
Abstract
Gastric cancer (GC) is the second cause of cancer-related death worldwide. Interleukin (IL)-16 has a vital role in the development and homeostasis of the immune system. In the present study, we evaluated an exon variant rs4072111 C/T polymorphism and 3′ UTR variant rs1131445 C/T within the miRNA binding with gastric cancer susceptibility in Iranian population. Genomic DNA was isolated from peripheral blood samples according to phenol chloroform extraction. The genotypes of IL-16 polymorphisms rs1131445 T/C and rs4072111 T/C were determined by polymerase chain reaction-restriction fragment length polymorphism method. In this case control study, a total of 256 patients with gastric cancer (238 cases (92.9 %) non-cardia and 18 cases (7.1 %) cardia) and 300 healthy control subjects were evaluated. In the present study, we found a significant association between rs4072111 of IL-16 gene and risk of GC in Iranian population. Individuals with CT genotype showed a significant association with 1.79-fold increased risk of GC (P = 0.008; adjusted OR 1.792; 95 % CI 1.164–2.759). The significant association was also detected for T allele of rs4072111 and increased risk of GC (P < 0.001; adjusted OR 1.981; 95 % CI 1.354–2.900). We also observed statistically a significant relationship between rs1131445 of IL-16 CT genotype and GC risk. Carriers of IL-16 CT genotype compared with TT genotype had 1.44 times higher increased likelihood of GC (P = 0.048; adjusted OR 1.445; 95 % CI 1.003–2.084). After stratification according to gender, we observed that in rs1131445, CT and CC male carriers had a higher risk of GC than females (P = 0.08; adjusted OR 1.608; 95 % CI 0.945–2.737 and P = 0.08; adjusted OR 2.186; 95 % CI 0.897–5.325, respectively). We also observed that for male carriers with C allele in rs1131445, there was a 1.53-fold higher risk of GC risk than female subjects (P = 0.029; adjusted OR 1.53; 95 % CI 1.04.4–2.248). We found that the rs1131445 T/C and rs4072111 T/C variants of IL-16 were significantly associated with increased risk of GC in Iranian population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer (GC) is one of the most common types of cancer and the second cause of cancer-related death worldwide [1, 2]. GC is classified as gastric cardia cancer (GCC) and gastric non-cardia cancer (GNCC) based on the anatomic site of the lesions. Several factors are contributed to GS development including Helicobacter pylori infection, male gender, tobacco smoking, and alcohol consumption [3–5]. Most of the cases with GC are diagnosed at advanced stages; therefore, there has been an excessive effort in order to decrease its high mortality rates in the last few years [6, 7]. According to this late diagnosis, surgery is considered as the gold standard curative option in related patients [8, 9]. On the other hand, several studies have investigated the related biomarkers including single nucleotide polymorphisms (SNPs) in early steps of GC carcinogenesis in driver genes recently. SNPs are known as the most common variation in human genome. As they might have a strong diagnostic and prognostic potential for several diseases, SNPs are widely used to identify people who are at risk to develop diseases and cancers in the last few years [10–12]. Interleukin (IL)-16 is a pro-inflammatory cytokine with a variety of crucial functions which was identified in 1982 [13, 14]. The IL-16 protein is involved in tumor growth, cells communication, and differentiation, and they have also a vital role in the development and homeostasis of the immune system [14, 15]. In addition, IL-16 might trigger the secretion of tumor-associated inflammatory cytokines including TNF-α, IL-1β, IL-6, and IL-15 via monocytes [16]. All these cytokines have been reported to play a significant role in human cancer development [17–19]. It has been demonstrated that SNPs of the IL-16 gene polymorphisms have been associated with several malignancies including gastric, nasopharyngeal carcinoma, colorectal, glioma, and prostate cancer [10, 11, 20–26]. Among these putative SNPs, we evaluated an exon variant rs4072111 C/T polymorphism and rs1131445 C/T polymorphism which is located on 3′ UTR of the IL-16 gene within the miRNA-binding site and GC susceptibility in Iranian population. The role of these two polymorphisms at IL-16 and cancer susceptibility has been controversial so far [10, 22, 23, 27–29].
Materials and methods
Study population
In this study, a total of 256 patients with GC (238 cases (92.9 %) were non-cardia and 18 cases (7.1 %) were cardia) and 300 healthy control subjects without a family history of GC enrolled in this study. All patients had been referred to the Gastroenterology and Liver Diseases Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran, between 2010 and 2014. Written informed consent was taken from patients, and the local ethics committee approved the study protocol which was in accordance with the principles of the Helsinki Declaration. All subjects were Iranian and genetically unrelated. Demographic, anthropometric, and clinical characteristics information of the cases and controls was registered using a self-administered questionnaire before diagnosis of gastric cancer. Body mass index (BMI) was calculated by weight (kg)/height (m2) formula.
DNA extraction
Genomic DNA was extracted from peripheral blood samples according to phenol chloroform extraction and ethanol precipitation protocol/method [30]. The quality and standard quantity of the extracted DNA were then determined by NanoDrop 1000 Spectrophotometer (Thermo Fisher Scientific Inc; Waltham, MA). Then the samples were frozen at −20 °C for further process.
IL-16 genotyping
The genotypes of IL-16 rs4072111 C/T and rs1131445 C/T polymorphism were determined by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method. Amplification of fragment of IL-16 was performed in a 25-μl reaction mixture containing 2.5 μl of 10X buffer, 0.5 μl of dNTP, 0.75 μl of MgCl2, and 0.5 μl of each primer. The sequences of PCR primers and characteristics of restriction enzymes used for RFLP are summarized in Table 1. In addition, 0.25 μl (2.5 unit) taq polymerase and 100 ng of genomic DNA were used to perform the PCR. The PCR conditions for the SNP were as follows: 95 °C for 5 min; 35 cycles of 95 °C for 45 s, 62 °C for 35 s, 72 °C for 40 s; and a final extension at 72 °C for 10 min. Then the RFLP procedure was performed with 15 μl of PCR product and 0.5 μl of restriction enzyme BsmAI for rs4072111 C/T and BsaAI for rs1131445 C/T polymorphism. Immediately, PCR products were incubated at 65 °C overnight. Genotyping process was done by investigators who were blinded to the subjects’ clinical data. The fragments were analyzed via 3 % agarose gel electrophoresis. The green viewer staining was used to visualize the DNA band. The fragmented RFLP products sizes are also presented in Table 1.
Sequencing
Sequencing method was done for 10 % of the PCR products to confirm the RFLP procedure using an ABI PRISM 3130xL Genetic analyzer (Applied Biosystems®, Invitrogen Life Technologies, Carlsbad, CA, USA) and the chain termination method.
Statistical analysis
The statistical significance of the genotype and allele distributions between the case and control groups was determined by χ 2 testing. P < 0.05 was considered statistically significant. All analyses were adjusted for possible confounder variables. Logistic regression was applied to calculate odds ratios (ORs) and 95 % confidence intervals (CIs) for the association between each genotype and GC. The logistic regression was also used to adjust confounding factors. Consistency of genotype frequencies with the Hardy-Weinberg equilibrium (HWE) for each SNP among cases and controls was evaluated using χ 2 test. For allele frequencies, the differences were tested using χ 2 test.
ROC curve analysis
To examine whether lifestyle modified the association between each polymorphisms and gastric cancer susceptibility in our population, stratified analyses were conducted. To create receiver-operating characteristic curves (ROC curve), we used the general mode of logistic regression and the area under the curve (AUC) was determined to compare the sensitivity and specificity of putative biomarkers. Statistical analysis was performed with the help of the SPSS statistical analysis software package, version 16 (SPSS Inc, Chicago, IL).
Results
Two hundred and fifty-six patients with GC (238 (92.9 %) non-cardia and 18 cases (7.1 %) cardia) and 300 healthy subjects including 152 males and 148 females were included in this study. The mean age of the GC patients was 54.30 ± 15.763 and it was 45.13 ± 16.491 in the control group. The characteristics of cases and control subjects enrolled in this study are presented in Table 2. The genotype and allele frequencies of the interleukin-16 gene rs1131445 variant C > T and rs4072111 C > T among the patients and control subjects are presented in Table 3. In the present study, we found a significant association between rs4072111 of IL-16 gene and risk of GC in Iranian population. Individuals with CT genotype showed a significant association with 1.79-fold increased risk of GC (P = 0.008; adjusted OR 1.792; 95 % CI 1.164–2.759). On the other hand, TT genotype of rs4072111 had a very slight decreased risk of GC (P = 0.016; adjusted OR 0.999; 95 % CI 1.448–36.483). The difference between the two groups for CT genotype remained significant after adjustment for confounding factors including age, BMI, and smoking status (P = 0.009; adjusted OR 2.235, 95 % CI = 1.223–4.085).
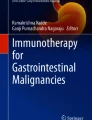
Male with TT allele had considerably higher risk of GC than female (P = 0.02; adjusted OR 13.184, 95 % CI = 1.503–115.609). The significant association was also detected for T allele of rs4072111 and increased risk of GC (P < 0.001; adjusted OR 1.981; 95 % CI 1.354–2.900). Patient with T allele had statistically significant association with 1.98-fold increased risk of GC compared to the control group. We also observed statistically a significant relationship between rs1131445 of IL-16 CT genotype and GC risk. Carriers of IL-16 CT genotype compared with TT genotype had 1.44 times higher increased likelihood of GC (P = 0.048; adjusted OR 1.445; 95 % CI 1.003–2.084). After stratification, we observed that in rs1131445, CT and CC male carriers had a higher risk of gastric cancer than females (P = 0.08; adjusted OR 1.608; 95 % CI 0.945–2.737 and P = 0.08; adjusted OR 2.186; 95 % CI 0.897–5.325, respectively) (Table 4). We also observed that in rs1131445 and males with C allele, there was a 1.53-fold higher risk of GC risk than female subjects (P = 0.029; adjusted OR 1.53; 95 % CI 1.04.4–2.248). In this study, we did not observe any significant differences between the cases and controls for the mean age (P = 0.152) or gender distribution (P = 0.856) which indicates that the matching according to these two variables was adequate. To assess the effect of SNPs and clinical features together or alone, on GC susceptibility, ROC curve analysis was performed for rs4072111 and the SNP risk alone an AUC of 0.034 (95 % CI = 0.504–0.600) was detected. For clinical features risk, an AUC of <001 (95 % CI = 0.633–0.721) was observed and for the combination of clinical features × SNP risk and AUC of <001 (95 % CI = 0.612–0.701) was detected (Fig. 1). Furthermore, for rs1131445 and the SNP risk alone, an AUC of 0.072 (95 % CI = 0.496–0.592) was detected. For clinical features risk, an AUC of <001 (95 % CI = 0.616–0.705) was observed and for the combination of clinical features × SNP risk and AUC of <001 (95 % CI = 0.612–0.701) was detected (Fig. 2).

ROC curves analysis for clinical features × SNP risk, clinical feature risk, and SNP risk (rs4072111)

ROC curves analysis for clinical features × SNP risk, clinical feature risk, and SNP risk (rs1131445)
Discussion
It has been demonstrated that pro-inflammatory mediators including cytokines, chemokines, and prostaglandins are contributed to cancer growth and progression [31, 32]. Cytokines such as tumor necrosis factor α, IL-6 [33, 34], and IL-16 [10, 11] as well as chemokines [35, 36] have been reported to play a significant role in human cancers. IL-16 as a cytokine has a key role in inflammatory response [37]. The IL-16 is produced by several activated cells including CD8+ T cells, B cells, and mast cells [38–40]. As a chemoattractant, the IL-16 proteins also bind to CD4 receptor which leads to activation of CD4+ T cells, macrophages, monocytes, dendritic, and eosinophils [41]. The protein can also trigger the secretion of several tumor-associated inflammatory cytokines including TNF-α, IL-1β, and IL-6 [13, 19, 33]. The role of IL-16 in cancer progression has been demonstrated in several studies [42–44]. In this regard, overexpression of IL-16 has been reported in a series of multiple myeloma as well as glioma patients [42, 45]. Increased IL-16 expression and its association with enhanced CD8+ T and progression of ovarian tumors have been also demonstrated in another study [46]. Furthermore, single nucleotide polymorphisms, the most common variants in genome, are considered as important biomarkers related to human cancer susceptibility [10, 27, 29]. SNPs are able to modify and increase the risk of cancer progression [47–49], whereas some other SNPs might decrease the cancer susceptibility [50–53]. They might also play a significant role in chemotherapy response and tumor drug resistance [54–57]. This might be due to their effect on transcriptome or proteome expression level of related genes [58–61]. Single nucleotide polymorphisms on regulatory regions (3′ and 5′ UTR), miRNA-binding sites, and exon variants of the genes have been the center of attention in the last few years. It is postulated that alterations on these regions might significantly modify the function of genes’ products. In this study, we explored the association of exon variant rs4072111 C/T polymorphism and 3′ UTR variant rs1131445 C/T polymorphism in the miRNA-binding site of the IL-16 gene and gastric cancer susceptibility in Iranian population. The role of these two putative IL-16 polymorphisms on cancer susceptibility has been controversial with some studies reporting the increased likelihood of the cancer susceptibility [27]‚ whereas the others indicated no association of these two SNPs and cancer risk [10, 22, 23, 28] and in addition to one study indicated the reduced risk of cancer risk [29]. In the present study, we found a significant association between rs4072111 of IL-16 gene and risk of gastric cancer in Iranian population. Patient with CT genotype showed a significant association with 1.79-fold increased risk of GC (P = 0.008; adjusted OR 1.792; 95 % CI 1.164–2.759). In addition, TT genotype of rs4072111 had a slight decreased risk of gastric cancer. This genotype seems to have a protective role in our population (P = 0.016; adjusted OR 0.999; 95 % CI 1.448–36.483). The significant association was also detected for T allele of rs4072111 and increased risk of GC (P < 0.001; adjusted OR 1.981; 95 % CI 1.354–2.900). We found that patient with T allele had statistically significant association with 1.98-fold increased risk of gastric cancer compared to the control group. We also observed statistically a significant relationship between rs1131445 of IL-16 CT genotype and GC risk. Carriers of IL-16 CT genotype compared with TT genotype had 1.44 times higher increased likelihood of GC (P = 0.048; adjusted OR 1.445; 95 % CI 1.003–2.084). Association of IL gene polymorphisms and GC risk have been reported in several previous studies [62–64]. In line of our study, Azimzadeh et al. revealed a significant association between the CC genotype of the rs1131445 polymorphism and CRC risk (P = 0.004). Similar to our findings, they observed that the C allele of the rs1131445 was strongly associated with CRC (P = 009) [11]. In another study, L Hughes and colleagues indicated that rs1131445 in IL-16 was significantly associated with susceptibility of prostate cancer and considered as a prognosis factor in early steps of prostate cancer among African Americans patients. They revealed that the TT genotype at rs1131445 in IL-16 was strongly associated with susceptibility of prostate cancer and considered as a prognosis factor in prostate cancer development [27]. However, in contrast to our findings, Tao Zhang et al. did not find any association between rs1131445 and rs4072111 with risk of non-cardia cancer. In their study, they did not observe any differences between the cases and controls for allele and genotype distribution in those polymorphisms. However, they found that carrier of CC genotype in rs11556218 and GG genotype in rs11556218 of IL-16 had 1.97 and 1.84-fold increased likelihood of non-cardia gastric cancer in a Chinese population, respectively [23]. A meta-analysis by Yanhui Zhao et al. showed that rs4072111 was not associated with cancer risk in Asian population [22]. In Iranian CRC patients, Azimzadeh et al. also revealed no association between CRC susceptibility and rs4072111 variant [10]. Similar to the results of Azimzadeh, the study of Xue Qin et al. on nasopharyngeal carcinoma (NPC) patients on Chinese population confirmed the previous findings on rs4072111 C/T polymorphism [28]. Furthermore, the study of Qi-Sheng Luo et al. on a series of Glioma patients also noted that rs4072111 of IL-16 was not associated with risk of glioma in Chinese population [24]. However, we found a strong association between this variant both in allelic and genotype form and risk of GC in our population. As we described previously, patient with CT genotype had an increased risk of GC, whereas TT carriers showed a slight decreased risk of gastric cancer. The significant association was also detected for T allele of rs4072111 and increased risk of GC (P < 0.001; adjusted OR 1.981; 95 % CI 1.354–2.900). On the other hand, consistent with our findings, Romani et al. observed statistically significant association between rs4072111 variant and susceptibility of chronic HBV infection development. They reported that carriers of T allele in this putative SNP had 1.47-fold higher risk of chronic disease development (\( P \) value 0.029; OR 1.471; 95 % CI 1.039–2.081) [12]. When we adjusted the patients according to the gender for rs4072111, we also observed that male carriers of T allele had a 1.98-fold higher risk of developing GC than females (\( P \) value 0.012; OR 1.986; 95 % CI 1.164–3.389). Another valuable study by Lin-Bo Gao et al. evaluated the association of IL-16 SNPs including rs4072111 C/T with serum levels of IL-16 and the risk of GC and CRC in a Chinese population. In contrast to our study which indicated the increased risk of GC in T allele carriers, they observed that female with T allele of rs4072111 had a decreased risk for CRC and GC in comparison to carriers of the C allele. However, they did not find any association between the putative SNP and serum level of IL-16 [29]. The limitations of the present study were as follows: (1) we did not evaluate the transcriptome or proteome expression of IL-16 tumors and matched controls in the present study since this would give us a more accurate description about the role of these two important variants on GC entity. (2) In this study, these two variants were independently evaluated for susceptibility of GC without considering the effect of other variants in interleukin family members including IL-1B, IL-20, IL17A, and IL-15.
Conclusion
In summary, we found that the rs1131445 T/C and rs4072111 T/C polymorphisms of IL-16 were significantly associated with increased risk of gastric cancer in Iranian population. Our study provided the first findings of association of IL-16 rs1131445 T/C and rs4072111 T/C variants with gastric cancer susceptibility and showed that the IL-16 rs1131445 T/C and rs4072111 T/C polymorphisms may be informative markers for gastric cancer. Further studies with larger sample sizes in different ethnic groups are needed to confirm our findings.
References
Ly QP, Sasson AR. Modern surgical considerations for gastric cancer. J Natl Compr Cancer Netw. 2008;6(9):885–94.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10–29. doi:10.3322/caac.20138.
Steevens J, Schouten LJ, Goldbohm RA, van den Brandt PA. Alcohol consumption, cigarette smoking and risk of subtypes of oesophageal and gastric cancer: a prospective cohort study. Gut. 2010;59(1):39–48. doi:10.1136/gut.2009.191080.
Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med. 2001;345(11):784–9. doi:10.1056/NEJMoa001999.
Sung NY, Choi KS, Park EC, Park K, Lee SY, Lee AK, et al. Smoking, alcohol and gastric cancer risk in Korean men: the National Health Insurance Corporation Study. Br J Cancer. 2007;97(5):700–4. doi:10.1038/sj.bjc.6603893.
Ychou M, Boige V, Pignon JP, Conroy T, Bouche O, Lebreton G, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29(13):1715–21. doi:10.1200/jco.2010.33.0597.
Bang YJ, Kim YW, Yang HK, Chung HC, Park YK, Lee KH, et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet. 2012;379(9813):315–21. doi:10.1016/s0140-6736(11)61873-4.
Kovoor PA, Hwang J. Treatment of resectable gastric cancer: current standards of care. Expert Rev Anticancer Ther. 2009;9(1):135–42. doi:10.1586/14737140.9.1.135.
Hartgrink HH, Jansen EP, van Grieken NC, van de Velde CJ. Gastric cancer. Lancet. 2009;374(9688):477–90. doi:10.1016/s0140-6736(09)60617-6.
Azimzadeh P, Romani S, Mohebbi SR, Kazemian S, Vahedi M, Almasi S, et al. Interleukin-16 (IL-16) gene polymorphisms in Iranian patients with colorectal cancer. J Gastrointestin Liver Dis. 2011;20(4):371–6.
Azimzadeh P, Romani S, Mohebbi SR, Mahmoudi T, Vahedi M, Fatemi SR, et al. Association of polymorphisms in microRNA-binding sites and colorectal cancer in an Iranian population. Cancer Genet. 2012;205(10):501–7. doi:10.1016/j.cancergen.2012.05.013.
Romani S, Hosseini SM, Mohebbi SR, Kazemian S, Derakhshani S, Khanyaghma M et al. Interleukin-16 gene polymorphisms are considerable host genetic factors for patients’ susceptibility to chronic hepatitis B infection. 2014; 2014:790753. doi:10.1155/2014/790753.
Center DM, Cruikshank W. Modulation of lymphocyte migration by human lymphokines. I. Identification and characterization of chemoattractant activity for lymphocytes from mitogen-stimulated mononuclear cells. J Immunol (Baltimore, Md: 1950). 1982;128(6):2563–8.
Yellapa A, Bahr JM, Bitterman P, Abramowicz JS, Edassery SL, Penumatsa K, et al. Association of interleukin 16 with the development of ovarian tumor and tumor-associated neoangiogenesis in laying hen model of spontaneous ovarian cancer. Int J Gynecol Cancer. 2012;22(2):199–207. doi:10.1097/IGC.0b013e318236a27b.
Fina D, Pallone F. What is the role of cytokines and chemokines in IBD? Inflamm Bowel Dis. 2008;14 Suppl 2:S117–8. doi:10.1002/ibd.20677.
Mathy NL, Scheuer W, Lanzendorfer M, Honold K, Ambrosius D, Norley S, et al. Interleukin-16 stimulates the expression and production of pro-inflammatory cytokines by human monocytes. Immunology. 2000;100(1):63–9.
Mochizuki Y, Nakanishi H, Kodera Y, Ito S, Yamamura Y, Kato T, et al. TNF-α promotes progression of peritoneal metastasis as demonstrated using a green fluorescence protein (GFP)-tagged human gastric cancer cell line. Clin Exp Metastasis. 2004;21(1):39–47.
Chung YC, Chang YF. Serum interleukin-6 levels reflect the disease status of colorectal cancer. J Surg Oncol. 2003;83(4):222–6. doi:10.1002/jso.10269.
Shanmugham LN, Petrarca C, Frydas S, Donelan J, Castellani ML, Boucher W, et al. IL-15 an immunoregulatory and anti-cancer cytokine. Recent advances. J Exp Clin Cancer Res. 2006;25(4):529–36.
Gao LB, Liang WB, Xue H, Rao L, Pan XM, Lv ML, et al. Genetic polymorphism of interleukin-16 and risk of nasopharyngeal carcinoma. Clin Chim Acta. 2009;409(1–2):132–5. doi:10.1016/j.cca.2009.09.017.
Zhu J, Qin C, Yan F, Wang M, Ding Q, Zhang Z, et al. IL-16 polymorphism and risk of renal cell carcinoma: association in a Chinese population. Int J Urol. 2010;17(8):700–7.
Zhao Y, Tao L, Wang B, Nie P, Tang Y, Zhu M. Interleukin-16 gene polymorphisms rs4778889, rs4072111, rs11556218, and cancer risk in Asian populations: a meta-analysis. Genet Test Mol Biomarkers. 2014;18(3):174–82. doi:10.1089/gtmb.2013.0386.
Zhang T, Wang H. Variants of interleukin-16 associated with gastric cancer risk. Asian Pac J Cancer Prev. 2013;14(9):5269–73.
Luo QS, Wang JL, Deng YY, Huang HD, Fu HD, Li CY, et al. Interleukin-16 polymorphism is associated with an increased risk of glioma. Genet Test Mol Biomarkers. 2014;18(10):711–4. doi:10.1089/gtmb.2014.0170.
Thomas G, Jacobs KB, Yeager M, Kraft P, Wacholder S, Orr N, et al. Multiple loci identified in a genome-wide association study of prostate cancer. Nat Genet. 2008;40(3):310–5. doi:10.1038/ng.91.
Comperat E, Roupret M, Drouin SJ, Camparo P, Bitker MO, Houlgatte A, et al. Tissue expression of IL16 in prostate cancer and its association with recurrence after radical prostatectomy. Prostate. 2010;70(15):1622–7. doi:10.1002/pros.21197.
Hughes L, Ruth K, Rebbeck TR, Giri VN. Genetic variation in IL-16 miRNA target site and time to prostate cancer diagnosis in African-American men. Prostate Cancer Prostatic Dis. 2013;16(4):308–14. doi:10.1038/pcan.2013.36.
Qin X, Peng Q, Lao X, Chen Z, Lu Y, Lao X, et al. The association of interleukin-16 gene polymorphisms with IL-16 serum levels and risk of nasopharyngeal carcinoma in a Chinese population. Tumour Biol. 2014;35(3):1917–24. doi:10.1007/s13277-013-1257-2.
Gao LB, Rao L, Wang YY, Liang WB, Li C, Xue H, et al. The association of interleukin-16 polymorphisms with IL-16 serum levels and risk of colorectal and gastric cancer. Carcinogenesis. 2009;30(2):295–9. doi:10.1093/carcin/bgn281.
Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16(3):1215.
Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–99. doi:10.1016/j.cell.2010.01.025.
Kundu JK, Surh YJ. Inflammation: gearing the journey to cancer. Mutat Res. 2008;659(1–2):15–30. doi:10.1016/j.mrrev.2008.03.002.
Muc-Wierzgon M, Nowakowska-Zajdel E, Kokot T, Kozowicz A, Wiczkowski A, Grochowska-Niedworok E, et al. Genetic dysregulation of TNF alpha and TNF alpha type II receptors in colon cancer at the II and III stage of disease. J Biol Regul Homeost Agents. 2006;20(1–2):10–4.
Kai H, Kitadai Y, Kodama M, Cho S, Kuroda T, Ito M, et al. Involvement of proinflammatory cytokines IL-1beta and IL-6 in progression of human gastric carcinoma. Anticancer Res. 2005;25(2a):709–13.
Speetjens FM, Kuppen PJ, Sandel MH, Menon AG, Burg D, van de Velde CJ, et al. Disrupted expression of CXCL5 in colorectal cancer is associated with rapid tumor formation in rats and poor prognosis in patients. Clin Cancer Res. 2008;14(8):2276–84. doi:10.1158/1078-0432.ccr-07-4045.
Kollmar O, Rupertus K, Scheuer C, Junker B, Tilton B, Schilling MK, et al. Stromal cell-derived factor-1 promotes cell migration and tumor growth of colorectal metastasis. Neoplasia (New York, NY). 2007;9(10):862–70.
Glass WG, Sarisky RT, Vecchio AM. Not-so-sweet sixteen: the role of IL-16 in infectious and immune-mediated inflammatory diseases. J Interf Cytokine Res. 2006;26(8):511–20. doi:10.1089/jir.2006.26.511.
Laberge S, Cruikshank WW, Kornfeld H, Center DM. Histamine-induced secretion of lymphocyte chemoattractant factor from CD8+ T cells is independent of transcription and translation. Evidence for constitutive protein synthesis and storage. J Immunol (Baltimore, Md : 1950). 1995;155(6):2902–10.
Sharma V, Sparks JL, Vail JD. Human B-cell lines constitutively express and secrete interleukin-16. Immunology. 2000;99(2):266–71.
Rumsaeng V, Cruikshank WW, Foster B, Prussin C, Kirshenbaum AS, Davis TA, et al. Human mast cells produce the CD4+ T lymphocyte chemoattractant factor, IL-16. J Immunol (Baltimore, Md : 1950). 1997;159(6):2904–10.
Center DM, Kornfeld H, Cruikshank WW. Interleukin 16 and its function as a CD4 ligand. Immunol Today. 1996;17(10):476–81.
Atanackovic D, Hildebrandt Y, Templin J, Cao Y, Keller C, Panse J, et al. Role of interleukin 16 in multiple myeloma. J Natl Cancer Inst. 2012;104(13):1005–20. doi:10.1093/jnci/djs257.
Koike M, Sekigawa I, Okada M, Matsumoto M, Iida N, Hashimoto H, et al. Relationship between CD4(+)/CD8(+) T cell ratio and T cell activation in multiple myeloma: reference to IL-16. Leuk Res. 2002;26(8):705–11.
Alexandrakis MG, Passam FH, Kyriakou DS, Christophoridou AV, Perisinakis K, Hatzivasili A, et al. Serum level of interleukin-16 in multiple myeloma patients and its relationship to disease activity. Am J Hematol. 2004;75(2):101–6. doi:10.1002/ajh.10444.
Liebrich M, Guo LH, Schluesener HJ, Schwab JM, Dietz K, Will BE, et al. Expression of interleukin-16 by tumor-associated macrophages/activated microglia in high-grade astrocytic brain tumors. Arch Immunol Ther Exp. 2007;55(1):41–7. doi:10.1007/s00005-007-0003-0.
Yellapa A, Bitterman P, Abramowicz JS, Bahr JM, Sharma S, Basu S, et al. Abstract A64: association of interleukin 16 with early metastasis of ovarian tumors. Clin Cancer Res. 2013;19(19 Supplement):A64-A.
Horikawa Y, Wood CG, Yang H, Zhao H, Ye Y, Gu J, et al. Single nucleotide polymorphisms of microRNA machinery genes modify the risk of renal cell carcinoma. Clin Cancer Res. 2008;14(23):7956–62. doi:10.1158/1078-0432.ccr-08-1199.
Bond GL, Hu W, Bond EE, Robins H, Lutzker SG, Arva NC, et al. A single nucleotide polymorphism in the MDM2 promoter attenuates the p53 tumor suppressor pathway and accelerates tumor formation in humans. Cell. 2004;119(5):591–602. doi:10.1016/j.cell.2004.11.022.
Nicoloso MS, Sun H, Spizzo R, Kim H, Wickramasinghe P, Shimizu M, et al. Single-nucleotide polymorphisms inside microRNA target sites influence tumor susceptibility. Cancer Res. 2010;70(7):2789–98. doi:10.1158/0008-5472.can-09-3541.
Xiong X-D, Luo X-P, Cheng J, Liu X, Li E-M, Zeng L-Q. A genetic variant in pre-miR-27a is associated with a reduced cervical cancer risk in southern Chinese women. Gynecol Oncol. 2014;132(2):450–4.
Ryan BM, Robles AI, McClary AC, Haznadar M, Bowman ED, Pine SR, et al. Identification of a functional SNP in the 3′ UTR of CXCR2 that is associated with reduced risk of lung cancer. Cancer Res. 2015;75(3):566–75.
Zeng X-F, Li J, Li S-B. A functional polymorphism in IL-1A gene is associated with a reduced risk of gastric cancer. Tumor Biol. 2014;35(1):265–8.
Haque S, Akhter N, Lohani M, Ali A, Mandal R. Matrix metalloproteinase-2-1306 C > T gene polymorphism is associated with reduced risk of cancer: a meta-analysis. Asian Pac J Cancer Prev. 2014;16(3):889–96.
Zaanan A, Dalban C, Emile J-F, Blons H, Fléjou J-F, Goumard C, et al. ERCC1, XRCC1 and GSTP1 single nucleotide polymorphisms and survival of patients with colon cancer receiving oxaliplatin-based adjuvant chemotherapy. J Cancer. 2014;5(6):425.
Beuselinck B, Karadimou A, Lambrechts D, Claes B, Wolter P, Couchy G, et al. VEGFR1 single nucleotide polymorphisms associated with outcome in patients with metastatic renal cell carcinoma treated with sunitinib—a multicentric retrospective analysis. Acta Oncol. 2014;53(1):103–12.
van der Mijn JC, Mier JW, Broxterman HJ, Verheul HM. Predictive biomarkers in renal cell cancer: insights in drug resistance mechanisms. Drug Resist Updat. 2014;17(4):77–88.
Leifler KS, Asklid A, Fornander T, Askmalm MS. The RAD51 135G > C polymorphism is related to the effect of adjuvant therapy in early breast cancer. J Cancer Res Clin Oncol. 2015;141(5):797–804.
Bibert S, Roger T, Calandra T, Bochud M, Cerny A, Semmo N, et al. IL28B expression depends on a novel TT/-G polymorphism which improves HCV clearance prediction. J Exp Med. 2013;210(6):1109–16.
Zhang B, Wang A, Xia C, Lin Q, Chen C. A single nucleotide polymorphism in primary-microRNA-146a reduces the expression of mature microRNA-146a in patients with Alzheimer’s disease and is associated with the pathogenesis of Alzheimer’s disease. Mol Med Rep. 2015;12(3):4037–42.
Wang D, Guo Y, Wrighton S, Cooke G, Sadee W. Intronic polymorphism in CYP3A4 affects hepatic expression and response to statin drugs. Pharmacogenomics J. 2011;11(4):274–86.
Pang B, Sun SP, Gao L, Zhu RL, Zhang LX, An C, et al. A single nucleotide polymorphism in PIK3CA gene is inversely associated with P53 protein expression in breast cancer. Med Oncol (Northwood, London, England). 2014;31(7):30. doi:10.1007/s12032-014-0030-8.
He BS, Pan YQ, Xu YF, Zhu C, Qu LL, Wang SK. Polymorphisms in interleukin-1B (IL-1B) and interleukin 1 receptor antagonist (IL-1RN) genes associate with gastric cancer risk in the Chinese population. Dig Dis Sci. 2011;56(7):2017–23. doi:10.1007/s10620-010-1557-y.
Pan XF, Yang SJ, Loh M, Xie Y, Wen YY, Tian Z, et al. Interleukin-10 gene promoter polymorphisms and risk of gastric cancer in a Chinese population: single nucleotide and haplotype analyses. Asian Pac J Cancer Prev. 2013;14(4):2577–82.
Lee KA, Ki CS, Kim HJ, Sohn KM, Kim JW, Kang WK, et al. Novel interleukin 1beta polymorphism increased the risk of gastric cancer in a Korean population. J Gastroenterol. 2004;39(5):429–33. doi:10.1007/s00535-003-1315-4.
Acknowledgments
We thank all patients and their families who supported us in this study.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kashfi, S.M.H., Behboudi Farahbakhsh, F., Nazemalhosseini Mojarad, E. et al. Interleukin-16 polymorphisms as new promising biomarkers for risk of gastric cancer. Tumor Biol. 37, 2119–2126 (2016). https://doi.org/10.1007/s13277-015-4013-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-4013-y