
Abstract
This study aimed to establish a new scoring model based on the early brain injury (EBI) indicators to predict the 90-day functional outcomes in patients with aneurysmal subarachnoid hemorrhage (aSAH). We retrospectively enrolled 825 patients and prospectively enrolled 108 patients with aSAH who underwent surgical clipping or endovascular coiling (derivation cohort = 640; validation cohort = 185; prospective cohort = 108) in our institute. We established a logistic regression model based on independent risk factors associated with 90-day unfavorable outcomes. The discrimination of the prognostic model was assessed by the area under the curve in a receiver operating characteristic curve analysis. The Hosmer–Lemeshow goodness-of-fit test and a calibration plot were used to evaluate the calibration of the prediction model. The developed scoring model named “TAPS” (total score, 0–7 points) included the following admission variables: age > 55 years old, WFNS grade of 4–5, mFS grade of 3–4, Graeb score of 5–12, white blood cell count > 11.28 × 109/L, and surgical clipping. The model showed good discrimination with the area under the curve in the derivation, validation, and prospective cohorts which were 0.816 (p < 0.001, 95%CI = 0.77–0.86), 0.810 (p < 0.001, 95%CI = 0.73–0.90), and 0.803 (p < 0.001, 95%CI = 0.70–0.91), respectively. The model also demonstrated good calibration (Hosmer–Lemeshow goodness-of-fit test: X2 = 1.75, df = 8, p = 0.988). Compared with other predictive models, TAPS is an easy handle tool for predicting the 90-day unfavorable outcomes of aSAH patients, which can help clinicians better understand the concept of EBI and quickly identify those patients at risk of poor prognosis, providing more positive treatment strategies. Trial registration: NCT04785976. Registered 5 March 2021-retrospectively registered, http://www.clinicaltrials.gov.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The concept of “early brain injury” (EBI) was introduced in a rat model in 2004 to explain the acute pathophysiological events that occur in the brain within the first 72 h of aneurysmal subarachnoid hemorrhage (aSAH) [1]. EBI is now believed to be an important determinant of unfavorable outcomes in patients with aSAH [2,3,4,5,6].
The first 72 h after aneurysm rupture are critical for patients, and most patients die within this dangerous period. At this stage, patients experience brain injuries due to blood release and accumulation, acute reactive hyperemia, transient cerebral ischemia, and systemic complications [7,8,9]. Moreover, these brain injuries can also increase the risk of complications in various body systems, resulting in a poor prognosis for the patient [10, 11]. At present, the definition of the EBI indicator is not clear, thus leading to a dilemma that although people know the criticality of EBI, the indicators cannot be effectively used in clinical practice. A recent review attempted to define EBI from the perspectives of four fields: clinical signs and symptoms, neuroimaging, invasive neuromonitoring, and neurohemoinflammation and systemic inflammation, which inspired us to explore the practical clinical application value of EBI [12].
Therefore, based on the definition of EBI, in this study, we aimed to (1) evaluate the relationship between EBI indicators and 90-day prognosis, (2) devise a new scoring system for aSAH patients based on EBI indicators that can intuitively evaluate their prognosis, and (3) compare EBI model with already published models to evaluate the advantages of EBI model comprehensively. The results will help clinicians better understand this critical period, improve their ability to perceive EBI indicators, identify those patients at risk early, and provide more positive treatment strategies.
Methods
Study Design
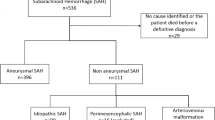
A total of 825 consecutive aSAH patients who underwent surgical clipping (SC) or endovascular coiling (EC) were retrospectively enrolled and divided into two independent cohorts (derivation cohort, n = 640, January 2015 to December 2019 and validation cohort, n = 185, January 2020 to December 2020). Furthermore, another independent cohort (prospective cohort, n = 108) was enrolled between April 2021 and September 2021. All patient data were from the Long-term Prognosis of Emergency Aneurysmal Subarachnoid Hemorrhage (LongTEAM) Registry study (registration no. NCT 04,785,976). In this study, all patients had angiographically documented aneurysms with subarachnoid hemorrhage (SAH), confirmed by either computed tomography (CT) or lumbar puncture. We set the inclusion criteria as follows: (1) age ≥ 18 years; (2) less than 72 h from the rupture to the admission and less than 72 h from the admission to treatment; (3) single aneurysm; and (4) complete 90-day follow-up. The main exclusion criteria were as follows: (1) previous history of ruptured aneurysm or SAH; (2) physical disability due to any previous disease; (3) treatment including external ventricular drainage, lumbar puncture, angiography, intubation, and/or mechanical ventilation at other hospitals before presentation to our hospital; and (4) missing data, including medical, radiological, and laboratory information. All available data without missing essential values from databases were used to meet the ten events per variable rule and maximize the generalizability and power of our results.
This study was approved by the Institutional Review Board of Beijing Tiantan Hospital (KY 2021–008-01). Informed consent was obtained from all individual participants or their authorized representatives for the study. All patients were managed according to the guidelines during hospitalization [13].
Parameters
All patients’ data were obtained from their medical records. We collected patients’ demographic information, medical history, size and location of the aneurysm, EBI indicators, and in-hospital complications. EBI indicators included clinical symptoms and consciousness scores on admission, first imaging characteristics and scores, and laboratory examination on admission. Clinical signs and condition of consciousness scores included early seizures and early loss of consciousness after ictus and the World Federation of Neurosurgical Societies (WFNS) grade [14]. Imaging characteristics and scores included acute hydrocephalus, the modified Fisher scale grade (mFS), the Graeb score, and the Subarachnoid Hemorrhage Early Brain Edema (SEBES) score [15,16,17]. The patient’s radiographic scores were assessed independently by two neurosurgeons, and a third radiologist would determine the final result in case of controversial results. Laboratory examination included the glucose level (GLU, fasting plasma glucose normal range: [3.9–6.1] mmol/L), white blood cell (WBC, normal range: [3.5–9.5] × 109/L) count, monocyte (MONO, normal range: [0.10–0.60] × 109/L) count, lymphocyte (LY, normal range: [1.10–3.2] × 109/L) count, neutrophil (NEUT, normal range: [1.80–6.30] × 109/L) count, and hemoglobin (HGB, normal range: [120–160 for male; 110–150 for female] g/L) level. Besides, we collected some ratio-related biomarkers that have been previously reported to be associated with prognosis, such as serum glucose/potassium ratio (GLU/K), neutrophil-to-lymphocyte ratio (NLR), mean platelet volume-to-platelet count ratio (MPV/PLT), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR) [18,19,20,21,22]. In-hospital complications such as delayed cerebral ischemia (DCI), intracranial infection, hypoproteinemia, pneumonia, and deep vein thrombosis were also collected. Supplementary Table 1 shows the detailed diagnostic criteria for the above in-hospital complications.
Outcome Measures
The neurosurgeon followed up with patients via telephone or an outpatient appointment 90 days after discharge. Unfavorable outcome was defined as an mRS score ≥ 3.
Statistical Analysis
All statistical analyses were performed using SPSS Statistics 26.0 (IBM, Armonk, New York, USA), GraphPad PRISM 8.3.0. (GraphPad Software Inc, San Diego, CA, USA), and R (version 2.12.2) software for Windows. p < 0.05 was considered statistically significant.
Descriptive variables were summarized as the mean ± standard deviation (SD) or median values with interquartile range (IQR) for continuous variables and frequencies (percentage) for categorical variables. Chi-squared tests or Fisher’s exact tests were used to compare categorical variables, and Student’s t-test or the Mann–Whitney test was used to compare the quantitative variables, as appropriate. Weighted kappa coefficients were used to test inter-rater agreement of imaging features (Supplementary Table 2). Only variables with p ≤ 0.05 in univariate analysis were entered in multivariate logistic regression analysis (forward stepwise) to identify the independent EBI risk factors associated with 90-day unfavorable outcomes. Associations were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). If there were continuous variables in the multivariate output results, the cutoff value was calculated by Youden’s index through receiver operating characteristic curve (ROC) analysis and reanalyzed into the multivariate regression model as new variables to obtain the final result. Multicollinearity was assessed using the tolerance and variance inflation factor (VIF).
We computed a prediction equation for 90-day unfavorable functional outcome in aSAH patients based on each risk factor’s β coefficients in the multivariate analysis, referring to the following Eq. (1):
with LP = a + b1X1 + b2X2 + … + bpXp, b1, b2,…, bp as the regression coefficients associated with each of the variables in the final logistic model [23]. Considering the utility and convenience of clinical application, we developed a new EBI risk-scoring system based on the β coefficients, and the ability of the model to discriminate was assessed by the area under the curve (AUC) in ROC analysis. Prediction accuracy was evaluated using Brier scores. The Hosmer–Lemeshow goodness-of-fit test and a calibration plot were used to evaluate the calibration of the prediction model.
Results
Patient Cohort
A total of 933 patients were included in the study, of whom 640 patients were included in the derivation cohort, 185 patients were included in the validation cohort, and 108 patients were included in the prospective cohort. The characteristics of the derivation, validation, and prospective cohorts are summarized in Tables 1 and 2. The 90-day unfavorable outcome rate was 17.5% (112/640) in the derivation cohort, 20.5% (38/185) in the validation cohort, and 15.7% (17/108) in the prospective cohort.
Independent Risk Factors Associated with 90-Day Unfavorable Outcomes in the Derivation Cohort
The forward stepwise multivariate analysis showed that age (p < 0.001, OR = 1.05, 95%CI = 1.02–1.07), WFNS grade of 4–5 (p < 0.001, OR = 4.32, 95%CI = 2.59–7.19), mFS grade of 3–4 (p = 0.014, OR = 3.05, 95%CI = 1.25–7.40), Graeb score of 5–12 (p = 0.008, OR = 2.56, 95%CI = 1.28–5.09), WBC count (p = 0.009, OR = 1.08, 95%CI = 1.02–1.14), and surgical clipping (p = 0.005, OR = 2.00, 95%CI = 1.24–3.23) were independent risk factors associated with 90-day unfavorable outcomes (Supplementary Table 3). ROC analysis was conducted for the two continuous variables (age and WBC count), and the cutoff value was determined by Youden’s index (age > 55, p < 0.001, sensitivity = 64.3%, specificity = 58.3%, Youden’s index = 0.23; WBC count > 11.28 × 109/L, p < 0.001, sensitivity = 83.0%, specificity = 46.8%, Youden’s index = 0.30).
Two indicators (age > 55 and WBC count > 11.28 × 109/L) were returned to the multivariate model to derive the final results. The model demonstrated that age > 55 years old (p < 0.001, OR = 2.51, 95%CI = 1.55–4.05), WFNS grade of 4–5 (p < 0.001, OR = 4.44, 95%CI = 2.70–7.32), mFS grade of 3–4 (p = 0.011, OR = 3.17, 95%CI = 1.31–7.71), Graeb score of 5–12 (p = 0.007, OR = 2.58, 95%CI = 1.30–5.13), WBC count > 11.28 × 109/L (p < 0.001, OR = 2.81, 95%CI = 1.59–4.98), and surgical clipping (p = 0.007, OR = 1.94, 95%CI = 1.20–3.14) were independent risk factors associated with 90-day unfavorable outcomes (Table 3). There was no evidence of multicollinearity between risk factors, with tolerance values above 0.10 and VIF values < 10 in all cases (Supplementary Table 2).
Model Performance
We constructed a new EBI scoring system based on the model output results, named the Tiantan Aneurysmal Subarachnoid Hemorrhage Prognostic Scoring System (TAPS), that allowed for the estimation of 90-day unfavorable outcomes in patients with aSAH, according to Eq. (1), where LP = − 4.714 + 0.919 × (age > 55 years old = yes) + 1.491 × (WFNS grade = 4–5) + 1.155 × (mFS grade = 3–4) + 0.947 × (Graeb score = 5–12) + 1.033 × (WBC > 11.28 × 109/L = yes) + 0.664 × (surgical clipping = yes). The AUC for this equation in the derivation, validation, and prospective cohort was 0.817, 0.811, and 0.794, respectively. The calibration plot also revealed a good concordance between the likelihood of predicted unfavorable outcome and actual unfavorable outcome in the derivation cohort (Brier = 0.109), validation cohort (Brier = 0.122), and prospective cohort (Brier = 0.119) (Fig. 1).

Discrimination and calibration according to the equation in the a derivation, b validation, and c prospective cohorts
Based on the β coefficients in the multivariate analysis, scores of 2 were assigned to a WFNS grade of 4–5 and scores of 1 were assigned to age > 55 years old, mFS grade of 3–4, Graeb score of 5–12, WBC > 11.28 × 109/L, and surgical clipping. The total score of the scoring system was 7 (range 0–7) points to predict the functional outcome of patients with aSAH 90 days after discharge (Table 4). In the derivation cohort, the AUC of the TAPS was 0.816 (p < 0.001, 95%CI = 0.772–0.859), which showed good calibration (Hosmer–Lemeshow goodness-of-fit test: X2 = 1.75, df = 8, p = 0.988). In the validation and prospective cohort, the AUC of the TAPS was 0.810 (p < 0.001, 95%CI = 0.725–0.896) and 0.803 (p < 0.001, 95%CI = 0.698–0.907) (Fig. 2).

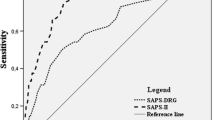
Comparison of AUC between TAPS and five other models in the a derivation, c validation, and e prospective cohorts. Probability of TAPS to predict 90-day unfavorable outcomes in the b derivation, d validation, and f prospective cohorts
When TAPS ranges from 6 to 7, the prediction risk of 90-day unfavorable outcomes was 68.1%, 70.0%, and 60.1% in the derivation, validation, and prospective cohort (Fig. 2).
Comparison of TAPS with other Predictive Models for aSAH Patients
We compared TAPS with five other prediction models (Table 5). TAPS is an easy-to-perform model that contains easily accessible indicators. In the derivation cohort, TAPS shows better discrimination than SAHIT (AUC = 0.802), FRESH (AUC = 0.784), Lai et al. 2020 (AUC = 0.742), HAIR (AUC = 0.727), and Mao et al. 2016 (AUC = 0.626). In the validation cohort, TAPS shows better discrimination than FRESH (AUC = 0.799), HAIR (AUC = 0.796), Lai et al. 2020 (AUC = 0.749), and Mao et al. 2016 (AUC = 0.694). In the prospective cohort, TAPS shows better discrimination than FRESH (AUC = 0.796), Mao et al. 2016 (AUC = 0.606), and Lai et al. 2020 (AUC = 0.546) (Fig. 2).
Discussion
Aneurysmal subarachnoid hemorrhage is a life-threatening condition with high disability and mortality rates [24, 25]. The 72-h period after a stroke is critical, and patient deaths are mostly due to EBI mechanisms [1,2,3,4, 12]. It is now widely accepted that EBI is a key factor leading to poor patient prognosis and is even more harmful than delayed complications, such as cerebral vasospasm (CVS) and DCI, occurring in the delayed phase [2, 4, 26]. Some abnormal changes in EBI indicators may also be a precursor to CVS and CVS-unrelated DCI, increasing the risk of unfavorable outcomes [17, 27]. From this point of view, controlling EBI is essential for patient prognosis.
Our study provides a prediction model named the “TAPS” based on the EBI indicators to predict unfavorable outcomes at 90 days after discharge in patients with aSAH. The model contains demographic information, clinical symptoms and consciousness scores on admission, first imaging characteristics and scores, laboratory examination on admission, and treatment modality. Finally, the model output results included six factors: age > 55 years old, WFNS grade of 4–5, mFS grade of 3–4, Graeb score of 5–12, WBC count > 11.28 × 109/L, and surgical clipping. According to the AUC results of the derivation (0.816), validation (0.810), and the prospective cohort (0.803), the TAPS was very stable with good performance in predicting 90-day unfavorable outcomes.
Before our study, some models had been published for the prognosis of patients with aSAH. In 2016, Mao et al. proposed a 3-month prognostic model for elderly aSAH patients, including age, hypertension, frailty, smoking, Hunt and Hess (HH) score, aneurysm number, and aneurysm size; the discrimination of the model in their validation cohort was 0.79 [28]. In 2020, Lai et al. proposed a 3-month prognostic model, including a Glasgow coma scale at 24 h after surgery, surgical clipping, and NLR; the discrimination of the model in their validation cohort was 0.86 [29]. In 2018, the SAHIT multinational cohort study proposed a 3-month prognostic model, including age, WFNS grade, premorbid hypertension, Fisher grade, size and location of the aneurysm, and surgical clipping; the discrimination of the model in their validation cohort was 0.81 [30]. In 2014, Lee et al. proposed a model named “HAIR” to predict in-hospital mortality for SAH patients, including age, HH score, intraventricular hemorrhage (IVH), and rebleed within 24 h of admission; the highest score of the model could predict 83.3% in-hospital mortality [31]. In 2016, Jens et al. proposed a model named “FRESH” to predict the 12-month outcomes for SAH patients, including age, HH score, APACHE-II score, and rebleed with 48 h of hospital admission; the discrimination of the model in their validation cohort was 0.77 [32]. Our study compared the similarities and differences of TAPS with the above five already published models. By comparing these models, TAPS had a stable and good ability to predict 90-day outcomes in patients with aSAH in the three cohorts; moreover, we found that although these models targeted slightly different populations or outcome events, the variables included did not have more than six dimensions: (1) demographic information; (2) clinical status; (3) imaging information; (4) medical history; (5) laboratory tests; and (6) treatment modality. Notably, SAHIT showed better discrimination than TAPS in our validation and prospective cohorts. We acknowledge that SAHIT is an excellent prognostic model. However, its computational process is very complex, which may restrict its clinical application.
Interestingly, among these models, only TAPS emphasizes the importance of preoperative inflammatory biomarkers (collection time of NLR was not stated in Lai’s study), further illustrating the importance of the inflammatory response during EBI. Inflammation is an extremely broad category of physiological and pathophysiological host responses to infection and tissue injury [33]. aSAH has also been shown as a state of systemic inflammation and immunosuppression [34]. More attention has been paid to the relationship between inflammation and DCI after aSAH. For example, previous studies showed that WBC could predict DCI after aSAH, which may be the main reason for unfavorable outcomes [35,36,37,38,39]. DCI was a major risk factor for poor outcomes in aSAH patients treated with SC and EC in our previous study published using the LongTEAM database [40]. Therefore, we hypothesized that WBC mediated this process. However, whether other mechanisms could explain the poor prognosis due to WBC needs to be confirmed in further studies.
In the TAPS, predictors such as age, the WFNS grade, and the mFS grade have all been demonstrated in previous literature to be related to poor prognosis in patients with aSAH [41, 42]. The International Subarachnoid Aneurysm Trial (ISAT) in 2002 and the Barrow Ruptured Aneurysm Trial (BRAT) in 2012 indicated that endovascular coiling was superior to surgical clipping [43, 44]. In our previous study, EC shows advantages in discharge and 90-day outcomes, in-hospital complications, and the number of risk factors over SC [40]. One study in 2018 regarded IVH as a binary variable in a multivariate regression model, and it was found to be associated with in-hospital mortality [45]. The potential reason for unfavorable outcomes caused by IVH might be the higher incidence of hydrocephalus and DCI [46]. In the TAPS, we used Graeb score to evaluate IVH more precisely, and it might be more helpful to improve the sensitivity to predict adverse events by incorporating Graeb score with mFS score. One study in 2018 conveyed the similar view, which showed accounting for IVH volume improved the prediction of DCI by the mFS [47].
The current understanding of EBI indicators is still limited, but it is encouraging that many reports have recently been published from basic research, which hypothesized from multiple aspects and designed experiments to successfully achieve the purpose of reducing specific EBI indicators [48,49,50,51]. In addition, in the field of clinical research, some articles have correlated certain preoperative parameters with prognosis using risk factor analysis to obtain indicators that have predictive value, such as reduced sulcal volume, higher serum levels of lactate dehydrogenase, monocyte-based inflammatory indices, glycemic indices, and high angiopoietin-1 levels [52,53,54,55,56]. However, how to apply EBI indicators with predictive significance that were derived from basic research widely and quickly to clinical practice and, in turn, how to return EBI indicators with a predictive value that were derived from clinical research to basic research for mechanistic elaboration involve the development of translational medicine and are a complex process.
Limitations
Some limitations of our study need to be discussed. First, the predictive model requires further external validation in a larger multicenter study. Second, when comparing different models, the results cannot deny the contribution of the original study because the different models target slightly different populations and outcome events. Third, the EBI indicators we included are all commonly used and easily accessible in clinical practice, and some other EBI indicators from the basic research may improve the model’s discrimination.
Conclusions
In this study, we established a new 90-day predictive model named “TAPS” based on EBI indicators for aSAH patients, which contains six predictors (age > 55 years old, WFNS grade 4–5, mFS grade 3–4, Graeb score 5–12, WBC count > 11.28 × 109/L, and surgical clipping) with a total score of 7 points. TAPS is an efficient and easily handled model with good discrimination and calibration, which is helpful for neurosurgeons to quickly identify those patients who are likely to have unfavorable outcomes.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Kusaka G, Ishikawa M, Nanda A, Granger DN, Zhang JH. Signaling pathways for early brain injury after subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2004;24:916–25.
Tso MK, Macdonald RL. Subarachnoid hemorrhage: a review of experimental studies on the microcirculation and the neurovascular unit. Transl Stroke Res. 2014;5:174–89.
Claassen J, Carhuapoma JR, Kreiter KT, Du EY, Connolly ES, Mayer SA. Global cerebral edema after subarachnoid hemorrhage: frequency, predictors, and impact on outcome. Stroke. 2002;33:1225–32.
Fujii M, Yan J, Rolland WB, Soejima Y, Caner B, Zhang JH. Early brain injury, an evolving frontier in subarachnoid hemorrhage research. Transl Stroke Res. 2013;4:432–46.
Ray B, Pandav VM, Mathews EA, et al. Coated-platelet trends predict short-term clinical outcomeafter subarachnoid hemorrhage. Transl Stroke Res. 2018;9:459–70.
Rass V, Helbok R. Early brain injury after poor-grade subarachnoid hemorrhage. Curr Neurol Neurosci Rep. 2019;19:78.
Sehba FA, Friedrich V. Early events after aneurysmal subarachnoid hemorrhage. Acta Neurochir Suppl. 2015;120:23–8.
Taki W, Sakai N, Suzuki H, et al. Determinants of poor outcome after aneurysmal subarachnoid hemorrhage when both clipping and coiling are available: Prospective Registry of Subarachnoid Aneurysms Treatment (PRESAT) in Japan. World Neurosurgery. 2011;76:437–45.
Fu C, Yu W, Sun L, Li D, Zhao C. Early cerebral infarction following aneurysmal subarachnoid hemorrhage: frequency, risk factors, patterns, and prognosis. Curr Neurovasc Res. 2013;10:316–24.
Radolf S, Smoll N, Drenckhahn C, Dreier JP, Vajkoczy P, Sarrafzadeh AS. Cerebral lactate correlates with early onset pneumonia after aneurysmal SAH. Transl Stroke Res. 2014;5:278–85.
Suzuki H, Sakurai M, Fujimoto M, Tsuchiya T, Sakaida H, Taki W. Complete recovery from aneurysmal subarachnoid hemorrhage associated with out-of-hospital cardiopulmonary arrest. Eur J Emerg Med. 2010;17:42–4.
Rass V, Helbok R. Early brain injury after poor-grade subarachnoid hemorrhage. Current Neurology and Neuroscience Reports. 2019 19.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43:1711–37.
Report of World Federation of Neurological Surgeons Committee on a universal subarachnoid hemorrhage grading scale. J Neurosurg. 1988 68: 985–986.
Claassen J, Bernardini GL, Kreiter K, et al. Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid hemorrhage: the Fisher scale revisited. Stroke. 2001;32:2012–20.
Graeb DA, Robertson WD, Lapointe JS, Nugent RA, Harrison PB. Computed tomographic diagnosis of intraventricular hemorrhage. Etiology and prognosis Radiology. 1982;143:91–6.
Ahn SH, Savarraj JP, Pervez M, et al. The subarachnoid hemorrhage early brain edema score predicts delayed cerebral ischemia and clinical outcomes. Neurosurgery. 2018;83:137–45.
Fujiki Y, Matano F, Mizunari T, et al. Serum glucose/potassium ratio as a clinical risk factor for aneurysmal subarachnoid hemorrhage. J Neurosurg. 2018;129:870–5.
Giede-Jeppe A, Reichl J, Sprügel M, et al. Neutrophil-to-lymphocyte ratio as an independent predictor for unfavorable functional outcome in aneurysmal subarachnoid hemorrhage. J Neurosurg. 2019;132:400–7.
Wang Z, Pei W, Chen L, Ning Y, Luo Y. Mean platelet volume/platelet count ratio is associated with poor clinical outcome after aneurysmal subarachnoid hemorrhage. J Stroke Cerebrovas Dis: Official J Nat Stroke Assoc. 2020;29:105208.
Yun S, Jun Yi H, Hoon Lee D, Hoon SJ. Clinical significance of platelet to neutrophil ratio and platelet to lymphocyte ratio in patients with aneurysmal subarachnoid hemorrhage. J Clin Neurosci Official J Neurosurg Soc Australasia. 2021;92:49–54.
Zhang P, Li Y, Zhang H, et al. Prognostic value of the systemic inflammation response index in patients with aneurismal subarachnoid hemorrhage and a Nomogram model construction. British journal of neurosurgery. 2020: 1–7. online ahead of print.
Sullivan LM, Massaro JM, D’Agostino RB Sr. Presentation of multivariate data for clinical use: the Framingham Study risk score functions. Stat Med. 2004;23:1631–60.
Time trends in outcome of subarachnoid hemorrhage. population-based study and systematic review. Neurology. 2010;74:1494–501.
The falling rates of hospital admission. case fatality, and population-based mortality for subarachnoid hemorrhage in England, 1999–2010. J Neurosurg. 2016;125:1–7.
Zhang JH. Vascular neural network in subarachnoid hemorrhage. Transl Stroke Res. 2014;5:423–8.
Sehba FA, Pluta RM, Zhang JH. Metamorphosis of subarachnoid hemorrhage research: from delayed vasospasm to early brain injury. Mol Neurobiol. 2011;43:27–40.
Yue Q, Liu Y, Leng B, et al. A prognostic model for early post-treatment outcome of elderly patients with aneurysmal subarachnoid hemorrhage. World Neurosurg. 2016;95:253–61.
Lai X, Zhang W, Ye M, Liu X, Luo X. Development and validation of a predictive model for the prognosis in aneurysmal subarachnoid hemorrhage. J Clin Lab Anal. 2020;34:e23542.
Jaja B, Saposnik G, Lingsma H, et al. Development and validation of outcome prediction models for aneurysmal subarachnoid haemorrhage: the SAHIT multinational cohort study. BMJ (Clinical research ed). 2018;360:j5745.
Lee V, Ouyang B, John S, et al. Risk stratification for the in-hospital mortality in subarachnoid hemorrhage: the HAIR score. Neurocrit Care. 2014;21:14–9.
Witsch J, Frey H, Patel S, et al. Prognostication of long-term outcomes after subarachnoid hemorrhage: the FRESH score. Ann Neurol. 2016;80:46–58.
Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008;454:428–35.
Saand A, Yu F, Chen J, Chou S. Systemic inflammation in hemorrhagic strokes - a novel neurological sign and therapeutic target? Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2019;39:959–88.
Al-Mufti F, Misiolek K, Roh D, et al. White blood cell count improves prediction of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. Neurosurgery. 2019;84:397–403.
Ma X, Lan F, Zhang Y. Associations between C-reactive protein and white blood cell count, occurrence of delayed cerebral ischemia and poor outcome following aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. Acta Neurol Belg. 2021;121:1311–24.
Mahta A, Azher A, Moody S, et al. Association of early white blood cell trend with outcomes in aneurysmal subarachnoid hemorrhage. World Neurosurgery. 2021;151:e803–9.
Hu P, Yang X, Li Y, et al. Predictive effects of admission white blood cell counts and hounsfield unit values on delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 2022;212:107087.
Kasius K, Frijns C, Algra A, Rinkel G. Association of platelet and leukocyte counts with delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage. Cerebrovascular Dis (Basel, Switzerland). 2010;29:576–83.
Li R, Lin F, Chen Y, et al. In-hospital complication-related risk factors for discharge and 90-day outcomes in patients with aneurysmal subarachnoid hemorrhage after surgical clipping and endovascular coiling: a propensity score-matched analysis. Journal of Neurosurgery. 2021: 1–12. online ahead of print.
Shen J, Yu J, Huang S, et al. Scoring model to predict functional outcome in poor-grade aneurysmal subarachnoid hemorrhage. Front Neurol. 2021;12:601996.
Takemoto Y, Hasegawa Y, Hashiguchi A, Moroki K, Tokuda H, Mukasa A. Predictors for functional outcome in patients with aneurysmal subarachnoid hemorrhage who completed in-hospital rehabilitation in a single institution. J Stroke Cerebrovasc Dis. 2019;28:1943–50.
McDougall CG, Spetzler RF, Zabramski JM, et al. The Barrow Ruptured Aneurysm Trial. J Neurosurg. 2012;116:135–44.
Molyneux AJ, Kerr RS, Yu LM, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366:809–17.
Stienen MN, Germans M, Burkhardt JK, et al. Predictors of in-hospital death after aneurysmal subarachnoid hemorrhage: analysis of a nationwide database (Swiss SOS [Swiss Study on Aneurysmal Subarachnoid Hemorrhage]). Stroke. 2018;49:333–40.
Jabbarli R, Reinhard M, Roelz R, et al. The predictors and clinical impact of intraventricular hemorrhage in patients with aneurysmal subarachnoid hemorrhage. International journal of stroke : official journal of the International Stroke Society. 2016;11:68–76.
Eagles ME, Jaja BNR, Macdonald RL. Incorporating a modified Graeb score to the modified fisher scale for improved risk prediction of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. Neurosurgery. 2018;82:299–305.
Xu P, Tao C, Zhu Y, et al. TAK1 mediates neuronal pyroptosis in early brain injury after subarachnoid hemorrhage. J Neuroinflammation. 2021;18:188.
Deng HJ, Deji Q, Zhaba W, et al. A20 establishes negative feedback with TRAF6/NF-kappaB and attenuates early brain injury after experimental subarachnoid hemorrhage. Front Immunol. 2021;12:623256.
Kuang H, Wang T, Liu L, et al. Treatment of early brain injury after subarachnoid hemorrhage in the rat model by inhibiting p53-induced ferroptosis. Neurosci Lett. 2021;762:136134.
Dodd WS, Noda I, Martinez M, Hosaka K, Hoh BL. NLRP3 inhibition attenuates early brain injury and delayed cerebral vasospasm after subarachnoid hemorrhage. J Neuroinflammation. 2021;18:163.
Yuan JY, Chen Y, Kumar A, et al. Automated quantification of reduced sulcal volume identifies early brain injury after aneurysmal subarachnoid hemorrhage. Stroke. 2021;52:1380–9.
McIntyre MK, Halabi M, Li B, et al. Glycemic indices predict outcomes after aneurysmal subarachnoid hemorrhage: a retrospective single center comparative analysis. Sci Rep. 2021;11:158.
Wang Y, Tian Y, Wang D, et al. High angiopoietin-1 levels predict a good functional outcome within 72 h of an aneurysmal subarachnoid hemorrhage: a prospective study from a single center. J Neurol Sci. 2015;356:72–6.
Feghali J, Kim J, Gami A, et al. Monocyte-based inflammatory indices predict outcomes following aneurysmal subarachnoid hemorrhage. Neurosurg Rev. 2021;44:3499–507.
Zheng S, Wang H, Chen G, et al. Higher serum levels of lactate dehydrogenase before microsurgery predict poor outcome of aneurysmal subarachnoid hemorrhage. Front Neurol. 2021;12:720574.
Acknowledgements
We acknowledge the contribution of all staff who participated in the present study.
Funding
This study was supported by the National Key Research and Development Program of China (Grant Nos. 2021YFC2501101 and 2020YFC2004701) and the National Natural Science Foundation of China (Grant Nos. 82071296, 81671129, and 81471210).
Author information
Authors and Affiliations
Contributions
Runting Li: conceptualization (equal); data curation (lead); formal analysis (lead); investigation (lead); methodology (equal); project administration (equal); software (lead); validation (lead); visualization (lead); writing original draft (lead); and writing review and editing (equal). Fa Lin: data curation (equal); methodology (equal); and software (equal). Yu Chen: data curation (equal); methodology (equal); and software (equal). Junlin Lu: data curation (equal); methodology (equal); and software (equal). Heze Han: data curation (equal); methodology (equal); and software (equal). Li Ma: data curation (equal). Yahui Zhao: data curation (equal). Debin Yan: data curation (equal). Ruinan Li: data curation (equal). Jun Yang: data curation (equal). Shihao He: data curation (equal). Zhipeng Li: data curation (equal). Haibin Zhang: data curation (equal). Kexin Yuan: data curation (equal). Ke Wang: data curation (equal). Qiang Hao: data curation (equal) and supervision (equal). Xun Ye: data curation (equal) and supervision (equal). Hao Wang: data curation (equal) and supervision (equal). Hongliang Li: data curation (equal) and supervision (equal). Linlin Zhang: data curation (equal) and supervision (equal). Guangzhi Shi: data curation (equal) and supervision (equal). Jianxin Zhou: data curation (equal) and supervision (equal). Yang Zhao: data curation (equal); resources (equal); and supervision (equal). Yukun Zhang: data curation (equal); resources (equal); and supervision (equal). Youxiang Li: data curation (equal); resources (equal); and supervision (equal). Shuo Wang: conceptualization (equal); funding acquisition (equal); resources (equal); supervision (equal); and writing review and editing (equal). Xiaolin Chen: conceptualization (equal); funding acquisition (equal); resources (equal); supervision (equal); and writing review and editing (equal). Yuanli Zhao: conceptualization (equal); resources (equal); supervision (equal); and writing review and editing (equal).
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Beijing Tiantan Hospital (KY 2021–008-01). Informed consent was obtained from all individual participants or their authorized representatives included in the study. All the analyses were performed in accordance with the Declaration of Helsinki and the local ethics policies.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Li, R., Lin, F., Chen, Y. et al. A 90-Day Prognostic Model Based on the Early Brain Injury Indicators after Aneurysmal Subarachnoid Hemorrhage: the TAPS Score. Transl. Stroke Res. 14, 200–210 (2023). https://doi.org/10.1007/s12975-022-01033-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12975-022-01033-4