
Abstract
Death receptor 4 (DR4) is a tumor suppressor gene and plays an important mediator of apoptosis. Polymorphism in DR4 gene may reduce apoptotic capacity and provoke proliferation of cell and cancer. We evaluated genetic polymorphisms of DR4 gene in association with risk of prostate cancer (PCa) in Northern Indian population. We have recruited 192 PCa patients and 225 cancer-free ages matched unrelated healthy control of similar ethnicity. They were genotyped for DR4, 141 (G > A), 209 (C > G), and 228 (A > C) polymorphisms using amplification refractory mutation system (ARMS) method. Variant genotype AA (OR = 2.54; p = 0.007) and A allele (OR = 1.51; p = 0.015) of DR4 141 demonstrated significant increased risk for PCa. Similarly, variant genotype GG (OR = 2.58; p = 0.003) and G allele carrier (CG + GG) (OR = 1.50; p = 0.043) of DR4 209 conferred increased risk. G allele (OR = 1.50, p = 0.005) was also statistically associated with PCa risk. High risk for PCa was also observed with respect to haplotypes A-G-A (OR = 2.86; Bonferroni correction Pc = 0.008) and A-G-C (OR = 3.18, Pc = 0.008). We observed significantly enhanced risk for PCa due to interaction between DR4 209 and 228 gene polymorphisms. Furthermore, a significantly increased risk of high Gleason grade tumor was found in the combined variant allele carrier (GA + AA) of DR4 141 compared with the GG genotype (OR = 2.27, Pc = 0.052). Interaction of smoking and genotypes did not further modulate the risk of PCa. Our observations suggested that genetic variants of the DR4 gene significantly influence the risk of PCa in North Indian population and might be involved in the etiology of PCa.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prostate cancer (PCa) is the most frequently diagnosed disease among men. It is assumed to be the second leading cause of death and reduced life expectancy among men in Western countries [1]. In India, it is the sixth most common diagnosed cancer among men [2]. The etiology of PCa is complex, and both environmental and genetic factors play an important role in the pathogenesis of PCa [3]. Although several individuals may be exposed to these risk factors, only a few develop PCa, suggesting that there is a variation in individual susceptibility to prostate carcinogenesis in the general population. Thus, it is possible that genetic differences may play an additional role.
Apoptosis (also called programmed cell death) is an evolutionary conserved tightly genetic pathway that eliminates hazardous and mutated cells to maintain the balance between the cell survival and cell death and sustain cellular homeostasis. Insufficient apoptosis and apoptotic signals promote genetic alterations and lead to increase cell proliferation and invasiveness and increase resistance to treatment of cancer. Evidence indicated the imbalance between the rates of proliferation and apoptosis in prostate cancer cell compared to normal prostate cells [4].
Death receptor 4 (DR4) is encoded by the TNFRSF10A and is located at 8p21-22. Loss of 8p21-22 chromosome is found in a variety of cancers including prostate carcinoma [5]. DR4 protein contains one single transmembrane helix as well as the apoptosis-triggering cytoplasmic death domain. The tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) activates the extrinsic apoptotic pathway through the engagement of the proapoptotic death receptor 4 (DR4, TNFRSF10A, and TRAILR-1), a member of the tumor necrosis factor (TNF) receptor superfamily.
TRAIL induces apoptosis by ligation to DR4 and results in trimerization of the receptors and clustering of their intracellular death domains. This leads to the creation of death-inducing signaling complexes followed by the conscription of the adaptor protein Fas-associated death receptor and subsequently triggers the binding and activation of caspase-8 and caspase-10 [6]. Inhibition of cell death signaling due to alterations in DR4 involves deregulated cell proliferation and predisposes to cancer [7]. The key elements of the DR4 ligand-binding domain are encoded by exons 3 and 4 [8].
Single-nucleotide polymorphisms (SNPs) found in exons 3 and 4 of DR4 (i.e., His141Arg G > A, Thr209Arg C > G, and Glu228Ala A > C) have been reported in different types of human cancers, including breast [9], colorectal [10], head and neck [11] as well as prostate carcinogenesis [12]. SNPs in DR4 gene may impair the apoptotic signals that represent the probable and promising etiologic pathways modifying the PCa penetrance. Since altered apoptosis is believed to increase carcinogenesis, we initiated this case control study to evaluate these polymorphisms of DR4 gene as risk factors of PCa susceptibility in North Indian population.
Materials and methods
Study subjects
One hundred ninety-two confirmed cases of PCa were enrolled at the Department of Urology (Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow) between January 2008 and December 2012. Tumor grade was evaluated in PCa samples by the Gleason scoring system [13]. Two hundred twenty-five ethnicity-matched unrelated healthy individuals were recruited as controls. None of the controls had history of cancer and all controls were matched with age and smoking habit. Total prostate-specific antigen (PSA) levels were determined in PCa and healthy controls by using CanAg EIA kits (Sweden). Informed consent was obtained from each of the eligible subjects. For each individual, demographic information and data on smoking status were obtained through face-to-face interview by using standard clinical performance. The research protocol was approved by the institutional research ethical board committee.
DNA extraction and genotyping
Five milliliters of peripheral blood samples was collected in EDTA vials from patients as well as controls and stored at −70 °C. The genomic DNA was extracted by using salting out method [14]. The quantification of DNA was done using Nanodrop Analyzer (ND-1000) spectrophotometer (Nano Drop Technologies, Inc.). The ratio of absorbance of DNA at 260 and 280 nm was 1.7–1.9. Isolated DNA was stored at −70 °C until further analysis.
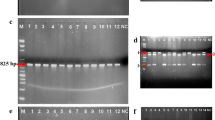
Genotyping was performed using amplification refractory mutation-specific (ARMS) PCR methodology for DR4 (G > A), (C > G), and (A > C) previously described [15]. Each PCR was carried out in a total volume of 12 μl. The PCR products were checked on 2.0 % agarose gel and consequently stained with ethidium bromide. Positive and negative controls were used in each genotyping assay, and 10 % of samples from patients and controls of each genotype were selected randomly and re-genotyped by two people from other laboratory in a blind fashion and results showed 100 % concordance.
Statistical analysis
Chi-square analysis was used to assess deviation from Hardy-Weinberg Equilibrium (HWE) and to compare the genotype, allele, and haplotype frequency between patients and controls. Odds ratio (OR) and 95 % confidence intervals (CI) were obtained by unconditional logistic regression analysis and adjusted for age and smoking. PCa patients with different Gleason grades and bone metastasis were identified using the same statistics as mentioned. Haplotype estimation and linkage disequilibrium were conducted using the Arlequin software version 2.00 by expectation–maximization algorithm. The significance level for all statistical tests was set at p < 0.05. Bonferroni correction p values were applied (Pc) for multiple comparisons. The homozygous genotype for the common allele in the control group was used as the reference in calculating ORs and 95 % confidence intervals. Power analysis was performed by G power software version 3.1 [16]. Data were analyzed using SPSS version 21(SPSS, Chicago, IL, USA).
Results
Demographic and clinical details of study subjects
A total of 417 individuals (192 PCa and 225 controls) were analyzed in the study. There was no statistical difference between age of the PCa patients (62.6 ± 8.9 years) and healthy controls (59.1 ± 10.4 years) and smoking habits (p = 0.327). As expected, there was high degree of statistical difference between serum PSA of PCa patients (212 ± 55.6 ng/ml) and controls (2.1 ± 0.9 ng/ml). Majority of the patients had high Gleason grade at the time of diagnosis (Gleason score 7 in 29.7 % and Gleason score >7 in 44.8 %), and 41.8 % of patients had bone metastasis (Table 1).
Association of DR4 genotype variants with PCa risk
The frequency distribution of genotypes and an allele of DR4 gene are shown in Table 2. Genotype frequencies were in accordance to HWE in control subjects. We observed significant difference in DR4 141 and 209 gene variants between cases and controls. Compared with the wild-type genotype GG, the variant genotype AA of DR4 141 was associated with 2.5-fold (OR, 2.54; p = 0.007) increase risk for PCa. The A allele (risk allele) also showed 1.5-fold increased risk (OR = 1.51; p = 0.015). The variant genotype GG of DR4 209 demonstrated statistically significant association with the risk of developing PCa (OR = 2.58; p = 0.003). We combined the variant GG genotype with the CG genotype (i.e., CG + GG), assuming a dominant genetic model (i.e., the G allele is dominant). We found that a significant increased risk of PCa was associated with the combined variant genotypes CG + GG compared with the CC wild genotype (OR = 1.50; p = 0.043). The variant allele frequency was higher in cases (42.4 %) than in controls (32.9 %); the results showed statistically significant risk with PCa (OR = 1.50; p = 0.005). However, no significant association was identified for the DR4 228 gene polymorphism with PCa risk. A post hoc power of the study was calculated to detect the probability of association between DR4 gene polymorphisms and PCa at α = 0.05 level of significance, assuming a mall effect size (w = 0.20). This analysis revealed that the current study has 88 % power to detect the association.
Association of DR4 haplotypes with PCa risk
The haplotype analysis revealed eight haplotypes from three investigated polymorphisms (141 G > A, 209 C > G, 228 A > C). Out of eight, five haplotypes demonstrated increased risk with PCa compared with the common haplotype G-C-A. However, after applying the Bonferroni correction, only two haplotypes (A-G-A OR = 2.86; Pc = 0.008, A-G-C OR = 3.18; Pc = 0.008) conferred significant increased risk of PCa (Table 3).
Interaction between DR4 141 G > A, 209 C > G, and 228 A > C genes polymorphisms with PCa risk
To analyze the combined effect of DR4 polymorphisms, a gene–gene interaction analysis was conducted. In comparison to control interaction between heterozygous genotype GA of DR4 141 and variant GG genotype of DR4 209 that showed increased frequency (3.1 vs 8.3 %; p = 0.012), variant genotype AA of DR4 141 and heterozygous genotype of DR4 209 revealed increased frequency in PCa patients (4.0 vs 9.9 %; p = 0.010) (Table 4). Similarly, GG-CC, GA-AA, and AA-AC (p = 0.021, 0.037, and 0.020) revealed increased frequency in PCa patients compared to controls (Table 5). Variant GG and AA of DR4 209 and 228 demonstrated increased risk (p = 0.013). All these findings, however, did not stay statistically significant when Bonferroni correction was applied. We found that a significant increased risk of PCa was associated with the interaction of heterozygous CG and variant genotype CC of DR4 209 and 228 compared with the CC-AA (OR = 4.37; p = 0.002). This result considered significant even after Bonferroni correction (Pc = 0.018) (Table 6).
Analysis of DR4 gene polymorphisms with risk for progression of PCa
For genotypic comparison, Gleason grades were subcategorized into three groups (low grade <7, intermediate grade 7, and high grade >7) based on the degree of differentiation between cells (Table 7). A statistically significant increased risk of high-grade PCa was found in variant allele carries (GA + AA) of the DR4 141 (G > A) (OR = 2.27; Pc = 0.052) compared with wild-type GG genotype. However, none of other polymorphisms of DR4 has shown significant risk with tumor grade.
Analysis of DR4 gene polymorphisms with risk for bone metastasis
We also studied DR4 gene variants and their risk associated with bone metastasis. The PCa patients were divided into two groups, one with bone metastasis and the other with non-metastasis. When these two groups were analyzed for susceptibility of bone metastasis, we did not find any significant risk (Table 8).
Association of DR4 gene polymorphisms with smoking habit in PCa
We evaluated the gene–smoking interaction to study the modulation of PCa risk with respect to DR4 polymorphisms. We divided the PCa patients into two groups, one non-smokers (never smoked) and the other as smokers (smoking more than 5 years). On analyzing the two groups for susceptibility to PCa, none of these polymorphisms demonstrated association (data not shown).
Discussion
Reports on genetic susceptibility to PCa from India are sparse. To the best of our knowledge, no published study has previously examined the association between variants of DR4 genes and risk of PCa in North Indian population. In this study, we have analyzed three SNPs of DR4 gene involved in apoptotic pathway in relation to PCa risk, and we found that SNPs and haplotypes were significantly associated with risk of PCa.
DR4 gene plays an essential role in the transmission of the apoptotic stimulus; deficient apoptosis would be expected to contribute to a transformed phenotype and tumor expansion [7]. Studies signify deletion of DR4 gene in the cancer cell line [17]. Genetic variations in DR4 gene might reduce apoptotic cell signaling and, therefore, contribute to the development of tumor cells. These three SNPs found to reside next to the DR4 ligand-binding ectodomain and may affect TRAIL binding and may result to abnormal apoptotic signaling. In this case control study, we found that variant genotype AA of DR4 141 (G > A) had a strong association with PCa (OR = 2.54; p = 0.007); variant allele A was also associated with PCa. Additionally, our result showed that variant genotype (GG) of DR4 209(C > G) revealed significant risk with PCa (OR = 2.58; p = 0.003). Similarly, variant allele carrier and variant allele also showed increased risk with PCa. This is in accordance with a study by Fisher et al. who also reported significant risk in lung cancer [8]. Our result is further supported by previous observations that loss of heterozygosity for markers on chromosome 8p is one of the most frequent somatic mutations occurring in more than 60 % of the prostate tumors, and deletion of 8p is a strong predictor of disease progression [18]. Conversely, Ulybina et al. and Frank et al. did not observe risk with lung cancer and breast cancer [9,15]. It is well established that frequency of gene polymorphism may vary among ethnic groups. Therefore, variation in distribution of gene frequencies between these studies may be justified on the basis of ethnicity difference. The Glu228Ala substitution resides within a conserved region of the extracellular cysteine-rich domain of DR4. Since the frequency of variant genotype of this polymorphisms of DR4 228 was low in our population, we could not observe any significant independent associations. Frank et al. and Taştemir et al. were also reported non-significant association with colorectal and lung cancer risk [10,19].
The haplotype analysis of DR4 (141, 209, and 228) and five haplotypes (G-C-C, G-G-C, A-C-A, A-G-A, and A-G-C) demonstrated higher risk, although statistically significant results persist only with two haplotypes (A-G-A and A-G-C) after applying Bonferroni correction for multiple comparisons with PCa. Accumulating evidence suggested that an analysis of the haplotypes may be more affirmative in predicting the disease association compared with an analysis of a single SNP [20]. Therefore, our findings on associations between DR4 haplotypes and risk of PCa further strengthen our observation. We also analyzed gene–gene interaction by different combinations to evaluate the synergistic effect on PCa. Only combination of heterozygous genotype CG and variant genotype CC of DR4 209 and 228 showed significant increased risk with PCa after applying Bonferroni correction. Subgroup analysis according to tumor grade may help in identifying prognostic factors involved in different PCa progression pathways. After stratification analysis by tumor grade, it appeared that the A allele carrier (GA + AA) of DR4 141 was associated with an increased risk of developing PCa. Our results further did not reveal any significant association with bone metastasis of PCa. However, this finding from our relatively small study needs validation by larger studies in the future. Lifestyle-related habits have been associated with PCa in various epidemiological studies. Case-only analysis, considered to be more appropriate for such interactions, was performed. However, no association of smoking with PCa risk was observed in this study.
A challenge is to interpret interactions of genetic and environmental factors for complex and multifactorial disease such as cancer. Some limitations do exist in our study. First, since the PCa cases and control subjects were enrolled from hospitals, inherent selection bias cannot be excluded. Second, sample size was low in some subgroups and haplotypes. Third, in addition to tobacco smoking, we did not obtain enough information on occupational exposure that may interact with the DR4 genotypes. In spite of this, current study has some advantages. All PCa patients were clinically confirmed, and the study subjects enrolled were of similar ethnicity since both PCa patients as well as controls were of North Indian ethnicity; the possibility of population admixture was ruled out. In addition, stringent quality control and reproducible genotyping measures were used to minimize systematic errors. We performed all possible data analyses to make satisfactory and reliable conclusion.
In summary, the study observed the association of DR4 141 (G > A) and 209 (C > G) genotype were associated with the susceptibility of PCa. At the haplotype level, individuals with haplotype combination of DR4 141, 209, and 228 were at greater risk for PCa. This result suggests that the change in apoptotic signals may modulate cancer susceptibility by promoting tumor cell growth and survival. Further, we observed multiplicative interaction between the DR4 209 and 228 allele carriers suggesting an important role in the pathology of PCa. Our results projected some promising findings of genetic risk factors for PCa. However, this study calls for further research in larger population of different ethnicities and validate with functional studies to understand the mechanisms by which this polymorphisms alters PCa risk. In the future, drug that target apoptotic and death receptor pathway might open new therapeutic strategy for PCa therapy.
References
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29.
Sinha R, Anderson DE, McDonald SS, Greenwald P. Cancer risk and diet in India. J Postgrad Med. 2003;49:222–28.
Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M, et al. Environmental and heritable factors in the causation of cancer—analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343:78–85.
Denmeade SR, Lin XS, Isaacs JT. Role of programmed (apoptotic) cell death during the progression and therapy for prostate cancer. Prostate. 1996;28:251–65.
MacGrogan D, Levy A, Bostwick D, Wagner M, Wells D, Bookstein R. Loss of chromosome arm 8p loci in prostate cancer: mapping by quantitative allelic imbalance. Genes Chromosom Cancer. 1994;10:151–9.
Henson ES, Johnston JB, Gibson SB. The role of TRAIL death receptors in the treatment of hematological malignancies. Leuk Lymphoma. 2008;49:27–35.
Bouralexis S, Findlay DM, Evdokiou A. Death to the bad guys: targeting cancer via Apo2L/TRAIL. Apoptosis. 2005;10:35–51.
Fisher MJ, Virmani AK, Wu L, Aplenc R, Harper JC, Powell SM, et al. Nucleotide substitution in the ectodomain of TRAIL receptor DR4 is associated with lung cancer and head and neck cancer. Clin Cancer Res. 2001;7:1688–97.
Frank B, Hemminki K, Shanmugam KS, Meindl A, Klaes R, Schmutzler RK, et al. Association of death receptor 4 haplotype 626C-683C with an increased breast cancer risk. Carcinogenesis. 2005;26:1975–77.
Frank B, Shanmugam KS, Beckmann L, Hemminki K, Brenner H, Hoffmeister M, et al. Death receptor 4 variants and colorectal cancer risk. Cancer Epidemiol Biomarkers Prev. 2006;15:2002–5.
Wolf S, Mertens D, Pscherer A, Schroeter P, Winkler D, Gröne HJ, et al. Ala228 variant of trail receptor 1 affecting the ligand binding site is associated with chronic lymphocytic leukemia, mantle cell lymphoma, prostate cancer, head and neck squamous cell carcinoma and bladder cancer. Int J Cancer. 2006;118:1831–35.
Langsenlehner T, Langsenlehner U, Renner W, Kapp KS, Krippl P, Hofmann G, et al. The Glu228Ala polymorphism in the ligand binding domain of death receptor 4 is associated with increased risk for prostate cancer metastases. Prostate. 2008;68:264–68.
Gleason DF, Mellinger GT. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J Urol. 1974;111:58.
Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16:1215.
Ulybina YM, Kuligina ES, Mitiushkina NV, Rozanov ME, Ivantsov AO, Ponomariova DN, et al. Coding polymorphisms in Casp5, Casp8 and DR4 genes may play a role in predisposition to lung cancer. Cancer Lett. 2009;278:183–91.
Faul F, Erdfelder E, Lang AG, Buchner A. G Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175.
Ozören N, Fisher MJ, Kim K, Liu CX, Genin A, Shifman Y, et al. Homozygous deletion of the death receptor DR4 gene in a nasopharyngeal cancer cell line is associated with TRAIL resistance. Int J Oncol. 2000;16:917–25.
Oba K, Matsuyama H, Yoshihiro S, Kishi F, Takahashi M, Tsukamoto M, et al. Two putative tumor suppressor genes on chromosome arm 8p may play different roles in prostate cancer. Cancer Genet Cytogenet. 2001;124:20–6.
Taştemir-Korkmaz D, Demirhan O, Kuleci S, Hastürk S. There is no significant association between death receptor 4 (DR4) gene polymorphisms and lung cancer in Turkish population. Pathol Oncol Res. 2013;19:779–84.
Stephens M, Smith NJ, Donnelly P. A new statistical method for haplotype reconstruction from population data. Am J Hum Genet. 2001;68:978–89.
Acknowledgments
We sincerely acknowledge the numerous patients and healthy control donors for making this study possible. The authors are thankful to the urologists in the department for providing the details of the clinical samples.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mittal, R.D., Mandal, R.K., Singh, A. et al. Death receptor 4 variants enhanced prostate cancer risk in North Indian population. Tumor Biol. 36, 5655–5661 (2015). https://doi.org/10.1007/s13277-015-3239-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-3239-z