
Abstract
Introduction
Compared with heterosexual individuals, sexual minorities who experienced sexual minority stigma had greater risks for psychopathology. Drawn from the psychological mediation framework, this study focused on the psychological mechanisms of resilience and family support through which sexual minority stigma affected depressive symptoms among sexual minorities in China.
Methods
In 2019, 301 LGBTQ individuals (10.78% lesbian, 56.21% gay, 21.24% bisexual, 20.93% others; 66.11% males, 25.91% females, 7.97% others) aged between 18 and 42 participated in an online survey in China. The survey assessed their minority stress, resilience, family support, and depressive symptoms. Data were analyzed using path analysis.
Results
Sexual minority stigma was negatively related to resilience and family support while positively related to depression. Resilience and family support were negatively associated with depression. Path analysis indicated that resilience and family support mediated the relationship between sexual minority stigma and depression.
Conclusions
The findings revealed the underlying mechanisms of how sexual minority stigma developed into depression. Both resilience and family support mediated the relationship between sexual minority stigma and depression. Future interventions could target both factors to alleviate the negative impact of sexual minority stigma on the mental health of Chinese sexual minorities.
Policy Implications
More interventions are needed to address mental health disparities in Chinese LGBTQ individuals who suffered from sexual minority stigma. Building up resilience of and cultivating family support for sexual minorities should be prioritized in the implementation of social policies in accordance with the Healthy China 2030 agenda.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Sexual minorities have been found to experience exacerbated mental health. Findings from different countries consistently indicated that, compared with heterosexuals, sexual minorities reported a significantly higher level of depression (Fergusson et al., 2005; Sandfort et al., 2006). A systematic review and meta-analysis of international population-based studies emphasized that sexual minority youth had elevated rates of depressive symptoms in comparison to heterosexual young people (Lucassen et al., 2017). However, more than half of the reviewed studies in the meta-analysis were conducted in the USA, with only two studies carried out in Asia. Sexual minorities in China also struggled with depression remarkably. A recent study in Shanghai indicated that 26.8% sexual minority individuals reported moderate-to-severe symptoms of depression and a feeling of loneliness (Su et al., 2018). While in Wenzhou, 34.6% participants reported major depressive symptoms during the past 6 months and 16.1% of them reported suicidal ideation (Pan et al., 2018). In addition, a national survey in China indicated 85% of lesbian, gay, bisexual, transgender, and queer (LGBTQ) students reported feeling depressed and around 40% of them had suicidal thoughts (Wei & Liu, 2019). Accumulating findings showed that mental health in Chinese sexual minorities was dire.
Sexual Minority Stigma and LGBT Depression in China
One of the explanations to their adverse mental health was that sexual minorities were constantly exposed to stress from prejudice, discrimination, or stigma (Hatzenbuehler, 2009; Meyer, 2003). These stressors were closely related to their mental health. According to the minority stress model, compared with heterosexual and cisgender individuals, sexual minorities suffered from excess stress because of their stigmatized social status (Meyer, 2003). The excess stress, defined as minority stress, was induced by an individual’s experiences of prejudice events (experienced stigma), anticipation of stigmatizing events (normative stigma), and internalized homophobia (self or internalized stigma) (Meyer, 2003). Recent literature supported the minority stress model in understanding stigma and mental health in Chinese sexual minorities. In a study of four cities in northeastern China, gay and bisexual men who experienced stigma were more frequently at risk with elevated depressive symptoms (Liu et al., 2018). Besides, anticipated stigma was positively related to depression 6 months later in a longitudinal sample of gay and bisexual men in Beijing, China (Choi et al., 2016). A study in southwest China found that gay and bisexual men with high internalized stigma experienced more psychological distress (Xu et al., 2017). Extending the minority stress framework, LGBTQ individuals also suffered from HIV-related vicarious stigma and media portrayal stigma (Thaker et al., 2018). These additional stressors led to poor mental health, particularly depression. Moreover, minority stigma could intersect with ethnic stigma in LGBT community and LGBT stigma in the community, creating multiple minority stress (McConnell et al., 2018). Overall, a number of sexual minority stigma stressors confronted by Chinese minorities resulted in a higher rate of depression compared with their heterosexual/cisgender counterparts.
The Psychological Mediation Framework
The established link between minority stress and mental health necessitated a nuanced understanding in how these stressors impaired mental health. The psychological mediation framework was thus proposed to explain the mechanisms linking stigma to mental health (Hatzenbuehler, 2009). It posited that stigma experienced by sexual minorities shaped intrapersonal and interpersonal processes which subsequently conferred risk for psychopathology (Hatzenbuehler, 2009). The framework postulated three processes, namely cognitive, affective, and interpersonal. Changes in cognitive processes included hopelessness, pessimism, and negative self-schema. Affective processes entailed maladaptive coping and rumination. Finally, interpersonal processes delineated occurrence of social isolation (Hatzenbuehler, 2009).
Role of Resilience
According to Hatzenbuehler (2009), at an intrapersonal level, chronic stigma initiated dysfunctional coping and emotional regulation processes because stigma depleted one’s self-control and psychological resources to regulate emotion. These deficits exposed sexual minorities to vulnerabilities in depression. Supporting this framework, Zheng et al. (2020) found that minority stress and stress to get married were associated with poor mental health through coping and negative cognition among Chinese single LGB individuals. However, few studies examined whether resilience might be activated by the stressful stigmatized experiences and how resilience functioned in the process of confronting stigma (Grant et al., 2003). Resilience referred to the ability to withstand and recover from adversity (Masten, 2007). As posited by Meyer (2015), resilience was interconnected with stigma. The quality of bouncing back and functioning adaptively was demonstrated in the presence of minority stress. Though adaptive in nature, resilience might be exhausted by chronic minority stress, and the drain of resilience might impact mental health. In a study of transgender in Jamaica, resilient coping was found to mediate sexual stigma and depression (Logie et al., 2020). More sexual stigma led to less resilient coping which then led to greater depression. In another study of HIV-positive MSM in Nanjing, China, resilience mediated perceived stigma and self-esteem, which led to depression (Yan et al., 2019). The present study sought to expand the psychological mediation framework to sexual minorities in China. We posited that sexual minority stigma predicted resilience which bridged the relation between stigma and depression.
Role of Social Support
Besides, in the framework by Hatzenbuehler (2009), social support was proposed to mediate the relation between minority stress and mental health at an interpersonal level. While social support entailed support from family, friends, and others, family support was particularly relevant to the wellbeing of sexual minorities in China. It was because Chinese valued family relationships over other social relationships. As such, prejudice from family members might disproportionally affect sexual minorities. A national cross-sectional survey revealed that more than a tenth of heterosexual participants were unable to accept LGBT family members (Wang et al., 2019). The rejection rate of family relationships was two to five times higher than those of other social relationships. The participants also reported a low acceptance rate of their own children being sexual minorities (Wang et al., 2019). The survey clearly demonstrated the profound rejection prevalent in families and the compelling role of family support in considering the process between stigma and psychopathology. A study among Chinese LGBs indicated that a low level of perceived parental support for sexual orientation was associated with elevated depression, anxiety, and loneliness (Shao et al., 2018). Conversely, family acceptance predicted greater general health status and protected against depression in LGBT young adults (Ryan et al., 2010; Snapp et al., 2015). Informed by the framework, the study by Chan and Mak (2019) indicated that peer isolation, along with negative self-concept and maladaptive coping, mediated the relation between HIV stigma and poor mental health for Chinese gay and bisexual men living with HIV. However, the study by Chan and Mak (2019) focused on peer support. We believed that family support was also worth an in-depth examination as it might put a greater strain on sexual minorities in a Chinese context. Besides, most previous studies were concerned with sexual minorities in a single city or a few cities in China. The present study addressed the gap by including a heterogeneous sample of sexual minorities across China, thereby providing a comprehensive perspective on the current stigmatizing experiences and protective processes across provinces in China. Besides, this study aimed to capture the experiences of all sexual minorities by including lesbians, gay, bisexuals, and transgenders.
The Present Study
Informed by the psychological mediation framework, the present study sought to gain a better understanding of the processes that explained the relationship between stigma and depression among sexual minorities in China. We proposed resilience as an intrapersonal psychological process and social support as an interpersonal one. The present study aimed to evaluate whether resilience and family support served as underlying psychological mechanisms accounting for the relation between sexual minority stigma and depression. The first hypothesis was that higher levels of sexual minority stigma would be associated with elevated depression, whereas greater resilience and family support would be associated with a lower level of depression. The second hypothesis was that resilience and family support would mediate the association between sexual minority stigma and depression, respectively. Identifying factors that mediate sexual minority stigma and mental health should shed light on potential interventions and social policies that target on reducing LGBT mental health disparities.
Method
Participants
The sample consisted of 301 Chinese participants. Participants self-reported their sexual orientation and gender. Of the 301 participants, 11% were lesbian, 56.1% were gay, 20.9% were bisexual, 6.6% were questioning, 1.3% were queer, 2.3% were asexual, and 1.7% were others. As for gender, 66.11% of them were males, 25.91% were females, 0.7% were transgender males, 4% were transgender females, 2.7% were queers, 0.3% were gender non-conforming, 0.3% were others.
Procedures
The current study adopted a cross-sectional design. Using convenient sampling method, data were collected from the social network application WeChat in the form of an online survey. Specifically, a peer leader from a national wide sexual minority group assisted to conduct data-push in his social network. Data collection started in July 2019 and lasted for 2 weeks. Participants whose age were 18 years old or above, who self-identified as sexual minority, and who were currently in China were included in the study. The survey took about 30–40 min to complete. After completion with quality check, participants were remunerated 15 Chinese yuan (approximately 2 US dollars) for their efforts.
The participants were from 29 provinces among the 34 provinces in China. A total of 450 participants completed the survey. Among them, 149 were excluded due to their ineligibility to the study. Specifically, 71 participants were excluded because their answering time was shorter than 13 min, which was the minimum reasonable time to complete the survey estimated by the research team; two participants were excluded for currently residing outside China. In addition, 65 participants failed to correctly answer attention check questions. Five participants were below 18 years old. Lastly, six participants were excluded because they self-identified as heterosexual and cisgender, thus not fitting the eligibility criteria. In total, 301 LGBTQ individuals were included for final analysis in this study. The institutional review board of Peking University approved the study procedures.
Measures
Sexual Minority Stigma
Sexual minority stigma was measured with a 20-item scale (Thaker et al., 2018) to identify how much one was stigmatized because of his or her identity during the past 3 months. Responses were rated on a 4-point scale ranging from “very often” (1) to “not at all” (4). The scale was composed of five subscales: experienced or enacted stigma (e.g., “how often have you been abused by doctors and nurses?”), HIV-related vicarious stigma (e.g., “how often do you think people with sexual minority identity are blamed for HIV/AIDS in society?”), self-stigma (e.g., “how often have you felt confused about your gender roles?”), media portrayal stigma (e.g., “how often have you been made fun or been called names by general public on streets and buses?”), and felt normative stigma (e.g., “how often do you think people with sexual minority identity feel pressured by their family members to get married to a woman, although they would prefer to be in a relationship with other genders?”). The responses to all items in the scale were added up to form an index score of overall stigma. Higher total scores indicated higher levels of stigma. The Chinese scale was developed via translation and back translation method. Cronbach’s α was .83 in this study.
Resilience
Resilience of LGBT individuals was assessed with the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) (Campbell-Sills & Stein, 2007). It measured how well one could bounce back from adversity. One sample item was “I am able to adapt when changes occur.” Items were rated on a 5-point scale ranging from 0 strongly disagree to 4 strongly agree. Scores of 10 items were summed to form a total score which ranged from 0 to 40. Higher scores indicated higher levels of resilience. The scale has showed good reliability and validity in previous studies (Kang et al., 2018; Yu et al., 2011). The scale was proven to be applicable for Chinese population (Wang et al., 2010) as well. The Cronbach’s α was .92 in the study.
Family Support
Family support was measured with four items from Multidimensional Scale of Perceived Social Support (MSPSS) (Canty-Mitchell & Zimet, 2000). The original scale had three subscales to measure support from family, friends, and significant others. The 4-item family support subscale was used in this study. The family subscale evaluated how well one was supported by the family. One sample item was “My family really tries to help me.” Items were rated on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree). Higher scores indicated higher levels of family support. A previous study which administered MSPSS in Chinese patients with methadone treatment showed that the scale was reliable (Cronbach’s α = .92) (Zhou et al., 2015). The Chinese scale underwent the translation and back translation process. The Cronbach’s α was .92 in the present study.
Depression
Depression was measured by Patient Health Questionnaire (PHQ-9) (Spitzer et al., 1999). One sample item was “feeling down, depressed, or hopeless.” Participants rated on a 4-point scale from 0 (strongly disagree) to 3 (strongly agree). The total score ranged from 0 to 27. In the preliminary analysis, the total score of PHQ-9 was dichotomized into 0 (< 10) or 1 (≥ 10). The threshold of 10 was used in current study as an existing literature suggested that 10 could be a cutting off value to indicate moderate depression (Kroenke et al., 2001). Furthermore, the average score of depression is 10.17 in this study. Therefore, we used 10 as a threshold to separate participants into two groups: less than moderately depressed and more than moderately depressed. The scale demonstrated good validity in previous studies (Yu et al., 2012; Zhang et al., 2013). The scale was applicable to Chinese general population as well with a Cronbach’s α of .86 (Wang et al., 2014). Higher scores indicated higher levels of depression. The Cronbach’s α for this sample was .91.
Data Analysis
First, t test and χ2 test were performed to examine the differences of demographic variables between participants who reported less than moderate depression and more than moderate depression. In order to perform chi-square test (each cell must have more than five counts), sexual orientation was grouped into four categories: lesbian, gay, bisexual, and others (containing “questioning”, “queer”, “asexual”, and “others”). Gender was grouped into three categories: female, male, and others (containing “transgender female”, “transgender male”, “queer”, “gender-nonconforming”, and “others”). Age, ethnicity, and monthly family income were significantly different between the two groups and thus were controlled in the following path analysis. Second, bivariate correlations were calculated among stigma, resilience, family support, depression, and other relevant variables. Finally, path analysis was conducted with PROCESS macro (Hayes, 2013), providing path coefficient estimates (β) and bootstrapped 95% confidence intervals (95% CI) for indirect effects based on 5000 bootstrapping resamples. The model composed of both resilience and family support as multiple mediators to test for pathways leading to depression precisely and parsimoniously (Preacher & Hayes, 2008). The bootstrapping method was thus adopted to test for multiple mediation among other statistical methods as it was more powerful and suitable (Preacher & Hayes, 2008). The sample size of 301 individuals was considered adequate for six of the most common and most recommended tests for mediation, when examining various parameters (Fritz & MacKinnon, 2007). There were no missing data in the sample. All statistical analyses were performed using SPSS 24.0. A p value of less than 0.05 was employed to indicate statistical significance.
Results
Sample Characteristics
As shown in Table 1, the range of age of participants (N = 301) was 18 to 42 years old (M = 24.15, SD = 4.55). Most participants were male (66.11%) and of Han ethnicity (94.68%). The rates of unemployment, part-time job, and full-time job were 48.84%, 5.32%, and 45.85%, respectively. Most of the participants were students (44.19%) and of a bachelor’s degree (64.78%). About one-third (29.57%) of participants had monthly family income of 5000-9999 Chinese Yuan (approximately 711–1423 US dollars). Regarding their sexual orientation, 169 (56.15%) participants were gay; 63 (20.93%) were bisexual; and 33 (10.96%) were lesbian. A total of 29 provinces were covered in this study. The top three data sources were from Guangdong 59(19.60%), Beijing 58(19.27%), and Shanghai 21(6.98%). Overall, the sample consisted of young LGBT individuals with high level of education from major cities or provinces of China.
Group Differences by Depression
More than half of the participants (n = 172, 57.14%) reported less than moderate depressive symptoms, while the others (n = 129, 42.86%) reported more than moderate depression. Table 1 presents the differences of key characteristics between participants who scored moderate and less moderate depression. Most of the variables (e.g., religion, education, work status, occupation, being a single child, gender) did not significantly differ between two groups (all ps > .05). Conversely, significant differences were found among age t(299) = 2.68, p = .008. The more than moderately depressed group was more likely to be older. Ethnicity was significantly different between two groups as well χ2 (1, N = 301) = 4.63, p = .03. Participants who were less than moderately depressed were more likely to be Han. Gender was also significantly different between two groups, χ2 (2, N = 301) = 6.43, p = .04. More females were more than moderately depressed. Lastly, monthly family income was significantly different between two groups χ2 (8, N = 301) = 21.63, p = .007 with lower monthly family income in less than moderately depressed group.
Associations Among Main Study Variables
As presented in Table 2, stigma was negatively associated with resilience (r = −.24, p < .001) and family support (r = −.22, p < .001) and was positively associated with depression (r = .37, p < 0.001). Resilience had a positive relationship with family support (r = .43, p < .001) and a negative relationship with depression (r = −.52, p < .001). Family support was negatively associated with depression (r = −.35, p < .001). Depression had a negative association with family income (r = −.17, p = .004). Ethnicity was positively associated with family income (r = .13, p =.023). Lastly, age was positively associated with family income (r = .12, p = .035) and negatively associated with depression (r = −.16, p = .005). We tested for multicollinearity by variance inflation factor (VIF). The VIF of sexual minority stigma, resilience, and family support were 1.09, 1.32, and 1.26, respectively, suggesting a low possibility of multicollinearity.
Path Analysis
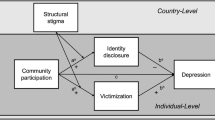
Potentially confounding variables that were significantly associated with depression were controlled in the model as covariates, including age, ethnicity, and monthly family income. The results of multiple mediation model are presented in Fig. 1. The model explained 12.44% variances in resilience, 9.63% variances in family support, and 36.31% variances in depression. As shown in Table 3, the multiple mediation analysis shown that the direct effect of stigma on depression was significant (β = 0.17, 95% CI [0.10, 0.24]). The indirect effects of stigma on depression via resilience (β = 0.06, 95% CI [0.02, 0.10]) and family support (β = 0.02, 95% CI [0.002, 0.05]) were also significant. Therefore, resilience significantly mediated the relation between sexual minority stigma and depression. Family support significantly mediated the effect of sexual minority stigma on depression as well.

Path analysis model for resilience and family support as multiple mediators of the relationship between sexual minority stigma and depression. Potential confounding variables that were significantly associated with depression were controlled in the model as covariates, including age, ethnicity, and monthly family income. Correlations between covariates and depression have been omitted for reasons of presentation simplicity. The solid line indicates significant coefficients
Discussion
The study examined the negative impact of sexual minority stigma and its potential pathways to depression among LGBTQ individuals in China. The study incorporated both intrapersonal level process, i.e., resilience, and interpersonal level process, i.e. family support as the mediating processes. Results confirmed that greater sexual minority stigma was associated with more severe depressive symptoms. In addition, both resilience and family support significantly mediated the relation between sexual minority stigma and depressive symptoms.
Consistent with the minority stress theory (Meyer, 2003) and previous findings, the results demonstrated that sexual minority stigma was positively associated with depression (Lewis et al., 2003; Logie et al., 2012). Given the representativeness of the sample, the results were likely to be applicable to the Chinese population. The results remarkably reflected that Chinese sexual minorities experienced stigma at multiple levels, from individual, interpersonal to structural (White Hughto et al., 2015). These experiences of stigma impacted not only their mental health, which was corroborated in the present study, but also their physical health (Lick et al., 2013). Thus, relative to their heterosexual peers, sexual minorities suffered physical and mental health disparities. The next step in research is to implement prospective research design to track sexual minorities to examine their experiences of stigma and the trajectories of change of their physical, mental, and sexual health.
In addition, resilience and family support were negatively associated with depression. The finding was consistent with those from previous studies (King & Richardson, 2017; Scandurra et al., 2017). Resilient individuals had adaptive resources to enact effective strategies to maintain their mental health. Individuals with more family support experienced less severe depressive symptoms.
Indirect Effects of Resilience and Family Support
As hypothesized, both resilience and family support constituted the mediating processes through which sexual minority stigma led to depression, which supported previous findings (Logie et al., 2020; Yan et al., 2019). Sexual minority stigma was negatively associated with resilience, which was negatively associated with depression. The findings could be explained in light of the psychological mediation framework. At an intrapersonal level, stigma eroded resilience and consequently intensified depressive symptoms. Resilience could be reflected from one’s flexible and adaptive coping strategies. Persistent and overwhelmingly distressing stigma might induce intense negative emotions that compromised one’s adaptive coping strategies. Sexual minorities might turn to maladaptive coping strategies to manage their distress. A study in Chinese gay and bisexual men showed that maladaptive coping mediated HIV stigma and mental health (Chan & Mak, 2019). These maladaptive coping strategies, albeit useful in the short term, might undermine their resilience towards sexual minority in the long term.
In an interpersonal process, family support mediated sexual minority stigma and depression. Revealing sexual orientations to others might not always be beneficial to one’s family relationships and mental health. For instance, coming out to siblings was associated with less internalized stigma in Italy gay men (Salvati et al., 2018). This was in stark contrast to the Chinese context in which sexual minority identity always provoked conflict against Chinese traditional family values (Hu et al., 2013; Lin et al., 2016). Confucianism emphasized filial piety, a reciprocal and authoritarian relationship between parents and children (Yeh & Bedford, 2003). Parents felt they were responsible of taking care of their children who were obliged to care for their parents in return when they grew up. Sexual minorities, under the pressure of filial piety, bore the burden of failing the family expectations of heterosexual marriage and having children. For instance, gay and bisexual men reported their primary source of pressure were showing filial piety and maintaining the family lineage (Kwok & Wu, 2015). Failure to fulfill family expectations was perceived as rebellious, ungrateful, and shameless. Sexual minorities with intense stigma might be alienated from their families. Meanwhile, they might be reluctant to seek support from families which was in fact the exact source of distress. Therefore, sexual minority stigma led to rejection from families, as well as a lower likelihood to seek family support to avoid further rejection and exclusion from families. The reduced family support resulted in elevated risk for psychopathology.
As demonstrated in the findings, intrapersonal and interpersonal processes served distinctive but interrelated mechanisms through which sexual minority stigma conferred adverse mental health outcomes. Future prospective studies should explore the bidirectional effects between these processes to explicate the intertwined mechanisms contributing to psychopathology. Future studies should also take into account how these mediators account for the impact of sexual stigma on other domains of health of sexual minorities within the Chinese context.
Implications
This study is of special relevance to healthcare professionals who provide services for sexual minorities. The results implied that sexual minorities became more vulnerable for poor mental health via lower resilience and lower family support. Sexual minorities represent a target population which warrants additional mental health support and more intensive intervention. Clinicians should be aware of emotional distress arose from sexual orientation when they provide healthcare in clinical settings. Besides, clinicians working with sexual minorities can educate sexual minorities how stigma influences sexual minority mental health outcomes. Being informed about the processes empowers and mobilizes them to adopt more adaptive coping strategies. Both resilience and family support could be potential targets of empirically based interventions to improve mental health among sexual minorities. From a strength-based perspective, recent literature argued that resilience can be built up to counteract the burden of stigma (Joyce et al., 2018). When working with LGBT clients, focusing on enhancing their resilience, or the ability to withstand adversity and maintain emotional equilibrium, can be a promising approach to ameliorate negative impacts of stigma. A growing number of resilience interventions, in the form of cognitive behavioral therapy (CBT), mindfulness-based interventions, or mixed interventions, were tested for their effectiveness in improving resilience and decreasing depressive symptoms (Joyce et al., 2018; Stallard & Buck, 2013; Steinhardt & Dolbier, 2008). A recent brief CBT intervention for recently gay and bisexual men in China successfully promoted resilience and reduced depressive symptoms (Yang et al., 2018), though with a relatively sample. It suggests that similar interventions may be useful for the broader Chinese sexual minority community to enhance resilience and reduce depression.
Meanwhile, interventions may cultivate families’ knowledge towards sexual minority stigma, encourage their understanding and acceptance of sexual minorities, strengthen their support to sexual minorities, and eventually improve the well-being of sexual minorities. Research on the interventions which served the LGBT youth in the context of family found that these interventions not only helped LGBT youth but also facilitated families to support their LGBT children (Ryan, 2010). While future interventions target on sexual minorities to guide them dealing with family rejection, family members can benefit from interventions to learn to provide support for LGBTQ family members. Stigma-reduction interventions targeting at families of sexual minorities are potentially useful to increase their given support as well. Future interventions should take a culturally informed combination approach which takes into account both intrapersonal level factors (e.g. resilience) and interpersonal level factors (e.g. family support).
The results of the present study led to some implications for policy makers. The Healthy China 2030 agenda prioritized health throughout the process of public policy implementation (Tan et al., 2017). The health of sexual minorities and their experiences of health disparities should be paid more attention as well. Policy makers should enact strategies and policies to foster an anti-stigma and more inclusive environment for sexual minorities. Meanwhile, community leaders, activists, and organizers should initiate and carry out inclusive social campaigns to address LGBQA stigma and raise public awareness. A structural level of change paves the way to successful interventions and long-lasting improvements in the well-being of sexual minorities.
Strengths and Limitations
The present study had its strengths. The study recruited participants national wide, covering 29 provinces out of 34 provinces of China. Aside from a wide range of regions, the sample consisted of diverse sexual orientations, including lesbian, gay, bisexual, question, queer, transgender, and gender non-conforming individuals. The study had several limitations. First, the study adopted a cross-sectional design. As such, causation could not be inferred. Longitudinal studies are needed to replicate current findings. Second, depressive symptoms were assessed by self-report measures which might cause self-report bias. Future studies should use more objective methods to assess depression, such as diagnoses by clinical psychiatrists. Third, both resilience and family support were measured by scales developed for general population. Future studies may use specific scales tapped on psychological resources for sexual minorities. Last, the sample was consisted of mostly gay, Han ethnic, young, and educated participants from major cities. Future studies of larger samples may be used to replicate the findings.
The study extended the understanding of the relationship among stigma, resilience, family support, and depression. The results highlighted the burden of sexual minority stigma on the mental health of sexual minorities in China. The findings indicated that sexual minority stigma positively impacted depression via lower resilience and lower family support. These factors are critical to future interventions with a goal of improving mental health of Chinese sexual minorities and a vision of healthy China.
References
Campbell-Sills, L., & Stein, M. B. (2007). Psychometric analysis and refinement of the Connor–Davidson resilience scale (CD-RISC): Validation of a 10-item measure of resilience. Journal of Traumatic Stress, 20(6), 1019–1028. https://doi.org/10.1002/jts.20271
Canty-Mitchell, J., & Zimet, G. D. (2000). Psychometric properties of the Multidimensional Scale of Perceived Social Support in urban adolescents. American Journal of Community Psychology, 28(3), 391–400. https://doi.org/10.1023/A:1005109522457
Chan, R. C. H., & Mak, W. W. S. (2019). Cognitive, regulatory, and interpersonal mechanisms of HIV stigma on the mental and social health of men who have sex with men living with HIV. American Journal of Men’s Health, 13(5), 1557988319873778–1557988319873778. https://doi.org/10.1177/1557988319873778
Choi, K. H., Steward, W. T., Miège, P., Hudes, E., & Gregorich, S. E. (2016). Sexual stigma, coping styles, and psychological distress: A longitudinal study of men who have sex with men in Beijing China. Archives of Sexual Behavior, 45(6), 1483–1491. https://doi.org/10.1007/s10508-015-0640-z.
Fergusson, D. M., Horwood, L. J., Ridder, E. M., & Beautrais, A. L. (2005). Sexual orientation and mental health in a birth cohort of young adults. Psychological Medicine, 35(7), 971–981. https://doi.org/10.1017/S0033291704004222
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Grant, K. E., Compas, B. E., Stuhlmacher, A. F., Thurm, A. E., McMahon, S. D., & Halpert, J. A. (2003). Stressors and child and adolescent psychopathology: Moving from markers to mechanisms of risk. Psychological Bulletin, 129(3), 447–466. https://doi.org/10.1037/0033-2909.129.3.447
Hatzenbuehler, M. L. (2009). How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychological Bulletin, 135(5), 707–730. https://doi.org/10.1037/a0016441
Hayes, A. F. (2013). Methodology in the social sciences.Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Press.
Hu, X., Wang, Y., & Wu, C. H. (2013). Acceptance concern and life satisfaction for Chinese LGBs: The mediating role of self-concealment. Social Indicators Research, 114(2), 687–701. https://doi.org/10.1007/s11205-012-0168-8.
Joyce, S., Shand, F., Tighe, J., Laurent, S. J., Bryant, R. A., & Harvey, S. B. (2018). Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open, 8(6), e017858. https://doi.org/10.1136/bmjopen-2017-017858
Kang, X., Fang, Y., Li, S., Liu, Y., Zhao, D., Feng, X., & Li, P. (2018). The benefits of indirect exposure to trauma: The relationships among vicarious posttraumatic growth, social support, and resilience in ambulance personnel in China. Psychiatry Investigation, 15(5), 452–459. https://doi.org/10.30773/pi.2017.11.08.1
King, S. D., & Richardson, V. E. (2017). Mental health for older LGBT Adults. Annual Review of Gerontology and Geriatrics, 37(1), 59–75.
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Kwok, D. K., & Wu, J. (2015). Chinese attitudes towards sexual minorities in Hong Kong: Implications for mental health. International Review of Psychiatry, 27(5), 444–454. https://doi.org/10.3109/09540261.2015.1083950
Lewis, R. J., Derlega, V. J., Griffin, J. L., & Krowinski, A. C. (2003). Stressors for gay men and lesbians: Life stress, gay-related stress stigma consciousness, and depressive symptoms. Journal of Social and Clinical Psychology, 22(6), 716–729. https://doi.org/10.1521/jscp.22.6.716.22932
Lick, D. J., Durso, L. E., & Johnson, K. L. (2013). Minority stress and physical health among sexual minorities. Perspectives on Psychological Science, 8(5), 521–548.
Lin, K., Button, D. M., Su, M., & Chen, S. (2016). Chinese college students’ attitudes toward homosexuality: Exploring the effects of traditional culture and modernizing factors. Sexuality Research and Social Policy, 13(2), 158–172. https://doi.org/10.1007/s13178-016-0223-3
Liu, Y., Jiang, C., Li, S., Gu, Y., Zhou, Y., An, X., & Pan, G. (2018). Association of recent gay-related stressful events with depressive symptoms in Chinese men who have sex with men. BMC Psychiatry, 18(1), 217–217. https://doi.org/10.1186/s12888-018-1787-7
Logie, C. H., Lacombe-Duncan, A., Wang, Y., Levermore, K., Jones, N., Ellis, T., & Grace, D. (2020). Adapting the psychological mediation framework for cisgender and transgender sexual minorities in Jamaica: Implications from latent versus observed variable approaches to sexual stigma. Social Science & Medicine, 245, 112663. https://doi.org/10.1016/j.socscimed.2019.112663
Logie, C. H., Newman, P. A., Chakrapani, V., & Shunmugam, M. (2012). Adapting the minority stress model: Associations between gender non-conformity stigma, HIV-related stigma and depression among men who have sex with men in South India. Social Science & Medicine, 74(8), 1261–1268. https://doi.org/10.1016/j.socscimed.2012.01.008
Lucassen, M. F., Stasiak, K., Samra, R., Frampton, C. M., & Merry, S. N. (2017). Sexual minority youth and depressive symptoms or depressive disorder: A systematic review and meta-analysis of population-based studies. Australian and New Zealand Journal of Psychiatry, 51(8), 774–787. https://doi.org/10.1177/0004867417713664
Masten, A. S. (2007). Resilience in developing systems: Progress and promise as the fourth wave rises. Development and Psychopathology, 19(3), 921–930. https://doi.org/10.1017/S0954579407000442
McConnell, E. A., Janulis, P., Phillips, G., II., Truong, R., & Birkett, M. (2018). Multiple minority stress and LGBT community resilience among sexual minority men. Psychology of Sexual Orientation and Gender Diversity, 5(1), 1.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
Meyer, I. H. (2015). Resilience in the study of minority stress and health of sexual and gender minorities. Psychology of Sexual Orientation and Gender Diversity, 2(3), 209–213. https://doi.org/10.1037/sgd0000132
Pan, X., Li, R., Ma, Q., Wang, H., Jiang, T., He, L., . . . Xia, S. (2018). Sexual risk behaviour, sexual victimisation, substance use and other factors related to depression in men who have sex with men in Wenzhou, China: A cross-sectional study. BMJ Open, 8(4), bmjopen-2016-013512. https://doi.org/10.1136/bmjopen-2016-013512
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891.
Ryan, C. (2010). Engaging families to support lesbian, gay, bisexual, and transgender youth: The family acceptance project. Prevention Researcher, 17(4), 11.
Ryan, C., Russell, S. T., Huebner, D., Diaz, R., & Sanchez, J. (2010). Family acceptance in adolescence and the health of LGBT young adults. Journal of Child and Adolescent Psychiatric Nursing, 23(4), 205–213. https://doi.org/10.1111/j.1744-6171.2010.00246.x
Salvati, M., Pistella, J., Ioverno, S., Laghi, F., & Baiocco, R. (2018). Coming out to siblings and internalized sexual stigma: The moderating role of gender in a sample of Italian participants. Journal of GLBT Family Studies, 14(5), 405–424. https://doi.org/10.1080/1550428X.2017.1369916
Sandfort, T. G. M., Bakker, F., Schellevis, F. G., & Vanwesenbeeck, I. (2006). Sexual orientation and mental and physical health status: Findings from a Dutch population survey. American Journal of Public Health, 96(6), 1119–1125. https://doi.org/10.2105/AJPH.2004.058891
Scandurra C, Amodeo AL, Valerio P, Bochicchio V, Frost DM. (2017). Minority stress, resilience, and mental health: a study of Italian transgender people. Journal of Socical Issues, 73(3), 563–85.
Shao, J., Chang, E. S., & Chen, C. (2018). The relative importance of parent-child dynamics and minority stress on the psychological adjustment of LGBs in China. Journal of Counseling Psychology, 65(5), 598–604. https://doi.org/10.1037/cou0000281
Snapp, S. D., Watson, R. J., Russell, S. T., Diaz, R. M., & Ryan, C. (2015). Social support networks for LGBT young adults: Low cost strategies for positive adjustment. Family Relations, 64(3), 420–430. https://doi.org/10.1111/fare.12124
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Group, a. t. P. H. Q. P. C. S. (1999). Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary care evaluation of mental disorders. Patient Health Questionnaire. Journal of the American Medical Association, 282(18), 1737-1744. https://doi.org/10.1001/jama.282.18.1737
Stallard, P., & Buck, R. (2013). Preventing depression and promoting resilience: Feasibility study of a school-based cognitive-behavioural intervention. British Journal of Psychiatry, 202(54), s18–s23. https://doi.org/10.1192/bjp.bp.112.119172
Steinhardt, M., & Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. Journal of American College Health, 56(4), 445–453. https://doi.org/10.3200/JACH.56.44.445-454
Su, X., Zhou, A. N., Li, J., Shi, L.-E., Huan, X., Yan, H., & Wei, C. (2018). Depression, loneliness, and sexual risk-taking among HIV-negative/unknown men who have sex with men in China. Archives of Sexual Behavior, 47(7), 1959–1968. https://doi.org/10.1007/s10508-017-1061-y
Tan, X., Liu, X., & Shao, H. (2017). Healthy China 2030: A vision for health care. Value in Health Regional Issues, 12, 112.
Thaker, J., Dutta, M., Nair, V., & Rao, V. P. (2018). The interplay between stigma, collective efficacy, and advocacy communication among men who have sex with men and transgender females. Journal of Health Communication, 23(7), 614–623. https://doi.org/10.1080/10810730.2018.1499833
Wang, L., Shi, Z., Zhang, Y., & Zhang, Z. (2010). Psychometric properties of the 10-item Connor-Davidson Resilience Scale in Chinese earthquake victims. Psychiatry and Clinical Neurosciences, 64(5), 499–504. https://doi.org/10.1111/j.1440-1819.2010.02130.x
Wang, W., Bian, Q., Zhao, Y., Li, X., Wang, W., Du, J., & Zhao, M. (2014). Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. General Hospital Psychiatry, 36(5), 539–544. https://doi.org/10.1016/j.genhosppsych.2014.05.021
Wang, Y., Hu, Z., Peng, K., Xin, Y., Yang, Y., Drescher, J., & Chen, R. (2019). Discrimination against LGBT populations in China. The Lancet Public Health, 4(9), e440–e441. https://doi.org/10.1016/S2468-2667(19)30153-7
Wei, C., & Liu, W. (2019). Coming out in Mainland China: A national survey of LGBTQ students. Journal of LGBT Youth, 16(2), 192–219. https://doi.org/10.1080/19361653.2019.1565795
White Hughto, J. M., Reisner, S. L., & Pachankis, J. E. (2015). Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions. Social Science & Medicine, 1982(147), 222–231. https://doi.org/10.1016/j.socscimed.2015.11.010
Xu, W., Zheng, L., Xu, Y., & Zheng, Y. (2017). Internalized homophobia, mental health, sexual behaviors, and outness of gay/bisexual men from Southwest China. International Journal for Equity in Health, 16(1), 36. https://doi.org/10.1186/s12939-017-0530-1
Yan, H., Li, X., Li, J., Wang, W., Yang, Y., Yao, X., & Li, S. (2019). Association between perceived HIV stigma, social support, resilience, self-esteem, and depressive symptoms among HIV-positive men who have sex with men (MSM) in Nanjing China. AIDS Care, 31(9), 1069–1076. https://doi.org/10.1080/09540121.2019.1601677
Yang, J. P., Simoni, J. M., Dorsey, S., Lin, Z., Sun, M., Bao, M., & Lu, H. (2018). Reducing distress and promoting resilience: a preliminary trial of a CBT skills intervention among recently HIV-diagnosed MSM in China. AIDS Care, 30(sup5), S39-s48. https://doi.org/10.1080/09540121.2018.1497768
Yeh, K.-H., & Bedford, O. (2003). A test of the dual filial piety model. Asian Journal of Social Psychology, 6(3), 215–228. https://doi.org/10.1046/j.1467-839X.2003.00122.x
Yu, X., Lau, J. T. F., Mak, W. W. S., Zhang, J., & Lui, W. W. S. (2011). Factor structure and psychometric properties of the Connor-Davidson Resilience Scale among Chinese adolescents. Comprehensive Psychiatry, 52(2), 218–224. https://doi.org/10.1016/j.comppsych.2010.05.010
Yu, X., Tam, W. W. S., Wong, P. T. K., Lam, T. H., & Stewart, S. M. (2012). The Patient Health Questionnaire-9 for measuring depressive symptoms among the general population in Hong Kong. Comprehensive Psychiatry, 53(1), 95–102. https://doi.org/10.1016/j.comppsych.2010.11.002
Zhang, Y. L., Liang, W., Chen, Z. M., Zhang, H. M., Zhang, J. H., Weng, X. Q., & Zhang, Y. L. (2013). Validity and reliability of Patient Health Questionnaire-9 and Patient Health Questionnaire-2 to screen for depression among college students in China. Asia-Pacific Psychiatry, 5(4), 268–275. https://doi.org/10.1111/appy.12103
Zheng, L., Hart, T. A., Noor, S. W., & Wen, G. (2020). Stressors based on sexual orientation and mental health among lesbian, gay, and bisexual individuals in China: Minority stress and perceived pressure to get married. Archives of Sexual Behavior, 49(5), 1769–1782. https://doi.org/10.1007/s10508-020-01693-z
Zhou, K., Li, H., Wei, X., Yin, J., Liang, P., Zhang, H., & Zhuang, G. (2015). Reliability and validity of the multidimensional scale of perceived social support in Chinese mainland patients with methadone maintenance treatment. Comprehensive Psychiatry, 60, 182–188. https://doi.org/10.1016/j.comppsych.2015.03.007
Funding
The study was supported by PKU startup grant for new faculty to GYZ.
Author information
Authors and Affiliations
Contributions
GYZ designed and executed the study. YXW and CKL analyzed the data and wrote a first draft of the paper. GYZ helped rewrite the manuscript. QW co-designed the study and provided feedback for the paper.
Corresponding author
Ethics declarations
Ethics Approval
The research protocol was approved by Institutional Review Board at Peking University. The study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki.
Informed Consent
All participants gave their informed consent before participating in the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, Y., Lao, C.K., Wang, Q. et al. The Impact of Sexual Minority Stigma on Depression: the Roles of Resilience and Family Support. Sex Res Soc Policy 19, 442–452 (2022). https://doi.org/10.1007/s13178-021-00558-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13178-021-00558-x