
Abstract
Powdered thickeners are used to modify drink consistency in the clinical management of dysphagia. These thickeners are composed of primarily modified maize starch; some varieties also incorporate powdered gums. Amylase is a digestive enzyme found in saliva that initiates the breakdown of starch. To determine the significance of this process in dysphagia management, we measured the effects of human saliva on the viscosity of thickened drinks. Two thickeners were studied: one comprising modified maize starch alone and one that included additional gums. These were added to drinks with neutral and acidic pH: water and orange juice. Two clinical scenarios were simulated: (1) the effect of saliva on fluid as it is swallowed and (2) the effect when saliva enters a cup and contaminates a drink. Saliva was found to reduce the viscosity of water thickened with maize starch in both scenarios: (1) 90% reduction after 10 s and (2) almost 100% reduction in viscosity after 20 min. The thickener composed of gums and maize starch showed a significant reduction but retained a level of thickening. In contrast, thickened orange juice (pH 3.8) was not observed to undergo any measurable reduction in viscosity under the action of saliva.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dysphagia has been defined as a mechanical disorder that affects the safety, efficiency, or quality of eating and drinking [1]. Individuals with inadequately managed dysphagia can be at risk of bolus aspiration, potentially leading to aspiration pneumonia and other respiratory problems [2]. Dehydration and malnutrition may also be observed which results in susceptibility to serious health problems [1, 3–5]. Dysphagia can have a profound impact on quality of life. The transport of a food or liquid bolus through swallowing has been shown to be significantly affected by the bolus’s flow properties such as viscosity [6–8] (which may be referred to informally as “thickness”). Knowledge of bolus flow properties is vital to the treatment of dysphagia and, as such, texture modification of foods and drinks forms a significant part of the clinician’s treatment toolkit [9].
Studies of bolus movement have shown that increased viscosity results in slower oropharyngeal transit times [6], giving the patient more time to prepare for the onset of pharyngeal swallow and engage airway protective mechanisms. This is widely thought to provide a desirable increase in swallow safety and many clinicians will therefore recommend the use of a thickener at strategic times in the rehabilitation of individuals with dysphagia. Obtaining the correct level of viscosity is very important clinically. If a bolus is too thick, then excessively long transit times can result, and for those individuals with weak swallowing musculature there may be insufficient clearance of the bolus resulting in residue within the oropharynx [10, 11]. Residue in the oropharynx is often aspirated when the airway reopens and breathing commences. In addition to these physiologic effects caused by a fluid that is too thick, very thick drinks are less palatable to many people and this can lead to a risk of their fluid intake falling below desirable levels [12]. Bolus viscosity should therefore be controlled to within a specific clinically determined range. The acceptable range depends on the physiologic nature of the dysphagia as assessed by a dysphagia specialist who examines an individual to determine the most appropriate management approach [9].
Several brands of powdered thickener are commercially available; they are used in practice in the clinical setting as well as in private homes and public eating and drinking establishments. Thickeners are very widely used to thicken drinks for individuals with dysphagia, even if only for a short period of time.
When a person eats and drinks, saliva is mixed into the bolus in the mouth. Saliva is secreted by the parotid, sublingual, and submandibular glands. Saliva secretion is stimulated by, among other things, the smell, taste, and anticipation of food or drink. Research reports that approximately 1000-1500 ml of saliva is produced daily by a healthy individual [13], though this quantity varies with many factors, including age and health. Saliva mixes with food and drink for the purpose of moistening the bolus and starting the digestive process. Saliva contains the digestive enzyme amylase which initiates the breakdown of the chemical and mechanical structure of foods and drinks, enabling the body to extract hydration and nutrients.
Thickeners available for the management of dysphagia use starch as the main active ingredient, generally in the form of granulated modified maize starch (E1442). When added to water, these granules swell and partly dissolve, resulting in a liquid with some weak interlinking bonds between the granules; it is this structure that is responsible for the thickening effect.
Salivary amylase is known to catalyse the hydrolysis of starch, breaking it down into simple carbohydrates and water as a part of the healthy digestion of foods [13]. However, this process would also be expected to break down the mechanical structure achieved by starch granules, thereby potentially reducing the viscosity of drinks thickened with starch-based thickeners. We hypothesised that this hitherto unquantified effect could be highly relevant to the clinical practice of dysphagia management, which is strongly dependent on texture modification. Two clinical scenarios were identified for investigation:
-
1.
When a drink is presented to the mouth there follows a period—the oral preparatory stage—in which a bolus of thickened fluid is formed in the oral cavity. The bolus will mix with saliva during its formation, and thus hydrolysis of starch will begin from this moment. If the viscosity of a thickened bolus changes significantly during swallowing, it could have serious implications for dysphagia therapy and therefore needs to be quantified.
-
2.
Following initial preparation, a thickened drink may be consumed gradually over a period of minutes to hours so there is a possibility of saliva entering the cup and “contaminating” the drink. This is more likely to occur with individuals who have difficulty swallowing their saliva and who may have excessive saliva collecting in the mouth. It is unknown whether a small volume of saliva would have an effect on a cup-sized volume of thickened drink, but there is some anecdotal evidence that this effect could result in a cup of fluid having a significantly reduced viscosity.
Different brands of thickener vary in composition: Many use maize starch alone, and others use starch along with one or more powdered gums. Gums are widely used in the food industry to increase the viscosity of fluids or to act as stabilisers; e.g., gums are found in many “milk shake”-style drinks for general consumption. Gums are used to add “bulk” with the aim of increasing satiety in low-fat or “diet” products, and some gums have a laxative effect, e.g., guar gum is a soluble fibre. Some currently available thickening powders designed for dysphagia therapy contain powdered gums that are not hydrolysed by amylase. Since these thickeners achieve an increased viscosity through the action of both maize starch and gums, it is not clear how the action of amylase would affect the mechanical structure and bulk viscosity of the thickened drink. We have included thickeners representing both types in our experiments.
As with most enzymes, the action of amylase to catalyse the hydrolysis of starch is dependent on pH. In practice, thickener powders may be added to a range of different drinks having a wide range of pH; in particular, several common drinks (fruit juices, cordials, sodas, and coffee) are acidic. Therefore, if amylase does act to break down starch thickeners in clinical situations, the reaction may be unpredictable depending on the drink that has been thickened. We have included investigation of a representative orange juice as well as water in experiments.
Materials and Methods
Two experiments were devised to examine the research questions outlined above, to quantify the effects of saliva on thickened drinks used in dysphagia management. Experiment 1 simulated the effect of saliva on a bolus of thickened liquid in the mouth prior to a swallow. Experiment 2 simulated the effect of saliva contamination of a glass of thickened liquid. Both protocols investigated the effects of an acidic beverage (orange juice) and the effect of additional gums in thickening powder.
Thickeners
Two commercially available thickening powders were investigated (see the Appendix for manufacturers’ details): type A was representative of thickeners comprised solely of maize starch, and type B was composed of maize starch with the addition of gums. Characteristics of the thickeners are given in Table 1.
Bulk Fluid Preparation
Two drinks were used (see the Appendix for details) to investigate the effects of saliva under neutral versus acidic conditions that may be encountered in practice: filtered tap water (neutral pH) and a widely available brand of orange juice with pH 3.8 (determined using Hanna Instruments 98127 pH meter, Leighton Buzzard, UK). The drinks were left standing for 1 h to equilibrate with room temperature, avoiding any significant temperature change after mixing. The drinks were dispensed into 200-ml measures in volumetric flasks, then each of the two thickeners was used to prepare each of the two fluids to stage 2 (custard) consistency [15] according to the manufacturers’ instructions. This resulted in four different preparations, with a significant difference between thickened and nonthickened drinks. Each mixture was stirred with a spoon for 30 s to achieve a smooth consistency, then left to stand for 30 min to minimise variation in consistency over time during the experiments [16].
Saliva Collection
Saliva was collected from two healthy males (aged 34 and 36 years) each day prior to experimentation. A strict protocol was followed to control for diet, time of day, and method of collection [17]. Ten millilitres of saliva was collected from each donor on each occasion over a period of 20-30 min. The saliva was stored in an airtight container and refrigerated until use. The saliva collected was composite, that is, from all the salivary glands. The composition of the saliva would be representative of most healthy individuals.
Amylase Inhibitor
To obtain viscosity data at specific time points, a small volume of acidic solution was added to prevent further saliva action occurring during the 2-min duration of viscosity measurement [18]. This inhibitor was a 10% w/v solution of citric acid powder in water, resulting in a pH of 1.6.
Viscosity Measurement
The viscosity of a fluid can be quantified by measuring its resistance to flow. This can be achieved in practice by inserting a sample of fluid in a small gap between two flat plates, holding one plate stationary and moving the other at a known speed. The fluid between the plates is thus subjected to a shear deformation, which represents flow (as opposed to other types of deformation, e.g., compression, extension, torsion). The force required to move the plate against the resistance of the fluid is directly proportional to the fluid’s viscosity [19]. Similarly, if a constant force was applied to the movable plate, then the resulting speed of motion would be inversely proportional to the fluid’s viscosity.
A Bohlin CVO rotational rheometer system (Malvern Instruments Ltd, Worchester, UK) was used to investigate the flow properties of the thickened fluids. To ensure uniform shear conditions across the radius of the circular sample, a cone-and-plate geometry was chosen (40-mm diameter, 4° angle). Throughout testing, the temperature of the samples during rheometry was maintained at 25 ± 0.1°C by the “Peltier Plate” control unit.
Experiment 1: Simulation of Saliva-Beverage Mix during Oral Preparatory Phase
Experimental protocol 1 was designed to assess the effect of amylase on the viscosity of the swallow bolus after an oral preparatory phase. For an individual with no oral difficulties, the fluid bolus, once formed, will move through the oral preparatory and oral phases in less than 1 s [14]. However, in an individual with oral preparatory or oral phase difficulties, this time frame can be much longer. In unpublished clinical observations, some individuals with severe oral and oral preparatory difficulties may retain the bolus in the oral cavity for up to 60 s. We have investigated dwell times from 10 to 60 s.
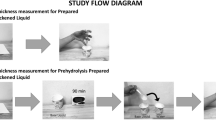
Figure 1 shows the testing protocol used. A batch of thickened fluid was produced according to the methods described above. A 10-ml sample was taken as the main batch for each measurement to represent a typical bolus of thickened fluid. One millilitre of human saliva was added to this bolus and stirred slowly and continuously. After 10 s, 1 ml of liquid amylase inhibitor was added to the bolus and stirred rapidly to ensure even distribution. This inhibitor is required to halt the action of amylase during the subsequent viscosity measurement process, which takes 2 min. Viscosity measurement on our Bohlin CVO rheometer required a sample size of 1.4 ml. This was obtained from the bolus fluid; the remaining bolus fluid was discarded and a fresh 10-ml sample was prepared for each viscosity measurement. This protocol was repeated five times for each of four thickened fluids: water and orange juice thickened with type A and B thickener.

Measurement protocol for Experiment 1: Simulation of saliva-beverage mix during oral preparatory phase. Protocol repeated five times, then stir time extended up to 60 s
The addition of 2 ml of total nonthickened fluid to a 10-ml thickened bolus would be expected to affect the overall viscosity, irrespective of amylase action. Therefore, for each batch of thickened fluid, a control bolus was also developed using a 1-ml water placebo in place of the saliva, plus 1 ml of citric acid in an otherwise identical protocol.
The viscosity measures were normalised against the viscosity of the control fluid (described in Analysis of Data section) and the results are presented in Table 2 as mean and standard deviation of the five repeated measures.
To evaluate any change in viscosity resulting from extended-duration oral preparatory phases, the protocol above was adapted by increasing the mixing time for saliva and bolus in 10-s intervals up to 60 s. This was repeated for the four test liquids. The results were normalised against the control measure and the results are displayed in Figs. 3 and 4.
Experiment 2: Simulation of Thickened Beverage Contaminated by Saliva
Experimental protocol 2 was designed to assess the effect of amylase on the viscosity of a thickened drink after contamination by a small volume of saliva. This was evaluated 10 min after contamination and at 10-min intervals up to 60 min; this was chosen to represent a reasonable time-frame for consumption.
Figure 2 shows the experimental protocol. A batch of thickened fluid was produced according to the methods described above, then the viscosity was measured to quantify any batch variation. One millilitre of human saliva was added to the bulk fluid (200 ml) and stirred for 30 s to obtain an even distribution of the saliva. After a wait period of 10 min, the fluid was again stirred to homogenise it and a sample was taken for viscosity measurement. This protocol was repeated five times for each of the four test fluids. The viscosity values were normalised against the initial batch viscosity measure and the results are given in Table 2.

Measurement protocol for Experiment 2: Simulation of thickened beverage contaminated by saliva. Protocol repeated five times, then wait time extended up to 60 min
The fluids were studied at consecutive 10-min intervals up to a 60-min maximum to provide a more complete quantification of the change in viscosity as a function of time. The bulk fluid was stirred for 30 s prior to each measurement to ensure a homogeneous fluid for appropriate sampling; this protocol mimics the repeated stirring of a thickened drink prior to drinking. This included an initial measurement immediately following the addition of saliva and 30 s of stirring. The measurement protocol was repeated using a 1-ml water placebo instead of the saliva, resulting in a second measurement series that served to control for any variation in the viscosity over time independent of the action of amylase. These measurements were normalised and are presented in Figs. 5 and 6.
Subjective Evaluation
Since viscosity measurement is not routinely performed in clinical practice, we sought to identify any visually perceptible effects of amylase. To this end we performed subjective assessment of the bulk fluids in beakers by visual inspection and through interaction by tilting and stirring.
Analysis of Data
Studies have shown that the viscosity achieved using thickeners is dependent on the properties of the medium in which the thickener was dissolved (pH, temperature, fat content, density) and the thickener itself. Water and orange juice have different viscosities, and the two thickener types will also result in different initial viscosities [20–22]. To normalise for these variations between the test fluids, and therefore isolate the effect of amylase, the viscosity measurement results have been normalised and scaled from 0 to 100%, where for each drink 0% represents the viscosity of the drink without the addition of thickener and 100% represents the viscosity of the thickened drink as produced, prior to the addition of saliva or placebo.
Results
Experiment 1: Simulation of Saliva-Beverage Mix during Oral Preparatory Phase
Table 2 shows that when 1 ml of saliva was added to a 10-ml thickened water bolus, a very large reduction in viscosity occurred within 10 s. For thickener A (starch only), the viscosity was reduced by 90%, and for thickener B (starch + gums), the viscosity was reduced by 69%. Figure 3 shows how the viscosity of these thickened fluids continued to decrease after longer mixing periods. After 20 s of mixing with saliva, water thickened with type A had lost 97% of its initial viscosity and decreased thereafter to end up very close to the viscosity of water at 60 s, with a 99% reduction in viscosity. For type B thickener, the reduction in viscosity appeared to decrease toward a stable level after 60 s, at which point its viscosity had been reduced by 89%.

The effect on viscosity of adding 1 ml of saliva to a 10-ml bolus of thickened water. Normalized: 100% = viscosity prior to addition of saliva; 0% = viscosity of water. a Type A thickener (maize starch only). b Type B thickener (starch plus gums)
When orange juice was used as the base drink to be thickened, Table 2 and Fig. 4 show that the addition of saliva produced no significant change in viscosity of the orange juice across the 60-s test period for either of the thickeners.

The effect on viscosity of adding 1 ml of saliva to a 10-ml bolus of thickened orange juice. Normalized: 100% = viscosity prior to addition of saliva; 0% = viscosity of orange juice. a Type A thickener (maize starch only). b Type B thickener (starch plus gums)
Experiment 2: Simulation of Thickened Beverage Contaminated by Saliva
Table 2 shows that when 1 ml of saliva was added to a beaker of 200 ml of thickened water, very large reductions in viscosity were observed. This effect occurred at a slower rate than in experiment 1; however, the final reductions in viscosity were just as large and occurred for both thickener types. Ten minutes after saliva was added and mixed, the viscosity of water thickened with type A was reduced by 99.5%. Figure 5 shows that this low viscosity level was sustained over a 60-min period. For thickener B, the reduction in viscosity was 91% after 10 min, and Fig. 5 shows that there was a slight increase in viscosity after this initial drop, with the liquid seeming to stabilise at a viscosity 90% less than its initial value.

The effect on viscosity of adding 1 ml of saliva to a 200-ml beaker of thickened water. Normalized: 100% = viscosity prior to addition of saliva; 0% = viscosity of water. a Type A thickener (maize starch only). b Type B thickener (starch plus gums)
When orange juice was investigated, the addition of saliva appeared to produce a small decrease in viscosity. Table 2 shows a 12% initial reduction in viscosity for both thickener types after 10 min. Figure 6 shows that after this initial fall, the viscosity of the fluids (both A and B) tended to rise slowly. The control liquids (no saliva added) also experienced a slight and steady increase in viscosity over the 60-min test period.

The effect on viscosity of adding 1 ml of saliva to a 200-ml beaker of thickened orange juice. Normalized: 100% = viscosity prior to addition of saliva; 0% = viscosity of orange juice. a Type A thickener (maize starch only). b Type B thickener (starch plus gums)
Subjective Assessment
Water Plus Thickener A
Following the addition of saliva, the thickened fluid began to break down after 10 min and the drink appeared, subjectively, to return to its prethickened state as a clear liquid with a thin, watery consistency.
Water Plus Thickener B
Following the addition of saliva, after 10 min the thickened fluid appeared reduced in viscosity when swilled in a beaker or stirred with a spoon, but it retained the opaque appearance of a thickened fluid and appeared significantly thicker than its prethickened state. This appearance is in contrast to the quantitative measures that showed considerable reduction in viscosity in Figs. 5 and 6.
Orange Juice
Over a period of 60 min, the addition of saliva had no visually apparent effect on orange juice thickened with either thickening powder.
Each of these subjective evaluations were clearly identified by the three investigators. However, this was not a controlled study and the results must be considered anecdotal.
Discussion
Methodological Considerations
Repeatability
We took efforts to minimise variation [17] in the properties of the harvested human saliva throughout these experiments (which occurred over several weeks) and found that the batch-to-batch variation was small in comparison to the magnitude of the viscosity changes. In practice, the properties of human saliva are known to vary significantly with age, health, medication, time of day, diet, and hydration level [13]. This variation is most likely to be greater for individuals with dysphagia.
The volumetric quantities of saliva and thickened drink were controlled in these experiments. The volumetric quantities used here (1 ml of saliva to 10 ml of bolus) were chosen to be representative of a swallow. However, in practice the ratio will vary widely as the quantity of saliva in the oral cavity for an individual will be affected by, for example, the medical condition, medications or treatments received, general health, and the ability of the person to deal with his/her own secretions. Often, individuals with cerebral palsy, motor neurone disease, and Parkinson’s disease have excessive saliva collecting in their mouth, while people who have received radiotherapy to the oropharyngeal area are known to experience severe xerostomia [12], which may necessitate the use of artificial saliva. Also, saliva is known to be stimulated by taste and smell and anticipatory knowledge of the foods and drinks to be received. This effect will vary with the food presented, previous experiences with food, eating environment, and so forth.
Stirring
When measuring the action of amylase in a beaker of thickened drink over 60 min, our protocol required repeated stirring every 10 min. This stirring may or may not be performed in clinical practice, either institutionally or in a home-care situation.
Temperature
The action of amylase on starch is a temperature-dependent reaction; this variable was not included in this study. However, pilot experimentation indicated the following: when using chilled water (5°C), the action of amylase appeared to slow to approximately half the rate at room temperature. When using hot water (65°C), the action of salivary amylase was accelerated, occurring slightly faster than at room temperature.
Experiment 1: Simulation of Saliva-Beverage Mix during Oral Preparatory Phase
We used a control measure whereby a 2-ml water placebo was added to a 10-ml thickened bolus to account for the viscosity reduction due to simple dilution of the thickened bolus irrespective of amylase action. This issue has relevance clinically because the addition of a volume of saliva will affect the viscosity of the fluid being drunk. That is, even when amylase has zero effect on viscosity, the bolus viscosity during a swallow is not equal to the viscosity of the drink in the cup.
When water was thickened, Fig. 3 shows that saliva significantly reduced the viscosity for both thickener types A and B, and that this effect could occur within the time frame of a swallow. We extended the time frame for the swallow to 60 s, intending to cover the range of time for an oropharyngeal swallow for an individual with dysphagia to clear a bolus from the oropharynx, including repeat swallows for residue. Most of the change in viscosity occurred within the first 10–20 s, which is within the range of time it takes for oropharyngeal swallowing for many individuals with dysphagia. This result has important implications for the management of dysphagia as it is clear that the longer a thickened liquid is held in the mouth, the more the viscosity may be reduced. A person with slow oropharyngeal swallowing will be particularly vulnerable in this situation, as will an individual who may swallow fast but retains fluid in the oropharynx (including the valleculae or pyriform sinuses) and will then be swallowing a much thinner fluid on repeat swallows. This may lead to an increased possibility for aspiration on repeat swallows.
Table 2 and Fig. 4 show that when orange juice was thickened, saliva had no significant effect on viscosity. These results indicate that if all other factors are equal, a swallow bolus of thickened orange juice would have a higher viscosity than thickened water, despite them initially having equal viscosity in the cup. This may explain, in part, some of the variability often seen in swallow function for any individual. Variability may be accounted for by physiologic reasons such as fatigue, medications, and so forth, or by bolus variables such as temperature or size. We now have an additional variable to consider: the pH of the fluid will modify the effect of saliva on the viscosity of the bolus swallowed.
We conclude that in practice it is not possible to predict the quantitative change in viscosity that would occur between the cup and the swallowed bolus for the general case, nor do we foresee this being possible due to the large number of variables encountered. However, it is important to consider this in the management of individuals with dysphagia, especially those who have oral difficulties that result in prolonged oropharyngeal swallows or who have residue resulting in repeat swallows, where the bolus of thickened drink could exhibit greater reduction in viscosity.
Experiment 2: Simulation of Thickened Beverage Contaminated by Saliva
Figure 5 shows that when water was thickened, saliva contamination significantly reduced the viscosity for both thickener types A and B. For thickener A the viscosity was reduced from “custard-thick” (stage 2) to almost the viscosity of water; thus, the thickening effect had been practically reversed. For thickener B the viscosity was also reduced by 90%, but the resulting mixture still had a higher viscosity than water.
Figure 6 shows that when orange juice was thickened, saliva had no significant effect on the viscosity. This result could be relevant in practice in situations where an individual’s saliva control is known to be poor and saliva is likely to mix with the thickened drink in the cup. Thus, it would seem that thickened orange juice would be unaffected by contamination from saliva. We suggest that this is something that clinicians may want to consider in their management of such an individual. We attribute the majority of the difference between orange juice and water to their differ pH values, but it is possible that other differences between the drinks also had a measurable effect. In practice, thickening powders are added to drinks having a wide variety of pH values and the action of salivary amylase will have a variable effect, strongly dependent on beverage pH. The pH of the orange juice used was 3.8, which is acidic although much weaker than the citric acid amylase inhibitor at pH 1.6. The specific effect of pH in this context may be a subject for future research. The addition of dilute citric acid to thickened drinks may be sufficient to prevent the action of amylase on starch; however, it has a very noticeable taste (similar to lemon juice) and therefore would not be widely applicable. Nevertheless, it is possible that the effects of saliva may be controlled to some extent by pH control.
The viscosity of the thickened drinks was observed to increase over the 60-min duration of study, for both control and orange juice products. This continual thickening has been documented as an inherent property of thickeners [16], and we hypothesise that the thickening was exaggerated slightly as a result of the repeated stirring [24].
In practice, if saliva has gotten into a cup of thickened drink fluid, the action that would then occur is unpredictable. It was observed that if the drink was thickened to at least stage 2 and no stirring was performed, then the saliva could be localised to only part of the cup, resulting in a pool of low-viscosity liquid within the higher-viscosity bulk. If separation of a low-viscosity pool was observed, the drink may be stirred. This would immediately reduce the average viscosity and lead to continued reduction in viscosity of the whole drink. Alternatively, more thickener might be added and stirred in. We simulated this situation and found that the drink would thicken temporarily and then break down again. This phenomenon of a low-viscosity pool within a higher-viscosity drink may relate to the observation that healthcare workers sometimes report anecdotally of thickened drinks “separating”; it is not the thickening powder separating out from the drink, but rather the thickened drink breaking down.
Subjective Perception
Viscosity measurements indicated a 90% reduction in thickening when amylase acted on water plus thickener B, which contained maize starch plus gums. However, this reduction in viscosity was not readily detected in the subjective assessment of the fluid [23]. This may be attributable to the non-Newtonian flow behaviour of thickened drinks [24] whereby the apparent viscosity at low flow rates (such as tipping in a cup) is different to the viscosity at higher flow rates (we tested at 40 s−1, which is thought to be representative of the higher flow rates experienced during a swallow [24]). We hypothesise that amylase acted to break down the mechanical structure of the maize starch component of the mixture, resulting in water thickened by the gum components alone. This resulting mixture could have different flow behaviour characteristics, where the reduction in viscosity is less apparent at low flow rates. This would be consistent with a weak gel-like material.
The clinical effects of swallowing a mixture as described above would be very hard to predict since there is a paucity of data of the effect of any thickened drinks during a human swallow. However, we can conclude that (1) the physical properties of thickened water are significantly affected by the action of amylase, even when the thickener contains additional gums; (2) subjective assessment is an unreliable predictor of viscosity compared with measurements at shear motion rates that may be physiologically representative of rates during swallowing; and (3) further work is required to quantify the effect of fluid properties (e.g., viscosity) on all aspects of swallowing and dysphagia.
Conclusions
We have shown that salivary amylase can significantly reduce the viscosity of drinks thickened with starch-based thickeners. This effect occurred within 10 s in our experimental protocol to simulate oropharyngeal swallowing. The effect was also apparent within 10 min in our protocol designed to simulate the contamination of a cup by saliva. The reduction in viscosity continued over time to result in a viscosity indistinguishable from that of water after 20-30 min.
A reduction in viscosity was also observed when the thickener powder contained gums in addition to starch, eventually reaching a viscosity level that had been reduced by 90%, although still higher viscosity than water.
The effect of saliva on viscosity was entirely negated when orange juice (having an acidic pH of 3.8) was used as the base drink to be thickened. We conclude that in clinical practice the effect of amylase will depend very strongly on the properties, particularly pH, of the drink that has been thickened. So while some low-pH drinks (such as orange juice, lemonade, or cola) will unlikely show any effect from the amylase, other neural-pH drinks (such as water, milk, and some types of tea) may be profoundly affected.
We conclude that in clinical practice it is likely that the viscosity of swallowed boluses is not equal to the viscosity of the drink in the cup because of saliva. However, without an evidential relationship between viscosity and flow in dysphagia, it is not possible to draw general conclusions for physiologic consequences at this stage. We have further shown that contamination of just 1 ml of saliva to 200 ml of thickened water can counteract the thickening effect, decreasing its viscosity almost back that of plain water. We would therefore recommend that the utmost care be taken to avoid contamination by saliva and that any contaminated drink be discarded. Attempts to rethicken by the addition of more thickener will be ineffective.
It is worth remembering that starch-based thickeners have been used successfully and effectively for more than a decade; therefore, the clinical implications of these experimental results must be considered in that context. There are important advantages to thickeners being broken down easily by the action of digestive enzymes: (1) to aid in clearing the throat if residues of drinks or soft foods remain after incomplete swallowing, and (2) to release the water to hydrate the patient. Though modified maize starch is affected by saliva, it is unlikely that gums would be an appropriate like-for-like replacement due to the potential problems with digestion. In particular, a laxative effect may be counterproductive to the aim of hydrating and nourishing the dysphagic individual.
Food technology is a sophisticated area of scientific investigation and has made important contributions to dysphagia management. Further work could provide a more complete picture of the effects of salivary amylase by investigating a wide range of drinks and thickeners, including prethickened drinks, and by considering the various qualities of saliva. We would recommend investigation into the feasibility of creating thickening agents that do not break down rapidly when in contact with salivary amylase but also do not have adverse consequences for hydration and nutrition.
Food thickeners have become a valuable tool in the management of individuals with dysphagia when they are used judiciously. Careful thought in their application is required, and information regarding the issues we have raised here should be conveyed to those who are preparing the drinks.
Appendix: Materials
Thickener Details
- Brand A:
-
“Thick & Easy,” Fresenius Kabi Ltd, Cestrian Court, Eastgate Way, Manor Park, Runcorn, Chesire, UK. Other examples of brands whose sole ingredient is modified maize starch include “Resource ThickenUp” (Nestle Nutrition, St Georges House, Croydon, UK.) and “Vitaquick” (Vitaflo International, 11-16 Century Building, Brunswick Business Park, Liverpool, UK)
- Brand B:
-
“Nutilis,” Nutricia Ltd, Newmarket House, Newmarket Avenue, White Horse Business Park, Trowbridge, Wiltshire, UK
Beverage Details
- Water:
-
tap water filtered to laboratory ISO 3696 Grade III standard
- Orange juice:
-
“Tropicana, smooth”, Tropicana UK Ltd., PO Box 6642, Leicester, LE4 8WZ, UK
References
Whelan K. Inadequate fluid intakes in dysphagic acute stroke. Clin Nutr. 2001;20(5):423–8.
Layne KA, Losinski DS, Zenner PM, Ament JA. Using the Fleming index of dysphagia to establish prevalence. Dysphagia. 1989;4(1):39–42.
Goulding R, Bakheit AM. Evaluation of the benefits of monitoring fluid thickness in the dietary management of dysphagic stroke patients. Clin Rehabil. 2000;14:119–24.
Finestone HM, Foley NC, Woodbury MG, Greene-Finestone L. Quantifying fluid intake in dysphagic stroke patients: a preliminary comparison of oral and nonoral strategies. Arch Phys Med Rehabil. 2001;82:1744–6.
Kayser-Jones J, Schell ES, Porter C, Barbaccia JC, Shaw H. Factors contributing to dehydration in nursing homes: inadequate staffing and lack of professional supervision. J Am Geriatr Soc. 1999;47(10):1187–94.
Dantas RO, Kern MK, Massey BT, Dodds WJ, Kahrilas PJ, Brasseur JG, Cook IJ, Lang IM. Effect of swallowed bolus variables on oral and pharyngeal phases of swallowing. Am J Physiol. 1990;258:G675–81.
Cichero JA, Jackson O, Halley PJ, Murdoch BE. Which one of these is not like the others? An inter-hospital study of the viscosity of thickened fluids. J Speech Lang Hear Res. 2000;43:537–47.
Miller JL, Watkin KL. The influence of bolus volume and viscosity on anterior lingual force during the oral stage of swallowing. Dysphagia. 1996;11:117–24.
Leonard R, Kendall K. Dysphagia assessment and treatment planning. San Diego: Singular Publishing Group A Team Approach; 1997.
Hamlet S, Choi J, Zormeier M, Shamsa F, Stachler R, Muz J, Jones L. Normal adult swallowing of liquid and viscous material: scintigraphic data on bolus transit and oropharyngeal residues. Dysphagia. 1996;11:41–7.
Dantas RO, Dodds WJ. Effect of bolus volume and consistency on swallow-induced submental and infrahyoid electromyographic activity. Braz J Med Biol Res. 1990;23:37–44.
Cichero JA, Murdoch BE. Dysphagia: foundation, theory and practice. Chichester: Wiley & Sons; 2006.
Hall JE. Guyton and hall textbook of medical physiology. 12th ed. Philadelphia: Saunders; 2010.
Logemann JA. Evaluation and treatment of swallowing disorders. 2nd ed. Austin: Pro-ed; 1998.
British Dietetic Association. National descriptors for texture modification in adults. http://www.bda.uk.com/publications/statements/NationalDescriptorsTextureModificationAdults.pdf (2009). Accessed 19 June 2009.
O’Leary M, Hanson B, Smith CH. Variation of the apparent viscosity of thickened drinks. Int J Lang Commun Disord. 2011;46(1):17–29.
Salimetrics LLC. Saliva collection and handling advice. http://www.salimetrics.com/spit-tips/publications/saliva-collection-handbook.php. Accessed 21 Feb 2011.
Fried M, Abramson S, Meyer JH. Passage of salivary amylase through the stomach in humans. Dig Dis Sci. 1987;32:1097–103.
Malkin AY. Rheology Fundamentals. ChemTec Publishing, Toronto. 1994.
Sopade PA, Halley PJ, Cichero JA, Ward LC. Rheological characterization of food thickeners marketed in Australia in various media for the management of dysphagia. I: water and cordial. J Food Eng. 2007;79:69–82.
Sopade PA, Halley PJ, Cichero JA, Ward LC, Liu J, Teo KH. Rheological characterization of food thickeners marketed in Australia in various media for the management of dysphagia. II. Milk as a dispersing medium. J Food Eng. 2008;84(4):553–62.
Sopade PA, Halley PJ, Cichero JA, Ward LC, Liu J, Varliveli S. Rheological characterization of food thickeners marketed in Australia in various media for the management of dysphagia. III. Fruit juice as a dispersing medium. J Food Eng. 2008;86(4):604–15.
Smith CH, Logemann JA, Burghardt WR, Zecker SG, Rademaker AW. Oral and oropharyngeal perception of viscosity across the age span. Dysphagia. 2007;21:209–17.
O’Leary M, Hanson B, Smith CH. Viscosity and non-Newtonian features of thickened fluids used for dysphagia therapy. J Food Sci. 2010;75:E330–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hanson, B., O’Leary, M.T. & Smith, C.H. The Effect of Saliva on the Viscosity of Thickened Drinks. Dysphagia 27, 10–19 (2012). https://doi.org/10.1007/s00455-011-9330-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-011-9330-8