
Abstract
Purpose of Review
Current clinical efforts to predict and prevent preterm birth are primarily focused on the mother and have made minimal progress in improving outcomes. However, recent data indicate that paternal factors can also influence timing of birth. Herein, we will review recent human and murine data examining the contribution of the father to pregnancy outcomes with an emphasis on environmental exposures that can negatively impact fertility and the timing of birth.
Recent Findings
Human epidemiology studies now clearly indicate that a variety of paternal factors (age, race, weight, smoking status) can influence sperm quality, birth timing and, in some studies, offspring health. Utilizing a mouse model, our data have demonstrated that developmental exposure of the male to the environmental toxicant TCDD (2,3,7,8-tetrachlorodibenzo-p-dioxin) is associated with a transgenerational reduction in sperm number and quality and an increased risk of preterm birth in an unexposed partner.
Summary
Toxicant exposure history can clearly influence sperm quality in men and mice. Murine data further indicate that exposures which negatively affect sperm quality also impair placental function, potentially leading to preterm birth and other adverse outcomes. Of particular concern, these changes have been linked to epigenetic alterations within the male germ cell which can then be transmitted across multiple generations. Since it is not possible to prevent an ancestral toxicant exposure in a human population, identifying lifestyle modifications that can be implemented during the preconception period to improve sperm quality should be explored for the therapeutic potential to reduce the incidence of PTB and its sequelae.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Preterm birth (PTB), defined as spontaneous delivery prior to 37-weeks gestation, is a major health concern and, globally, impacts millions of babies and their families. Collectively, complications associated with prematurity are the leading cause of death in children less than 5 years of age. Furthermore, surviving infants often face life-long disability, including visual deficits, cerebral palsy, and diminished mental capacity [1]. Although infection during pregnancy can increase the risk of PTB, in many cases, the underlying cause of early parturition is unknown. Therefore, developing a better understanding of the factors that contribute to PTB is imperative if we are to make major strides in reducing this outcome.
Each year, the March of Dimes releases its Preterm Birth Report Card, detailing current statistics across the USA. The most recent report indicates that 9.93% of babies in the USA are born preterm, an increase over the previous 2 years [2]. The report also details the persistence of racial and geographic disparities in the incidence of PTB but offered little insight with regard to possible mechanisms. Shortly after the March of Dimes report was published, another study presented evidence of the continued decline in human sperm counts and suggested that exposure to environmental toxicants was a likely contributing factor [3•]. At first glance, these two reports appear to be unrelated. But are they? As will be discussed herein, our data, using a mouse model, have demonstrated that poor sperm quality due to a history of direct or ancestral exposure to the environmental toxicant TCDD (2,3,7,8-tetrachlorodibenzo-p-dioxin) can be directly linked to PTB in his unexposed partner [4, 5].
For decades, environmental toxicants have been known to contaminate industrial environments and to have a potentially negative effect on human and animal populations. TCDD and related organochlorines represent just one family of toxicants among thousands of manmade chemicals present within our environment. Current regulations do not require rigorous safety testing [6]; thus, human health effects are identified subsequent to their introduction into the environment. Over the last several decades, a number of these manmade environmental contaminants have been identified as endocrine disruptors (EDCs). Exposure to EDCs, especially during development, alters tissue response to sex steroids and can compromise not only adult reproductive health but can also promote numerous diseases including cancer (reviewed in [7]). In our laboratory, we have used TCDD as a representative EDC to explore the potential contribution of developmental exposure to the risk of PTB in adulthood.
Our murine studies demonstrated that developmental TCDD exposure of either males or females led to a significant risk of a subsequent adult pregnancy ending in PTB [5]. Interestingly, pups sired by a father with a history of TCDD exposure also exhibited intrauterine growth restriction (IUGR), which was linked to placental dysfunction and alterations in expression of Igf2 [8, 9]. Placental dysfunction, prematurity, and offspring IUGR persisted across several generations without additional TCDD exposure, suggesting toxicant-associated epigenetic changes occurred within the male germline.
Epigenetic marking of DNA is a mechanism by which gene expression can be altered without a change in the DNA sequence (rev by [7, 10, 11]. Epigenetic marking of DNA is an important process by which fetal cells are directed to differentiate into the different organ systems despite each cell possessing identical DNA. Lifestyle choices, diet, and environmental exposures can also contribute to epigenetic alterations which accumulate over time and contribute to age-related changes and disease susceptibility. Although these marks are stable, epigenetic changes to somatic cells are not inherited by the next generation. In contrast, epigenetic marks occurring within the germ cell can be inherited and can impact offspring health [11].
Although several studies in rodents and humans demonstrate alterations to the sperm epigenome can negatively impact pregnancy outcomes and offspring health [9, 12,13,14,15], currently, clinical efforts to prevent adverse pregnancy outcomes focus nearly exclusively on the mother. However, studies described herein suggest that initiating preventive measures in mid-gestation is inadequate because this approach cannot impact development of the placenta, which is heavily influenced by paternal genes [16,17,18]. Furthermore, we and others have identified inflammation as an important mediator of placental function related to parturition (both term and preterm) [5, 19]. Specifically, inflammation promotes breakdown of the fetal membranes, an early event associated with timing of delivery [20]. Using our murine model, we have demonstrated that the paternal-derived risk of toxicant-associated PTB could be eliminated when male mice were provided an anti-inflammatory preconception diet containing fish oil. Although numerous studies have examined the ability of fish oil supplementation to increase gestation length in women at risk of PTB, results have not consistently demonstrated a clear benefit [21,22,23]. However, none of these studies initiated treatments prior to pregnancy or included both parents. Although additional laboratory-based and clinical studies are needed, current data indicate that inclusion of the father in efforts to improve pregnancy outcomes is warranted.
Paternal Factors and Adverse Pregnancy Outcomes in Humans
Multiple maternal factors, including age, smoking status, and race have long been known to contribute to the risk of PTB and other adverse outcomes; however, women with no known risk factors can also deliver early [2]. Recent epidemiological studies now suggest that these same maternal-derived clinical parameters, arising on the paternal side, can also negatively influence pregnancy outcomes in their partners (reviewed in [24•, 25] Table 1). Specifically, both younger (< 25) and older (40+ years) fathers confer an increased risk of PTB and low birthweight to their children [26, 27] while the latter group had partners that more frequently developed gestational diabetes [27]. More than a decade ago, Muglia and colleagues were the first to report an increased risk of PTB associated with a Black paternal partner [28]. Although an unexpected finding at that time, numerous studies have since confirmed and expanded Muglia’s original report [29, 30]. For example, Li et al. [31] correlated the birth outcomes of singleton babies born in the USA between 1989 and 2013 with the race and ethnicity of both parents. This broad ethnicity study found that compared to all other races/ethnicities, non-Hispanic black fathers conferred the greatest risk of PTB to their partners. Significantly, the contribution of a non-Hispanic black father to risk of PTB was even greater when his partner was also non-Hispanic black.
Paternal lifestyle factors have also recently been examined for the potential to influence timing of delivery and child health (for example, [25, 32, 42]). Multiple studies indicate that paternal obesity impairs fertility, with some studies additionally finding that reproductively successful obese men have children with compromised health (reviewed by [33, 34•]). For example, Soubry and colleagues identified hypomethylation of IGF2 in infants born to obese fathers, an epigenetic modification previously linked to intrauterine growth restriction (IUGR) [37,38,39]. Furthermore, paternal obesity has also been found to increase the risk of PTB, preeclampsia, and small for gestational age, independent of whether or not the mother was also obese [35, 36, 40, 41, 45]. Like obesity, paternal smoking is known to negatively affect fetal growth [46], potentially leading to IUGR [47, 48], however the influence of paternal smoking on gestation length is less clear. Although several studies examining the impact of paternal smoking on gestation length identified only a synergistic effect with maternal risk factors [49, 50], a recent meta-analysis of 24 studies examining “passive” smoking revealed a significant influence of exposure to second hand smoke on PTB risk [51]. Interestingly, a large study from researchers in China found that the risk of spontaneous miscarriage was also significantly increased in association with paternal smoking [52].
Consequences of Human Exposure to TCDD
Studies described above taken with other recent findings demonstrate the important role of the father in contributing to not only pregnancy establishment and maintenance but also fetal development and future health. In addition to these lifestyle factors, unintentional paternal toxicant exposure may also influence pregnancy outcomes. Unfortunately, humans and other animals are exposed to a wide array of manmade environmental toxicants, many of which act as endocrine disrupting compounds (EDCs, [53]). Indeed, the US National Toxicology Program estimates that more than 80,000 manmade chemicals are present within our environment, most of which have not undergone testing to determine their potential risk to human health. Furthermore, many environmental toxicants are slow to degrade, enter our food chain, and accumulate in human adipose tissues. Not surprisingly, ingestion of contaminated food is the primary source of exposure for most human and animal populations [54, 55]. Although epidemiological evidence supports a role for exposure to environmental EDCs in increasing a woman’s risk of delivering preterm (reviewed in [56]), examination of the paternal partner has largely been neglected. For example, a significant increased risk for PTB was observed in women living within 4 km of a municipal solid waste incinerator [57], suggesting exposure to airborne toxicants adversely affected pregnancy outcomes. It is likely that the male partners of these women also resided near the incinerator; yet, the potential influence of his exposure to pregnancy outcome was not considered.
Of the numerous toxicants produced by combustion and/or manufacturing processes, compounds that bind the aryl hydrocarbon receptor (AhR) are of particular concern. When activated by endogenous and dietary ligands, the AhR is an important regulator of the normal immune and reproductive responses in both males and females [58,59,60]. However, binding of the AhR to environmental toxicants such as 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) can have significant, and multi-generational adverse consequences. TCDD, which has frequently been described as the most toxic manmade compound, has no commercial value, but is produced as an unwanted by-product of numerous manufacturing processes. Additionally, TCDD and other environmental are present in cigarette smoke, car exhaust, medical waste incinerators and smoke arising from forest fires [4]. Thus, chronic, low-dose exposure to TCDD and related compounds is common and difficult to completely avoid. Murkerjee [61] reported that within the general North American population, levels of TCDD average 5–10 ppt; however, women in industrialized countries exhibit higher levels (20–27 ppt). Adverse human health effects have been observed at < 68 ppt; however, Edmond et al. [62] state, “epidemiologic data suggest that there is little or no margin of exposure for humans” with regard to the adverse effects of developmental exposures.
Relevant to the current review, several large-scale population exposures to TCDD have occurred and demonstrate numerous long-term consequences of such exposure (reviewed in [63]). For example, in July of 1976, an explosion at the Icmesa chemical company, located near Seveso, Italy, resulted in the release of a toxic cloud heavily contaminated with TCDD. Within the 17,000 residents of Seveso itself, numerous people fell ill and there was a notable change in the male/female ratio in children conceived immediately after the explosion [64]. In the years since the accident, the health of the Seveso population, as well as the approximately 100,000 residents in neighboring towns, has been closely monitored (rev by [65]). Among the numerous studies arising from this population, Mocarelli and colleagues examined the sperm quality of young men born in Seveso shortly after the explosion compared to an age-matched, unexposed cohort [66]. Their analysis revealed that men in the exposed group exhibited lower sperm numbers, reduced progressive motility as well as a reduction in total motile count compared to the unexposed controls. They concluded that developmental exposure of males to TCDD permanently reduces sperm quality [66, 67]; however, to date, fertility and pregnancy outcomes have not been assessed in this group. Nevertheless, based on the epidemiology data described above, pregnant partners of these men should be carefully monitored for PTB and other adverse outcomes.
Although accidental industrial exposures of large populations to high levels of TCDD are rare, toxicant exposures are commonly associated with military service. For example, burn pits are frequently used to destroy military refuse, a process that produces abundant TCDD and numerous other EDCs [68]. Furthermore, current military personnel deployed to Afghanistan or Iraq can be exposed to these toxicants due to smoke arising from oil fires, which often occur in these countries [69,70,71]. Although the potential long-term reproductive consequences of these exposures have yet to be definitively determined, there is increased awareness of potential chemical toxicity. For this reason, the US Veteran’s Administration has developed a “Burn Pit” registry to attempt to identify and track potential adverse effects of exposures associated with military service [72].
In addition to current exposure threats to our military forces, during the American War in Vietnam, numerous American military personnel were exposed to TCDD as a consequence of “Operation Ranch Hand”. From 1962 to 1971, the US Air Force sprayed at least 11 million gallons of the herbicide Agent Orange, which was known to be contaminated with TCDD, over large areas of central and South Vietnam in an effort to destroy the dense vegetation enemy forces used for cover [73]. It is estimated that up to 1.5 million American servicemen were exposed to high doses of TCDD as a consequence of Operation Ranch Hand. Unfortunately, numerous long-term health effects have been attributed to this exposure, with many Ranch Hand veterans developing serious health problems, including cancer. Although no study has conclusively demonstrated an increase in infertility or PTB risk in this exposed population, Michalek et al. [43] described a significant increase in the incidence of PTB in partners of Ranch Hand Veterans compared to the partners of an unexposed Veteran population. For this study, serum TCDD was measured in men approximately 20 years after military service and body burden at the time of conception (during or shortly after service in Southeast Asia) estimated based on the known pharmacokinetics of this toxicant. Analysis revealed that the PTB risk was significantly increased in partners of Ranch Hand Veterans with estimated body burdens consistent with either “background” levels or estimated high dose exposure compared to partners of unexposed men. Interestingly, Veterans with a moderate estimated body burden of TCDD exhibited a PTB rate below that of the unexposed Veterans, which was also lower than the incidence observed in the background and high exposure groups. These results led the authors to surmise that PTB risk was not associated with paternal TCDD exposure. However, TCDD and numerous other EDCs exhibit a biphasic effect, in which both high and low dose exposures are damaging, while a modest dose is less impactful [44], mirroring the results obtained in the Ranch Hand retrospective study. A biphasic effect of TCDD exposure associated with Operation Ranch Hand is also suggested by the occurrence of infant death, which was highest in the background and high exposure categories, but lower in the moderate exposure group [43]. However, the percent of infant deaths was higher in all Ranch Hand Veterans compared to the unexposed exposure group. Alternatively, as suggested by the authors, it is also possible that extrapolation of TCDD body burden at conception was imprecise, since elimination of TCDD from the body varies with body type and is dose-dependent. Thus, reassessment of the Ranch Hand/PTB data may be of value [62].
Despite the uncertainty with regard to PTB risk, it is well-established that children of TCDD exposed Veterans are more likely to exhibit spina bifida and other neural tube defects compared to the general population [74]. Even more concerning, although there has been no carefully designed scientific study, there is empirical evidence that even the grandchildren of Agent Orange Veterans exhibit serious health problems which may be related to ancestral TCDD exposure [75,76,77]. How might it be possible for a man’s TCDD exposure associated with Operation Ranch Hand to impact not only the health of his child, but also that of his grandchild? As will be discussed below, toxicant-associated epigenetic alterations to the germline can be transmitted to future generations and can influence development of disease. Although epigenetic modifications are most commonly a consequence of in utero toxicant exposures, spermatogenesis is a continuous process from puberty until death [78]. Thus, even an adult exposure would have the potential to permanently damage the testicular stem cells that give rise to a man’s sperm, and, therefore, his progeny [79]. It is also worth noting that the average age of the American serviceman in Vietnam is estimated at 22, with some as young as 17 [80]. Since the human male can continue to mature into his early twenties [78], participation in Operation Ranch Hand may have resulted in a “late stage” developmental TCDD exposure for some Veterans.
Of course, it is not just the American military that continues to be impacted by Operation Ranch Hand. Although difficult to determine precisely, it is estimated that up to 4 million South Vietnamese residents were also unintentionally exposed to Agent Orange during the American war [81]. As many as 400,000 Vietnamese died as a direct result of acute TCDD exposure. Among the surviving Vietnamese population, a wide range of health issues have been noted and are likely linked to TCDD exposure, including high rates of early pregnancy loss, spontaneous PTB, congenital birth defects and numerous cancers [82,83,84,85]. Unfortunately, the heavy contamination of some areas of Vietnam combined with its tendency to bioaccumulate and resistance to degradation has resulted in the persistence of TCDD in parts of the country [86]; thus, significant human exposure is ongoing. Although we cannot yet definitively state that an adult man’s exposure to TCDD and/or other EDCs is a major contributor to the incidence of PTB, the frequent occurrence of adverse pregnancy outcomes among human populations with known exposures should not be ignored.
In Utero Exposure of Males and Adverse Outcomes Across Multiple Generations
Human studies described above raise significant concerns regarding the long-term consequences of exposure to environmental EDCs such as TCDD. However, developing an understanding of the mechanisms of these effects is critical if we are to identify protective measures. Since human exposure typically starts in utero, as a consequence of maternal environmental exposures, we previously developed an animal model of developmental TCDD exposure, enabling us to examine the adult reproductive effects in the offspring. In our model, pregnant mice are exposed to a single TCDD dose (10 μg/kg) by gavage on embryonic day 15.5 (E15.5), when organogenesis is complete. Although a high dose compared to typical human exposures, mice are markedly less sensitive to this toxicant and exhibit a more rapid clearance compared to humans (days versus years). Furthermore, at this dose during late pregnancy, TCDD is not teratogenic or abortigenic in mice and pups are born at term (E20). However, nearly half of all male and female adult offspring (F1) exhibit infertility [4, 5, 87] while PTB (parturition <E19) is common in F1females that are able to become pregnant as well as in pregnancies arising in partners of F1males. Notably, ~ 25% of “late preterm” pups (born on E18.5) do not survive to weaning, while pups born <E18 exhibit 100% mortality within the first week of life [8]. Incredibly, in the absence of direct TCDD exposure, F3females and control partners of F3males exhibit a similar risk of spontaneous PTB (Table 2) and high pup mortality [9, 88]. These results are particularly important since the F3 animals are the first generation that were not directly exposed to TCDD. Specifically, exposure of a pregnant female (human or other animal) results in direct exposure of the mom (F0), the fetus (F1), as well as the germ cells present within the fetus, which have the potential to become the F2 generation (Fig. 1). Toxicant-associated disorders within the F2 generation is thus a consequence of direct exposure and termed a “multi-generational” effect [11]. In contrast, disorders occurring in the F3 generation or beyond are a consequence of indirect or ancestral exposure and are considered “transgenerational” effects (reviewed by [11]).

Multi- and transgenerational consequences of developmental TCDD exposure of the male in humans and mice several studies have revealed that exposure of pregnant mice (F0 generation) is associated with adverse reproductive outcomes in male offspring (F1 generation). Since the F2 generation is present as germ cells within the F1 fetus, this generation is also directly exposed and exhibits similar outcomes as the F1 generation. F3 generation mice, the first without direct exposure, exhibit only modest improvements in reproductive outcomes. Data is limited with regard to the F4 generation, but some effects have been noted. In humans, specific information regarding developmental exposure of males to TCDD is quite limited, but some effects have been described. The persistence of PTB and significant adverse health outcomes in children born years after the American War in Vietnam support the occurrence of multi-generational effects of human TCDD exposure. Although it is difficult to definitively assess the possible transgenerational effects of developmental TCDD exposure in humans, similarities between human and mouse spermatogenesis strongly suggest this possibility
The transgenerational occurrence of subfertility and adverse pregnancy outcomes in our model is significant and implicates a role for toxicant mediated epigenetic modifications within the germline of both sexes. To fully understand the environmental risk of toxicant exposures to poor pregnancy outcomes, the impact of toxicants on the reproductive system of each sex must be considered. Equally important, it is not currently understood whether the epigenetic transfer of information to each sex differs when the information occurs from the paternal versus the maternal germ line. Therefore, environmental toxicants acting as androgen versus estrogen or progesterone disrupting agents will need more in-depth study. Nevertheless, since the placenta is heavily influenced by paternally imprinted genes in humans and mice [5, 16, 18] and placental inflammatory signaling is a critical determinant of the timing of parturition [5, 19], epigenetic studies described herein will focus on the male.
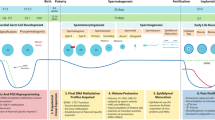
We recently conducted a methylation specific microarray analysis of late pregnancy placentae (E18.5), derived from control and F1males which identified ~ 2200 differentially methylated regions, including regions corresponding to the regulation of genes known to be important for pregnancy maintenance [9]. For example, we identified hypermethylation of the progesterone receptor (Pgr) in E18.5 placentae derived from F1male mice compared to controls. Validation studies confirmed Pgr hypermethylation in F1male derived placentae compared to control, and further demonstrated hypermethylation of this gene in F1male sperm as well as F3male sperm and placentae [9]. Hypermethylation is typically associated with gene silencing [90] and, not surprisingly, we identified reduced placental Pgr mRNA in late pregnancy placenta from toxicant-exposed males compared to unexposed controls [5, 88]. Premature loss of Pgr mRNA was closely correlated with PTB in these mice.
Preterm human babies frequently exhibit intrauterine growth restriction (IUGR) and evidence suggests that a poorly functioning placenta may be related to reduced size [91]. Furthermore, hypomethylation of placental IGF2 has been demonstrated in association with IUGR in human infants [37,38,39]. IGF2 is a paternally expressed imprinted gene in both mice and humans and is known to contribute to the regulation of fetal growth [92]. In our studies with toxicant exposed mice, we have identified IUGR in offspring of F1males (F2 pups) and offspring of F2males (F3 pups) compared to age matched control offspring. Consistent with these findings, our microarray analysis also identified this gene as hypomethylated in F1male-derived placentae. Validation studies confirmed Igf2 hypomethylation in both F1male-derived placentae and sperm. Although sperm and placentae from F3males also exhibited a reduction in Igf2 methylation, these changes did not reach significance [9]. Nevertheless, taken together, these data support our hypothesis that paternal exposure to TCDD leads to an altered sperm epigenome, which influences fertility, placental function, and pregnancy outcome transgenerationally.
Preconception Paternal Fish Oil Therapy and Prevention of Preterm Birth
While it may be possible for individuals and governmental agencies to take steps to reduce ongoing exposure to certain environmental toxicants, clearly, it is not possible to prevent an exposure that has previously occurred. Thus, we explored the potential utility of using an anti-inflammatory preconception diet to improve reproductive outcomes associated with a history of in utero exposure to TCDD. To this end, we examined the potential efficacy of preconception fish oil supplementation of fathers to improve pregnancy outcomes. Fish oil is an especially rich source of omega-3 fatty acid, which is known to exhibit anti-inflammatory effects [93]. Optimal reproductive health in humans is dependent on adequate intake of not only omega-3, but also omega-6 polyunsaturated fatty acids (PUFAS) [23]. Since mammals have only a limited capacity to synthesize these compounds [94], these essential fatty acids must be obtained via diet or supplementation. Although humans evolved on a diet of 1:1 omega-6 to omega-3s, over the last century, intake of omega-6 PUFAs has dramatically increased among Western populations and most Americans now consume a diet with ≥ 25:1 omega-6 to omega-3 [95]. In the Southern USA, it is estimated that this ratio can approach 40:1 among some individuals [95]. Excess intake of omega-6 or inadequate intake of the omega-3 fatty acids (i.e., fish oil) has been linked to systemic inflammation and exacerbation of inflammatory diseases (reviewed by [94]).
Inflammation of the placenta, fetal membranes, and decidua is an essential element of term parturition [20, 96]. Significantly, pathologic activation of inflammatory signaling cascades as a consequence of infection or sterile inflammatory triggers can induce spontaneous PTB [96]. Thus, numerous studies have examined the ability of maternal fish oil supplementation to increase gestational length in women at risk of PTB, but results have not consistently demonstrated efficacy [22, 23]. Based on our data, presented above, we surmise that the inconsistent ability of fish oil to prevent PTB in clinical trials is due to the failure to initiate treatment prior to conception. Furthermore, because of the role of the paternal parent in contributing to placental health and function, preconception treatment of the father should be considered. Thus, using our murine model, we examined the impact of preconception paternal fish oil supplementation on pregnancy outcomes in his partner. In contrast to a high rate of PTB in partners of F1males maintained on the standard diet, 100% of partners of F1males provided a fish oil-supplemented diet prior to mating delivered at term ([89] Table 2). Although Pgr mRNA expression was significantly reduced in E18.5 placentae derived from F1males, preconception paternal fish oil protected against the loss of placental Pgr mRNA [5]. Preconception fish oil supplementation of the male also eliminated IUGR and normalized placental weights from F2 pups [89].
To begin to identify a possible mechanism for these profound effects, we next examined expression of prostaglandin dehydrogenase (PGDH) in control and F1male (± fish oil) derived placentae. PGDH is the enzyme that catabolizes the inflammatory prostaglandin E2 (PGE2) to its inactive form. Our studies revealed that, compared to controls, late pregnancy samples obtained from control females mated to F1males exhibited a dramatic decrease in PGDH immunolocalization within the placenta and fetal membranes while fish oil supplementation prevented the premature loss of this enzyme. As expected, loss of PGDH was associated with an increase in the inflammatory prostaglandin, PGE2 [88, 89]. As yet, we have not determined whether the fish oil diet is capable of normalizing the sperm and placental epigenome or is primarily acting via suppression of inflammation.
Conclusions
Concomitant with industrialization, the rate of PTB has risen, suggesting a possible association between pollution and adverse pregnancy outcomes [97,98,99]. Although several studies have examined maternal toxicant exposure with regard to PTB risk (reviewed by [52, 100]), our studies in mice and epidemiologic evidence in humans suggest that the developmental exposure history of the father is also an important contributor to this major health problem (Fig. 1). Unfortunately, current clinical and research efforts to reduce or prevent PTB focus on the mother—often only well into pregnancy once events placing her at risk of this event have already begun. Not surprisingly, preventive measures taken after the inflammatory processes of PTB have begun have only minimal benefit. Significantly, our studies in mice support a successful reduction in PTB risk following a paternal intervention (Table 2). Since evidence strongly indicates the paternal parent is also an important contributor to timing of birth in women (Table 1), exploring paternal intervention strategies to reduce the incidence of PTB in women should be considered.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Behrman RE, Butler AS, editors. Preterm Birth: Causes, Consequences, and Prevention. Washington (DC): The National Academies Collection: Reports funded by National Institutes of Health; 2007.
MarchOfDimes. Premature birth report CARD. In: 2018; 2018. https://www.marchofdimes.org/mission/prematurity-reportcard-tv.aspx. 23 May 19
• Levine H, Jorgensen N, Martino-Andrade A, Mendiola J, Weksler-Derri D, Mindlis I, et al. Temporal trends in sperm count: a systematic review and meta-regression analysis. Hum Reprod Update. 2017;23(6):646–59. https://doi.org/10.1093/humupd/dmx022 This is a comprehensive meta-analysis identified declining sperm counts among men from North America, Europe and Australia during 1973–2011. Significantly, they identified a 50–60% decline among men unselected by fertility.
Bruner-Tran KL, Gnecco J, Ding T, Glore DR, Pensabene V, Osteen KG. Exposure to the environmental endocrine disruptor TCDD and human reproductive dysfunction: translating lessons from murine models. Reprod Toxicol. 2017;68:59–71. https://doi.org/10.1016/j.reprotox.2016.07.007.
Ding T, McConaha M, Boyd KL, Osteen KG, Bruner-Tran KL. Developmental dioxin exposure of either parent is associated with an increased risk of preterm birth in adult mice. Reprod Toxicol. 2011;31(3):351–8. https://doi.org/10.1016/j.reprotox.2010.11.003.
Melnick R, Lucier G, Wolfe M, Hall R, Stancel G, Prins G, et al. Summary of the National Toxicology Program's report of the endocrine disruptors low-dose peer review. Environ Health Perspect. 2002;110(4):427–31. https://doi.org/10.1289/ehp.02110427.
Tiffon C. The impact of nutrition and environmental epigenetics on human health and disease. Int J Mol Sci. 2018;19(11). https://doi.org/10.3390/ijms19113425.
Ding T, Lambert LA, Aronoff DM, Osteen KG, Bruner-Tran KL. Sex-dependent influence of developmental toxicant exposure on group B streptococcus-mediated preterm birth in a murine model. Reprod Sci. 2018;25(5):662–73. https://doi.org/10.1177/1933719117741378.
Ding T, Mokshagundam S, Rinaudo PF, Osteen KG, Bruner-Tran KL. Paternal developmental toxicant exposure is associated with epigenetic modulation of sperm and placental Pgr and Igf2 in a mouse model. Biol Reprod. 2018;99(4):864–76. https://doi.org/10.1093/biolre/ioy111.
Bruner-Tran KL, Resuehr D, Ding T, Lucas JA, Osteen KG. The role of endocrine disruptors in the epigenetics of reproductive disease and dysfunction: potential relevance to humans. Curr Obstet Gynecol Rep. 2012;1(3):116–23. https://doi.org/10.1007/s13669-012-0014-7.
Skinner MK. Endocrine disruptors in 2015: epigenetic transgenerational inheritance. Nat Rev Endocrinol. 2016;12(2):68–70. https://doi.org/10.1038/nrendo.2015.206.
Lambrot R, Xu C, Saint-Phar S, Chountalos G, Cohen T, Paquet M, et al. Low paternal dietary folate alters the mouse sperm epigenome and is associated with negative pregnancy outcomes. Nat Commun. 2013;4:2889. https://doi.org/10.1038/ncomms3889.
Siklenka K, Erkek S, Godmann M, Lambrot R, McGraw S, Lafleur C, et al. Disruption of histone methylation in developing sperm impairs offspring health transgenerationally. Science. 2015;350(6261):aab2006. https://doi.org/10.1126/science.aab2006.
Estill MS, Krawetz SA. The epigenetic consequences of paternal exposure to environmental contaminants and reproductive toxicants. Curr Environ Health Rep. 2016;3(3):202–13. https://doi.org/10.1007/s40572-016-0101-4.
Ibrahim Y, Hotaling J. Sperm epigenetics and its impact on male fertility, pregnancy loss, and somatic health of future Offsprings. Semin Reprod Med. 2018;36(3–04):233–9. https://doi.org/10.1055/s-0038-1677047.
Barton SC, Adams CA, Norris ML, Surani MA. Development of gynogenetic and parthenogenetic inner cell mass and trophectoderm tissues in reconstituted blastocysts in the mouse. J Embryol Exp Morphol. 1985;90:267–85.
Maltepe E, Fisher SJ. Placenta: the forgotten organ. Annu Rev Cell Dev Biol. 2015;31:523–52. https://doi.org/10.1146/annurev-cellbio-100814-125620.
Wang X, Miller DC, Harman R, Antczak DF, Clark AG. Paternally expressed genes predominate in the placenta. Proc Natl Acad Sci U S A. 2013;110(26):10705–10. https://doi.org/10.1073/pnas.1308998110.
Houben ML, Nikkels PG, van Bleek GM, Visser GH, Rovers MM, Kessel H, et al. The association between intrauterine inflammation and spontaneous vaginal delivery at term: a cross-sectional study. PLoS One. 2009;4(8):e6572. https://doi.org/10.1371/journal.pone.0006572.
Menon R, Richardson LS, Lappas M. Fetal membrane architecture, aging and inflammation in pregnancy and parturition. Placenta. 2019;79:40–5. https://doi.org/10.1016/j.placenta.2018.11.003.
Harris WS. Recent trials challenge the benefits of Omega-3. Keio J Med. 2015;64(4):65. https://doi.org/10.2302/kjm.64-003-ABST.
Jordan RG. The challenge of preterm birth. J Midwifery Womens Health. 2008;53(1):96.
McGregor JA, Allen KG, Harris MA, Reece M, Wheeler M, French JI, et al. The omega-3 story: nutritional prevention of preterm birth and other adverse pregnancy outcomes. Obstet Gynecol Surv. 2001;56(5 Suppl 1):S1–13.
• Meng Y, Groth SW. Fathers Count: The Impact of Paternal Risk Factors on Birth Outcomes. Matern Child Health J. 2018;22(3):401–8. https://doi.org/10.1007/s10995-017-2407-8 This is a retrospective cross-sectional analysis of birth certificate records (2004 to 2015) from the Finger Lakes Region in New York. Potential paternal risk factors examined included age, race/ethnicity, and education on four birth outcomes (preterm birth, low birthweight, high birthweight and small for gestational age). After controlling for maternal factors, several paternal factors (age, race, education) were found to contribute significantly to birth outcomes.
Oldereid NB, Wennerholm UB, Pinborg A, Loft A, Laivuori H, Petzold M, et al. The effect of paternal factors on perinatal and paediatric outcomes: a systematic review and meta-analysis. Hum Reprod Update. 2018;24(3):320–89. https://doi.org/10.1093/humupd/dmy005.
Goisis A, Remes H, Barclay K, Martikainen P, Myrskyla M. Paternal age and the risk of low birth weight and preterm delivery: a Finnish register-based study. J Epidemiol Community Health. 2018;72(12):1104–9. https://doi.org/10.1136/jech-2017-210170.
Khandwala YS, Baker VL, Shaw GM, Stevenson DK, Lu Y, Eisenberg ML. Association of paternal age with perinatal outcomes between 2007 and 2016 in the United States: population based cohort study. BMJ. 2018;363:k4372. https://doi.org/10.1136/bmj.k4372.
Palomar L, DeFranco EA, Lee KA, Allsworth JE, Muglia LJ. Paternal race is a risk factor for preterm birth. Am J Obstet Gynecol. 2007;197(2):152 e1–7. https://doi.org/10.1016/j.ajog.2007.03.035.
Shachar BZ, Mayo JA, Lyell DJ, Stevenson DK, Shaw GM, Blumenfeld YJ. Risk for spontaneous preterm birth among inter-racial/ethnic couples. J Matern Fetal Neonatal Med. 2018;31(5):633–9. https://doi.org/10.1080/14767058.2017.1293029.
Simhan HN, Krohn MA. Paternal race and preterm birth. Am J Obstet Gynecol. 2008;198(6):644 e1–6. https://doi.org/10.1016/j.ajog.2007.11.046.
Li Y, Luo Z, Holzman C, Liu H, Margerison CE. Paternal race/ethnicity and risk of adverse birth outcomes in the United States, 1989-2013. AIMS Public Health. 2018;5(3):312–23. https://doi.org/10.3934/publichealth.2018.3.312.
Portha B, Grandjean V, Movassat J. Mother or father: who is in the front line? Mechanisms underlying the non-genomic transmission of obesity/diabetes via the maternal or the paternal line. Nutrients. 2019;11(2). https://doi.org/10.3390/nu11020233.
Dodd JM, Du Plessis LE, Deussen AR, Grivell RM, Yelland LN, Louise J, et al. Paternal obesity modifies the effect of an antenatal lifestyle intervention in women who are overweight or obese on newborn anthropometry. Sci Rep. 2017;7(1):1557. https://doi.org/10.1038/s41598-017-01672-w.
• Houfflyn S, Matthys C, Soubry A. Male Obesity: Epigenetic Origin and Effects in Sperm and Offspring. Curr Mol Biol Rep. 2017;3(4):288–96. https://doi.org/10.1007/s40610-017-0083-5 A number of recent studies have suggested or presented data indicating epigenetic changes in sperm can influence offspring health. This paper summarizes the current data on paternal obesity, molecular/epigenetic mechanisms impacting sperm and transmission of disease conditions to offspring. Perhaps of greater interest, they introduce the concept of “paternal origins of health and disease (POHaD)”.
Moss JL, Harris KM. Impact of maternal and paternal preconception health on birth outcomes using prospective couples' data in add health. Arch Gynecol Obstet. 2015;291(2):287–98. https://doi.org/10.1007/s00404-014-3521-0.
Galaviz-Hernandez C, Sosa-Macias M, Teran E, Garcia-Ortiz JE, Lazalde-Ramos BP. Paternal Determinants in Preeclampsia. Front Physiol. 2018;9:1870. https://doi.org/10.3389/fphys.2018.01870.
Guo L, Choufani S, Ferreira J, Smith A, Chitayat D, Shuman C, et al. Altered gene expression and methylation of the human chromosome 11 imprinted region in small for gestational age (SGA) placentae. Dev Biol. 2008;320(1):79–91. https://doi.org/10.1016/j.ydbio.2008.04.025.
Koukoura O, Sifakis S, Soufla G, Zaravinos A, Apostolidou S, Jones A, et al. Loss of imprinting and aberrant methylation of IGF2 in placentas from pregnancies complicated with fetal growth restriction. Int J Mol Med. 2011;28(4):481–7. https://doi.org/10.3892/ijmm.2011.754.
Koukoura O, Sifakis S, Zaravinos A, Apostolidou S, Jones A, Hajiioannou J, et al. Hypomethylation along with increased H19 expression in placentas from pregnancies complicated with fetal growth restriction. Placenta. 2011;32(1):51–7. https://doi.org/10.1016/j.placenta.2010.10.017.
He Y, Xie X, Tang W, Ma X. Maternal and paternal obesity and adverse pregnancy outcomes in China: a cohort study. Lancet. 2017. https://doi.org/10.1016/S0140-6736(17)33190-2.
Goran MI, Plows JF, Ventura EE. Effects of consuming sugars and alternative sweeteners during pregnancy on maternal and child health: evidence for a secondhand sugar effect. Proc Nutr Soc. 2018;1–10. https://doi.org/10.1017/S002966511800263X.
Quansah R, Jaakkola JJ. Paternal and maternal exposure to welding fumes and metal dusts or fumes and adverse pregnancy outcomes. Int Arch Occup Environ Health. 2009;82(4):529–37. https://doi.org/10.1007/s00420-008-0349-6.
Michalek JE, Rahe AJ, Boyle CA. Paternal dioxin, preterm birth, intrauterine growth retardation, and infant death. Epidemiology. 1998;9(2):161–7.
Vandenberg LN, Colborn T, Hayes TB, Heindel JJ, Jacobs DR Jr, Lee DH, et al. Hormones and endocrine-disrupting chemicals: low-dose effects and nonmonotonic dose responses. Endocr Rev. 2012;33(3):378–455. https://doi.org/10.1210/er.2011-1050.
McCowan LM, North RA, Kho EM, Black MA, Chan EH, Dekker GA, et al. Paternal contribution to small for gestational age babies: a multicenter prospective study. Obesity (Silver Spring). 2011;19(5):1035–9. https://doi.org/10.1038/oby.2010.279.
Zhao L, Chen L, Yang T, Wang L, Wang T, Zhang S, et al. Parental smoking and the risk of congenital heart defects in offspring: an updated meta-analysis of observational studies. Eur J Prev Cardiol. 2019. https://doi.org/10.1177/2047487319831367.
Banderali G, Martelli A, Landi M, Moretti F, Betti F, Radaelli G, et al. Short and long term health effects of parental tobacco smoking during pregnancy and lactation: a descriptive review. J Transl Med. 2015;13:327. https://doi.org/10.1186/s12967-015-0690-y.
Hillman S, Peebles DM, Williams DJ. Paternal metabolic and cardiovascular risk factors for fetal growth restriction: a case-control study. Diabetes Care. 2013;36(6):1675–80. https://doi.org/10.2337/dc12-1280.
Liu W, Huang C, Cai J, Wang X, Zou Z, Sun C. Household environmental exposures during gestation and birth outcomes: a cross-sectional study in Shanghai, China. Sci Total Environ. 2018;615:1110–8. https://doi.org/10.1016/j.scitotenv.2017.10.015.
Andriani H, Kuo HW. Adverse effects of parental smoking during pregnancy in urban and rural areas. BMC Pregnancy Childbirth. 2014;14:414. https://doi.org/10.1186/s12884-014-0414-y.
Cui H, Gong TT, Liu CX, Wu QJ. Associations between passive maternal smoking during pregnancy and preterm birth: evidence from a meta-analysis of observational studies. PLoS One. 2016;11(1):e0147848. https://doi.org/10.1371/journal.pone.0147848.
Wang L, Yang Y, Liu F, Yang A, Xu Q, Wang Q, et al. Paternal smoking and spontaneous abortion: a population-based retrospective cohort study among non-smoking women aged 20-49 years in rural China. J Epidemiol Community Health. 2018;72(9):783–9. https://doi.org/10.1136/jech-2017-210311.
Beszterda M, Franski R. Endocrine disruptor compounds in environment: as a danger for children health. Pediatr Endocrinol Diabetes Metab. 2018;24(2):88–95. https://doi.org/10.18544/PEDM-24.02.0107.
Gonzalez N, Marques M, Nadal M, Domingo JL. Occurrence of environmental pollutants in foodstuffs: a review of organic vs. conventional food. Food Chem Toxicol. 2019;125:370–5. https://doi.org/10.1016/j.fct.2019.01.021.
Zennegg M. Dioxins and PCBs in meat - still a matter of concern? Chimia (Aarau). 2018;72(10):690–6. https://doi.org/10.2533/chimia.2018.690.
Stillerman KP, Mattison DR, Giudice LC, Woodruff TJ. Environmental exposures and adverse pregnancy outcomes: a review of the science. Reprod Sci. 2008;15(7):631–50. https://doi.org/10.1177/1933719108322436.
Candela S, Bonvicini L, Ranzi A, Baldacchini F, Broccoli S, Cordioli M, et al. Exposure to emissions from municipal solid waste incinerators and miscarriages: a multisite study of the MONITER project. Environ Int. 2015;78:51–60. https://doi.org/10.1016/j.envint.2014.12.008.
Hansen DA, Esakky P, Drury A, Lamb L, Moley KH. The aryl hydrocarbon receptor is important for proper seminiferous tubule architecture and sperm development in mice. Biol Reprod. 2014;90(1):8. https://doi.org/10.1095/biolreprod.113.108845.
Hernandez-Ochoa I, Karman BN, Flaws JA. The role of the aryl hydrocarbon receptor in the female reproductive system. Biochem Pharmacol. 2009;77(4):547–59. https://doi.org/10.1016/j.bcp.2008.09.037.
Lawrence BP, Vorderstrasse BA. New insights into the aryl hydrocarbon receptor as a modulator of host responses to infection. Semin Immunopathol. 2013;35(6):615–26. https://doi.org/10.1007/s00281-013-0395-3.
Mukerjee D. Health impact of polychlorinated dibenzo-p-dioxins: a critical review. J Air Waste Manag Assoc. 1998;48(2):157–65.
Emond C, Michalek JE, Birnbaum LS, DeVito MJ. Comparison of the use of a physiologically based pharmacokinetic model and a classical pharmacokinetic model for dioxin exposure assessments. Environ Health Perspect. 2005;113(12):1666–8. https://doi.org/10.1289/ehp.8016.
White SS, Birnbaum LS. An overview of the effects of dioxins and dioxin-like compounds on vertebrates, as documented in human and ecological epidemiology. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2009;27(4):197–211. https://doi.org/10.1080/10590500903310047.
Pesatori AC, Consonni D, Bachetti S, Zocchetti C, Bonzini M, Baccarelli A, et al. Short- and long-term morbidity and mortality in the population exposed to dioxin after the "Seveso accident". Ind Health. 2003;41(3):127–38.
Eskenazi B, Warner M, Brambilla P, Signorini S, Ames J, Mocarelli P. The Seveso accident: a look at 40years of health research and beyond. Environ Int. 2018;121(Pt 1:71–84. https://doi.org/10.1016/j.envint.2018.08.051.
Mocarelli P, Gerthoux PM, Needham LL, Patterson DG Jr, Limonta G, Falbo R, et al. Perinatal exposure to low doses of dioxin can permanently impair human semen quality. Environ Health Perspect. 2011;119(5):713–8. https://doi.org/10.1289/ehp.1002134.
Mocarelli P, Gerthoux PM, Patterson DG Jr, Milani S, Limonta G, Bertona M, et al. Dioxin exposure, from infancy through puberty, produces endocrine disruption and affects human semen quality. Environ Health Perspect. 2008;116(1):70–7. https://doi.org/10.1289/ehp.10399.
Aurell J, Gullett BK, Yamamoto D. Emissions from open burning of simulated military waste from forward operating bases. Environ Sci Technol. 2012;46(20):11004–12. https://doi.org/10.1021/es303131k.
Doucet I. Desert storm syndrome: sick soldiers and dead children? Med War. 1994;10(3):183–94.
Emmerova M, Jirava F. Is gulf War syndrome really a mystery? Med Confl Surviv. 2004;20(3):209–17. https://doi.org/10.1080/1362369042000248811.
Woodall BD, Yamamoto DP, Gullett BK, Touati A. Emissions from small-scale burns of simulated deployed U.S. military waste. Environ Sci Technol. 2012;46(20):10997–1003. https://doi.org/10.1021/es3021556.
Butler DA, Styka AN, Savitz DA, editors. Assessment of the Department of Veterans Affairs Airborne Hazards and Open Burn Pit Registry. Washington (DC); 2017.
Lewis J. Smokey Bear in Vietnam. Environ Hist. 2006;11(3):598–603.
Institute Of Medicine. Veterans and agent Orange: health effects of herbicides used in Vietnam. Washington, DC: National Academies Press; 1994.
Ornstein C, Fresques H. ProPublica, Hixenbaugh M. The children of agent Orange. Virginia-pilot. 2016. https://www.propublica.org/article/the-children-of-agent-orange. 23 May 19
Peterson B. Vietnam War veterans' kids say agent Orange impact 'a nightmare'. 2018. https://abcnews.go.com/Politics/vietnam-war-veterans-kids-agent-orange-impact-nightmare/story?id=59059570. 23 May 19
WFLA. Agent Orange effects being seen in grandchildren of Vietnam War veterans. 2018. https://www.wfla.com/8-on-your-side/investigations/impacts-being-seen-in-grandchildren-of-vietnam-war-veterans-is-it-agent-orange-/1183887612. 23 May 19
Part 2: Making women and men. In Johnson M, editor. Essential reproduction. Wiley; 2010.
Skinner MK. What is an epigenetic transgenerational phenotype? F3 or F2. Reprod Toxicol. 2008;25(1):2–6. https://doi.org/10.1016/j.reprotox.2007.09.001.
U.S. War Dog Association. Vietnam Statistics. http://www.uswardogs.org/vietnam-statistics/. 15 April 19
Stellman JM, Stellman SD. Agent Orange during the Vietnam War: the lingering issue of its civilian and military health impact. Am J Public Health. 2018;108(6):726–8. https://doi.org/10.2105/AJPH.2018.304426.
Anh NT, Nishijo M, Tai PT, Maruzeni S, Morikawa Y, Anh TH, et al. Maternal risk factors associated with increased dioxin concentrations in breast milk in a hot spot of dioxin contamination in Vietnam. J Expo Sci Environ Epidemiol. 2014;24(5):489–96. https://doi.org/10.1038/jes.2013.73.
Nghi TN, Nishijo M, Manh HD, Tai PT, Van Luong H, Anh TH, et al. Dioxins and Nonortho PCBs in breast Milk of Vietnamese mothers living in the largest hot spot of dioxin contamination. Environ Sci Technol. 2015;49(9):5732–42. https://doi.org/10.1021/es506211p.
Schecter A, Pavuk M, Constable JD, Daile C, Papke O. A follow-up: high level of dioxin contamination in Vietnamese from agent orange, three decades after the end of spraying. J Occup Environ Med. 2002;44(3):218–20.
Tai PT, Nishijo M, Anh NT, Maruzeni S, Nakagawa H, Van Luong H, et al. Dioxin exposure in breast milk and infant neurodevelopment in Vietnam. Occup Environ Med. 2013;70(9):656–62. https://doi.org/10.1136/oemed-2012-101021.
Ngo TH, Hien TT, Thuan NT, Minh NH, Chi KH. Atmospheric PCDD/F concentration and source apportionment in typical rural, agent Orange hotspots, and industrial areas in Vietnam. Chemosphere. 2017;182:647–55. https://doi.org/10.1016/j.chemosphere.2017.05.050.
Bruner-Tran KL, Osteen KG. Developmental exposure to TCDD reduces fertility and negatively affects pregnancy outcomes across multiple generations. Reprod Toxicol. 2011;31(3):344–50. https://doi.org/10.1016/j.reprotox.2010.10.003.
Bruner-Tran KL, Ding T, Yeoman KB, Archibong A, Arosh JA, Osteen KG. Developmental exposure of mice to dioxin promotes transgenerational testicular inflammation and an increased risk of preterm birth in unexposed mating partners. PLoS One. 2014;9(8):e105084. https://doi.org/10.1371/journal.pone.0105084.
McConaha ME, Ding T, Lucas JA, Arosh JA, Osteen KG, Bruner-Tran KL. Preconception omega-3 fatty acid supplementation of adult male mice with a history of developmental 2,3,7,8-tetrachlorodibenzo-p-dioxin exposure prevents preterm birth in unexposed female partners. Reproduction. 2011;142(2):235–41. https://doi.org/10.1530/REP-11-0070.
Zeng Y, Chen T. DNA methylation reprogramming during mammalian development. Genes (Basel). 2019;10(4). https://doi.org/10.3390/genes10040257.
Koutsaki M, Sifakis S, Zaravinos A, Koutroulakis D, Koukoura O, Spandidos DA. Decreased placental expression of hPGH, IGF-I and IGFBP-1 in pregnancies complicated by fetal growth restriction. Growth Hormon IGF Res. 2011;21(1):31–6. https://doi.org/10.1016/j.ghir.2010.12.002.
Kadakia R, Josefson J. The relationship of insulin-like growth factor 2 to fetal growth and adiposity. Horm Res Paediatr. 2016;85(2):75–82. https://doi.org/10.1159/000443500.
Rogero MM, Calder PC. Obesity, inflammation, toll-like receptor 4 and fatty acids. Nutrients. 2018;10(4). https://doi.org/10.3390/nu10040432.
Calder PC. Omega-3 polyunsaturated fatty acids and inflammatory processes: nutrition or pharmacology? Br J Clin Pharmacol. 2013;75(3):645–62. https://doi.org/10.1111/j.1365-2125.2012.04374.x.
Massiera F, Barbry P, Guesnet P, Joly A, Luquet S, Moreilhon-Brest C, et al. A Western-like fat diet is sufficient to induce a gradual enhancement in fat mass over generations. J Lipid Res. 2010;51(8):2352–61. https://doi.org/10.1194/jlr.M006866.
Hadley EE, Richardson LS, Torloni MR, Menon R. Gestational tissue inflammatory biomarkers at term labor: a systematic review of literature. Am J Reprod Immunol. 2018;79(2):e12776. https://doi.org/10.1111/aji.12776.
Burris HH, Baccarelli AA, Wright RO, Wright RJ. Epigenetics: linking social and environmental exposures to preterm birth. Pediatr Res. 2016;79(1–2):136–40. https://doi.org/10.1038/pr.2015.191.
Nieuwenhuijsen MJ, Dadvand P, Grellier J, Martinez D, Vrijheid M. Environmental risk factors of pregnancy outcomes: a summary of recent meta-analyses of epidemiological studies. Environ Health. 2013;12:6. https://doi.org/10.1186/1476-069X-12-6.
Porpora MG, Piacenti I, Scaramuzzino S, Masciullo L, Rech F, Benedetti Panici P. Environmental contaminants exposure and preterm birth: a systematic review. Toxics. 2019;7(1). https://doi.org/10.3390/toxics7010011.
Kumar S, Sharma S, Thaker R. Occupational, environmental, and lifestyle factors and their contribution to preterm birth - an overview. Indian J Occup Environ Med. 2017;21(1):9–17. https://doi.org/10.4103/ijoem.IJOEM_155_16.
Acknowledgments
We gratefully acknowledge the assistance of Ms. Evelyn Hipp for contributing her artistic talent to Fig. 1.
Funding
Studies presented herein were supported in part by VA I01 BX002853, NIEHS ES14942, Amag Pharmaceuticals and the Vanderbilt University School of Medicine Medical Scholars Program.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Shilpa Mokshagundam, Alison Barlow, and Tianbing Ding declare no conflict of interest. Kaylon L. Bruner-Tran reports grants from National Institute of Environmental Health Science, the Department of Veteran Affairs, the Environmental Protection Agency, and from AMAG Pharmacueticals, during the conduct of the study. Kevin G. Osteen reports grants from Gates Foundation, the Environmental Protection Agency, the National Institute of Environmental Health Science, and from the Department of Veteran Affairs, during the conduct of the study.
Human and Animal Rights and Informed Consent
This article does not contain any new studies with humans or animals subjects performed by the any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Environmental Exposures and Pregnancy Outcomes
Rights and permissions
About this article

Cite this article
Bruner-Tran, K.L., Mokshagundam, S., Barlow, A. et al. Paternal Environmental Toxicant Exposure and Risk of Adverse Pregnancy Outcomes. Curr Obstet Gynecol Rep 8, 103–113 (2019). https://doi.org/10.1007/s13669-019-00265-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13669-019-00265-w