
Abstract
Depression is a major public health problem in the Russian Federation and is particularly of concern for men who have sex with men (MSM). MSM living in Moscow City were recruited via respondent-driven sampling and participated in a cross-sectional survey from October 2010 to April 2013. Multiple logistic regression models compared the relationship between sexual identity, recent stigma, and probable depression, defined as a score of ≥23 on the Center for Epidemiological Studies Depression scale. We investigated the interactive effect of stigma and participation in the study after the passage of multiple “anti-gay propaganda laws” in Russian provinces, municipalities, and in neighboring Ukraine on depression among MSM. Among 1367 MSM, 36.7% (n = 505) qualified as probably depressed. Fifty-five percent identified as homosexual (n = 741) and 42.9% identified as bisexual (n = 578). Bisexual identity had a protective association against probable depression (reference: homosexual identity AOR 0.71; 95%CI 0.52–0.97; p < 0.01). Those who experienced recent stigma (last 12 months) were more likely to report probable depression (reference: no stigma; AOR 1.75; 95%CI 1.20–2.56; p < 0.01). The interaction between stigma and the propaganda laws was significant. Among participants with stigma, probable depression increased 1.67-fold after the passage of the anti-gay laws AOR 1.67; 95%CI 1.04–2.68; p < 0.01). Depressive symptoms are common among MSM in Russia and exacerbated by stigma and laws that deny homosexual identities. Repeal of Russia’s federal anti-gay propaganda law is urgent but other social interventions may address depression and stigma in the current context.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Depression and other mental health disorders represent a large proportion of the global burden of disease and are the second leading cause of global disability [1, 2]. In the Russian Federation, this trend is consistent, if not magnified, among men. Here, the prevalence of depressive symptoms in men residing in urban areas has been reported as high as 23% in 1999–2000, as defined by a score of ≥16 on the Center for Epidemiological Studies Depression (CES-D) scale [3]. As of 2011, the suicide rate among Russian men was estimated at 35.1 per 100,000 persons—one of the highest in the world. [4] Global reports suggest that men who have sex with men (MSM) often have higher prevalence of depression than heterosexual men [5], and the little research that has been conducted in Russia on the topic suggests that such patterns may persist among MSM [6]. Analysis of HIV-infected MSM found that over one-third have reported symptomology indicative of probable depression and more than half of MSM in Moscow have reported hazardous or harmful levels of alcohol abuse that may be related to depression [7].
Across settings, research among MSM has shown that homophobia and social stigma may contribute to depression [8]. While less is known from the Russian Federation, research from similar epidemiologic settings in Central Asia has provided some insight, demonstrating that even where homosexuality has been decriminalized, stigmatization of homosexuality persists [9], and MSM who regularly practice the receptive role during anal intercourse experience increased levels of stigma [10]. Social stigma in Central Asia has been associated with reduced access to health and social services among MSM [9, 11], including key HIV prevention and treatment services [9]. Depressive symptoms among MSM in Central Asia has been explained in part by high prevalence of community-level stigma [9]. Research from other countries with similar contexts in which homosexuality is decriminalized but where there is no legal protection for MSM against discrimination [12] have demonstrated the association between increased levels of perceived and experienced stigma and depression among MSM [13, 14] and inconsistent use of condoms and depression among MSM [15]. Social support [16] and social cohesion [13] within the MSM community, however, appear to have a protective effect against depression among MSM in these countries.
Recent events within Russia provide context and rationale for understanding the factors associated with poor mental health outcomes among MSM. In June 2013, the Russian government issued the “anti-gay propaganda law,” a national ban on “propaganda for non-traditional sexual relations” that criminalized the sharing of information related to same sex practices. The law effectively legitimized public stigma and violence against lesbian, gay, bisexual, and transgender people (LGBT) in Russia [17, 18]. This came on the heels of similar laws in the City of St. Petersburg (March 2012) that would fine individuals up to 500,000 rubles (approximately $17,000 USD) for spreading “homosexual propaganda,” as well as other related legislation in multiple oblasts (administrative divisions) across the Russian Federation, and a widely praised draft law in neighboring Ukraine (October 2012) that would impose up to 5 years imprisonment for spreading “propaganda of homosexuality [19].” While Russia’s national anti-gay propaganda law was not passed until 2013, the St. Petersburg, other provincial laws, and Ukraine bill (subsequently revoked in 2015 after the conclusion of this study) [20] received heavy media attention at the time, prompted considerable political and social discussion around the acceptance of homosexuality in Russia, and built substantial support for a possible federal law in Russia. Subsequently, a poll conducted by the Pew Research Center in 2013 found that nearly three in four Russians believed that society should not accept homosexuality [21]. Political analysts have since suggested that Russian President Vladimir Putin’s stance that homosexuality is a threat to Russian society [17] is part of a political narrative that deliberately links non-traditional sexualities to an imperialistic West [18]. Given related literature [22] and current events in Russia, this research sought to assess the level of depression among MSM in Moscow, Russia, explore the relationship between sexual identity and depressive symptoms among MSM in Russia, and explore the role of environmental changes in acceptance of homosexuality in the Russian Federation as it relates to depression.
Methods
The data for this analysis was gathered through a cross-sectional, NIH-funded study conducted in Moscow, Russia, between October 2010 and April 2013. The research was a collaborative effort conducted jointly by Johns Hopkins University and AIDS Infoshare, a local non-governmental organization that provides anonymous HIV testing and counseling and STI screening and treatment in an LGBT-friendly context in Moscow. All sampling, data collection, and biologic testing methods have been previously described [7, 23].
Participants
Inclusion criteria required participants to be fluent in Russian, assigned male at birth, aged 18 years or older, currently reside in Moscow, report anal sex with a man in the past 12 months, and provide verbal informed consent. Participants were recruited via respondent-driven sampling (RDS), a chain recruitment method that is used to reach hidden or hard-to-reach populations [24]. Participants were provided 1000 rubles (approximately $40 USD) as reimbursement for their participation in the study and 500 rubles ($20 USD) for each peer recruited into the study. Thirty-one waves of recruitment produced a sample of 1367 participants for the analysis [23].
Measures
Informed by formative research [25], cognitive testing [26], and pilot testing methods, the structured survey was designed to gather information on sociodemographic characteristics, sexual practices and identity, substance use, experienced and perceived stigma, and mental health symptoms. Depression symptoms were the outcome of interest and sexual identity, stigma, and other known correlates [13, 15, 27–30] of depression were covariates of interest for this analysis. Measures of sexual identity and practices were adapted from the US CDC’s National Health Behavior Survey [31] and included questions about sexual identity (“heterosexual,” “homosexual,” “bisexual,” or “other”) and about the sex of the respondent’s sexual partners in the last 12 months (male or female).
The CES-D scale [32] was used as a screening tool for current (past 7 days) depressive symptomology (Cronbach’s α 0.889). The CES-D score was stratified into three categories: “unlikely to be depressed” (CES-D <16), “possibly depressed” (CES-D 16–22), and “probably depressed” (CES-D ≥23) [32]. Given that 36.7% endorsed a score of probably depressed (n = 505) and 11% of the sample scored in the possibly depressed range (n = 121), coupled with our interest in understanding the factors that were correlated with greater probability of depression [33], scores were transformed to a binary variable: “unlikely or possibly depressed” (CES-D <23) and probably depressed (CES-D ≥23).
A five-item scale was used to identify recent (last 12 months) experienced stigma (Cronbach’s α 0.713). This was a subscale of a larger stigma scale that had been developed from qualitative research [25], underwent cognitive testing [26] among MSM participants for further refinement, and were reviewed by MSM participants to assess face validity. The experienced stigma subscale included experience of public mocking, poor treatment by family members, experience of physical assault, being forced to move accommodation, and experiencing poor treatment within healthcare facilities due to sexual preferences. A positive indication for any one of these five variables was defined as a recent experience of stigma. The alcohol use disorders identification test (AUDIT), a validated scale in Russia, was included in the survey for identification of alcohol use in the last 12 months (Cronbach’s α = 0.80) [34]. AUDIT scores were stratified into three groups: a score <8 representing abstinence or low use, 8–15 “hazardous use,” and ≥16 “harmful use,” including those with potential alcohol dependency (score of 20 or higher), according to WHO categories [35].
Statistical Analysis
Survey data were analyzed using the STATA version 14 statistical software (Stata Corporation, College Station, USA). Depression, measured by the CES-D score, was the primary outcome of interest. Descriptive analysis was performed using Pearson’s chi-squared test. Sensitivity analyses were performed first using binary logistic analysis with unlikely to be depressed and a combined “possibly or probably depressed” and then using ordered logistic analysis with all three categories. A final sensitivity analysis was performed to test whether the model results changed with the inclusion of bisexual behavior (reporting both male and female sex partners) in place of bisexual identity.
Data collected via RDS recruitment are often weighted during statistical analysis to provide population prevalence estimates. Population estimates for the population characteristics and depression were calculated using the RDS-II estimator (Volz-Heckathorn) and bootstrapping with 1000 iterations to produce 95% confidence intervals (95%CI) [36]. Both crude sample proportions and RDS-weighted population prevalence estimates are provided in Appendix.
On exploratory analysis, the linear relationship between CES-D scores and time in which participants were surveyed was evaluated given increasing homophobia and the ultimate passage of the propaganda law. This relationship was significant, thus, we included the date of when participants completed the survey as a covariate in the model. This was transformed to a binary variable with March 7, 2012 as a breakpoint: the date in which the governor of St. Petersburg signed a law banning the sharing of homosexual propaganda [37]. While our study took place in Moscow City, political and media attention to the St. Petersburg law created an atmosphere of increased violence and discrimination against the LGBT population across Russia. The category for participation in the survey after the passage of the law is also inclusive of other key time periods that signify the deteriorating climate for LGBT populations, including the passage of the draft Ukraine law that received wide support and discussion in Russia (October 2012) and the date when the anti-gay propaganda law was introduced to the Russian Parliament (January 2013) [38]. Our model tests for an increase in the odds of probable depressive symptoms before and after the St. Petersburg law as a binary variable and as an interaction term with experienced stigma.
Variables known to be associated with depression symptoms (income, sexual identity, experience of stigma, social connectedness, alcohol use) [13, 15, 27–30] or with a p value of p < 0.10 in bivariate analysis were included in the multivariable model. The Furnival-Wilson leaps-and-bounds algorithm was used to perform variable selection on a wide array of models with depression as the outcome of interest and socioeconomic, demographic, experiential, and behavioral factors as predictor variables. Akaike’s information criteria were used to select the best model, and multiple logistic regression was used to obtain adjusted odds ratios (AOR) for the variables in the selected model. Collinearity for the model was checked using variance inflation factors (VIFs). While the VIF for the interaction between survey date and experience of stigma was 2.88, all other VIFs were well under 2.0, indicating that collinearity is not of concern. Pearson’s goodness-of-fit test was used to check model fit.
Ethical Review
The study was approved by both the Ethics Committee of the State Medical University, IP Pavlov, St. Petersburg, Russia, and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board, Baltimore, Maryland.
Results
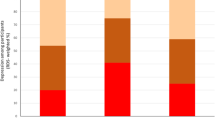
A total of 1376 MSM with a median age of 30 years [IQR 24–36] were enrolled in the study, 85.7% of whom were born within Russia. Over half (55%) identified as homosexual, 42.9% identified as bisexual, and 2.1% identified as other sexual identities, including heterosexual. By contrast, 64.6% reported only male sexual partners, while 35.4% reported both male and female partners in the last 12 months. Thirty-six percent reported experiencing stigma due to their sexual preferences. Over one-third (36.7%) qualified as probably depressed (n = 505), 11% as possibly depressed (n = 151), and 52.3% unlikely to be depressed according to the CES-D (n = 720).
Table 1 presents the participant demographic and behavioral characteristics stratified by depression symptomatology. Appendix Table 1 presents the RDS-weighted estimates stratified by depression symptomatology. Those with symptoms indicating probable depression (CESD ≥23) were more likely to have full-time employment (59.7%) than those with symptoms indicating unlikely or possible depression (CESD <23; 51.4%, p = 0.03). MSM in the probable depression group were more likely to identify as homosexual (64.7% vs. 49.5, p < 0.001) and less likely to report feeling comfortable with their sexual orientation (86.5 vs. 93.2%; p value <0.001) than those in the unlikely/possible depression group. Those with probable depression scores reported higher levels of experienced stigma (62.7 vs. 39.4%; p value <0.001) than those who were possibly/unlikely depressed. A larger proportion of those with probable depression had been detained in jail or prison (8.6%) than those with unlikely/possible depression (4.6%; p value <0.01). A greater proportion of those in the group with probable depression participated in the survey after the “propaganda law” was signed into law in St. Petersburg (61.4%) compared to those in the unlikely/possibly depressed group (48.7%; p value <0.001).
Table 2 displays the bivariate and multivariable logistic regression analyses of sexual identity, stigma, passage of the anti-gay propaganda laws, and other correlates with probable depression. After controlling for other confounders, the odds of probable depression was 29% lower among those identifying as bisexual (AOR 0.71 95%CI 0.52–0.97; p = 0.03) as compared to those reporting homosexual identity. The adjusted odds of depression was nearly twice as high for those who reported experiencing stigma in the last 12 months (ref: little/no stigma; AOR 1.75; 95%CI 1.20–2.56; p < 0.01). Those who reported discomfort with their sexual identity had almost sixfold increased odds of depression relative to those who reported feeling comfortable with their sexual identity (AOR 5.85; 95%CI 2.71–12.64; p < 0.001). A history of jail or detention was associated with a nearly twofold increased odds of probable depression (AOR 1.78; 95%CI 1.00–3.17; p = 0.05) compared to those who did not have a history of detention. Probable depression was also 35% lower for those with five or more sexual partners in the last 6 months (ref: ≤1 partner; AOR 0.54; 95%CI 0.37–0.81; p < 0.01).
Prior to including the interaction between time and experienced stigma in the multivariable model, the adjusted odds of depression for those who were surveyed after the signing of the St. Petersburg propaganda law was 1.5-fold greater than that of participants who were surveyed before the approval of the law (AOR 1.65, 95%CI 1.23–2.22; p = 0.001). After including the interaction between time and experience of stigma in the final model, the adjusted odds of depression associated with the survey date was no longer significant (AOR 1.34, 95%CI 0.95–1.91; p = 0.10). The interaction itself, however, was significant, and computed estimates for the combination with the interaction were highly significant. In this case, among people with experienced stigma, depression increased twofold after the passage of the St. Petersburg law (ref: participation prior to the law; AOR 2.24; 95%CI 1.49–3.39; p < 0.001). Finally, in the period after the law was passed, the odds of probable depression among people with experienced stigma were almost threefold that of those without experienced stigma (AOR 2.92; 95%CI 2.02–4.24; p < 0.001).
A sensitivity analysis was performed with the same multivariable model but including the variable measuring behavioral bisexuality in terms of the gender of reported sex partners in the last 12 months (in lieu of bisexual identity). Here, the association became stronger as the adjusted odds ratio dropped from 0.71 (95%CI 0.52–0.97, p = 0.03) in the previous model to 0.58 (95%CI 0.42–0.81; p < 0.01).
Discussion
Depression is common in the Russian Federation, and particularly so for MSM. Over a third of MSM in this sample qualified with “probable depression” according to the CES-D scale, and nearly half scored high enough to qualify as at least “possibly depressed.” These estimates for MSM in Russia exceed the general estimates of 23% for possible depression (CES-D cutoff of 16) in men in urban areas of Russia [3]. While methodological differences and temporal effects may play a role, differences may also be explained, in part, by the high prevalence of experienced stigma and its strong relationship with depressive symptoms.
Evidence has shown that sexual identity may be a correlate of depression and other mental health outcomes. In this study, bisexual identity appears to provide a protective effect against depression among MSM in Russia. Discomfort with sexual identity was also strongly associated with depressive symptoms. The protective relationship between bisexual identity and depression contradicts the general body of research, which predominantly originates from the USA, that has demonstrated increased risk for poor mental health outcomes with bisexual identity and similarly high risk for poor social wellbeing compared to those who identify as homosexual or heterosexual [22].
One reason for this surprising discrepancy may be the context of increasing and state-sanctioned homophobia in Russia. In a country that has criminalized information related to same sex behaviors, and ultimately criminalized LGBT visibility, the political and social environment has become increasingly hostile towards MSM. The discourse around the anti-gay movement has promoted traditional morals, masculinity, and traditional sexual relations and has been associated with increased violence towards LGBT populations and may decrease individual comfort with one’s sexual identity [18]. It is possible that endorsing a level of opposite-sex attraction in addition to same-sex attraction allows a degree of psychological refuge from feelings of exclusion, self-stigma, and experiences of violence. Discomfort with sexual identity may further be measuring underlying, internalized homophobia, which has demonstrated significant impact on mental health, including anxiety and depression [39].
The experience of detention in jail or prison also had a strong relationship with depressive symptoms. While we did not collect information about the reason for imprisonment, it would be interesting to know if sexual identity played either a real or perceived role in the justification for imprisonment.
Several factors limit the inferences of this study. The study was cross-sectional, limiting our ability to determine the temporal relationship between sexual identity and depression and prevents causal association. However, the use of recall periods for experiences of stigma (past 12 months) and depression (past 7 days) allows some interpretation of temporality. We utilized a tool to measure depression symptoms rather than depression diagnosed by a mental health professional, which may potentially misclassify participants; however, the CES-D has been well-established and validated in the Russian context. Enrollment and testing methods, criteria for study inclusion, and financial incentives may have influenced our sample. It is also possible that RDS did not reach particular subgroups within the MSM community. However, this study is unusual in its success of recruiting a large number of MSM (31 waves and over 1300 MSM) in a highly stigmatized setting. Despite potential limitations, RDS seems to have been one of the most productive pathways of recruiting MSM in this context [23].
Our results show that homosexual identity, experience of stigma, and experience of imprisonment are all associated with depressive symptoms in MSM in Russia. The passing of anti-gay propaganda laws in the region in 2012 and in the Russian Federation in 2013 [40], which effectively criminalizes information related to homosexual and bisexual identity, further modifies the relationship between stigma and depression among MSM. Because social support has been shown to be protective against depression in MSM in this context [41], interventions that build social support in the MSM community in Russia and enable access to non-stigmatizing mental health services may help to combat the negative effects of stigma and help protect against depression in this population.
References
Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the global burden of disease study. Lancet. 2010; 382(9904): 1575–1586.
Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013. doi:10.1371/journal.pmed.1001547.
Bobak M, Pikhart H, Pajak AK, et al. Depressive symptoms in urban population samples in Russia, Poland and the Czech Republic. Br J Psychiatry. 2006; 188(4): 359–365. doi:10.1192/bjp.188.4.359.
World Health Organization. Preventing suicide: a global imperative. Geneva, Switzerland: World Health Organization; 2014. http://www.who.int/mental_health/suicide-prevention/world_report_2014/en/. Accessed 30 August 2016.
King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry. 2008; 8(70). doi:10.1186/1471-244X-8-70.
Wirtz AL, Zelaya CE, Latkin C, et al. The HIV care continuum among men who have sex with men in Moscow, Russia: a cross-sectional study of infection awareness and engagement in care. Sex Transm Infect. 2016; 92: 161–167. doi:10.1136/sextrans-2015-052076.
Wirtz AL, Zelaya CE, Latkin C, et al. Alcohol use and associated sexual and substance use behaviors among men who have sex with men in Moscow, Russia. AIDS Behav. 2016; 20: 523–536.
Mayer KH, Bekker LG, Stall R, et al. Comprehensive clinical care for men who have sex with men: an integrated approach. Lancet. 2012; 380(9839): 378–387. doi:10.1016/S0140-6736(12)60835-6.
Wirtz AL, Kirey A, Peryskina A, et al. Uncovering the epidemic of HIV among men who have sex with men in Central Asia. Drug Alcohol Depend. 2013; 132(1): S17–S24. doi:10.1016/j.drugalcdep.2013.06.031.
Latypov A, Rhodes T, Reynolds L. Prohibition, stigma, and violence against men who have sex with men: effects on HIV in Central Asia. Central Asian Survey. 2013; 32(1): 52–65. doi:10.1080/02634937.2013.768059.
Republic of Tajikistan. Tajikistan National AIDS spending assessment (2008–09) flow of resources and expenditures for the response to HIV and AIDS. Dushanbe, Tajikistan: National Coordination Committee to Combat HIV/AIDS, TB, and Malaria in the Republic of Tajikistan, MoH of the Republic of Tajikistan; 2011.
Itaborahy LP, Zhu J. State-sponsored homophobia: a world survey of laws criminalizing same-sex sexual acts between consenting adults. In: International Lesbian, Gay, Bisexual, Trans, and Intersex Association. ILGA report. ILGA. http://old.ilga.org/Statehomophobia/ILGA_State_Sponsored_Homophobia_2015.pdf. Accessed 30 Aug 2016.
Stahlman S, Grosso A, Ketende S, et al. Depression and social stigma among MSM in lesotho: implications for HIV and sexually transmitted infection prevention. AIDS Behav. 2015; 19(8): 1460–1469. doi:10.1007/s10461-015-1094-y.
Choi KH, Steward WT, Miege P, et al. Sexual stigma, coping styles, and psychological distress: a longitudinal study of men who have sex with men in Beijing, China. Arch Sex Behav. 2016; 45(6): 1483–1491. doi:10.1007/s10508-015-0640-z.
Deuba K, Ekström AM, Shrestha R, et al. Psychosocial health problems associated with increased HIV risk behavior among men who have sex with men in Nepal: a cross-sectional survey. PLoS One. 2013;8(3). doi:10.1371/journal.pone.0058099.
Li J, Mo PK, Wu AM, et al. Roles of self-stigma, social support, and positive and negative effects as determinants of depressive symptoms among HIV infected men who have sex with men in China. AIDS Behav. Published online first. 2016. doi:10.1007/s10461-016-1321-1.
Persson E. Banning “homosexual propaganda”: belonging and visibility in contemporary Russian media. Sex Cult. 2015; 19: 256–274. doi:10.1007/s12119-014-9254-1.
Bartholomew RE. Beware the medicalisation of deviance in Russia: remembering the lessons of history. J R Soc Med. 2014; 107(5): 176–177. doi:10.1177/0141076814532393.
Roberts S. Ukraine gives initial approval to anti-gay law. Pink News. http://www.pinknews.co.uk/2012/10/02/ukraine-gives-initial-approval-to-anti-gay-law/. Accessed 30 Aug 2016.
Draft law of ex-MP Kolesnichenko banning “gay propaganda” was removed from consideration in Verkhovna Rada. Gay Alliance Ukraine. http://upogau.org/eng/inform/uanews/worldnews_975.html. Accessed 16 Dec 2016.
Reilly K. Russia’s anti-gay laws in line with public’s views on homosexuality. Washington, DC: Pew Research Center; 2013.
Kertzner RM, Meyer IH, Frost DM, et al. Social and psychological well-being in lesbians, gay men, and bisexuals: the effects of race, gender, age, and sexual identity. Am J Orthopsychiatry. 2009; 79(4): 500–510. doi:10.1037/a0016848.
Wirtz AL, Mehta SH, Latkin C, et al. Comparison of respondent-driven sampling estimators to determine HIV prevalence and population characteristics among men who have sex with men in Moscow, Russia. PLoS One. Published online first. 2016. doi:10.1371/journal.pone.0155519
Magnani R, Sabin K, Saidel T, et al. Review of sampling hard-to-reach and hidden populations for HIV surveillance. AIDS. 2005; 19(Suppl 2): S67–S72.
Wirtz A, Zelaya C, Peryshkina A, et al. Social and structural risks for HIV among migrant and immigrant men who have sex with men in Moscow, Russia: implications for prevention. AIDS Care. 2013; 26: 387–395. doi:10.1080/09540121.2013.819407.
Willis G. Cognitive interviewing and questionnaire design: a training manual. Rockville, MD: National Center for Health Statistics. 1994, Working Paper #7.
Ahaneku H, Ross MW, Nyoni JE, et al. Depression and HIV risk among men who have sex with men in Tanzania. AIDS Care. 2016; 1: 140–147. doi:10.1080/09540121.2016.1146207.
Secor AM, Wahome E, Micheni M, et al. Depression, substance abuse and stigma among men who have sex with men in coastal Kenya. AIDS. 2015; 29(3): S251–S259. doi:10.1097/QAD.0000000000000846.
Tomori C, McFall AM, Srikrishnan AK, et al. Diverse rates of depression among men who have sex with men (MSM) across India: insights from a multi-site mixed method study. AIDS Behav. 2016; 20(2): 304–316. doi:10.1007/s10461-015-1201-0.
Safren SA, Thomas BE, Mimiaga MJ, et al. Depressive symptoms and human immunodeficiency virus risk behavior among men who have sex with men in Chennai, India. Psychol Health Med. 2009; 14(6): 705–715. doi:10.1080/13548500903334754.
MacKellar DA, Gallagher KM, Finlayson T, et al. Surveillance of HIV risk and prevention behaviors of men who have sex with men—a national application of venue-based, time-space sampling. Public Health Rep. 2007; 122(Suppl 1): 39–47.
Radloff LS. The CES-D scale: a self-report depression scale for research in general population. Appl Psychol Meas. 1977; 1: 385–401.
Stall R, Mills TC, Williamson J, et al. Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDs among urban men who have sex with men. Am J Public Health. 2003; 93(6): 939–942.
Saunders JB, Aasland OG, Babor TF, et al. Development of the alcohol-use disorders identification test (AUDIT)—WHO collaborative project on early detection of persons with harmful alcohol-consumption. Addiction. 1993; 88(6): 791–804.
Babor T, Higgins-Biddle J, Saunders JB, Monteiro M. The alcohol use disorders identification test: guidelines for primary care. Geneva, Switzerland: WHO; 2001.
Schonlau M, Liebau E. Respondent-driven sampling. Stata J. 2012; 12(1): 72–93.
Elder M. St. Petersburg bans ‘homosexual propaganda.’ The Guardian. 2012. https://www.theguardian.com/world/2012/mar/12/st-petersburg-bans-homosexual-propaganda. Accessed 30 Aug 2016.
Baczynska G, de Corbonnel A. Russian parliament backs ban on “gay propaganda.” Reuters. http://www.reuters.com/article/us-russia-gay-idUSBRE90O0QT20130125. Accessed 30 Aug 2016.
Igartua KJ, Gill K, Montoro R. Internalized homophobia: a factor in depression, anxiety, and suicide in the gay and lesbian population. Can J Commun Ment Health. 2003; 22(2): 15–30. doi:10.7870/cjcmh-2003-0011.
O Vnesenii Izmenenij v Stat’ju 5 Federal’nogo Zakona “O Zasite Detej ot Informacii, PricinJajusej Vred ih Zdorov’ju i Razvitiju” i Otdel’nye Zakonodatel’nye Akty Rossijskoj Federacii v Celjah Zasity Detej ot Informacii, Propagandirujusej Otricanie Tradicionnyh Semejnyh Cennostej [On Amendments to Article 5 of the Federal Law “On Protection of Children from Information Harmful to Their Health and Development” and to Certain Legislative Acts of the Russian Federation with the Aim of Protecting Children from Information that Promotes the Denial of Traditional Family Values]. Moscow: Sobranie Zakonodatel’stva Rossiiskoi Federatsii [Russian Federation Collection of Legislation]; 2013. No. 26, Item 3208. Russian. http://asozd2.duma.gov.ru/main.nsf/(Spravka)?OpenAgent&RN=44554-6&02 [http://perma.cc/Y2WQ-EFXH]. Accessed 30 Aug 2016.
Logie CH, Newman PA, Chakrapani V, et al. Adapting the minority stress model: associations between gender non-conformity stigma, HIV-related stigma and depression among men who have sex with men in South India. Soc Sci Med. 2012; 74(8): 1261–1268. doi:10.1016/j.socscimed.2012.01.008.
Acknowledgements
We wish to thank SANAM clinic and Tatiana Bondarenko for insight, support, and use of the SANAM clinic for conduct of qualitative research and the Be Safe study. We appreciate the efforts put forth by Irina Deobald and Konstantin Dyakonov in the formative phases of this project. We are deeply thankful to the participants who contributed their time and personal experiences to this study.
Authors’ Contributions
CB, ALW, CEZ, NG, VM, AP, and CL collaborated in the design and oversight of the overall study. PD and KI collected data. EH conducted data analysis. ALW reviewed and provided input to the statistical analysis. EH and ALW wrote the initial drafts of this manuscript. All authors had full access to the data, reviewed and edited the manuscript, and all take responsibility for its integrity as well as the accuracy of the analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by both the Ethics Committee of the State Medical University, IP Pavlov, St. Petersburg, Russia, and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board, Baltimore, Maryland.
Funding
Funding for this study came from the National Institute of Mental Health (NIMH R01 MH085574-01A2) “High Risk Men: Identity, Health Risks, HIV and Stigma” funded from 2009 to 2014. Drs. Wirtz, Latkin, Galai, and Beyrer are also supported by the Johns Hopkins University Center for AIDS Research (P30AI094189).
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 35 kb)
Rights and permissions
About this article

Cite this article
Hylton, E., Wirtz, A.L., Zelaya, C.E. et al. Sexual Identity, Stigma, and Depression: the Role of the “Anti-gay Propaganda Law” in Mental Health among Men Who Have Sex with Men in Moscow, Russia. J Urban Health 94, 319–329 (2017). https://doi.org/10.1007/s11524-017-0133-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-017-0133-6