
Abstract
The effects of treatment with probiotics on the immunological and hematobiochemical changes in Trypanosoma brucei infection were investigated. Probiotic strains used are Bifidobacterium BB-12, Lactobacillus acidophilus LA-5, Lactobacillus delbrueckii LBY-27, Lactobacillus paracasei LC-01, and Streptococcus thermophilus STY-31. Thirty rats randomly assigned to five groups were used in the experiment. Groups A to C received 1 × 109 CFU, 5 × 109 CFU, and 10 × 109 CFU of the multi-strain probiotics daily and respectively from day 0 post-supplementation (PS) to termination. Group D and E were the infected and uninfected controls respectively. On day seven PS, groups A to D were challenged intraperitoneally with approximately 1 × 106 trypanosomes. Parasitemia, nitric oxide level, hematobiochemical parameters, and antibody titer to heterologous antigen stimulation were monitored post-infection. By days 7 and 16 PS, probiotics-treated groups had significantly lower (p < 0.05) mean creatinine concentration than the controls; however, on day 7 PS, there were no significant variations in the leukocyte counts (LC), total erythrocyte counts (TEC), and the packed cell volume (PCV) in all experimental groups. Following infection, by day 16 PS, the pre-patent period, parasitemia levels, and antibody titer were similar in all infected groups. Furthermore, the probiotics-treated groups and the infected control had significantly lower PCV, TEC, and LC values when compared to the uninfected control, and probiotics treated groups (A and C) had only marginally lower nitric oxide levels than the infected control. Treatment with the probiotic strains gave a creatinine-lowering effect, was innocuous to the hematopoietic system, but was not sufficiently immunostimulatory in trypanosomosis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Trypanosomosis is a group of diseases caused by Trypanosoma spp. and it remains a very important human and animal health challenge. The hallmarks of the pathology of animal trypanosomosis are anemia, immunosuppression, oxidative damage, and hematobiochemical derangements [1,2,3,4,5].
The most commonly used chemotherapeutic or chemoprophylactic agents (including diminazene, homidium, and isometamidium salts) against animal trypanosomosis are over four decades old, and the problem of drug resistance is widespread [6, 7]. Even when clinical cure is achieved in animal patients, relapse of infections may follow shortly afterwards due to the inability of most trypanocides to sufficiently reach trypanosomes present in the brain [8], and due to failure of immunological defense of the body. Poor predictability of returns on investment resulting from high cost of research, development, clinical trials, and drug licensing is a disincentive to development of novel trypanocidal drugs by major pharmaceutical firms. The few attempts on drug developments notwithstanding, experts have opined that novel licensed trypanocides are not likely to be available in the near future; hence, fine and optimum use of the few available trypanocides is strongly advocated [6, 8].
Probiotics have immunomodulatory functions, and could improve overall health [9, 10]. Use of probiotics in hemoparasite infections with Plasmodium falciparum [11], Babesia microti [12, 13], Trypanosoma cruzi [14], and Trypanosoma brucei [15] gave positive results with respect to levels of parasitemia and immune responses. Antioxidant and serum biochemistry normalizing effects of certain probiotic strains have been documented [16, 17]. Although the bioactivities of probiotics are strain specific [18, 19], it has been shown that multi-strain probiotics mix could be more beneficial and more effective than single strains, even the individual strains that constitute the mixtures themselves [20, 21].
Proprietary probiotic strains whose biological and immunological attributes have been largely documented were chosen for this study, namely, Bifidobacterium BB-12, Lactobacillus acidophilus LA-5, Lactobacillus delbrueckii LBY-27, Lactobacillus paracasei LC-01, and Streptococcus thermophilus STY-31. Treatments with Bifidobacterium animalis subsp. lactis BB-12 modulated T cells and natural killer cell functions in respiratory infections of human patients [22]; it also induced interleukin-10 (IL −10) production in swine immune cells in vitro [23]. Tabasco et al. [24] demonstrated that the presence of Streptococcus thermophilus STY-31 acts at gene transcription level to enhance the production of bioactive molecules from Lactobacillus acidophilus LA-5. The well-established immunomodulatory and antioxidant properties of Lactobacillus acidophilus have been reported [25, 26]. More so, strains of Streptococcus thermophilus and Lactobacillus delbrueckii subsp. bulgaricus act synergistically in co-cultures [27]. Strains of Lactobacillus delbrueckii subsp. bulgaricus positively modulated mice macrophage functions in vitro and in vivo thereby inhibiting growth of tumor cells [28]. When administered orally, Lactobacillus paracasei subsp. paracasei L- 01 withstood intestinal stress, positively modulated intestinal micro-flora, and elicited antioxidant and immunity enhancing effects [29,30,31]. Sreeja and Prajapati [32] opined that patients with depressed immune function may benefit from administration of probiotics. Inflammatory biomarkers were improved in patients suffering gestational diabetes mellitus who consumed a probiotic mix containing Bifidobacterium BB-12, Lactobacillus acidophilus LA-5, Lactobacillus delbrueckii LBY-27, and Streptococcus thermophilus STY-31 [33].
Considering that immunosuppression and hematobiochemical derangements are cardinal features of trypanosomosis, we hypothesized that treatments with the probiotic strains used in this study could improve the resistance, the clinical pathological course, and the immune response to Trypanosoma brucei infection in rat models. Hence, this study investigated the effects of treatment with a probiotic mix on parasitemia, immune response, and hematobiochemical changes in trypanosomic rats.
Materials and Methods
Ethical Consideration
Ethical considerations for the use of the animal models in this study were based on the procedures of the Animal Use and Care Committee of the Faculty of Veterinary Medicine of the study institution, which agree with the NIH guidelines [34].
Experimental Animals
Thirty (30) male Sprague-Dawley rats weighing between 240 and 268 g were used for the study. Following 2 weeks of acclimatization, the rats were randomly assigned to five groups (n = 6) namely, A, B, C, D, and E. They were housed in fly-proof cages and fed with proprietary animal feed ad libitum while being allowed access to fresh drinking water.
Probiotics and Trypanosomes
The Trypanosoma spp. used in this work was isolated from a dog presented at the veterinary teaching hospital of the university, clinically ill from trypanosomosis. The isolated trypanosome was identified as Trypanosoma brucei at the department of veterinary parasitology and entomology of the university. The live multi-strain probiotics mix was obtained from CHR® (Netherlands). There were approximately 25 × 109 CFU of organisms per gram of the freeze dried culture. The mix contained the following five strains of probiotic organisms in equal proportion: Bifidobacterium BB-12, Lactobacillus acidophilus LA-5, Lactobacillus delbrueckii LBY-27, Lactobacillus paracasei LC-01, and Streptococcus thermophilus STY-31.
Treatment and Infection with Trypanosoma brucei
Groups A, B, and C received 1 × 109 CFU, 5 × 109 CFU, and 10 × 109 CFU of the multi-strain probiotics (MP) daily and respectively from day 0 post-supplementation (PS) to termination of the study. Groups D and E were the infected and the uninfected controls respectively, and therefore did not receive any treatment with probiotics. MP was delivered to rats in indicated groups as a suspension in 1 ml of distilled water administered through gastric gavages. On day 7 PS, groups A, B, C, and D were challenged intraperitoneally with approximately 1 × 106 Trypanosoma brucei suspended in phosphate buffered saline (PBS).
Blood Collection, Parasitemia, and Assays
A drop of peripheral blood on glass slide taken from tail tip snip was used for the detection and estimation of parasitemia by rapid matching technique [35] from 48 h post-infection in experimental animals. About 1.5 ml of blood was collected from the retro-bulbar plexus of the medial canthus of rats. One milliliter of blood was collected into plain eppendorf tubes, allowed to clot, and centrifuged at 3000 rpm for 5 min to separate the serum for biochemical assays, while the remaining 0.5 ml of blood was collected into sodium EDTA-treated bottles for hematological studies. The concentrations of blood urea nitrogen, and creatinine on days 7 and 16 PS were determined using commercial kits (Randox®, UK), while the serum nitric oxide levels were determined by the modified Griess method [36] on the same days. The total and differential leukocyte counts, the total erythrocyte count, and packed cell volumes were determined on days 7 and 16 PS using Leishman, hemocytometer, and micro-hematocrit methods respectively [37, 38].
Immunization of Rats with Sheep Erythrocytes
All the experimental animals were immunized with heterologous antigen—a 10% sheep erythrocyte, on day 17PS; 6 days later, (day 23 PS), sera harvested from rats in all the experimental groups were assayed for antibody titer levels by direct hemagglutination technique using 2% sheep erythrocytes as described by Ikeme and Adelaja [39]. Rats in all the infected groups (groups A–D) were severely ill by day 25 PS and were sacrificed the same day on humane grounds.
Data Analysis and Result Presentation
Data obtained were analyzed with ANOVA statistic using SPSS version 20. Variations in means were separated using the least significant difference (LSD) post hoc tests. Heteroscedasticity was accommodated with Welch’s robust test of equality of means [40]. Significance was accepted at p < 0.05. The results were presented as means ± standard error of mean using tables and figures.
Results
Serum Urea and Creatinine Concentrations
Supplementation with the probiotic mix led to significantly lower (p < 0.001) mean serum creatinine concentrations in groups B and C compared to the uninfected control (group E) (Table 1). Following infection, by day 16 PS, treatment with probiotics at 1 × 109 CFU daily (group A) resulted in a significantly lower (p < 0.001) mean serum creatinine concentration when compared to the levels in infected control. There was no significant variation in mean blood urea concentration across all the experimental groups on day 7 PS (Table 2). A general increase in urea concentration was seen on day 16 PS; however, the values were similar in all infected groups.
Pre-patent Period, Parasitemia, Antibody Titer, and Nitric Oxide Concentration
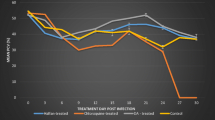
Infection established in all challenged groups within four (4) days. There were no statistically significant variations in mean pre-patent periods across all infected groups (Fig. 1). By day 12 PS (Fig. 2), the omnibus Welch’s ANOVA indicated no significant variation [Welch’s F(df 3, 10.301) = 1.317, p = 0.321] in the mean parasitemia across all the infected groups. However, with post hoc multiple comparison, the probiotics-supplemented groups A and C had similar mean parasitemia with group D (infected control) while group B (infected +5B CFU) had values significantly (p < 0.05) higher than that of group D (infected untreated) and group A. On day 16 PS, groups A, C, and D had similar mean parasitemia. Group B had significantly higher (p < 0.05) mean parasitemia than group C. On day 22 PS, there were no significant variations in mean parasitemia across all the experimental groups.

Mean pre-patent period (in days) of rats treated with multi-strain probiotics and infected with Trypanosoma brucei. A, infected +1 billion cfu; B, infected +5 billion cfu; C, infected +10 billion cfu; D , infected + untreated

Mean parasitemia (×106 trypanosomes/ml of blood) of rats treated with multi-strain probiotics and infected with Trypanosoma brucei
Following challenge with heterologous antigen, the mean antibody titers were similar across all infected groups by day 23 PS (Fig. 3). Prior to infection, by day 7 PS, probiotics supplementation did not result in significant variations in serum nitric oxide (NO) levels across all the experimental groups (Table 3). Following infection, by day 16 PS, probiotics-treated groups A (infected +1B CFU) and C (infected +10BCFU) had lower NO values which were similar to the level seen in the uninfected control. The infected control and group B had significantly higher (p < 0.05) serum NO levels compared to the uninfected control.

Mean antibody titer (log2 of HA unit/ml) on day 23 post-supplementation of rats treated with multi-strain probiotics and infected with Trypanosoma brucei. A, infected +1 billion cfu; B, infected +5 billion cfu; C, infected +10 billion cfu; D, infected + untreated; E, uninfected + untreated. * Significant variation (p < 0.05) from all other groups
Total Erythrocyte Count, Packed Cell Volume, Total and Differential Leukocyte Counts
Supplementation with probiotic strains, by day 7 PS, did not result in any significant variation in total erythrocyte counts and packed cell volumes in all the experimental groups (Tables 4 and 5); however, following infection, by day 16 PS, the total erythrocyte counts and the packed cell volumes were significantly lower in all infected groups compared to the uninfected control (group E).
There were no statistically significant variations in mean total white blood cell count across the groups by day 7 PS (Table 6). By day 16 post-supplementation (corresponding to day 9 post-infection), group E (uninfected control) had significantly higher (p < 0.05) total white blood cell count compared to all other experimental groups, while all infected groups maintained similar total leukocyte count. The mean absolute neutrophil and lymphocyte counts followed the same pattern as the total leukocyte counts (Tables 7 and 8).
Discussion
Before and after infection with Trypanosoma brucei, treatments with the probiotic strains resulted in significantly lower levels of serum creatinine in probiotics-supplemented groups compared to the control groups. Creatinine is a byproduct of muscle catabolism which is usually excreted via the kidney. It is elevated in conditions of kidney damage, severe muscle catabolism, and dehydration [41]. Cachexia and loss of muscle mass have been associated with animal trypanosomosis, where it could be secondary to anorexia, or directly mediated by tumor necrosis factor [3]. Trypanosoma brucei is markedly tissue invasive [42]; consequently, impaired kidney function reflected by elevated serum creatinine and blood urea nitrogen is a common finding in the disease [1, 43]. The findings from this work indicate that treatment with the probiotic strains produced a creatinine-lowering effect in animal trypanosomosis, conceivably by the improvement of the patients’ nutrition, thereby forestalling emaciation, interference with elaboration and function of tumor necrosis factor, or amelioration of trypanosomosis associated kidney damage. The creatinine-lowering effect of the probiotic strains in this study strongly supports the findings in recent reports [16, 19, 44] where it was shown that certain probiotic strains ameliorated oxidative damage of the kidney in rats with experimentally induced nephrotoxicity.
Pre-infection administration of probiotics did not prolong the onset of parasitemia as depicted by the absence of any meaningful variation in the mean pre-patent periods following challenge with trypanosomes. This was so even in groups where the probiotics were administered in excess of the recommended minimum dose of about 5 × 109 CFU daily for 5 days [45]. This finding suggests that the probiotic strains studied neither enhanced the resistance nor susceptibility of the models to the establishment of trypanosomiasis. Some workers reported a delay in onset of parasitemia in rats treated with the probiotic, Saccharaomyces cerevisiae and later challenged with Trypanosoma spp. [15]. Similarly, significantly longer pre-patent period and shorter duration of parasitemia were reported in mice infected with Plasmodium chaubodi following treatment with the probiotic Lactobacillus casei ATCC 7469 [46]. Our finding is at variance with the reports stated above, and the basis of this may not be unconnected to the fact that the bioactivities and effects of probiotics are strain specific [18, 19], and may vary with disease models.
The levels of parasitemia did not vary meaningfully between probiotic-treated groups and the control group in the later stages of acute trypanosomosis; in fact, during the first few days of infection (day 12 PS), parasitemia progressed more rapidly in probiotics-treated group B compared to the infected control. Studies reporting worse outcome of disease conditions associated with probiotic treatments are few. Treatments with some probiotic strains enhanced susceptibility to cryptosporidiosis in mice [47], and exacerbated chronic colitis by depression of neutrophil mobilization in murine models [48]. In this study, it is conceivable that during the early stages of the infection, treatment with the probiotic mix may have worsened the immunity and consequently aggravated the parasitemia in group B. This, however, remains to be proven bearing in mind that other probiotics-treated groups and the infected control had similar levels of parasitemia. With respect to levels of parasitemia, this finding contrasts reports [11,12,13,14,15] by several workers on the subject of use of probiotics in hemoparasitosis.
The similar nitric oxide (NO) levels recorded on day 7 PS in naïve probiotics-treated groups, as well as the uninfected control, suggest that treatments with the probiotic strains do not, on their own, elicit any meaningful change in NO levels in vivo. Following infection, why the NO levels continued to rise in group B (infected +5 billion CFU probiotics) is unclear; however, what is obvious is that other probiotic-treated groups had relatively lower NO levels and lower parasitaemia. A cursory look at the pattern of the NO and parasitemia levels in all the experimental groups suggests some degree of direct correlation between the two parameters; nonetheless, this remains to be established. It appears that higher NO levels may be associated with more severe parasitemia and pathologies in animal trypanosomosis contrary to what is seen with many other infectious diseases. Sternberg et al. [49] showed that the inhibition of NO production in vivo results in reduced parasitemia in Trypanosoma spp. infection. Beschin et al. [50] also reported the immunosuppressive effect of NO in early stages of trypanosomosis which resulted in high parasitemia. In Plasmodium chaubodi infection of mice, Martinez-Gomez et al. [46] reported significantly higher levels of nitric oxide and reduced parasitemia in the probiotics-treated groups when compared to the controls; however, their findings may be attributed to the distinctiveness of the hemoparasite, probiotic strains, and experimental animal models used. It has been noted that while NO acts to eliminate invading pathogens in various infections [51], it mediates immunosuppression in trypanosomosis [49, 50].
When parasitemia peaked in the infected groups, and all the experimental groups were challenged with a heterologous immunogen, the antibody titer thus elicited was similar across all the infected groups, notwithstanding treatments with probiotics. Lower levels of agglutinins to heterologous immunogens in trypanosome-infected animals compared to the control groups have been reported by several workers [52, 53], and this agrees with our findings. Probiotics strains could improve immunocompetence by stimulating general non-specific immunity, and by enhancing both innate and specific immune functions [54, 55]. Eze et al. [15] reported that supplementation of rat diet with Saccharomyces cerevisiae resulted in an increase in antibody titer to sheep erythrocytes, which decreased upon the establishment of Trypanosoma brucei infection; in addition, the supplemented groups maintained a significantly higher antibody titer than both the uninfected and infected controls. In this study, across the infected groups, no significant variation in mean antibody titer was noted as revealed by a one-time direct hemagglutination test (DHAT) by day 23 PS. Further, DHAT was practically impossible due to the onset of mortalities in the infected groups, and surviving animals were humanely sacrificed by day 25 PS due to severe illness. Although the uninfected control had significantly higher titer as at day 23 PS, it is conceivable that further stimulation with the antigen may have been necessary to elicit elevated antibody titers in infected groups bearing in mind that anamnestic response is a well-established concept in immunology [56, 57]. In addition, the route of probiotics administration to rats in this study may have affected the level of humoral immune responses recorded in probiotics-treated groups. It has been shown that mice that received Lactobacillus casei intraperitoneally showed a slightly better resistance to Babesia microti infection when compared to mice that were treated orally [12]. Additional and more narrowed studies may be warranted on this subject using the probiotic strains.
By day seven of supplementation with probiotics, the total and differential leukocyte counts, total erythrocyte count (TEC), and mean packed cell volumes (PCV) of rats in all the experimental groups did not show any meaningful disparity. This agrees with previous reports that treatment with probiotics did not result in any significant variation in hematological parameters of rats [58], and of broilers [59]. Following infection, both the probiotics-treated groups and the infected control had significantly lower PCV, TEC, and differential and total leukocyte counts, which were below the reference ranges [60]; hence, trypanosomosis-induced anemia and leukopenia had set in. Anemia and leukopenia characterized by neutropenia, lymphopenia, eosinopenia, and monocytosis are typically seen in animal trypanosomosis [1, 2, 4]. The mean absolute lymphocyte and neutrophil counts followed a similar pattern with the mean total leukocyte counts. Basophils are hardly ever seen in mammalian blood and were not detected in this study. It appears, therefore, that treatments with the probiotic strains neither improved nor depressed the hematopoietic systems of rats suffering trypanosomosis.
In conclusion, treatments with the probiotic strains gave a creatinine-lowering effect in trypanosomosis and were innocuous to the hematopoietic system; however, our findings on the pre-patent period, parasitemia, leukocyte counts, nitric oxide level, and antibody titer levels clearly indicate that treatment with the probiotic strains was not sufficiently immunostimulatory in Trypanosoma brucei infection of rats. It appears the presence and bioactivities of the probiotic strains do not positively interfere with the pathogenesis and development of immunosuppression in trypanosomosis. The biological meaning of the findings above is that with respect to Trypanosoma brucei infections, treatments with the probiotic mix do not enhance immunity; however, the creatinine-lowering effect thus elicited could be of clinical significance, and studying the underlying mechanism(s) of this effect may satisfy future research interests.
References
Reddy BS, Kumari KN, Sivajothi S, Rayulu VC (2016) Haemato-biochemical and thyroxin status in Trypanosoma evansi infected dogs. J Parasit Dis 40:491–495
Anene BM, Chukwu CC, Anika SM (1989) Immunosuppression of humoral immune response in canine trypanosomosis. Microbios Letters 40:37–46
Vincendeau P, Bouteille B (2006) Immunology and immunopathology of African trypanosom iasis. Ann Braz Acad Sci 78:645–665
Nweze NE, Okoro HO, Robaian MA, Omar RMK, Tor-Anyiin TA, Watson DG, Igoli JO (2017) Effects of Nigerian red propolis in rats infected with Trypanosoma brucei brucei. Comp Clin Pathol 26:1129–1133
Eze JI, Ajanwachukwu N, Animoke PC, Onoja SO, Anosa GN, Eze UU (2016) Immune response, anaemia and oxidative stress in Trypanosoma brucei brucei infected rats fed vitamin E supplemented diet. Anti-Infective Agents 14:28–37
Geerts S, Holmes PH, Eisler MC, Diall O (2001) African bovine trypanosomiasis: the problem of drug resistance. Trends Parasitol 17:25–28
Rathore NS, Manuja A, Kumar Manuja B, Choudhary S (2016) Chemotherapeutic approaches against Trypanosoma evansi: retrospective analysis, current status and future outlook. Curr Top Med Chem 16:2316–2327
Giordani F, Morrison LJ, Rowan TG, De Koning HP, Barrett MP (2016) The animal trypanosomiasis and their chemotherapy: a review. Parasitology 143:1862–1889
Laskowska E, Jarosz LS, Gradzki Z (2018) Effect of the EM Bokashi® multimicrobial probiotic preparation on the non-specific immune response in pigs. Probiotic Antimicro Prot. https://doi.org/10.1007/s12602-018-9460-5
Yousefi B, Eslami M, Ghasemian A, Kokhaei P, Salek-Farrokhi A, Darabi N (2019) Probiotics importance and their immunomodulatory properties. J Cell Physiol 234:8008–8018
Villarino NF, LeCleir GR, Denny JE, Dearth SP, Harding CL, Sloan SS et al (2016) Composition of the gut microbiota modulates the severity of malaria. PNAS 113:2235–2240
Bautista-Garfias CR, Gomez MB, Aguilar BR, Ixta O, Martinez F, Mosqueda J (2005) The treatment of mice with Lactobacillus casei induces protection against Babesia microti infection. Parasitol Res 97:472–477
Bautista-Garfias CR, Sandoval A, Aguilar BR (2008) Effect of high- and low-molecular-weight components of Lactobacillus casei on resistance against Babesia microti in NIH mice. Ann N Y Acad Sci 1149:152–154
Bautista-Garfias CR, Alvarez M, Martínez-Gómez F (2008) The inoculation of Lactobacillus casei in NIH mice induces a protective response against Trypanosoma cruzi (ninoa strain) infection. Vet Mex 39:139–144
Eze JI, Orajaka LJE, Okonkwo NC, Ezeh IO, Ezema C, Anosa GN (2012) Effect of probiotic (Saccharomyces cerevisiae) supplementation on immune response in Trypanosoma brucei brucei infected rats. Exp Parasitol 132:434–439
Majlesi M, Shekarforoush SS, Ghaisari HR, Nazifi S, Sajedianfard J, Eskandari MH (2017) Effects of probiotic Bacillus coagulans and Lactobacillus plantarum on alleviation of mecury toxicity in rats. Probiotics Antimicr Prot 9:300–309
Lutgendorff F, Trulsson LM, Van Minnen LP, Rijkers GT, Timmerman HM, Franzen LE et al (2008) Probiotics enhance pancreatic glutathione biosynthesis and reduce oxidative stress in experimental acute pancreatitis. Am J Physiol Gastrointest Liver Physiol 295:G1111–G1121
Travers MA, Florent I, Kohl L, Grellier P (2011) Probiotics for the control of parasites: an overview. J Parasitol Res 2011:610769. https://doi.org/10.1155/2011/610769
Raghuvanshi R, Chaudhari A, Kumar GN (2016) Amelioration of cadmium-and mercury-induced liver and kidney damage in rats by genetically engineered probiotic Escherichia coli Nissle 1917 producing pyrroquinoline quinine with oral supplementation of citric acid. Nutrition 32:1285–1294
Chang HY, Chen JH, Chang JH, Lin HC, Lin CY, Peng CC (2017) Multiple strains probiotics appear to be the most effective probiotics in the prevention of necrotizing enterocolitis and mortality: an updated meta-analysis. PLoS One 12:e0171579. https://doi.org/10.1371/journal.pone.0171579
Chapman CM, Gibson GR, Rowland I (2011) Health benefits of probiotics: are mixtures more effective than single strains? Eur J Nutr 50:1–17
Meng H, Lee Y, Ba Z, Peng J, Lin J, Boyer AS, Fleming JA, Furumoto EJ, Roberts RF, Kris-Etherton PM, Rogers CJ (2016) Consumption of Bifidobacterium animalis subsp. lactis BB-12 impacts upper respiratory tract infection and the function of NK and T cells in healthy adults. Mol Nutr Food Res 60:1161–1171
Arenas-Padilla M, Duarte-Gutierrez JL, Mata-Haro V (2018) Bifidobacterium animalis ssp. lactis Bb12 induces IL-10 through cell membrane-associated components via TLR2 in swine. J Appl Microbiol 125:1881–1889
Tabasco R, Garcia-Cayuela T, Pelaez C, Requena T (2009) Lactobacillus acidophilus La-5 increases lactacin B production when it senses live target bacteria. Int J Food Microbiol 132:109–116
Amdekar S, Singh V, Kumar A, Sharma P, Singh R (2013) Lactobacillus casei and Lactobacillus acidophilus regulate inflammatory pathway and improve antioxidant status in collagen-induced arthritic rats. J Interf Cytokine Res 33:1–8
Patel B, Kumar P, Banerjee R, Basu M, Pal A, Samanta M, Das S (2016) Lactobacillus acidophilus attenuates Aeromonas hydrophila induced cytotoxicity in catla thymus macrophages by modulating oxidative stress and inflammation. Mol Immunol 75:69–83
Herve-Jimenez L, Guillouard I, Guedon E, Boudebbouze S, Hols P, Monnet V, Maguin E, Rul F (2009) Postgenomic analysis of Streptococcus thermophilus cocultivated in milk with Lactobacillus delbrueckii subsp. bulgaricus: involvement of nitrogen, purine, and iron metabolism. Appl Environ Microbiol 75:2062–2073
Guha D, Banerjee A, Mukherjee R, Pradhan B, Peneva M, Aleksandrov G, Suklabaidya S, Senapati S, Aich P (2019) A probiotic formulation containing Lactobacillus bulgaricus DWT1 inhibits tumor growth by activating pro-inflammatory responses in macrophages. J Funct Foods 56:232–245
Kim HS, Chae HS, Jeong SC, Ham JS, Im SK, Ahn CN, Lee JM (2005) Antioxidant activity of some yogurt starter cultures. Asian-Australas J Anim Sci 18:255–258
De Palencia PF, Lopez P, Corbi AL, Pelaez C, Requena T (2008) Probiotic strains: survival under simulated gastrointestinal conditions, in vitro adhesion to Caco-2 cells and effect on cytokine secretion. Eur Food Res Technol 227:1475–1484
Zhang H, Sun J, Liu X, Hong C, Zhu Y, Liu A, Li S, Guo H, Ren F (2013) Lactobacillus paracasei subsp. paracasei LC01 positively modulates intestinal microflora in healthy young adults. J Microbiol 51:777–782
Sreeja V, Prajapati JB (2013) Probiotic formulations: application and status as pharmaceuticals—a review. Probiotics Antimicro Prot 5:81–91
Hajifaraji M, Jahanjou F, Abbasalizadeh F, Aghamohammadzadeh N, Abbasi MM, Dolatkhah N (2018) Effect of probiotic supplements in women with gestational diabetes mellitus on inflammation and oxidative stress biomarkers: a randomized clinical trial. Asia Pac J Clin Nutr 7:581–591
NIH (2011) Guide for the care and use of laboratory animals. National Academy Press, Washington DC
Herbert WJ, Lumsden WHR (1976) Trypanosoma brucei: a rapid “matching” method for estimating the host’s parasitemia. Exp Parasitol 40:427–431
Green LC, Wagner DA, Glogowski J, Skipper PL, Wishnok JS, Tannenbaum SR (1982) Analysis of nitrate, nitrite, and (15n) nitrate in biological fluids. Anal Biochem 126:131–138
Coles EH (1986) Veterinary clinical pathology. WB Saunders, Philadelphia
Thrall MA, Weiser MG (2002) Hematology laboratory procedures for veterinary technicians. Mosby Incorporated, Missouri
Ikeme MM, Adelaja AO (1990) Effect of the timing of antigen stimulation on parasitaemia profile and subsequent immunodepression in an experimentally induced Trypanosoma brucei infection. RevE˙ lev Med Vet Pays Trop 43:331–336
Welch BL (1951) On the comparison of several mean values: an alternative approach. Biometrika 38:933–943
Bush BM Interpretation of laboratory results for small animal clinicians. Blackwell Scientific Publication, London
Taylor K, Authie EM (2004) Pathogenesis of animal trypanosomiasis. In: Maudlin I, Holmes PH, Miles M A. (eds.) The trypanosomiases. Cab International, Wallingford, pp331–353
Akpa PO, Ezeokonkwo RC, Eze CA, Anene BM (2008) Comparative efficacy assessment of pentamidine isethionate and diminazene aceturate in the chemotherapy of Trypanosoma brucei brucei infection in dogs. Vet Parasitol 151:139–149
Sengul E, Gelen SU, Yildinm S, Celebi F, Cinar A (2019) Probiotic bacteria attenuates cisplatin-induced nephrotoxicity through modulation of oxidative stress, inflammation and apoptosis in rats. Asian Pac J Trop Biomed 9:116–122
Gupta V, Garg R (2009) Probiotics. Indian J Med Microbiol 27:202–209
Martinez-Gomez F, Ixta-Rodriguez O, Aguilar-Figueroa B, Hernandez-Cruz R, Monroy-Ostria A (2006) Lactobacillus casei ssp. rhamnosus enhances non specific protection against Plasmodium chabaudi in mice. Salud Publica Mex 48:498–503
Oliveira BCM, Widmer G (2018) Probiotic product enhances susceptibility of mice to cryptosporidiosis. Appl Environ Microbiol 84:e01408–e01418
Zheng B, van Bergenhenegouwen J, van de Kant HJG, Folkert G, Garsesen J, Vos AP, Morgan ME, Kraneveld AD (2016) Specific probiotic dietary supplementation leads to different effects during remission and relapse in murine chronic colitis. Benefic Microbes 7:205–213
Sternberg J, Mabbott N, Sutherland I, Liew FY (1994) Inhibition of nitric oxide synthesis leads to reduced parasitemia in murine Trypanosoma brucei infection. Infect Immun 62:2135–2137
Beschin A, Brys L, Magez S, Radwanska M, De Baetselier P (1998) Trypanosoma brucei infection elicits nitric oxide-dependent and nitric oxide-independent suppressive mechanisms. J Leukoc Biol 63:429–439
De Groote MA, Fang FC (1995) NO inhibitions: antimicrobial properties of nitric oxide. Clin Infect Dis 21:S162–S165
Goodwin LG, Green DG, Guy MW, Voller A (1972) Immunosuppression during trypanosomiasis. Br J Exp Pathol 53:40–43
Roelants GE, Pinder M (1984) Immunobiology of African trypanosomiasis. In: Marchalonis JJ (ed) Immunobiology of parasites and parasitic infections. Springer, Boston MA, pp 225–274
Fang H, Elina T, Heikki A, Seppo S (2000) Modulation of humoral immune response through probiotic intake. FEMS Immunol Med Microbiol 29:47–52
Famularo G, Moretti S, Marcellini S, Simone CD (1997). Stimulation of immunity by probiotics. In: Fuller R (ed.) Probiotics 2. Springer, Dordrecht, pp133–161
Jonker EF, Visser LG (2017) Single visit rabies pre-exposure priming induces a robust anamnestic antibody response after simulated post-exposure vaccination: results of a dose-finding study. J Travel Med 24:1–8
Lightowler MW, Donadeu M, Elaiyaraja M, Maithal K, Kumar KA, Gauci CG, Firestone SM, Sarasola P, Rowan TG (2016) Ananmnestic responses in pigs to the Taenia solium TSOL 18 vaccine and implications for control strategies. Parasitology 143:416–420
Anukam KC, Osazuwa EO, Reid G, Ozolua RI (2004) Feeding probiotic strains Lactobacillus rhamnosus gr-1 and Lactobacillus fermentum RC-14 does not significantly alter hematological parameters of Sprague-dawley rats. Haema 7:497–501
Alkhalf A, Alhaj M, Al-homidan I (2010) Influence of probiotic supplementation on blood parameters and growth performance in chickens. Saudi J Biol Sci 17:219–225
Ihedioha JI, Okafor C, Ihedioha TE (2004) The hematological profile of the Sprague-dawley outbred albino rat in Nsukka, Nigeria. Anim Res Int 1:125–132
Acknowledgments
We are grateful to the staff of Veterinary Medicine Laboratory, University of Nigeria for their technical support, and to CHR® (Netherland) for providing us with the probiotic strains used in the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Statement
All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Okolo, C.C., Nweze, N.E. & Eze, I.J. Hematobiochemical and Immunological Responses of Rats Treated with Multi-strain Probiotics and Infected with Trypanosoma brucei. Probiotics & Antimicro. Prot. 12, 952–960 (2020). https://doi.org/10.1007/s12602-019-09592-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12602-019-09592-z