
Abstract
The International Dysphagia Diet Standardization Initiative (IDDSI) flow test is useful for the global standardization of food consistencies of dysphagia patients. In clinical practice, different compositions of food thickeners are commonly used, directly influencing viscosity parameters and swallowing physiology. We aimed to compare the IDDSI thickness levels, remaining volume in the syringe (RVS), and viscosity parameters of three different food thickeners. As a secondary objective, we compared the cost of preparing 100 mL of thickened drinks using the studied thickeners. Thickeners A (xanthan gum), B (corn starch, tara gum, xanthan gum, and guar gum), and C (corn starch) were prepared in increasing concentrations from 1 to 7 g/100 mL and were assayed in quintuplicate using the IDDSI flow test. Thickeners A, B, and C presented statistically different results for the IDDSI levels, RVS, and viscosity parameters at all concentrations. Thickener A reached higher levels in the IDDSI framework, RVS, and viscosity parameters compared with thickeners B and C. A large range of RVS was observed at different concentrations for thickener B compared with C. Regarding viscosity, thickeners B and C, with corn starch in their composition, showed exponential behavior as concentrations increased, while thickener A presented a linear trend. The thickener composition was significantly influenced by IDDSI classification, RVS, and viscosity parameters. The study shows that xanthan gum thickeners present less variability in IDDSI, RVS, and viscosity compared with starch-based thickeners.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dysphagia rehabilitation entails compensation (Lazarus et al. 2002; Logemann 1999). Postural maneuvers, changes in viscosity, texture, volume, and delivery are examples of such strategies. Using thickeners to alter viscosity is a common clinical practice (Ortega et al. 2017), although it should be employed only under circumstances where no other treatment option is available (Logemann 1998).
Although some studies have reported that thickener use may increase stasis in pharyngeal recesses (Newman et al. 2016; Steele et al. 2015) and alter the texture and taste of liquids (Lotong et al. 2003; Ong et al. 2018; Stokes et al. 2013), this strategy has proven effective in improving swallowing safety in patients with dysphagia by reducing the risk of liquid penetration into the airway (Clavé et al. 2006; Hind et al. 2012; Molfenter and Steele 2013; Newman et al. 2016). Several studies have shown the urgent need for standard terminologies for dysphagia patients, reporting that the current terminologies are imprecise and confusing, hindering clinical practice and causing inaccuracies among patients, caretakers and professionals globally (Cichero 2013; Cichero et al. 2017; Steele et al. 2015). To address these issues, the International Dysphagia Diet Standardization Initiative (IDDSI) launched a new framework for the categorization of foods and drinks for dysphagia patients. A key element of this initiative was the development of a new test to measure the flow of a liquid using a syringe. In this framework, there are five levels—from zero to four—to measure the thickness of any drink based on the remaining volume in the syringe (RVS) after a gravity flow test with a 10 mL syringe (Cichero et al. 2017).
Historically, a variety of starches (STs) and gums have been used to thicken liquids (Cichero 2013). There are several brands of food thickeners based on xanthan gum (XG) and ST. XG is a polysaccharide gum derived from Xanthomonas campestris through a fermentation process (Law et al. 2015). There are different forms of ST, but they are defined as polysaccharides composed of a long polymeric chain of glucose units. Different effects on the oral and pharyngeal phases have been documented for both thickeners (Newman et al. 2016; Ong et al. 2018; Vilardell et al. 2015). However, few studies examined the behavior of different thickeners using the IDDSI framework without the participation of human subjects (Barbon and Steele 2018; Kim et al. 2018). Recently, a report showed that commercially available XG-based and ST-based thickeners exhibit distinct behaviors in IDDSI flow tests regarding their apparent viscosity (Kim et al. 2018). Other researchers compared similar thickeners using the IDDSI framework, but found no significant differences between them (Barbon and Steele 2018). Inconsistent sampling methods and instruments have limited the ability of these studies to assess the variability of thickener agents using the flow test proposed by IDDSI. Therefore, there is a call for new research to evaluate the performance of different thickening agents in flow tests.
This study compared the IDDSI flow test results by analyzing the framework level, RVS, viscosity parameters, and cost analysis in water samples with progressively higher concentrations of three commercially available thickeners based on XG and/or ST.
Materials and methods
Selected thickeners
Three commercially available food thickeners in Brazil were randomly selected for this study. Table 1 presents the composition and manufacturer preparation instructions.
Sample preparation
Samples were prepared using colored mineral water at a controlled temperature (20–25 °C). For each test, 100 mL of mineral water was used, and one drop of Mix® food coloring (Mix®, São Paulo, Brazil) was added to improve visibility and enable greater accuracy of the record of RVS and the IDDSI level. Each test mixture was prepared by weighing each component, resulting in a progressive thickener concentration starting at 1% weight/volume (w/v) until level four on the IDDSI scale was reached. Each sample was prepared according to the manufacturer’s instructions (Table 1) and tested in quintuplicate.
Flow test: IDDSI level and RVS
The flow test was performed according to IDDSI instructions (IDDSI - International Dysphagia Diet Standardization Initiative 2020). Ten milliliter of thickened water was added to a 10 mL syringe (BD®, barrel length from 0 to 10 mL line = 61.5 mm). To avoid leakage, the syringe nozzle was blocked using a finger. The nozzle was left open for 10 s and then blocked again, and the RVS was recorded. IDDSI levels were then attributed: level zero for volumes between 0,0 and 0,9 mL; level one, between 1,0 and 3,9 mL; level two, between 4,0 and 7,9 mL; level three, between 8,0 and 9,9 mL; and level four, 10,0 mL.
Viscosity parameters
Apparent viscosity was evaluated using a rotational viscometer (Brookfield, Mod LV-T, São Paulo, Brazil). The spindle was chosen to keep a dial reading between 10 and 90, following the equipment guidelines. The settings were fixed at 1.5 rpm for 30 s at 25 ± 2 °C.
Cost estimation
The cost of the three thickeners on American e-commerce websites was compared in US dollar terms. Since the packs differ in terms of weight content, the cost per gram and per 100 g (Table 1) was calculated based on thickener prices on nine different e-commerce websites. These costs were used to estimate the cost of preparing 100 mL of drink at each IDDSI level, based on the thickener quantity found in this study.
Statistical analysis
All results are presented as mean ± standard deviation. Statistical analysis was performed with the Kruskal Wallis test for the concentrations 1 g/100 mL–5 g/100 mL, and the Mann Whitney test for the concentrations 6 g/100 mL and 7 g/100 mL, with a global significance level of 5%.
Results
In the flow test, the concentrations to reach IDDSI level four were different for each product. Thickener A reached level four at a concentration of 5 g/100 mL, while B and C required 7 g/100 mL to attain the same level in the IDDSI framework. Figure 1 presents the variability of the IDDSI levels at different concentrations for all the studied thickeners. Figure 2 demonstrates the cost of preparing 100 mL of thickened drink in each IDDSI level, for the studied thickeners, in US dollars.

Flow test of all concentrations of thickener A (A), B (B) and C (C). Bars represent average volume of remaining liquid in syringe (RLS) in mL, and error bars represent standard deviation of quintuplicate. Bars are pattern-filled according to IDSSI level

Cost estimation to prepare 100 mL of a thickened drink reaching each IDDSI level for studied thickeners in US dollars. *Cost of preparing 100 mL of a thickened drink.
Thickeners A, B, and C presented statistically different IDDSI levels and RVS at all investigated concentrations, as shown in Table 2. Thickener A had higher IDDSI levels than thickeners B and C (Fig. 1). Thickener A did not reach level one at the initial concentration (1 g/100 mL). Furthermore, thickeners A and B attained higher RVS values compared with thickener C, following the A > B > C trend, except at a concentration of 7 g/100 mL.
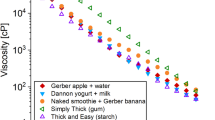
Table 2 shows the statistically different viscosity parameters for all the agents. Thickener A presented the highest viscosity compared with thickeners B and C. The last two did not behave consistently with respect to the viscosity levels. Additionally, thickeners B and C presented an exponential rise in viscosity as concentrations increased; this pattern was not repeated with thickener A, which showed a linear trend (Fig. 3).

Comparison of viscosity in all concentrations for thickeners A, B and C. Each value is represented as an average with the standard deviation (error bars) of quintuplicate
Discussion
Polysaccharides are biopolymers found in many organisms and are responsible for many different functions. They have been used as thickeners owing to their ability to increase the viscosity of a liquid, as they form gels when in solution (Toneli et al. 2005). Food thickeners are mainly composed of ST and its derivatives (Salles et al. 2019), gum-based polysaccharides, or a mixture of these. Previous studies have shown that thickener composition influences the rheological behavior of liquids, among other factors, such as temperature, time to thicken, and even liquid type (Garcia et al. 2005, 2008; Park et al. 2014; Salles et al. 2019; Toneli et al. 2005).
This study presented evidence that, at every concentration, an XG-based thickener (A) reaches higher viscosity levels compared with ST-based (C) or mixed (B) thickeners. A pattern of A > B > C was established regarding IDDSI levels and RVS measurements, except at a concentration of 7 g/100 mL, in which B and C reached similar levels. This similarity is likely because both thickeners reached saturation at this concentration level.
With regard to thickener composition, it has been documented that agents based on gums, such as tara gum, guar gum, and XG, are able to alter the consistency of liquids in lower amounts than ST-based thickeners. Other researchers found the need for a much higher mass of ST-based thickeners than XG-based thickeners to reach the same IDDSI level in the flow test (Barbon 2018; Barbon and Steele 2018).
As observed in previous studies (Alves et al. 2017; Barbon 2018; Barbon and Steele 2018), thickener A (XG-based) did not reach level one on the IDDSI framework at a concentration of 1 g/100 mL (the lowest concentration in the test), instead reaching level two or three (Fig. 1). This suggested that the thickener mixing instructions must consider volumes higher than 100 mL of water/liquid for level one preparations. This is a better practice than suggesting a lower mass of thickener because it may be difficult to obtain less than 1 g in clinical practice, as the measuring spoon offered with the product usually holds 1–2 g. These recommendations do not apply to commercial thickeners based on ST (thickener C) or mixed (thickener B), which reached every level from one to four in the tested concentrations.
Thickener B (a mix of XG, tara gum, guar gum, and corn ST) testing resulted in distinct RVS values at a concentration of 4 g/100 mL (Fig. 1). This high variability implied a risk of negative outcomes in clinical practice since inaccuracies in liquid preparation may lead to safety and efficiency limitations regarding food ingestion, as well as inconsistencies in manufacturer instructions. Clinically, dysphagia patients and professionals such as speech and language pathologists, clinicians, nutritionists, nurses, and caregivers must be aware that adding a certain amount of thickener B to a liquid may result in different IDDSI levels. This information is paramount to the precise preparation of a thickened liquid. There have been few studies on thickeners composed of a mix of gums and ST, and extant research did not provide information about their efficacy in swallowing physiology or their behavior in the IDDSI flow test (Killeen et al. 2015; Salles et al. 2019; Silva et al. 2017; Vallons et al. 2014). Therefore, research is required to evaluate the IDDSI framework for this type of thickener, both on its own and its application for patients with dysphagia.
Thickener C (ST-based) also presented different RVS values for a single concentration. At 3 g/100 mL, the IDDSI levels ranged from zero to one. However, thickener A did not register any level of variability. It is not yet possible to assert that small differences in RVS values have any clinical significance regarding safe swallowing and penetration/aspiration (Barbon 2018; Barbon and Steele 2018). The IDDSI framework is a new methodology, and there is still a lack of studies assessing the clinical relevance of each level in patients with dysphagia. Although some recent publications evaluated swallowing of different consistencies in healthy subjects based on the IDDSI framework, these consistencies do not exceed 1 mL in the flow test (Steele et al. 2019; Valenzano et al. 2020). However, this methodology prevents the assessment of clinical effects stemming from RVS variability within a single level, as observed in this study. Therefore, we recommend that professionals use thickened liquids with RVS values that fall close to the center of each level range (Barbon and Steele 2018), until further evidence allows a better understanding of the clinical significance of these disparities (Steele et al. 2015).
Thickener A attained higher viscosity levels than thickeners B and C. As the concentration increased, the viscosity as well as the volume of fluid flowing through the syringe decreased. The viscosity parameters increased linearly for higher concentrations of thickener A and exponentially for thickeners B and C (Fig. 3). Even though there were differences in the viscosity parameters of thickeners B and C, they were not significant enough to influence the IDDSI levels and RVS, despite the B > C trend holding for every concentration. These small changes in viscosity may not be related to flow test results in corn ST-based thickeners, in accordance with existing literature, suggesting that the flow test might not be sensitive enough to measure viscosity changes of liquids thickened with ST-based products (Kim et al. 2018). Moreover, a recent study with several types of thickeners could not establish any correlation between viscosity and IDDSI/NDD (National Dysphagia Diet) classifications (Kim et al. 2018).
Our results suggested that XG-based thickeners, followed by ST-based thickeners, could be preferentially recommended for patients with dysphagia, instead of mixed thickeners, due to lower variability between flow test levels, RVS values, and their linear viscosity trend as concentrations increased. However, among XG- and ST-based products, professionals should also consider other clinical aspects when recommending a thickening agent. For instance, studies with human subjects revealed that ST-based agents may be less efficient in decreasing the frequency of penetration/aspiration events (Newman et al. 2016) while increasing pharyngeal residue after swallowing (Vilardell et al. 2015). In addition, they may be less soluble in some liquids and may alter their taste and opacity, resulting in a less pleasant drinking experience (Ong et al. 2018) compared with XG-based thickeners. ST-based agents also begin to be hydrolyzed by salivary amylase, which significantly reduces the viscosity of the liquid in the mouth (Hanson et al. 2012a, b; Lee et al. 2016; Vallons et al. 2014, 2015). Furthermore, thickened liquids should always be prescribed with caution (Logemann 1998), since patients who need thickening agents are more prone to developing complications such as dehydration (Cichero 2013) (Flynn et al. 2018). Psychosocial issues have also been associated with thickener use, affecting the quality of life of these patients (Ekberg et al. 2002).
As previously reported (Schmidt and de Oliveira 2015), commercial thickeners can be costly, with the cost depending on the brand and composition. Despite not being the cheapest in terms of cost/100 g, a lower amount of thickener A is needed to reach IDDSI levels, which makes it commercially viable at levels two and three. Thus, multidisciplinary teams and caregivers should not only consider the cost per unit, but also the cost per level while choosing a thickener.
This study had some limitations. First, the study assessed a single brand of thickener for each composition. A higher number of products and compositions should be experimentally evaluated to further clarify some of the issues raised by our results, preferentially following IDDSI flow test guidelines. Second, this study used food coloring to improve the visibility of the liquid; however, we do not know what effect, if any, the food coloring had on the action of thickeners with water, which could influence the results regarding the level of IDDSI and RVS. Future studies should consider using samples of water and food thickeners, without adding other substances. Comparisons between patients with dysphagia and healthy subjects should also be performed to better understand the impact of thickeners’ use on swallowing physiology. Professionals should always stay abreast of the available scientific evidence before offering any guidance to patients and caregivers, considering the safe ingestion of liquids as well as the composition and cost–benefit ratio of thickening agents.
Conclusion
This study revealed that the thickener composition significantly influences IDDSI levels, RVS, and viscosity. The evaluated XG-based thickener appeared to provide more accurate and/or safe preparations for patients and caregivers to use, and medical professionals to prescribe. ST-based and mixed thickeners proved to be less than ideal recommendations when accounting for clinically safer food products because their viscosity behavior fluctuated at different concentrations, which may compromise the safety and efficiency of swallowing in patients with dysphagia.
Abbreviations
- IDDSI:
-
International dysphagia diet standardization initiative
- RVS:
-
Remaining volume in the syringe
- XG:
-
Xanthan gum
- ST:
-
Starch
References
Alves DC, Alves NA, Dantas RO (2017) Consistency stability of water thickened with maltodextrin, xanthan gum and potassium chloride. J Texture Stud 48(6):530–533
Barbon CEA (2018) Characterizing the flow of thickened barium and non-barium liquid recipes using the IDDSI flow test. Dysphagia. https://doi.org/10.1007/s00455-018-9915-6
Barbon CEA, Steele CM (2018) Thickened liquids for dysphagia management: a current review of the measurement of liquid flow. Curr Phys Med Rehabil Rep 6(4):220–226. https://doi.org/10.1007/s40141-018-0197-6
Cichero JAY (2013) Thickening agents used for dysphagia management: effect on bioavailability of water, medication and feelings of satiety. Nutr J. https://doi.org/10.1186/1475-2891-12-54
Cichero JAY, Lam P, Steele CM, Hanson B, Chen J, Dantas RO, Duivestein J, Kayashita J, Lecko C, Murray J, Pillay M, Riquelme L, Stanschus S (2017) Development of international terminology and definitions for texture-modified foods and thickened fluids used in dysphagia management: the IDDSI framework. Dysphagia 32(2):293–314. https://doi.org/10.1007/s00455-016-9758-y
Clavé P, Kraa MDE, Arreola V, Girvent M, Farre R (2006) The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment Pharmacol Ther 24:1385–1394. https://doi.org/10.1111/j.1365-2036.2006.03118.x
de Toneli JTCL, Murr FEX, Park KJ (2005) Estudo da reologia de polissacarídeos utilizados na indústria de alimentos. Rev Brasileira Prod Agroind 7(2):181–204
Ekberg O, Hamdy S, Woisard V, Hannig AW, Ortega P (2002) Social and psychological burden of dysphagia : its impact on diagnosis and treatment. Dysphagia 17:139–146. https://doi.org/10.1007/s00455-001-0113-5
Flynn E, Ch S, Cd W, Walshe M (2018) Modifying the consistency of food and fluids for swallowing difficulties in dementia (Review). Cochrane Library 9:1–51. https://doi.org/10.1002/14651858.CD011077.pub2.www.cochranelibrary.com
Garcia JM, Iv EC, Matta Z, Clark M (2005) Viscosity measurements of nectar- and honey-thick liquids : product, liquid, and time comparisons. Dysphagia 335:325–335. https://doi.org/10.1007/s00455-005-0034-9
Garcia JM, Iv EC, Matta Z, Clark M (2008) Serving temperature viscosity measurements of nectar- and honey-thick liquids. Dysphagia 23:65–75. https://doi.org/10.1007/s00455-007-9098-z
Hanson B, Cox B, Kaliviotis E, Smith CH (2012a) Effects of saliva on starch-thickened drinks with acidic and neutral pH. Dysphagia 27:427–435
Hanson B, O’Leary MT, Smith CH (2012b) The effect of saliva on the viscosity of thickened drinks. Dysphagia 27:10–19
Hind J, Divyak E, Zielinski J, Taylor A, Hartman M, Gangnon R, Robbins J (2012) Comparison of standardized bariums with varying rheological parameters on swallowing kinematics in males. JRRD 49(9):1399–1404
IDDSI - International Dysphagia Diet Standardization Initiative. (2020). https://www.iddsi.org/. Accessed 20 May 2020
Killeen L, Lansink M, Schröder D (2015) Tolerability and product properties of a gum-containing thickener in patients with dysphagia. Rehab Nurs J. https://doi.org/10.1097/rnj.0000000000000011
Kim Y, Jeong GY, Yoo B (2018) Comparative study of IDDSI flow test and line spread test of thickened water prepared with different dysphagia thickeners. J Texture Stud. https://doi.org/10.1111/jtxs.12360
Law V, Knox C, Djoumbou Y, Jewison T, Guo AC, Liu Y, Maciejewski A, Arndt D, Wilson M, Neveu V, Tang A, Gabriel G, Ly C, Adamjee S, Dame ZT, Han B, Wishart YZ, Wishart DS (2015) Xanthan gum. drugbank 4.0: shedding new light on drug metabolism. Nucleic Acids Res 42:1091–1097
Lazarus C, Logemann A, Wook C, Rademaker AW, Kahrilas J (2002) Effects of voluntary maneuvers on tongue base function for swallowing. Folia Phoniatr Logop 10016:171–176
Lee H, Yoon S, Yoo W, Yoo B, Hy L (2016) Effect of salivary reaction time on flow properties of commercial food thickeners used for Dysphagic patients. Clin Nutr Res 5:55–59
Logemann JA (1998) Evaluation and treatment of swallowing disorders. Curr Opin Otolaryngol Head Neck Surg 6:395–400
Logemann JA (1999) Behavioral management for oropharyngeal. Dysphagia 60208:199–212
Lotong V, Chun SS, Chambers E IV, Garcia JM (2003) Texture and flavor characteristics of beverages containing commercial thickening agents for dysphagia diets. J Food Sci 68(4):1537–1541. https://doi.org/10.1111/j.1365-2621.2003.tb09680.x
Molfenter SM, Steele CM (2013) The relationship between residue and aspiration on the subsequent swallow: an application of the normalized residue ratio scale. Dysphagia 28(4):494–500. https://doi.org/10.1007/s00455-013-9459-8
Newman R, Vilardell N, Clavé P, Speyer R (2016) Effect of bolus viscosity on the safety and efficacy of swallowing and the kinematics of the swallow response in patients with oropharyngeal dysphagia: white paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 31(2):232–249. https://doi.org/10.1007/s00455-016-9696-8
Ong JJ, Steele CM, Duizer LM (2018) Sensory characteristics of liquids thickened with commercial thickeners to levels specified in the International Dysphagia Diet Standardization Initiative (IDDSI) framework. Food Hydrocoll. https://doi.org/10.1016/j.foodhyd.2017.12.035
Ortega O, Martín A, Clavé P (2017) Diagnosis and management of oropharyngeal Dysphagia among older persons, state of the art. J Am Med Dir Assoc 18(7):576–582. https://doi.org/10.1016/j.jamda.2017.02.015
Park JH, Kim H, Oh B, Lee M, Hwang I, Lee S, Han TR (2014) Comparison of different gum-based thickeners using a viscometer and line spread test : a preliminary study. Ann Rehabil Med 38(1):94–100
Salles A, Lenz D, Souza D (2019) Lack of Standardization in commercial thickeners used in the management of Dysphagia. Analls Nutr Metab 75:246–251. https://doi.org/10.1159/000504334
Schmidt H, de Oliveira VR (2015) Avaliação reológica e sensorial de espessantes domésticos em diferentes líquidos como alternativa na disfagia. Brazilian J Technol 18(1):42–48
da Silva APS, Cuti LK, Mancopes R, Prolla ID (2017) Thickeners sold in Brazil: analysis of the composition and suitability for children under the age of 3. BRASPEN J 32(4):4–7
Steele CM, Abdulrahman W, Sona A, Lam P, Lecko C, Leigh C, Nagy A, Namasivayam AM, Nascimento WV, Odendaal I, Smith CH, Wang H (2015) The influence of food texture and liquid consistency modification on swallowing physiology and function : a systematic review. Springer 30:2–26. https://doi.org/10.1007/s00455-014-9578-x
Steele CM, Peladeau-Pigeon M, Barbon CAE, Guida BT, Tapson MS, Valenzano TJ, Waito AA, Wolkin TS, Hanson B, Ong JJ-X, Duizerd LM (2019) Modulation of tongue pressure according to liquid flow properties in healthy swallowing. JSLHR 62:22–33
Stokes JR, Boehm MW, Baier SK (2013) Oral processing, texture and mouthfeel: from rheology to tribology and beyond. Curr Opin Colloid Interface Sci 18(4):349–359. https://doi.org/10.1016/j.cocis.2013.04.010
Valenzano TJ, Guida BT, Peladeau-Pigeon M, Steelea CM (2020) Respiratory – swallow coordination in healthy adults during drinking of thin to extremely thick liquids: a research note. JSLHR 63:702–709
Vallons KJR, Helmens HJ, Oudhuis AACM (2014) Effect of human saliva on the consistency of thickened drinks for individuals with dysphagia. Int J Lang Commun Disord 50(2):1–11. https://doi.org/10.1111/1460-6984.12120
Vallons KJR, Oudhuis LAACM, Helmens HJ, Kistemaker C (2015) The effect of oral processing on the viscosity of thickened drinks for patients With Dysphagia. Ann Rehabil Med 39(5):772–777
Vilardell N, Rofes L, Arreola V, Speyer R, Clave P (2015) A comparative study between modified starch and xanthan gum thickeners in post-stroke oropharyngeal Dysphagia. Dysphagia 31(2):169–179. https://doi.org/10.1007/s00455-015-9672-8
Funding
This study did not provide funding to any institution, company or industry.
Author information
Authors and Affiliations
Contributions
JVH, main author of the manuscript, conceptualization, and design, conducting the analysis and critical interpretation of the literature, writing original draft, editing and final review. HSAT, investigation, methodology, analysis, and interpretation of the literature, editing and final review of the manuscript; CM de S, investigation, conducting the methodology, supervision (supporting), analysis, and interpretation of the literature, editing and final review of the manuscript; JAA, investigation, methodology, analysis, editing and final review of the manuscript; F de SF, analysis, editing and final review of the manuscript; PGM, methodology, analysis, editing and final review of the manuscript; LFM, senior author, conceptualization, and design, conducting the analysis and critical interpretation of the literature, writing and final revision.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they do not have any conflict of interest.
Ethical statement
This study did not involve any human or animal testing. This research did not require submission to analysis by the Ethics Committee because there were no interventions performed with humans nor any data collected from them. This research was conducted in accordance to the World Medical Association Declaration of Helsinki.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vergara, J., Teixeira, H.S., de Souza, C.M. et al. Flow test by the International Dysphagia Diet Standardization Initiative reveals distinct viscosity parameters of three thickening agents. J Food Sci Technol 59, 3627–3633 (2022). https://doi.org/10.1007/s13197-022-05369-5
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13197-022-05369-5