
Abstract
In recent era, cancer is a major global health hazard and is mostly treated with either radio or chemotherapy. The above treatment procedure induces a secondary concern named as oral mucositis (OM). The disorder OM is specifically associated with oral mucosa and leads to bleeding, pain, difficulty in swallowing of solids, as well as fluids and speech difficulty. Curcumin is explored for prevention as well as treatment of OM. The article was organized via collection of enormous literatures by using the keywords like oral mucositis, chemotherapy, anti-inflammatory, curcumin, and clinical trials from search engines of different domains like Scopus, PubMed/MEDLINE, Science Direct, and Google Scholar with an increasing order of their year of publications. A numerous antineoplastic therapies resulted OM, as a devastating side effect. Moreover, the expanded pathogenesis of the disease permits a sound predictability over the patient’s risk, thereby directing its adaptability and management protocols towards the achievement of novel therapeutics. An augmented interest towards curcumin as a potential therapeutic emerged because of its easy accessibility, antioxidant, anti-inflammatory, antiulcer, antimicrobial, and wound-healing abilities along with reduced side effects. Curcumin can potentially alter OM and OM-induced weight loss but showed a great heterogeneity.
Graphical Abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Currently, cancer is a prevailing health issue throughout the world. Around 19.3 million new cancer cases were detected globally in 2020 [113], and on an average 70% of the case prevailed in low and middle-income countries. The oral cancer scenario in India is accomplished with one third of the global incidence/mortality rate and considered to be predominant in men at their younger age group compared to the western world. Despite of the significant modernization in theranostics of oral cancers, the up growing treatment cost created a financial strain over patients as well as healthcare providers [3, 85]. The treatment protocols comprising of radiation therapy (RT), cytotoxic chemotherapy (CT), or both is considered to be more effective including their long- and short-term adverse effects together with mucositis [28, 111]. The secondary reactions can be associated with any region of the mucosal layer associated with gut, with a special emphasis to oral cavity. The mechanisms associated with the cytotoxicity include inhibitory impact over the repair and replication of DNA, cell death followed by DNA damage, and restriction over cell-cycle [77]. Nevertheless, the complexity of molecular pathways associated with damage of oral epithelia is yet a known phenomenon [104, 110]
Oral mucositis (OM) is critically manifested via ulceration, edema, and erythema of oral mucosa resulting an intrusive life quality through the tenure of treatment. The development of OM predominantly allied with several factors such as gender, poor oral hygiene, tobacco use, age, dosage and types of drugs used in chemotherapy, frequency of radiotherapy, and alcohol consumption [108, 109]. OM induced via chemotherapy is manifested with a reduced keratinocyte growth factor (KGF), early release of inflammatory cytokines, as well as reactive oxygen species (ROS) leads to an increased mucosal apoptosis and instigation of transcription factors like NF-Kβ [27]. Moreover, the OM prorogued via radiotherapy is exhibited with the release of ROS and inflammatory cytokines, aggravating several reaction oriented cellular apoptosis followed by mucosal inflammation and injuries of salivary glands and arterioles [18, 84]. OM is usually prevalent with patients subjected for conventional CT (20 to 40%), high-dose CT (80%), recipients (patients) of hematopoietic cell transplants (75 to 100%), and with almost each victim associated with head and neck squamous carcinoma (HNSC) and experiencing RT [32, 88, 106].
The OM aggravated via chemotherapy seems to be milder and recovered faster compared with its onset via radiotherapy of head and neck carcinoma [10, 19]. Conversely, as per as the studies are concerned, the treatment of OM is found to be controversial and provides supportive treatment modalities which was disapproved for preventive and therapeutic measures [26, 56, 65, 66]. Because of the inevitable situations provoked via OM, there may be a need for parenteral or enteral nutrition [48, 57], followed by administration of systemic analgesics like opoids [15, 40, 58], hospitalizations [34, 42], use of costly resources [42, 93], and risk of sepsis [6, 64,65,66, 101, 117].
OM could be resulted via injuries governed by bruxism, sharpened teeth, microorganisms, and food [1, 98]. Furthermore, the xerostomia, taste alteration, and dysphagia, developed by OM, could be manifested with some systemic syndromes like psychological changes, anorexia, and lethargy. Consequently, the prolonged and recurrent hospitalizations along with the nutritional, analgesic, and supportive care aggravated by OM condition might increase the need of major economy and potential resources as the severity of the disease is concerned. Three tools like Oral Mucositis Grading Scale from World Health Organization (WHO-OMGS) (incorporating clinical criteria for evaluation of OM) [38], Common Terminology Criteria for Adverse Events in fifth revision (CTCAE v5.0) (for considering OM impact via capability of eating, necessity for intervention, and pain intensity), and finally the Radiation Therapy Oncology Group (RTOG) (for defining harshness of RT-prompted OM by means of a four-point scale) [38]. With the acclimatization of immense novel anticancer agents, a quenched therapeutic alternatives (with mere success rate) are available towards the prevention and/or treatment of OM [40, 110].
Despite of the devastating clinical consequences, the patients were being offered very less towards the effective treatment policy for prevention or mitigation of OM. Still, the OM continues to be a substantial challenge for patients experiencing cancer treatment. Few of the smart interventions with their strong supportive evidences are nevertheless applicable for OM. Meanwhile, the impacts of such therapies are quite unclear, which causes great variance in the treatment protocols in several medical centers [40, 125]. Regardless of an intense understanding of the in-depth complexities of pathogenesis and interventions for OM, there is an urge for adapting brilliant strategies which can reduce the disruptive treatment impacts over the healthy tissues [40, 125].
Thus, the mission for searching of challenging alternatives from the natural sources become a significant option for transforming the field of research. In contrast with the synthetic ones, natural compounds reveal easy accessibility with fewer side effects and offer beneficial properties (e.g., antioxidant, antimicrobial and anti-inflammatory properties), thus converting them to be considered promising therapeutics. The assessment of results of objective and subjective mucositis was described in Table 1 [12]. Apart from the fewer side effects, toxicity robustness (caused by antineoplastic drugs or radiation) by the natural products is found to be one of the finest protective measures in victims during their therapy [37, 38].
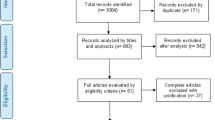
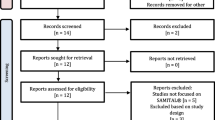
The article was a systematic review organized via collection of enormous literatures by using the keywords like oral mucositis, chemotherapy, anti-inflammatory, curcumin, and clinical trials from search engines of different domains like Scopus, PubMed/MEDLINE, Science Direct, and Google Scholar with an increasing order of their year of publications. Around 300 articles from several publishers were being analyzed; few of them were rejected based on non-suitability of the required information. It takes a long period between December 2022 and May 2024, for compiling the information for making such an excited and impactful article.
Curcuma longa (turmeric) is a popular, culinary/traditional medicine system in the regions like Southeast Asia and China. Among the contents, three curcuminoids, such as demethoxycurcumin, bisdemethoxycurcumin, and curcumin are the key components present in turmeric. Diferuloylmethane or curcumin (1,7-bis(4-hydroxy-3-methoxyphenyl) hepta-1,6-diene-3,5-dione) is usually obtained from the rhizomes of C. longa and other species of Curcuma [54, 68]. Curcumin showed a potential antioxidant as well as anti-inflammatory (via reduction of TNF-α and NF-Kβ) properties along with maintain cell growth and apoptosis [9, 17, 54, 79, 79]. The antioxidant effect of curcumin was governed by an elevated plasma levels of glutathione peroxidase (GSH) and superoxide dismutase (SOD), improved activity of catalase, and reduced level of lipid peroxidase in plasma. The above changes used to suppress the oxidative stress level thereby contributed for anti-inflammatory response [99]. Because of the bioavailability issue, curcumin (belongs to class IV under biopharmaceutical classification) via oral route of administration possesses a low systemic availability and chemical instability, rapid elimination, and low therapeutic response [7]. The in vivo study data revealed that the nano-curcumin at a dose of 20 mg/kg is equipotent with pure curcumin at a dose of 400 mg/kg [115]. Several techniques/approaches like administration with adjuvants e.g. bioconjugates [glycine, turmeric oil, epigallocatechin-3-gallate (EGCG) and alanine], piperine, and lipids (phospholipids), nanoparticulate approaches like micelles, liposomes, nanogels, niosomes, dendrimers, metal and solid lipid nanoparticles, nanomicelles, by using proteins (soy protein isolate and BSA) and several other methods like emulsification and hydrogel have been implemented for enhancing the bioavailability and metabolic resistance of curcumin [53, 90]. Figure 1(1) and 1(2) were showing the bioavailability issues, delivery strategies, and different forms of curcumin needed for its bioavailability enhancement [5, 116]. The effectiveness of curcumin (Sina Curcumin) against chemotherapy (CT) and radio-chemotherapy (RCT) induced OM was also found to be promising [24, 35, 39, 49, 63, 74, 86]. The current review is basically emphasizing on the effectiveness of curcumin on patients undergoing CT and RCT with or without head and neck radiotherapy but associated with OM development.

(1) Showing bioavailability issues, delivery strategies, and forms of curcumin to be administered for its bioavailability enhancement. (2) (A) Different strategies for curcumin nanoformulation preparation. (B) Schematic illustrations of the polymer-curcumin conjugate micelles. PLA linked with curcumin by tris along with hydrophilic PEG as corona generating the hydrophobic block of micelles; a controlled release system.
Cytotoxic Regimens Associated with Oral Mucositis
Epidemiology
Cancer in its devastating mode is expanding globally with an ultimate race. Several patients treated either by myeloablative chemotherapy or with radiation therapy (RT)/RCT (specifically in head & neck (H&N) cancer) will mostly develop OM as an adverse event of the treatment intervention [118]. Moreover, OM is considered to be the greatest severity that occurs with the patients during Hematopoietic cell transplantation (HCT) (42%) [29]. The onset rate for severe OM (SOM) in clinical trial patients (placebo-treated), with an exposure of total body irradiation, is around 98% [119, 121]. The severity of OM is highly prevalent in adults (24.4%) and children (25.6%) compared to the elderly (9.2%). The frequency of OM development among the patients enduring HCT regimens of reduced-intensity was of 73.2% versus the myeloablative of 86.5% and methotrexate, cyclosporine/methotrexate and prophylaxis via sirolimus/tacrolimus modulated graft-versus-host disease (GvHD) [25, 52]. H&N cancer patients (65%) treated with RT or RCT revealed SOM [8, 20]. The incidence rate of OM is greatly influenced via radiation field, tumor site, and use of concomitant and dose variable RT/RCT [114]. Similarly, the incidence rate of OM in numerous chemotherapy treated patients include the following: breast cancer (in 65% of patients (> 1400 patients) treated with doxorubicin, docetaxel, and cyclophosphamide with 5% SOM), lung cancer (in 15% of patients (> 1500 patients) treated with platinum/gemcitabine along with 1% SOM), colon cancer (in 14% of patients (898 patients) treated with 5-fluorouracil along with 1.7% SOM), non-Hodgkin lymphoma (in 6.6% of > 1400 treated patients), and 63.57% in pediatric cancer patients [30, 37].
Clinical Manifestations and Outcomes
The acute OM is manifested with pseudomembranous formations, ulceration, and atrophy followed by a primary erythema of oral mucosa (initial 3–4 days) [15]. The intensity got maximized within 2 weeks followed by a spontaneous healing at around 21 days [28, 69]. The progression of OM in myeloablative HCT was reported to be worst and faster compared to nonablative chemotherapy. The clinical manifestations of OM specifically generated via a cumulative doses of radiation (from 15 to 20 grays (Gy) with low severity and up to 30 Gy with maximum severity) [4, 28, 69]. RT-induced OM in H&N cancer patients revealed a significant weight loss [20, 43, 89, 96, 122, 124]. Chronic OM was developed in (approximately in 8% of patients with 3.8% developing mouth ulcerations) after H&N RT (post radiation therapy) and revealed with atrophy, telangiectasias, and erythema [41, 67].
Differential Diagnosis
OM can be diagnosed on the basis of onset, patient history, and clinical findings. The clinical course of OM (evaluating the lesions) should not be confused with viral (Herpes simplex virus [HSV]) or secondary fungal (candidiasis) infections. The HSV-induced ulcers differs from OM and usually localized in the areas like the gingivae, keratinized mucosa of the tongue dorsum, and hard palate. On a clinical back ground (swab test or biopsy), the non-HSV viral infections, bacterial, and deep fungal infections (oral) should be differentiated from OM. However, the differential diagnosis towards oral ulceration in OM is deeply associated with erythema multiforme/Stevens–Johnson syndrome and drug eruption [40].
Risk Factors
Patient-Linked Factors
Sex is an important criteria as most of the reported data revealed that females are highly prone towards development of OM [98] and also equally supported by dosimetric analysis (on the basis of calculation of body weight (in kg) or surface area) and performance of baseline [22, 98]. In addition to the above, some non-significant factors like smoking habit, age, body mass index, oral hygiene, genetic variations with drug metabolic pathway, immune signaling, and mechanism of cellular repair are also associated with the risk of OM [50, 98]. Similarly, various other factors associated with development of OM include use of certain medication, comorbidities, preceding therapy, neutropenia/leukopenia, and uncontrolled diabetes mellitus [41].
Tumorigenic Factors
Few tumorigenic factors like stage and site may aggravate the risk for OM and SOM [98]. Radiation regimen (field and dose) associated with H&N cancer therapy increases the risk of exposure for the mucosal tissues leading to development of OM [40].
Treatment-Linked Factors
Several risk factors linked with prognosis of OM are enhanced dose/fractions of RT [70], chemotherapy (by melphalan and methotrexate) [22], and myeloablative situation prior to HCT [23, 77, 105].
Risk Associated with Pediatric Patients
Children with high level of anxiety, low body weight, nausea/vomiting, and previous history of OM are on high priority towards development of OM [16, 75]. Microbial disease conditions such as oral Candida infections, HSV type 1, non-specific bacterial infections [44, 75], retinoblastoma, lymphoma, nephroblastoma, neuroblastoma, and chemotherapy (via daunorubicin, doxorubicin, methotrexate, etoposide, vincristine, cytarabine, and busulfan) reportedly enhanced the risk of OM in pediatric cancer patients [30, 44, 120].
Pathophysiology of OM
Since last decades, the researchers have put significant impact for indulging the complexity of mucositis [110]. A model of five phases started with (i) commencement of cell injury, (ii) boosting of cytokines level, (iii) responses associated with primary damage, (iv) amplification of the signals of inflammatory cascades, and finally (v) the ulceration followed by mucosal repair via proliferation of epithelia [28, 40, 71, 111]. The cascades of OM along with their phases were narrated in Fig. 2 [79, 80]. The phase initiation in mucositis resembles with the CT and/or RCT-based cell damage/injury of oral mucosa in different cancer patients and begins instantly with the initiation of antineoplastic therapy [21, 104, 110]. The upregulation of second phase was by generation of messengers which is associated with development of cytotoxicity, reactive nitrogen species (RNS) and the oxygen species (ROS) causing DNA damage and death of suprabasal and basal epithelial cells [28, 110, 111] with the activation of apoptosis via the induction of nuclear factors like κB (NF-κB) and p53 [13, 123]. The stimulation and release of pro-inflammatory cytokines (via activation of transcription factor) such as tumor necrosis factor (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6) lead to endothelial damage by restraining tissue oxygenation, thereby resulting death of basal cells of epithelia [11, 13, 15, 28, 62, 123]. The pathways depicting the impact of radio-chemotherapy over the healthy oral mucosa and the impact of herbal medicines on cancer chemotherapy-induced OM were depicted in Fig. 3A & B [97]. The signaling as well as amplification (third phase) is subjected to enzyme activation, apoptosis, vascular permeability, and tissue damage resulting in the activation of molecules towards innate immune response causing additional tissue damage [15, 33]. The mucositis-based ulceration (due to the disruption between mucosal and submucosal integrity) as the clinical symptom was noticed in fourth phase along with pain [40, 104, 111]. The increased production of pro-inflammatory cytokines leading to tissue damage was observed in neutropenic [13, 123]. The pathophysiology mucositis was narrated in Fig. 4 [88]. The common infectious elements causing several infections in such patients include Candida albicans, herpes simplex, and Aspergillus [88]. The natural healing of the conditions are usually achieved after the cessation of chemotherapy which can be confirmed by migration, epithelial proliferation, and promotion of extracellular matrix differentiation [28, 111]. After the recovery of the oral mucosa, still the patient has a high risk of recurrence of the disease (because of the residual angiogenesis) [15, 40, 87].

Reproduced with permission from reference [55]
The schematic description of different phases in the biologic progression of mucositis.

Reproduced with permission from reference [62]
A Schematic summary of pathways depicting the possible effects of radio-chemotherapy on the healthy oral mucosa and potential effects of herbal medicine on cancer therapy-induced oral mucositis and its potential related mechanisms. B The potential mechanisms of the effectiveness of herbal bioactive compounds for the treatment of cancer therapy-induced oral mucositis. Herbs with anti-inflammatory and anti-microbial properties can disrupt two main stages of mucositis development with chemotherapy and radiation therapy. Radio-chemotherapy in the first phase of mucositis development increases inflammatory markers. On the other hand, herbal medicine with several mechanisms suppresses inflammatory pathways. For example, these natural products prevent LOX and COX-2activity. As shown in the figure, LOX increases the levels of LTE-4, and COX-2 increases PGE2, both metabolites of polyunsaturated fatty acids, which play a significant role in increasing inflammation. Radio-chemotherapy also increases the amounts of NF-Kb, which increases inflammatory cytokines such as TNF-α, IL-6, and IL-1. NF-Kb also increases the level of NO and the level of COX-2. These inflammatory factors initiate the process of progression of mucositis. Herbal medicine also suppresses the activity of NF-Kb, which results in a significant reduction in inflammatory markers. In addition, herbs with anti-microbial properties can play a significant role in inhibiting mucositis development. COX, cyclooxygenase; LOX, lipoxygenase; PG, prostaglandin; LT, leukotriene; NO, nitric oxide; iNOS, inducible NO synthase; TNF-α, tumor necrosis factor-α; NF-Kb, nuclear factor-KB; IL, interleukin.

Reproduced with permission from reference [64]
Mucositis pathophysiology: a normal tissue and b initiation phase and primary injury response. Radio and chemotherapy-induced damages lead to an increase in DNA double strand brakes and ROS production with a consequent induction of cell apoptosis and DAMPS release. DAMPs and ROS signaling promote the NF-κB-mediated transcription of cytokines; c amplification of the injury signal. The effectors produced during the previous phase lead to an amplification of the injury signal. The released TNF-α initiates the activation of MAPK that sustains NF-κB activity. During this stage, the primary damage signaling is amplified through positive-feedback loop mechanisms. d Ulceration. Breaks in the submucosa allow microorganisms to invade this tissue district leading to mononuclear-infiltrating cells-mediated inflammation response. (e) Tissue re-epithelialization. Stimuli from the submucosa extracellular matrix and mesenchyme promote the healing process.
Curcumin, a Potential Therapeutic Against OM
Curcumin, the key content among the components of curcuma longa is a lipophilic polyphenol and was vastly studied as well as applied towards numerous therapies [55, 61]. Curcumin regulates the cellular apoptosis and proliferation via interacting with kinases, growth factors, transcription factors, enzymes, proteins, and receptors [31, 51, 60, 103]. Curcumin is proven to be beneficial against OM by upregulating TGF-β1, thereby promoting re-epithelialization via stimulation of fibronectin and production of collagen through fibroblasts, thereby accelerating the granulation rate [73, 95, 103]. Apart from that, the nuclear factor-κB (NF-κB) instigation was significantly inhibited by curcumin followed by the activation of nuclear factor erythroid 2-related factor 2 (Nrf2) [73, 95, 103]. COX-2 could be induced selectively via inflammatory and mitogenic stimuli, thereby resulting an elevated prostaglandin synthesis (IL-6). The upregulation of superoxide dismutase (SOD) expression was significantly activated by NF-κB [73, 95, 103]. The summary of descriptive characteristics of included clinical studies containing turmeric preparations against mucositis that was discussed in Table 2 [76]. The expression of the enzymes like glutathione peroxidase (GSH-px), catalase (CAT), SOD, and glutathione (GSH) were enhanced by curcumin by regulating Nrf2 [73, 95, 103]. Similarly, curcumin prorogued the wound-healing activity by declining the levels of lipid peroxides (LPs) [81].
The assessment of a placebo-controlled study of curcumin mouthwash (on pediatrics undergoing CT) towards prevention of OM was conducted [39] and compared with chlorhexidine mouthwash (0.2%, 30 drops twice daily) and Curcumall® (a ginger-curcumin dietary supplement) at 10 drops twice daily during the CT treatment. The results revealed the safety and tolerability of curcumin mouthwash on the patients [39]. In another study, the effectiveness of curcumin mouthwash was analyzed (via a randomized trial) in cancer patients enduring RT and experiencing OM [86]. The case group received curcumin mouthwash (0.004% at a dilution ratio of 1:5, thrice daily for 20 days), whereas the targeting of control group was carried out via chlorhexidine mouthwash (0.2% at a dilution ratio of 1:1, thrice daily for 20 days). The result unveiled a faster wound healing efficiency with a better patient compliance by curcumin mouth wash for managing RT-induced OM (p < 0.001) [86]. The nanomicelles containing curcumin was evaluated for their efficacy against OM (32 patients) in neck and head cancer patients undergoing RT [35]. The case group was receiving Sina Curcumin® [one capsule containing nanomicelles of curcumin (80 mg)] developed by Exir Nano Sina, an industry from Tehran (Iran) during RT, and the control group was subjected to placebo tablets containing lactose. As per the available report, all patients developed OM from placebo group, compared with 32% of the test group [35].
Kia et al. revealed the effectiveness of the curcumin nanomicelles (capsules) towards the prevention/treatment of CT/RT induced OM over the palliative treatments against the head and neck RT induced OM. The report denoted no such significant difference in OM severity at an elevated dose (more than 1 capsules a day) [59]. Normando et al. reported that the patients receiving curcumin mouthwash or gel experienced a low grade pain, mucositis, erythema, and ulceration, denoting an effective control system. Moreover, further clinical trials are obligatory for confirming the impact of curcumin against OM [76]. Shah et al. conducted a randomized clinical trial (with 74 neck and head cancer patients) for evaluating the safety and efficacy of mouth wash containing curcumin nanoparticles (0.1%) and benzydamine mouthwash (0.15%) against radiation-induced oral mucositis (RIOM). The outcomes of MIT analysis revealed a reduced risk (50%) of onset of RIOM in both the mouthwashes. Moreover, curcumin mouthwash (0.1%) has significantly delayed the onset of RIOM [102].
Soni et al. evaluated the impact of turmeric formulation against RCT induced OM in oral cancer patients. Patients, randomized in different groups, received capsules with equal volume of bio-enriched turmeric formulation (BTF) [either at high or low dose, i.e., 1.5 or 1.0 g/day or with the amendment of placebo] on regular basis for a duration of 6 weeks along with RCT. The finding revealed that, BTF (BCM-95®) showed a substantial reduction in RCT induced OM, oral pain, dermatitis, and dysphagia in cancer patients (oral) [107]. Adhvaryu et al. evaluated the impact of curcumin against head and neck cancer induced OM undergoing RCT via a controlled clinical trial group. The results demonstrated a significant reduction in onset of mucositis in both, the curcumin treated and the control groups. Curcumin denoted a remarkable protective efficiency against RCT induced OM. However, a perfectly designed RCT with a prolonged follow-up towards the prognostic implications is imperative [2].
Rao et al. evaluated the effectiveness of turmeric for prevention and treatment of radiation-induced OM. A randomized controlled clinical trial (single-blind) was conducted by considering patients (n = 40) for turmeric gargle or povidone-iodine (n = 40) undergoing CT/RCT. The OM was assessed via RTOG (Radiation Therapy Oncology Group) all over the investigation period. The findings of the study revealed that, in comparison to the gargle of povidone-iodine, the case group who received turmeric gargle showed a delayed and reduced level of OM with the statistical significance (P < 0.001 to P < 0.0001). Patients dealing with turmeric gurgles and undergoing radiation therapy denoted a delayed and reduced severity of OM thus received complete recommendation [91].
Fardad et al. estimated the effectiveness of curcumin, mucosamin, and chlorhexidine against RT/RCT induced OM. The double blind randomized trials (with 71 adult patients suffering from RT/RCT induced OM) were conducted for mucosamin, curcumin, and chlorhexidine groups. On the basis of WHO modulated measures (such as Numerical Rating Scale (NRS) and Oral Mucositis Assessment Scale (OMAS) towards erythema), a thorough recovery was noticed (after third day of receiving the medication) in curcumin group and was considered to be too early paralleled to other groups (P < 0.05). Similarly, the OMAS score towards ulceration revealed (from 5th day onwards) a smart and faster approach in the curcumin group, compared with other groups (P = 0.04). Thus, on the basis of the findings, it can be concluded that though all approaches were effective against OM, but curcumin bids a faster recovery compared to chlorhexidinem and ucosamin [45].
Clinical trials conducted by Zhang et al. have explored curcumin for treatment as well as prevention of OM in carcinoma patients (head and neck). The meta-analysis has unveiled the safety and efficacy of curcumin against CT/RT prompted OM in different cancer patients. Curcumin has significantly abridged the weight loss (conducted six studies with 266 patients) of patients in both therapeutic as well as prophylactic phases. It has also reduced the OM severity compared with chlorhexidine. It has been concluded that curcumin was found to be a safe and natural bioactive which can efficiently preclude and treat RT/CT induced OM along with weight loss [126]. Mansourian et al. evaluated the impact of topical gel of curcuma longa against RT-induced mucositis in neck and head carcinoma patients against a control group. The patients (37) were administered with topical gel of curcuma longa (for 8 weeks) prior of undergoing RT for evaluating the presence/absence of OM. The results revealed an impact of curcumin gel for restricting the progress of OM in case group compared to controls. Thus, it has been concluded that the curcuma formulation was successful in limiting mucositis and thereby helpful in reducing the RT-induced oral lesions size [74].
Another research comprised of the determination of combinational therapeutic response of curcumin and honey against OM by adopting pre and post-test design quasi-experimental non-equivalent control group along with the non-probability purposive sampling technique. The results inferred the effectiveness of the curcumin honey combination against OM [49]. Luer et al. studied the potential difference between the synthetic (sCUR) and naturally derived curcumin (nCUR) against OM. They reported an equipotentiality (via in vitro assays) of both sCUR and nCUR against OM. The sCUR was found to be highly pure, soluble (in DMSO), odorless, tasteless, and lacking batch-to-batch variability of CUR content compared to nCUR. Thus, it was recommended as a promising agent against OM [72].
Dharman et al. have conducted the clinical trials [nine studies with 582 patients undergoing radiation therapy (RT)/RCT] of curcumin administered orally (1500–2000 mg/day), mouth wash of nano curcumin (80 mg/day/0.1%mouthwash), and curcumin topical gel (at an increased frequency) without observing any serious adverse effects. The meta-analysis of case data revealed a reduction in severity as well as delayed onset of the OM during the exposure of RT/RCT compared with the control group. The therapy (curcumin) reduced the level OM (Grade 3). The pain score of curcumin treated group exhibited a significant reduction compared to chlorhexidine. The therapy of curcumin was found to be safe, efficacious, and immensely delay the severity and onset of the RT/RCT-induced OM. Hence, it was recommended against OM with more clinical trial approaches for further clarification [36].
Patents
The prevention and treatment protocol for mucositis containing either single or combinational approaches of curcumin was invented by Sonis et al. for the patients/individuals preparing to undergo or undergoing cancer therapy [112]. In another study, Rezvani et al. have invented the anticipation and management of mucositis by a combinational approach of curcumin with sunflower oil and α-tocopherol [92]. Novel methods and compositions were designed by Bascomb et al. that provide cytoprotection (either alone or in amalgamation with several chemo or radiation cancer therapies) against cancer-induced digestive mucositis, oral mucositis, intestinal mucositis, and esophageal mucositis [14]. Similarly, the innovative approach of Rosenthal et al. comprised of a therapeutic composition containing biocompatible reverse-thermal gelation polymer against mucositis [94]. Moreover, a novel composition comprising of gamma-cyclodextrin and curcumin (1:1) was invented by Parkkinen et al. The developed complex of curcumin (stable and water-soluble) was effective against cancer-induced gastrointestinal and oral mucositis and was found to be applicable against animal and human subjects [82].
Expert Opinion
Being a culinary constituent, curcumin is effective towards the prevention/treatment of OM (palliative and local treatments) induced either by radiotherapy or chemotherapy. Though plenty of options are available for the treatment of OM, but still curcumin in its differential formulation approaches could be highly effective (evidenced from clinical trial outcomes) with minimum side effects and maximum safety. The need of the hour to explore such therapeutic is maintenance of its purity, defining of dosing accuracy, wide clinical trial approach with a sufficient number of patients, validated/approved clinical trial protocol by the competent authority, and the industrial scale-up. Statistical approach–based validation of clinical data could be an advanced approach which can accelerate the process of clinical trial efficacy with minimum error and maximum output. Some advanced therapeutic controlled trials with novel formulations like nano-therapeutics such as curcumin-loaded liposomes, phytosomes, trasferosomes, and ethosomes could be developed which can accelerate the healing process. Similarly, some oral mucoadhessive sprays containing the drug components could be planned for a better and prompt therapy. Multiple drug approach from natural origin could be a great choice to overcome resistant mucositis.
Conclusions and Future Perspectives
A numerous antineoplastic therapies resulted OM, as a devastating side effect. Moreover, the expanded pathogenesis of the disease permits a sound predictability over the patient’s risk thereby directing its adaptability and management protocols towards the achievement of novel therapeutics. Nevertheless, standard guidelines towards management of OM (prevention and treatment) have displayed any effectiveness significantly. In recent era, an augmented interest towards curcumin (a natural product) as a potential therapeutic was emerged because of its easy accessibility, antioxidant, anti-inflammatory, antiulcer, antimicrobial, and wound-healing abilities along with reduced side effects. Curcumin can potentially alter OM and OM-induced weight loss but showed a great heterogeneity. Furthermore, in view of the limitations, the benefits must be corroborated via high-quality RCTs. Over few years, multiple efforts have been appended for developing nature based therapies. Natural compounds were now being exposed for clinical trials. Despite of the advancements made in this area (few products already existing in the market), still more investigations are essential to ensure the market appearance/launching of such products in bulk.
Data Availability
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
References
Abt E (2021) Probiotics may lower the risk of oral mucositis in cancer patients. J Evid-Based Dental Pract 21(4):101639
Adhvaryu M, Vakharia B, Reddy N (2018) Curcumin prevents mucositis and improves patient compliance in head and neck cancer patients undergoing radio-chemotherapy. Ann Med Chem Res 4:1–9
Agheli R, Siavashpour Z, Reiazi R, Azghandi S, Cheraghi S, Paydar R (2024) Predicting severe radiation-induced oral mucositis in head and neck cancer patients using integrated baseline CT radiomic, dosimetry, and clinical features: a machine learning approach. Heliyon 10(3):1–13
Al-Ansari S, Zecha JA, Barasch A et al (2015) Oral mucositis induced by anticancer therapies. Curr Oral Heal Report 2:202–211
Alibakhshi A, Ranjbari J, Pilehvar-Soltanahmadi Y et al (2016) An update on phytochemicals in molecular target therapy of cancer: potential inhibitory effect on telomerase activity. Curr Med Chem 23(22):2380–2393
Alkhouli M, Laflouf M, Comisi JC (2021) Assessing the topical application efficiency of two biological agents in managing chemotherapy-induced oral mucositis in children: a randomized clinical trial. J Oral Biol Cranio Res 11(3):373–378
Anand P, Kunnumakkara AB, Newman RA et al (2007) Bioavailability of curcumin: problems and promises. Mol Pharm 4(6):807–818
Anderson CM, Lee CM, Saunders DP et al (2019) Phase IIb, randomized, double-blind trial of GC4419 versus placebo to reduce severe oral mucositis due to concurrent radiotherapy and cisplatin for head and neck cancer. J Clinic Oncol 37(34):3256
Anthwal A, Thakur BK, Rawat MS et al (2014) Synthesis, characterization and in vitro anticancer activity of C-5 curcumin analogues with potential to inhibit TNF-α-induced NF-κB activation. Bio Med Res Int 2014:524161
Arbabi-kalati F, Arbabi-kalati F, Deghatipour M et al (2012) Evaluation of the efficacy of zinc sulfate in the prevention of chemotherapy-induced mucositis: a double-blind randomized clinical trial. Arch Iran Med Amer Inst Math 15(7):413–417
Ariyawardana A, Cheng KKF, Kandwal A et al (2019) Mucositis study group of the Multinational Association of Supportive Care in Cancer/International Society for Oral Oncology (MASCC/ISOO). Systematic review of anti-inflammatory agents for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer 27(10):3985–3995
Arun P, Sagayaraj A, Azeem MSM et al (2020) Role of turmeric extract in minimising mucositis in patients receiving radiotherapy for head and neck squamous cell cancer: a randomised, placebo-controlled trial. J Laryngol Otol 134(2):159–164
Bailly C (2019) Potential use of edaravone to reduce specific side effects of chemo-, radio- and immuno-therapy of cancers. Int Immunopharmacol 77:105967
Bascomb N, Maki J, Young FS (2009) Compositions and methods for mucositis and oncology therapies. EP2259844A1
Basile D, Di NP, Corvaja C et al (2019) Mucosal injury during anti-cancer treatment: from pathobiology to bedside. Cancers 11(6):857
Bektaş-Kayhan K, Küçükhüseyin Ö, Karagöz G et al (2012) Is the MDR1 C3435T polymorphism responsible for oral mucositis in children with acute lymphoblastic leukemia. Asian Pac J Cancer Prev 13(10):5251–5255
Belfiore E, Di Prima G, Angellotti G, Panzarella V, De Caro V (2024) Plant-derived polyphenols to prevent and treat oral mucositis induced by chemo-and radiotherapy in head and neck cancers management. Cancers 16(2):260
Bensadoun RJ, Le Page F, Darcourt V et al (2006) Radiation-induced mucositis of the aerodigestive tract: prevention and treatment. MASCC/ISOO mucositis group’s recommendations. Bull du Cancer 93(2):201–211
Bergamaschi L, Vincini MG, Zaffaroni M, Pepa M, Angelicone I, Astone A, Bergamini C, Buonopane S, Conte M, De Rosa N, Deantoni C (2024) Management of radiation-induced oral mucositis in head and neck cancer patients: a real-life survey among 25 Italian radiation oncology centers. Support Care Cancer 32(1):38
Berger K, Schopohl D, Bollig A (2018) Burden of oral mucositis: a systematic review and implications for future research. Oncol Res Treat 41(6):399–405
Bertolini M, Sobue T, Thompson A et al (2017) Chemotherapy induces oral mucositis in mice without additional noxious stimuli. Trans Oncol 10(4):612–620
Blijlevens N, Schwenkglenks M, Bacon P et al (2008) Prospective oral mucositis audit: oral mucositis in patients receiving high-dose melphalan or BEAM conditioning chemotherapy—European Blood and Marrow Transplantation Mucositis Advisory Group. J Clinic Oncol 26(9):1519–1525
Bourhis J, Lapeyre M, Tortochaux J et al (2006) Phase III randomized trial of very accelerated radiation therapy compared with conventional radiation therapy in squamous cell head and neck cancer: a GORTEC trial. J Clinic Oncol 24(18):2873–2878
Charantimath S (2016) Use of curcumin in radiochemotherapy induced Oral mucositis patients: a control trial study. World Acad Sci Eng Technol Int J Med Health Biomed Bioeng Pharm Eng 10(3):147–152
Chaudhry HM, Bruce AJ, Wolf RC et al (2016) The incidence and severity of oral mucositis among allogeneic hematopoietic stem cell transplantation patients: a systematic review. Biol Blood Marrow Transplant 22(4):605–616
Chaveli-López B, Bagán-Sebastián JV (2016) Treatment of oral mucositis due to chemotherapy. J Clinic Exp Dentist 8(2):e201–e209
Chaveli-López B (2014) Oral toxicity produced by chemotherapy: a systematic review. J Clinical Exp Dentist 6(1):e81–e90
Cinausero M, Aprile G, Ermacora P (2017) New frontiers in the pathobiology and treatment of cancer regimen-related mucosal injury. Front Pharmacol 8:354
Colella G, Boschetti CE, Vitagliano R (2023) Interventions for the prevention of oral mucositis in patients receiving cancer treatment: evidence from randomised controlled trials. Current Oncol 30(1):967–980
Curra M, Gabriel AF, Ferreira MBC et al (2021) Incidence and risk factors for oral mucositis in pediatric patients receiving chemotherapy. Support Care Cancer 29:6243–6251
Das L, Vinayak M (2014) Curcumin attenuates carcinogenesis by down regulating proinflammatory cytokine interleukin-1 (IL-1α and IL-1β) via modulation of AP-1 and NF-IL6 in lymphoma bearing mice. Int Immunopharmacol 20(1):141–147
Daugėlaitė G, Užkuraitytė K, Jagelavičienė E et al (2019) Prevention and treatment of chemotherapy and radiotherapy induced oral mucositis. Medicina 55(2):25
Davy C, Heathcote S (2021) A systematic review of interventions to mitigate radiotherapy-induced oral mucositis in head and neck cancer patients. Support Care Cancer 29(4):2187–2202
De SV, Bossi P, Sanguineti G et al (2016) Mucositis in head and neck cancer patients treated with radiotherapy and systemic therapies: literature review and consensus statements. Crit Rev Oncol/Hematol 100:147–166
Delavarian Z, Pakfetrat A, Ghazi A et al (2019) Oral administration of nanomicelle curcumin in the prevention of radiotherapy-induced mucositis in head and neck cancers. Spe Care Dentist 39(2):166–172
Dharman SGM, Shanmugasundaram K, Sampath RK (2021) A systematic review and meta-analysis on the efficacy of curcumin/turmeric for the prevention and amelioration of radiotherapy/radiochemotherapy induced oral mucositis in head and neck cancer patients. Asian Pac J Cancer Prevent 22(6):1671–1684
Di Fede O, Canepa F, Maniscalco L, Tozzo P, Matranga D, Giuliana G (2023) Prevention and the treatment of oral mucositis: the efficacy of sodium bicarbonate vs other agents: a systematic review. BMC Oral Health 23(1):4
Elad S, Cheng KKF, Lalla RV et al (2020) MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 126(19):4423–4431
Elad S, Meidan I, Sellam G et al (2013) Topical curcumin for the prevention of oral mucositis in pediatric patients: Case series. Alternat Therapies Health Med 19(3):21–24
Elad S, Yarom N, Zadik Y et al (2022) The broadening scope of oral mucositis and oral ulcerative mucosal toxicities of anticancer therapies. CA: A Cancer J Clinic 72(1):57–77
Elad S, Zadik Y (2016) Chronic oral mucositis after radiotherapy to the head and neck: a new insight. Support Care Cancer 24:4825–4830
Elting LS, Chang YC (2019) Costs of oral complications of cancer therapies: estimates and a blueprint for future study. JNCI Monographs. 53:lgz010
Elting LS, Cooksley CD, Chambers MS et al (2007) Risk, outcomes, and costs of radiation-induced oral mucositis among patients with head-and-neck malignancies. Int J Radiation Oncol Biol Physic 68(4):1110–1120
Fadda G, Campus G, Lugliè P (2006) Risk factors for oral mucositis in paediatric oncology patients receiving alkylant chemotherapy. BMC Oral Heal 6(1):1–8
Fardad F, Ghasemi K, Ansarinejad N et al (2023) A comparative study to assess the effectiveness of curcumin, mucosamin, and chlorhexidine in chemotherapy-induced oral mucositis. Explore 19(1):65–70
Farias GA, Silveira FM, Curra M et al (2022) Risk factors associated with the development of oral mucositis in pediatric oncology patients: Systematic review and meta-analysis. Oral Disease 28(4):1068–1084
Fede O, Canepa F, Maniscalco L et al (2023) Prevention and the treatment of oral mucositis: the efficacy of sodium bicarbonate vs other agents: a systematic review. BMC Oral Health 23(1):1–13
Fidan Ö, Arslan S (2021) Development and validation of the oral mucositis risk assessment scale in hematology patients. Seminar Oncol Nurs 37(3):151159
Francis M, Williams S (2014) Effectiveness of Indian turmeric powder with honey as complementary therapy on Oral mucositis: A nursing perspective among Cancer patients in Mysore. Nurs J India 105(6):258–260
Frey-Furtado L, Magalhães I, Azevedo MJ, et al (2023) The role of biotics as a therapeutic strategy for oral mucositis-a systematic review. Probiot Antimicrob Protein 1–14
Gandhy SU, Kim K, Larsen L et al (2012) Curcumin and synthetic analogs induce reactive oxygen species and decreases specificity protein (Sp) transcription factors by targeting microRNAs. BMC Cancer 12:564
Garming LK, Ringdén O, Remberger M et al (2021) Oral mucositis after tacrolimus/sirolimus or cyclosporine/methotrexate as graft-versus-host disease prophylaxis. Oral Disease 27(5):1217–1225
Ghalandarlaki N, Alizadeh AM, Ashkani-Esfahani S (2014) Nanotechnology-applied curcumin for different diseases therapy. Bio Med Res Int 2014:394264
Gupta SC, Patchva S, Koh W et al (2012) Discovery of curcumin, a component of golden spice, and its miraculous biological activities. Clinic Exp Pharmacol Physiol 39(3):283–299
Gupta SC, Sung B, Kim JH et al (2013) Multitargeting by turmeric, the golden spice: from kitchen to clinic. Molecul Nutri Food Res 57(9):1510–1528
Harris DJ, Eilers J, Harriman A et al (2008) Putting evidence into practice®: evidence-based interventions for the management of oral mucositis. Clinic J Oncol Nurs 12(1):141–152
Hearnden V, Sankar V, Hull K (2012) New developments and opportunities in oral mucosal drug delivery for local and systemic disease. Adv Drug Deliv Review 64(1):16–28
Kawashita Y, Koyama Y, Kurita H (2019) Effectiveness of a comprehensive oral management protocol for the prevention of severe oral mucositis in patients receiving radiotherapy with or without chemotherapy for oral cancer: a multicentre, phase II, randomized controlled trial. Int J Oral Maxillofacial Surg 48(7):857–864
Kia SJ, Basirat M, Saedi HS et al (2021) Effects of nanomicelle curcumin capsules on prevention and treatment of oral mucosits in patients under chemotherapy with or without head and neck radiotherapy: A randomized clinical trial. BMC Complement Médecine Therapeutiq 21:1–11
Kim SG, Veena MS, Basak SK et al (2011) Curcumin treatment suppresses IKKβ kinase activity of salivary cells of patients with head and neck cancer: a pilot study. Clinic Cancer Res 17(18):5953–5961
Kocaadam B, Şanlier N (2017) Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit Rev Food Sci Nutri 57(13):2889–2895
Kudrimoti M, Curtis A, Azawi S (2016) Dusquetide: A novel innate defense regulator demonstrating a significant and consistent reduction in the duration of oral mucositis in preclinical data and a randomized, placebo-controlled phase 2a clinical study. J Biotechnol 239:115–125
Kumar D, Kaur P, Bansal N et al (2016) A prospective randomized study evaluating the role of Oral curcumin along with chemoradiation in management of locally advanced head and neck carcinoma. Int J Trop Disease Health 16(1):1–7
Kusiak A, Jereczek-Fossa BA, Cichońska D et al (2020) Oncological-therapy related oral mucositis as an interdisciplinary problem-literature review. Int J Environ Res Public Health 17(7):2464
Lalla RV, Bowen J, Barasch A et al (2014) MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 120(10):1453–1461
Lalla RV, Saunders DP, Peterson DE (2014) Chemotherapy or radiation-induced oral mucositis. Dent Clinic North Amer 58(2):341–349
Lalla RV, Treister N, Sollecito T et al (2017) Oral complications at 6 months after radiation therapy for head and neck cancer. Oral disease 23(8):1134–1143
Lestari ML, Indrayanto G (2014) Curcumin. In: profiles of drug substances, excipients and related methodology. Academic Press, pp 39
Li J, Zhu C, Zhang Y et al (2023) Incidence and risk factors for radiotherapy-induced oral mucositis among patients with nasopharyngeal carcinoma: a meta-analysis. Asian Nurs Res 17(2):70–82
Li K, Yang L, Xin P et al (2017) Impact of dose volume parameters and clinical factors on acute radiation oral mucositis for locally advanced nasopharyngeal carcinoma patients treated with concurrent intensity-modulated radiation therapy and chemoradiotherapy. Oral Oncol 72:32–37
Logan RM, Stringer AM, Bowen JM et al (2007) The role of pro-inflammatory cytokines in cancer treatment-induced alimentary tract mucositis: pathobiology, animal models and cytotoxic drugs. Cancer Treat Review 33(5):448–460
Luer SC, Goette J, Troller R (2014) Christoph Aebi synthetic versus natural curcumin: bioequivalence in an in vitro oral mucositis model. BMC Complement Alternat Med 14:1–7
Mani H, Sidhu GS, Kumari R et al (2002) Curcumin differentially regulates TGF-beta1, its receptors and nitric oxide synthase during impaired wound healing. Bio Factor 16(1–2):29–43
Mansourian A, Amanlou M, Shirazian S et al (2015) The effect of “Curcuma longa” topical gel on radiation-induced oral mucositis in patients with head and neck cancer. Iran J Radiation Res 13(3):269–274
Mendonca RM, Araujo M, Levy CE et al (2015) Oral mucositis in pediatric acute lymphoblastic leukemia patients: evaluation of microbiological and haematological factors. Pediatr Hematol Oncol 32:322–330
Normando AGC, de Menêses AG, de Toledo IP et al (2019) Effects of turmeric and curcumin on oral mucositis: a systematic review. Phytother Res 33(5):1318–1329
Oronsky B, Goyal S, Kim MM et al (2018) A review of clinical radioprotection and chemoprotection for oral mucositis. Translation Oncology 11(3):771–778
Overgaard J, Hansen HS, Specht L et al (2003) Five compared with six fractions per week of conventional radiotherapy of squamous- cell carcinoma of head and neck: DAHANCA 6 and 7 ran-domised controlled trial. Lancet 362:933–940
Panahi Y, Hosseini MS, Khalili N et al (2016a) Effects of curcumin on serum cytokine concentrations in subjects with metabolic syndrome: a post-hoc analysis of a randomized controlled trial. Biomed Pharmacother 82:578–582
Panahi Y, Saadat A, Shadboorestan A et al (2016b) An updated review of natural products intended to prevent or treat oral mucositis in patients undergoing radio-chemotherapy. Current Pharm Biotechnol 17(11):949–961
Panchatcharam M, Miriyala S, Gayathri VS et al (2006) Curcumin improves wound healing by modulating collagen and decreasing reactive oxygen species. Molecul Cellular Biochem 290(1–2):87–96
Parkkinen J (2013) Soluble complexes of curcumin. US 8,568,815 B2
Patel P, Robinson PD, Baggott C, Gibson P, Ljungman G, Massey N, Ottaviani G, Phillips R, Revon-Riviere G, Treister N, White M (2021) Clinical practice guideline for the prevention of oral and oropharyngeal mucositis in pediatric cancer and hematopoietic stem cell transplant patients: 2021 update. Eur J Cancer 154:92–101
Patil K, Guledgud MV, Kulkarni PK, KeShari D, Tayal S (2015) Use of curcumin mouthrinse in radio-chemotherapy induced oral mucositis patients: a pilot study. J Clin Diagn Res 9(8):ZC59
Patil K, Guledgud MV, Kulkarni PK et al (2016) Use of curcumin mouth rinse in radio-chemotherapy induced Oral Mucositis patients: A pilot study. J Clinic Diagnos Res 9(8):ZC59–ZC62
Peterson DE, Lalla RV (2010) Oral mucositis: the new paradigms. Current Opinion Oncol 22(4):318–322
Pulito C, Cristaudo A, Porta C et al (2020) Oral mucositis: the hidden side of cancer therapy. J Exp Clinic Cancer Res 39(1):210
Raber DJE, Elad S, Barasch A (2010) Oral mucositis. Oral Oncol 46(6):452–456
Rahimi HR, Nedaeinia R, Sepehri SA et al (2016) Novel delivery system for natural products: nano-curcumin formulations. Avicenna J Phytomed 6(4):383–398
Rao S, Dinkar C, Vaishnav LK et al (2014) The Indian spice turmeric delays and mitigates radiation-induced oral mucositis in patients undergoing treatment for head and neck cancer: an investigational study. Integrat Cancer Therapies 13(3):201–210
Rezvani M (2003) Curcumin for the prevention and/or treatment of tissue damage. AU2003229923A1
Rodrigues-Oliveira L, Kowalski LP, Santos M et al (2021) Direct costs associated with the management of mucositis: a systematic review. Oral Oncol 118:105296
Rosenthal GJ, Etter JB, Rodell TC, et al (2003) Treatment of mucositis. WO2002041837A2, 2001, 2006
Rujirachotiwat A, Suttamanatwong S (2021) Curcumin upregulates transforming growth factor-_1, its receptors, and vascular endothelial growth factor expressions in an in vitro human gingival fibroblast wound healing model. BMC Oral Health 21(1):535
Russo G, Haddad R, Posner M et al (2008) Radiation treatment breaks and ulcerative mucositis in head and neck cancer. Oncologist 13(8):886–898
Safarzadeh S, Shirban F, Bagherniya M et al (2022) The effects of herbal medicines on cancer therapy-induced oralmucositis: a literature review. Phytother Res 36(1):243–265
Sahebkar A, Serban MC, Ursoniu S et al (2015) Effect of curcuminoids on oxidative stress: a systematic review and meta-analysis of randomized controlled trials. J Function Food 18:898–909
Saldanha SP, Almeida VD (2014) A comparative study to assess the effectiveness of turmeric mouth wash versus saline mouth wash on treatment induced oral mucositis (tiom) in a selected hospital at mangalore. J Clinic Res Bioeth 5(6):1–5
Sampson MM, Nanjappa S, Greene JN (2017) Mucositis and oral infections secondary to gram negative rods in patients with prolonged neutropenia. Oral Disease 12(3):229–241
Shah S, Rath H, Sharma G et al (2020) Effectiveness of curcumin mouthwash on radiation-induced oral mucosits among head and neck cancer patients: a triple-blind, pilot randomised controlled trial. Ind J Dent Res 31(5):718–727
Shehzad A, Lee YS (2010) Curcumin: multiple molecular targets mediate multiple pharmacological actions: a review. Drugs Future 35(2):113
Shetty SS, Maruthi M, Dhara V et al (2022) Oral mucositis: current knowledge and future directions. Dis Mon 68(5):101300
Shouval R, Kouniavski E, Fein J et al (2019) Risk factors and implications of oral mucositis in recipients of allogeneic hematopoietic stem cell transplantation. Europe J Haematol 103(4):402–409
Singh V, Singh AK (2020) Oral mucositis. Nat J Maxillofacial Surgery 11(2):159–168
Soni TP, Gupta AK, Sharma LM et al (2022) A randomized, placebo-controlled study to evaluate the effect of bio-enhanced turmeric formulation on radiation-induced oral mucositis. ORL; J Oto-Rhino-Laryngology and Its Related Specialties 84(2):103–113
Sonis ST, Eilers JP, Epstein JB (1999) Validation of a new scoring system for the assessment of clinical trial research of oral mucositis induced by radiation or chemotherapy. Mucositis Study Group Cancer 85(10):2103–2113
Sonis ST, Elting LS, Keefe D et al (2004) Perspectives on cancer therapy-induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer 100(9):1995–2025
Sonis ST (2021) A hypothesis for the pathogenesis of radiation-induced oral mucositis: when biological challenges exceed physiologic protective mechanisms. Implications for pharmacological prevention and treatment. Support Care Cancer 29(9):4939–4947
Sonis ST (2009) Mucositis: The impact, biology and therapeutic opportunities of oral mucositis. Oral Oncol 45(12):1015–1020
Sonis ST (2002) Treatment and prevention of mucositis in cancer patients. WO2003024391A2
Sung H, Ferlay J, Siegel RL (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J Clinician 71(3):209–249
Szturz P, Wouters K, Kiyota N et al (2018) Altered fractionation radiotherapy combined with concurrent low- dose or high- dose cisplatin in head and neck cancer: a systematic review of literature and meta- analysis. Oral Oncol 76:52–60
Szymusiak M, Hu X, Leon PPA et al (2016) Bioavailability of curcumin and curcumin glucuronide in the central nervous system of mice after oral delivery of nano-curcumin. Int J Pharmaceutic 511(1):415–423
Toden S, Goel A (2017) The Holy Grail of curcumin and its efficacy in various diseases: is bioavailability truly a big concern? J Restorat Med 6(1):27–36
Tran PHL, Duan W, Tran TTD (2019) Recent developments of nanoparticle-delivered dosage forms for buccal delivery. Int J Pharmaceutic 571:118697
Ueno T, Zenda S, Konishi T et al (2019) The post hoc analysis comparing the severity grades of chemoradiotherapy-induced oral mucositis scored between the central and local assessors in a multicenter, randomized controlled trial of rebamipide for head and neck cancer. Int J Clinic Oncol 24:241–247
Vagliano L, Feraut C, Gobetto G et al (2011) Incidence and severity of oral mucositis in patients undergoing haematopoietic SCT—results of a multicentre study. Bone Marrow Ttransplant 46(5):727–732
Valer JB, Curra M, Gabriel ADF et al (2021) Oral mucositis in childhood cancer patients receiving high-dose methotrexate: prevalence, relationship with other toxicities and methotrexate elimination. Int J Paedia Dentist 31(2):238–246
Vasconcellos FPM, Gomes MF, Almeida SM et al (2023) Evaluation of oral mucositis, candidiasis, and quality of life in patients with head and neck cancer treated with a hypofractionated or conventional radiotherapy protocol: a longitudinal, prospective, observational study. Head Face Med 19(1):1–10
Vera-Llonch M, Oster G, Ford CM et al (2007) Oral mucositis and outcomes of allogeneic hematopoietic stem-cell transplantation in patients with hematologic malignancies. Support Care Cancer 15:491–496
Vigarios E, Epstein JB, Sibaud V (2017) Oral mucosal changes induced by anticancer targeted therapies and immune checkpoint inhibitors. Support Care Cancer 25(5):1713–1739
Villa A, Sonis ST (2023) Radiotherapy-induced severe oral mucositis: pharmacotherapies in recent and current clinical trials. Expert Opinion Investigation Drugs 32(4):301–310
Volpato LER, Silva TC, Oliveira TM et al (2007) Radiation therapy and chemotherapy-induced oral mucositis. Revista Brasil Otorrinolaringolog 73:562–568
Wardill HR, Sonis ST, Blijlevens NMA et al (2020) Prediction of mucositis risk secondary to cancer therapy: a systematic review of current evidence and call to action. Support Care Cancer 28:5059–5073
Zecha JAEM, Raber DJE, Nair RG et al (2016) Low-level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: part 2: proposed applications and treatment protocols. Support Care Cancer 24(6):2793–2805
Zhang L, Tang G, Wei Z (2021) Prophylactic and therapeutic effects of curcumin on treatment-induced oral mucositis in patients with head and neck cancer: a meta-analysis of randomized controlled trials. Nutr Cancer 73(5):740–749
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Not applicable.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sarangi, M.K. Potentiality of Curcumin Against Radio-Chemotherapy Induced Oral Mucositis: A Review. Indian J Surg Oncol (2024). https://doi.org/10.1007/s13193-024-02082-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13193-024-02082-x