balla A, Lee Y, Yoon IS, Maeng HJ (2020) Differential effects of 1α,25-Dihydroxyvitamin D(3) on the expressions and functions of hepatic CYP and UGT enzymes and its pharmacokinetic consequences in vivo. Pharmaceutics 12:1129
Elsby R, Atkinson H, Butler P, Riley RJ (2022) Studying the right transporter at the right time: an in vitro strategy for assessing drug-drug interaction risk during drug discovery and development. Expert Opin Drug Metab Toxicol 18:619–655
Evans AM, Fornasini G (2003) Pharmacokinetics of L-carnitine. Clin Pharmacokinet 42:941–967
Fu X, Dolnikowski GG, Patterson WB, Dawson-Hughes B, Zheng T, Morris MC, Holland TM, Booth SL (2019) Determination of vitamin D and its metabolites in human brain using an Ultra-pressure LC-Tandem Mass Spectra Method. Curr Dev Nutr 3:nzz074
Giacomini KM, Huang SM (2013) Transporters in drug development and clinical pharmacology. Clin Pharmacol Ther 94:3–9
Goa KL, Brogden RN (1987) l-Carnitine. A preliminary review of its pharmacokinetics, and its therapeutic use in ischaemic cardiac disease and primary and secondary carnitine deficiencies in relationship to its role in fatty acid metabolism. Drugs 34:1–24
Gui B, Chen Q, Hu C, Zhu C, He G (2017) Effects of calcitriol (1, 25-dihydroxy-vitamin D3) on the inflammatory response induced by H9N2 influenza virus infection in human lung A549 epithelial cells and in mice. Virol J 14:10
Guillot X, Semerano L, Saidenberg-Kermanac’h N, Falgarone G, Boissier MC (2010) Vitamin D and inflammation. Joint Bone Spine 77:552–557
Haussler MR, Whitfield GK, Haussler CA, Hsieh JC, Thompson PD, Selznick SH, Dominguez CE, Jurutka PW (1998) The nuclear vitamin D receptor: biological and molecular regulatory properties revealed. J Bone Miner Res 13:325–349
Hedman CJ, Wiebe DA, Dey S, Plath J, Kemnitz JW, Ziegler TE (2014) Development of a sensitive LC/MS/MS method for vitamin D metabolites: 1,25 Dihydroxyvitamin D2&3 measurement using a novel derivatization agent. J Chromatogr B Analyt Technol Biomed Life Sci 953–954:62–67
Hurst EA, Homer NZ, Mellanby RJ (2020) Vitamin D metabolism and profiling in veterinary species. Metabolites 10:371
Imamura Y, Murayama N, Okudaira N, Kurihara A, Okazaki O, Izumi T, Inoue K, Yuasa H, Kusuhara H, Sugiyama Y (2011) Prediction of fluoroquinolone-induced elevation in serum creatinine levels: a case of drug-endogenous substance interaction involving the inhibition of renal secretion. Clin Pharmacol Ther 89:81–88
Iwata D, Kato Y, Wakayama T, Sai Y, Kubo Y, Iseki S, Tsuji A (2008) Involvement of carnitine/organic cation transporter OCTN2 (SLC22A5) in distribution of its substrate carnitine to the heart. Drug Metab Pharmacokinet 23:207–215
Jacobsson L (1983) A method for the calculation of renal clearance based on a single plasma sample. Clin Physiol 3:297–305
Jernberg JN, Bowman CE, Wolfgang MJ, Scafidi S (2017) Developmental regulation and localization of carnitine palmitoyltransferases (CPTs) in rat brain. J Neurochem 142:407–419
Jin HE, Kim IB, Kim CK, Maeng HJ (2013) Determination of cefdinir levels in rat plasma and urine by high-performance liquid chromatography-tandem mass spectrometry: application to pharmacokinetics after oral and intravenous administration of cefdinir. Biomed Chromatogr 27:1423–1430
Jones G (2008) Pharmacokinetics of vitamin D toxicity. Am J Clin Nutr 88:582s–586s
Jong NN, Nakanishi T, Liu JJ, Tamai I, Mckeage MJ (2011) Oxaliplatin transport mediated by organic cation/carnitine transporters OCTN1 and OCTN2 in overexpressing human embryonic kidney 293 cells and rat dorsal root ganglion neurons. J Pharmacol Exp Ther 338:537–547
Kato Y, Sugiura M, Sugiura T, Wakayama T, Kubo Y, Kobayashi D, Sai Y, Tamai I, Iseki S, Tsuji A (2006) Organic cation/carnitine transporter OCTN2 (Slc22a5) is responsible for carnitine transport across apical membranes of small intestinal epithelial cells in mouse. Mol Pharmacol 70:829–837
Katz R (2004) Biomarkers and surrogate markers: an FDA perspective. NeuroRx 1:189–195
Kido Y, Tamai I, Ohnari A, Sai Y, Kagami T, Nezu J, Nikaido H, Hashimoto N, Asano M, Tsuji A (2001) Functional relevance of carnitine transporter OCTN2 to brain distribution of L-carnitine and acetyl-L-carnitine across the blood-brain barrier. J Neurochem 79:959–969
Kim YC, Kim IB, Noh CK, Quach HP, Yoon IS, Chow ECY, Kim M, Jin HE, Cho KH, Chung SJ, Pang KS, Maeng HJ (2014) Effects of 1α,25-dihydroxyvitamin D3, the natural vitamin D receptor ligand, on the pharmacokinetics of cefdinir and cefadroxil, organic anion transporter substrates, in rat. J Pharm Sci 103:3793–3805
Kimura N, Okuda M, Inui K (2005) Metformin transport by renal basolateral organic cation transporter hOCT2. Pharm Res 22:255–259
Koepsell H, Endou H (2004) The SLC22 drug transporter family. Pflugers Arch 447:666–676
Kuwajima M, Lu K, Sei M, Ono A, Hayashi M, Ishiguro K, Ozaki K, Hotta K, Okita K, Murakami T, Miyagawa J, Narama I, Nikaido H, Hayakawa J, Nakajima H, Namba M, Hanafusa T, Matsuzawa Y, Shima K (1998) Characteristics of cardiac hypertrophy in the juvenile visceral steatosis mouse with systemic carnitine deficiency. J Mol Cell Cardiol 30:773–781
Lamhonwah AM, Barić I, Lamhonwah J, Grubić M, Tein I (2018) Attention deficit/hyperactivity disorder as an associated feature in OCTN2 deficiency with novel deletion (p.T440-Y449). Clin Case Rep 6:585–591
Lancaster CS, Hu C, Franke RM, Filipski KK, Orwick SJ, Chen Z, Zuo Z, Loos WJ, Sparreboom A (2010) Cisplatin-induced downregulation of OCTN2 affects carnitine wasting. Clin Cancer Res 16:4789–4799
Le QD, Duong VA, Lee SH, Maeng HJ (2023) Bioanalytical method validation, biopharmaceutical and pharmacokinetic evaluation of GSK-650394, a serum-and glucocorticoid-regulated kinase 1 inhibitor. Arab J Chem 16:104462
Lee SG, Cho KH, Nguyen TT, Vo DK, Chae YJ, Maeng HJ (2022) Inhibitory effect of 20(S)-protopanaxadiol on cytochrome P450: potential of its pharmacokinetic interactions in vivo. Biomed Pharmacother 153:113514
Lee SJ, Joo SA, Kim H, Lee Y, Chung SJ, Chae YJ, Maeng HJ (2023) Involvement of CYP3A4 and MDR1 in altered metabolism and transport of indinavir in 1,25(OH)(2)D(3)-treated Caco-2 cells. Eur J Pharm Sci 183:106396
Li Y, Talebi Z, Chen X, Sparreboom A, Hu S (2021) Endogenous biomarkers for SLC transporter-mediated drug-drug Interaction evaluation. Molecules 26:10
Lin L, Yee SW, Kim RB, Giacomini KM (2015) SLC transporters as therapeutic targets: emerging opportunities. Nat Rev Drug Discov 14:543–560
Longo N, Di Amat C, Pasquali M (2006) Disorders of carnitine transport and the carnitine cycle. Am J Med Genet C Semin Med Genet 142c:77–85
Lysne V, Bjørndal B, Vik R, Nordrehaug JE, Skorve J, Nygård O, Berge RK (2015) A protein extract from Chicken reduces plasma homocysteine in rats. Nutrients 7:4498–4511
Maeng HJ, Durk MR, Chow EC, Ghoneim R, Pang KS (2011) 1α,25-dihydroxyvitamin D3 on intestinal transporter function: studies with the rat everted intestinal sac. Biopharm Drug Dispos 32:112–125
Maeng HJ, Doan TNK, Yoon IS (2019) Differential regulation of intestinal and hepatic CYP3A by 1α,25-dihydroxyvitamin D(3): effects on in vivo oral absorption and disposition of buspirone in rats. Drug Dev Res 80:333–342
Mccann MR, De La Rosa G, Rosania MVGR, Stringer KA (2021) L-Carnitine and Acylcarnitines: Mitochondrial Biomarkers for Precision Medicine. Metabolites 11:1
Minematsu T, Giacomini KM (2011) Interactions of tyrosine kinase inhibitors with organic cation transporters and multidrug and toxic compound extrusion proteins. Mol Cancer Ther 10:531–539
Miyagawa J, Kuwajima M, Hanafusa T, Ozaki K, Fujimura H, Ono A, Uenaka R, Narama I, Oue T, Yamamoto K et al (1995) Mitochondrial abnormalities of muscle tissue in mice with juvenile visceral steatosis associated with systemic carnitine deficiency. Virchows Arch 426:271–279
Mochizuki T, Mizuno T, Maeda K, Kusuhara H (2021) Current progress in identifying endogenous biomarker candidates for drug transporter phenotyping and their potential application to drug development. Drug Metab Pharmacokinet 37:100358
Motohashi H, Inui K (2013) Organic cation transporter OCTs (SLC22) and MATEs (SLC47) in the human kidney. AAPS J 15:581–588
Müller F, Sharma A, König J, Fromm MF (2018) Biomarkers for in vivo assessment of transporter function. Pharmacol Rev 70:246–277
Nguyen TT, Duong VA, Vo DK, Jo J, Maeng HJ (2021) Development and validation of a bioanalytical LC-MS/MS method for simultaneous determination of Sirolimus in Porcine whole blood and lung tissue and pharmacokinetic application with coronary stents. Molecules 26:1
Okuda M, Saito H, Urakami Y, Takano M, Inui K (1996) cDNA cloning and functional expression of a novel rat kidney organic cation transporter, OCT2. Biochem Biophys Res Commun 224:500–507
Pauly DF, Pepine CJ (2003) The role of carnitine in myocardial dysfunction. Am J Kidney Dis 41:S35-43
Pearson DJ, Tubbs PK (1967) Carnitine and derivatives in rat tissues. Biochem J 105:953–963
Rebouche CJ (2004) Kinetics, pharmacokinetics, and regulation of L-carnitine and acetyl-L-carnitine metabolism. Ann N Y Acad Sci 1033:30–41
Rebouche CJ, Engel AG (1984) Kinetic compartmental analysis of carnitine metabolism in the human carnitine deficiency syndromes. Evidence for alterations in tissue carnitine transport. J Clin Invest 73:857–867
Rebouche CJ, Lombard KA, Chenard CA (1993) Renal adaptation to dietary carnitine in humans. Am J Clin Nutr 58:660–665
Robien K, Oppeneer SJ, Kelly JA, Hamilton-Reeves JM (2013) Drug-vitamin D interactions: a systematic review of the literature. Nutr Clin Pract 28:194–208
Schoindre Y, Terrier B, Kahn JE, Saadoun D, Souberbielle JC, Benveniste O, Amoura Z, Piette JC, Cacoub P, Costedoat-Chalumeau N (2012) Vitamin D and autoimmunity. First part: fundamental aspects. Rev Med Interne 33:80–86
Shepard RM, Deluca HF (1980) Plasma concentrations of vitamin D3 and its metabolites in the rat as influenced by vitamin D3 or 25-hydroxyvitamin D3 intakes. Arch Biochem Biophys 202:43–53
Slitt AL, Cherrington NJ, Hartley DP, Leazer TM, Klaassen CD (2002) Tissue distribution and renal developmental changes in rat organic cation transporter mRNA levels. Drug Metab Dispos 30:212–219
Taieb J, Prager GW, Melisi D, Westphalen CB, D’esquermes N, Ferreras A, Carrato A, Macarulla T (2020) First-line and second-line treatment of patients with metastatic pancreatic adenocarcinoma in routine clinical practice across Europe: a retrospective, observational chart review study. ESMO Open 5:1
Tamai I, Ohashi R, Nezu J, Yabuuchi H, Oku A, Shimane M, Sai Y, Tsuji A (1998) Molecular and functional identification of sodium ion-dependent, high affinity human carnitine transporter OCTN2. J Biol Chem 273:20378–20382
Tang NL, Ganapathy V, Wu X, Hui J, Seth P, Yuen PM, Wanders RJ, Fok TF, Hjelm NM (1999) Mutations of OCTN2, an organic cation/carnitine transporter, lead to deficient cellular carnitine uptake in primary carnitine deficiency. Hum Mol Genet 8:655–660
Thorpe JB, Rajabi N, Decatanzaro D (2012) Circadian rhythm and response to an acute stressor of urinary corticosterone, testosterone, and creatinine in adult male mice. Horm Metab Res 44:429–435
Türk D, Müller F, Fromm MF, Selzer D, Dallmann R, Lehr T (2022) Renal transporter-mediated drug-biomarker interactions of the endogenous substrates creatinine and N(1)-methylnicotinamide: a PBPK modeling approach. Clin Pharmacol Ther 112:687–698
Urakami Y, Kimura N, Okuda M, Inui K (2004) Creatinine transport by basolateral organic cation transporter hOCT2 in the human kidney. Pharm Res 21:976–981
US-FDA (2020) In vitro drug interaction studies-cytochrome P450 enzyme and transporter mediated drug interactions. FDA Guidline 1:1
Vo DK, Nguyen TT, Maeng HJ (2022) Effects of 1α,25-dihydroxyvitamin D(3) on the pharmacokinetics and biodistribution of ergothioneine, an endogenous organic cation/carnitine transporter 1 substrate, in rats. J Pharm Investig 52:341–351
Volpe DA (2016) Transporter assays as useful in vitro tools in drug discovery and development. Expert Opin Drug Discov 11:91–103
Walter JH (1996) L-carnitine. Arch Dis Child 74:475–478
Wang Y, Zhu J, Deluca HF (2012) Where is the vitamin D receptor? Arch Biochem Biophys 523:123–133
Weir MR (2011) Short-term effects of vitamin D receptor activation on serum creatinine, creatinine generation, and glomerular filtration. Kidney Int 80:1016–1017
Wyss M, Kaddurah-Daouk R (2000) Creatine and creatinine metabolism. Physiol Rev 80:1107–1213
Yoon IS, Son JH, Kim SB, Choi MK, Maeng HJ (2015) Effects Of 1α,25-dihydroxyvitamin D3 on intestinal absorption and disposition of adefovir dipivoxil and its metabolite, adefovir, in rats. Biol Pharm Bull 38:1732–1737
Yoon JH, Nguyen TT, Duong VA, Chun KH, Maeng HJ (2020) Determination of Kd025 (Slx-2119), a selective Rock2 inhibitor, in rat plasma by high-performance liquid chromatography-tandem mass spectrometry and its pharmacokinetic application. Molecules 25:1369
York CM, Cantrell CR, Borum PR (1983) Cardiac carnitine deficiency and altered carnitine transport in cardiomyopathic hamsters. Arch Biochem Biophys 221:526–533
Zhao Y, Liu G, Angeles A, Christopher LJ, Wang Z, Arnold ME, Shen JX (2016) A validated LC-MS/MS method for the quantitative measurement of creatinine as an endogenous biomarker in human plasma. Bioanalysis 8:1997–2005
Zhou T, Zhang Z, Luo F, Zhao Y, Hou X, Liu T, Wang K, Zhao H, Huang Y, Zhang L (2020) Comparison of First-Line treatments for patients with extensive-stage small cell Lung Cancer: a systematic review and network Meta-analysis. JAMA Netw Open 3:e2015748
Acknowledgements
This work was supported by the Gachon University Research Fund of 2020 (GCU- 202008420005) and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (NRF-2021R1F1A1060378).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
All authors (D.-K. Vo, T.-T.-L. Nguyen, and H.-J. Maeng) declare that they have no conflict of interest.
Research involving in human and animal participants
The animal investigations were conducted after receiving approval of the Institutional Animal Care and Use Committee in Gachon University (approval No. GIACUC-R2019020, July 1st, 2019).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Vo, DK., Nguyen, TTL. & Maeng, HJ. Impact of 1α,25-dihydroxyvitamin D3 on biodistribution and pharmacokinetics of L-carnitine and creatinine, organic cation/carnitine transporter 2 and organic cation transporter 2 biomarkers. J. Pharm. Investig. 54, 389–402 (2024). https://doi.org/10.1007/s40005-023-00659-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40005-023-00659-2