
Abstract
Youth who experience aggression at the hands of peers are at an increased risk for a variety of adjustment difficulties, including depressive and anxiety symptoms and lower self-esteem. The links between peer victimization and internalizing problems are robust, but less work has been done to identify individual-level protective factors that might mitigate these outcomes. The current study investigated whether hope served as a moderator of the prospective links from peer victimization to depressive and anxiety symptoms and self-esteem during adolescence. Participants included 166 high school students (64% female; 88% Black/African American). Youth completed self-report measures at three different time points across the Spring semester of an academic year. As predicted, hope interacted with peer victimization to predict changes in depressive and anxiety symptoms over the course of the semester. That is, for youth with low levels of hope, peer victimization predicted more stable patterns of depressive and anxiety symptoms. For adolescents with average levels of hope, however, peer victimization did not influence anxiety and depressive symptoms over time. Finally, for adolescents with high levels of hope, peer victimization predicted greater decreases in anxiety symptoms over time. Hope did not interact with peer victimization to predict self-esteem. Rather, hope uniquely predicted higher levels of self-esteem, whereas peer victimization uniquely predicted lower levels of self-esteem. The current study provides initial support for the notion that hope can serve as a protective factor among youth who are victims of peer aggression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Peer victimization, or the experience of aggressive acts by peers, is common among youth and is associated with a host of negative psychosocial outcomes, including internalizing problems (i.e., emotional problems associated with anxiety and depressive disorders), that can persist throughout the lifespan (McDougall & Vaillancourt, 2015; Reijntjes et al., 2010). Given the negative outcomes that are associated with peer victimization and their potential lasting effects, it is important to identify protective factors that might mitigate these associations. Hope—a cognitive, motivational set comprised of goals, motivation to achieve goals, and the strategies developed to achieve a goal—is best conceptualized as a trait variable that has been shown to be related to a host of important psychosocial outcomes (Snyder, 2002; Snyder et al., 2003). Among youth, higher levels of hope are associated with lower internalizing problems as well as higher levels of self-esteem (e.g., Vacek et al., 2010; Valle et al., 2006). There is also some evidence to suggest that hope may serve as a protective factor in the face of stressful life events (e.g., Valle et al., 2006). Therefore, the goal of the current short-term longitudinal study was to examine whether hope moderates the prospective associations between peer victimization and internalizing symptoms over a 4-month period during adolescence.
Peer Victimization
Peer victimization is a troubling and pervasive problem among youth today. In fact, one longitudinal study found that 24% of children experienced chronic victimization from kindergarten through 12th grade (Ladd et al., 2017). Adolescents who are victimized by peers are at an increased risk for a variety of negative psychosocial outcomes, including depression, anxiety, suicidal ideation, conduct problems, lower school performance, and a negative attitude toward school (Halliday et al., 2021). Experiences of victimization can be physical (i.e., being hit, kicked, pushed, chased, or threatened by a peer; Crick et al., 1999) or relational (i.e., experiencing an attempt by a peer to damage one’s social relationships or status through behaviors such as gossip, rumor spreading, and ostracism; Crick & Gropter, 1996). Many youth, however, experience both physical and relational victimization simultaneously (Casper & Card, 2016; Nylund et al., 2007), and prior work has shown that adolescents perceive different forms of victimization as equally distressing (Nishina & Juvonen, 2005). Additionally, physical and relational victimization both make similar contributions to the prediction of youth’s daily and long-term adjustment (e.g., Nishina & Juvonen, 2005; Rudolph et al., 2014); thus, the impact of peer victimization may best be understood by considering its frequency rather than its specific forms.
Youth who experience peer victimization are more likely to exhibit symptoms of depression and anxiety, and evidence suggests that these effects can persist over time (McDougall & Vaillancourt, 2015; Reijntjes et al., 2010). For example, one longitudinal study found that youth who reported victimization in 5th grade showed higher levels of depressive symptoms in 10th grade (Bogart et al., 2014). Other findings have demonstrated that peer victimization predicts subsequent increases in anxiety symptoms (Lewis & Araya, 2014; Stapinski et al., 2015). Furthermore, youth who are victimized during childhood and adolescence are more likely to be diagnosed with either a depressive or anxiety disorder in young adulthood (Copeland et al., 2013; Lewis & Araya, 2014).
Prior work has shown that internalizing problems and self-esteem are significantly associated (Sowislo & Orth, 2013; Steiger et al., 2015), with evidence suggesting that there is a bidirectional association between these constructs (Saint-Georges & Vaillancourt, 2020). Further, evidence also indicates that there are transactional associations between peer victimization, self-esteem, and internalizing problems (Saint-Georges & Vaillancourt, 2020). That is, Saint-Georges and Vaillancourt (2020) found evidence of a cascading model whereby lower self-esteem predicted increases in depressive symptoms, which predicted subsequent increases peer victimization. Additionally, lower self-esteem predicted increases in depressive symptoms (Saint-Georges & Vaillancourt, 2020). Peer victimization may also have a negative impact on self-esteem (van Geel et al., 2018). That is, youth who are victimized by peers are more likely to exhibit lower self-esteem both concurrently (Malecki et al., 2015; Tsaousis, 2016; Salmivalli & Isaacs, 2005) and over time (Bogart et al., 2014; Boulton et al., 2010; Overbeek et al., 2010; van Geel et al., 2018). In fact, previous studies have shown that children and adolescents who experienced peer victimization had lower global self-worth and perceptions of social acceptance 6-months later (Boulton et al., 2010) and lower self-esteem 1 year later (Overbeek et al., 2010). Moreover, a recent meta-analysis with 16,230 youth showed that peer victimization was associated with decreased self-esteem over time (van Geel et al., 2018). Taken together, there is a need for additional research to identify protective factors that may buffer youth from the harmful effects of peer victimization on internalizing problems over time.
Hope
Hope can be conceptualized as a cognitive, motivational set that is comprised of goals, agency thinking, and pathways thinking (Snyder, 1994; 2002). Goals reflect the mental endpoints of purposeful behavior and are considered to be the anchors of hope theory. One can have short-term goals (e.g., going for a 10-minute walk), or long-term goals that require more planning and initiative (e.g., running a marathon). Further, goals can either stand-alone, or they can be subgoals of a larger, more complex goal (e.g., running a mile before running a marathon). Agency thinking involves the motivation required to initiate or sustain movement toward a goal, whereas pathways thinking refers to the routes that are developed in order to meet a goal. For example, if one had a goal of getting into college, pathways thinking would involve determining the routes needed to meet that goal, such as studying for standardized exams, doing well in school, and getting letters of recommendation from teachers. Agency thinking, on the other hand, involves having the motivation and self-talk needed for goal attainment.
According to Snyder (2002), individuals with higher levels of hope tend to generate more goals, are more likely to persist in their pursuit of a goal in the face of obstacles, and are more likely to develop alternative pathways to achieve a goal if one route is blocked. Furthermore, high-hope individuals are more likely to focus on successes rather than failures while in pursuit of a goal (Snyder, 2002). Hope theory also suggests that the perception about the attainment of goals is a driving force behind emotional experiences. In other words, perceptions of movement towards one’s goal or goal attainment can contribute to positive emotions, while unsuccessful goal pursuit contributes to negative emotions (Snyder, 2002). Similarly, an individual with low levels of hope is more likely to experience negative emotions, especially when goal attainment is hindered or blocked (Snyder, 2002).
Hope, although similar, is conceptually distinct from the construct of optimism, (i.e., a cross-situational expectation for positive outcomes; Scheier & Carver, 1985; 1987). Specifically, hope theory may better explain human’s goal-directed cognitions and behaviors (Snyder, 1995). Optimistic individuals may have positive beliefs about achieving a goal, which is similar to agency thinking; however, they may lack pathways cognitions (i.e., the routes that one develops to achieve their goals), which are important for goal attainment (Snyder, 1995). Hope can also be distinguished from self-efficacy. Specifically, self-efficacy theory (Bandura, 1977; 1989) suggests that there are two types of expectancies in a situation: outcome expectancies (i.e., belief in whether a behavior can achieve an outcome) and efficacy expectancies (i.e., belief that one is able to engage in the behavior needed to achieve the outcome). Outcome expectancies and efficacy expectancies are related to pathways thinking and agency thinking, respectively. However, efficacy expectancies are conceptualized as being situation specific, whereas hope theory suggests that these components are inherent to the individual apply across situations (Snyder, 1995). Further, hope theory suggests that both pathways and agency thinking are necessary for goal achievement, whereas self-efficacy theory places greater emphasis on efficacy expectancies (Snyder, 1995).
Hopeful thinking is associated with more adaptive functioning across the lifespan. For example, hope is positively associated with greater academic achievement, higher levels of perceived competence and self-esteem, and lower levels of depressive and anxiety symptoms among children and adolescents (Dixson et al., 2017; Halama & Dedova, 2007; Lewis & Kliewer, 1996; Snyder et al., 1997). Higher hope has also been linked to higher life satisfaction, (Valle et al., 2006), better social adjustment with family and friends (Kwon, 2002), greater perceived social support (Barnum et al., 1998), better academic functioning, and more school engagement (Marques et al., 2015). Similarly, compared to their low-hope counterparts, adults with higher levels of hope report fewer depressive and anxiety symptoms (Snyder et al., 1991), better academic (Chang, 1998) and athletic (Curry et al., 1997) performance in college, and higher life satisfaction (Chang, 1998).
Hope may be especially important in situations where an individual experiences environmental stressors, and some research suggests that hope serves as a protective factor against the negative outcomes associated with adverse life experiences (Valle et al., 2006; Visser et al., 2013). One investigation found that hope attenuated the effects of negative life events on depressive symptoms among a diverse sample of college students (Visser et al., 2013). In other words, high-hope individuals showed fewer depressive symptoms after experiencing negative life events. In another cross-sectional study, results showed that among youth with lower levels of hope, life satisfaction was lower for adolescents who experienced a greater number of stressful life events; for adolescents with higher levels of hope, however, life satisfaction was not associated with the number of stressful life events (Valle et al., 2006). This study also found that low-hope individuals were more likely to exhibit internalizing problems when they experienced stressful life events, whereas there was no association between stressful life events and internalizing problems for high-hope individuals. Finally, previous research has shown that hope was associated with lower levels of internalizing and externalizing problems in a sample of children whose mothers were incarcerated, even after controlling for social support and stress (Hagen et al., 2005). Taken together, there is some preliminary evidence to support the notion that hope may buffer the negative outcomes associated with experiences of peer victimization.
The Current Study
The majority of prior research on peer victimization has focused on the negative psychosocial outcomes associated with these experiences (e.g., Halliday et al., 2021) or predictors of peer aggression and victimization (e.g., Oncioiu et al., 2020). Comparatively less is known, however, regarding individual-level factors that are protective for youth who experience peer aggression. One recent study investigated whether a positive future orientation—a conceptually related but distinct concept from hope—moderated the association between peer victimization and internalizing problems among a sample of African American adolescents (Hong et al., 2021). Results indicated that a positive future orientation did not interact with peer victimization when internalizing problems was the outcome variable. However, a positive future orientation buffered the effects of peer victimization on suicidal ideation and peer aggression. It should be noted that this study was cross-sectional, and it is important to identify individual-level factors that moderate the prospective links from peer victimization to internalizing problems over time. The current study sought to address this gap in the literature by being the first study to examine whether hope moderated the longitudinal associations between peer victimization and internalizing problems. The identification of intrapersonal strengths that buffer the negative effects associated with peer victimization could serve as a potential target for prevention and intervention efforts. Additionally, given that peer victimization during adolescence is not uncommon (e.g., Kann et al., 2018), and the negative psychosocial outcomes stemming from this interpersonal stressor can persist into adulthood (Lewis & Araya, 2014; McDougal & Vaillancourt, 2015; Stapinski et al., 2015), it is important to identify protective factors during this crucial period of development. Based on the fact that hope has previously been found to buffer the negative outcomes associated with stressful life events (Valle et al., 2006; Visser et al., 2013), we hypothesized that hope would attenuate the prospective links from peer victimization to depressive symptoms, anxiety symptoms, and self-esteem.
Method
Participants
Participants for the study included 166 adolescents (64% girls) from a high school located in a large urban school district in the Southeastern United States. All students in grades 9–12 were eligible to participate (n = 420). During the fall semester, consent forms were sent home to caregivers. Three hundred and twenty-eight consent forms were returned (78%), and 322 caregivers provided consent for their child’s participation, which was approximately 76% of eligible adolescents. Adolescents also provided written assent prior to data collection. The overall participation rate of eligible students was 40%; data were missing for 36% of students who had transferred to another school or were absent on the days in which Time 1 data were collected. The final sample included 106 girls and 60 boys with ages ranging from 14 to 19 years (M = 15.86, SD = 1.22). Note that Time 1 outcome data were missing for two to four participants who completed the independent, but not the dependent, variable measure(s). Further, 30 participants were absent on the days in which data were collected at Time 2, 47 participants were absent at Time 3, and four participants did not complete one or more outcome measures at Time 3. A series of independent samples t-tests indicated that participants with missing outcome data did not differ from those with complete data on any independent or dependent variable at Time 1. Thus, these participants were retained in the final analyses.
The majority of participants self-identified as Black/African American (88%), 6% identified as Hispanic/Latinx, 3% identified as biracial/multiracial, and 3% identified as another race/ethnicity. Socioeconomic data were not collected for individual participants, but according to school records, 93% of all students were eligible for free or reduced-price lunch. At the time of data collection, the high school was located in a community in which 43% of families lived below the federal poverty line (US Census Bureau, 2011). Further, violent crime rates in the community were almost four times higher than the national average (Federal Bureau of Investigation, 2010–2014).
Procedure
The study was approved by the researchers’ and the school district’s Institutional Review Boards and by school administrators. Data were collected across three time points spanning a total of 4 months during the spring semester of an academic year. Data collection first took place in late January and early February (Time 1); due to time constraints, the peer victimization measure was administered 2–3 weeks after the other Time 1 study measures. Data were collected again in mid-March (Time 2), followed by a third round of data collection in mid-May (Time 3). Data collection took place during 50-minute study hall periods. Trained research assistants were present in each classroom to administer standardized instructions and answer any questions. To facilitate accurate responses and maintain confidentiality, no school staff or non-participating students were in the classrooms during data collection. The same procedures were employed across all time points. Of note, approximately 57% (n = 94) of participants took part in three brief informational sessions on goal setting following Time 1 data collection. However, participation in these sessions was not associated with changes in any study outcome variableFootnote 1, and therefore it was not included as a covariate in the subsequent analyses. All students were compensated for their participation with a t-shirt at the conclusion of the study.
Measures
Peer Victimization
The Revised Peer Experiences Questionnaire (RPEQ; Prinstein et al., 2001) is an 18-item self-report measure that was administered at Time 1. The current study utilized the 9-item victimization subscale, which measures physical (e.g., “A teen hit, kicked, or pushed me in a mean way”) and relational (e.g., “A teen gossiped about me so that others would not like me”) experiences of victimization. Participants were asked to rate how often each instance occurred on a 5-point scale ranging from 1 (Never) to 5 (Several Times a Week). Items were averaged, with higher scores indicating more frequent peer victimization. The RPEQ has shown to be a reliable and valid measure of peer victimization across a variety of samples (De Los Reyes & Prinstein, 2004; Queirós & Vagos, 2016). In the current study, the internal consistency for the measure was good (α = 0.85).
Hope
The Trait Hope Scale (HS; Snyder et al., 1991) is a 12-item self-report questionnaire that was administered at Time 1. The questionnaire consists of a 4-item pathways subscale (e.g., “There are lots of ways around any problem”), a 4-item agency subscale (e.g., “My past experiences have prepared me well for my future”), and 4 filler items. Participants were asked to rate each item on an 8-point scale that ranges from 1 (Definitely False) to 8 (Definitely True). The eight agency and pathways items were averaged, with higher scores indicating higher levels of hope. The HS has demonstrated good psychometric properties among a variety of different samples, including adolescents (Babyak et al., 1993; Snyder et al., 1991). Internal consistency for the measure in this sample was adequate (α = 0.71).
Depressive Symptoms
The Beck Depression Inventory, 2nd Edition (BDI-II) is a 21-item measure developed to assess depressive symptoms in adolescents and adults from ages 13 to 80 years (Beck et al., 1996). The BDI-II was administered at Times 1–3. Adolescents were asked to rate the extent to which each item described how they had felt during the past 2 weeks on a 4-point scale ranging from 0 to 3. Participants completed items that assessed different symptoms of depression, such as sadness, agitation, feelings of guilt, and loss of appetite. Items were averaged, with higher scores indicating higher depressive symptoms. Prior research suggests that this measure has demonstrated good psychometric properties among adolescent samples (Rausch et al., 2017). In this study, the BDI-II demonstrated good internal consistency (⍺’s = 0.85-0.93).
Anxiety Symptoms
The Multidimensional Anxiety Scale for Children-10 (MASC-10) is a 10-item self-report questionnaire developed to measure the physical symptoms of anxiety, social anxiety, harm avoidance, and separation anxiety among children between 8 and 19 years old (March, 1997). The MASC-10 was administered at Times 1–3. Youth rated items (e.g., “I’m afraid that other kids will make fun of me”) on a 4-point scale ranging from 0 (Never True About Me) to 3 (Often True About Me). Items were averaged, with higher scores indicating higher anxiety symptoms. Prior research suggests that this measure has demonstrated adequate psychometric properties among different samples, including adolescents (Osman et al., 2009; March et al., 1999). In this study, the MASC-10 demonstrated adequate internal consistency (⍺’s = 0.68 − 0.79).
Self-Esteem
The Rosenberg Self-Esteem Scale (RSES; Rosenberg, 1965) is a 10-item, widely used measure of personal beliefs about self-worth that was administered at Times 1–3. Respondents were asked to rate each item (e.g., “I feel that I have a number of good qualities”) on a 4-point scale ranging from 1 (Strongly Agree) to 4 (Strongly Disagree). Five items were reverse scored, and then all items were averaged, with higher scores indicating higher self-esteem. Prior research suggests that this measure has demonstrated good psychometric properties in adolescent samples (e.g., Bagley et al., 2001; Schmitt & Allik, 2005). In this study, the RSES demonstrated good internal consistency (⍺’s = 0.80-0.85).
Analytic Method
Descriptive statistics and bivariate correlations were first estimated using SPSS (Version 27). The moderating effects of hope on the prospective associations between peer victimization and internalizing symptoms were then examined by estimating a series of multilevel models within SAS (University Edition). Two-level models were specified, such that occasions at level 1 were nested within persons at level 2. Full-information maximum likelihood estimation was used to accommodate the missing outcomes at Times 1 (1–2%), 2 (18%), and 3 (28–31%), as this approach has been shown to provide less biased parameter estimates compared to other methods of handling missing data (Arbuckle, 1996). The significance of fixed effects was evaluated using Wald test p-values, and the significance of random effects was evaluated using likelihood ratio tests.
The continuous predictors—peer victimization and hope—were standardized prior to analyses to aid in the interpretation of their effects. Gender, age, and race were evaluated as potential covariates and were included in the multilevel models if they were significantly associated with one or more outcome variables at the bivariate level. Time in months was centered so that intercept corresponded to Time 1. Effect sizes were measured by calculating the proportion reduction in each variance component (i.e., random intercept variance and residual variance) and the total R 2 (i.e., squared correlation between the actual outcomes and the outcomes predicted by fixed effects in the models; see Hoffman, 2015). Finally, significant interactions were interpreted by calculating regions of significance for the moderator variable (Bauer & Curran, 2005).
Results
Preliminary Analyses
Descriptive statistics (i.e., M, SD, minimum, maximum) and bivariate correlations are presented in Table 1. Gender and race were included as covariates in the multilevel models given their significant associations with the internalizing problem outcomes. In contrast, age was not associated with outcome variables at any time point and was therefore not included as a covariate in the subsequent analyses. Of note, 73.5% of children reported having experienced at least one incident of peer victimization since the beginning of the school year at Time 1. A review of raw mean/sum scores revealed that adolescents’ experiences of peer victimization at Time 1 as measured by the RPEQ were comparable to a sample of adolescents from three large cities across the United States (i.e., 0.54 SD difference; Adrian et al., 2019). Additionally, adolescents had comparable levels of hope, as measured by the HS, to a sample of adolescents from urban and rural environments in the Midwest (i.e., 0.52 SD difference; Van Ryzin, 2011). With regard to depressive symptoms, the average BDI-II score in the current sample was similar to a sample of predominately Black/African American, low-income youth drawn from three large northeastern cities (i.e., 0.20 SD difference; Rausch et al., 2017). Adolescents in the current sample exhibited similar levels of anxiety symptoms, as measured by the MASC-10, as a large sample of low-income adolescents drawn from three large cities across the United States (i.e., 0.07 SD difference; Feldman et al., 2021). Finally, adolescents in the current sample reported similar levels of self-esteem, as measured by the RSES, in comparison to a sample of youth from two cities in the western United States (i.e., 0.93 SD difference; Fu et al., 2017).
Unconditional Multilevel Models
Empty means, random intercept models were initially estimated to partition the variance in internalizing symptoms across persons and time. For depressive symptoms, 45% of the total variance was due to person mean differences (i.e., random intercept variance), and 55% was due to within-person residual variance. Next, a fixed linear effect of time was added, which revealed significant decreases in depressive symptoms over the 4-month period, b = − 0.04, SE = 0.01, p < .001; this effect accounted for 6% of the level-1 residual variance. A random variance in the linear time slope (and its covariance with the random intercept) was added to examine individual differences in change over time, but this was not significant, − 2ΔLL (2) = 1.75, p = .41. Therefore, analyses proceeded using random intercept, fixed linear time slope models.
For anxiety symptoms, 51% of the total variance was due to person mean differences, and 49% was due to within-person residual variance. A fixed linear effect of time revealed significant decreases in anxiety symptoms over the 4-month period, b = − 0.04, SE = 0.01, p = .001, and this effect accounted for 5% of the level-1 residual variance. The random variance of the linear time slope was nonsignificant, − 2ΔLL (2) = 3.83, p = .15, so the analyses proceeded using random intercept, fixed linear time slope models.
For self-esteem, 51% of the total variance was due to person mean differences, and 49% was due to within-person residual variance. A fixed linear effect of time revealed nonsignificant decreases in self-esteem over the 4-month period, b = − 0.02, SE = 0.01, p = .11, and this effect accounted for 1% of the level-1 residual variance. The random variance of the linear time slope was also nonsignificant, − 2ΔLL (2) = 1.39, p = .50. Accordingly, a series of alternative covariance structure models were evaluated to ensure appropriate tests of subsequent fixed effects (see Hoffman, 2015), and analyses proceeded using random intercept, 1-lag Toeplitz models.Footnote 2
Conditional Multilevel Models
Depressive Symptoms
Peer victimization, hope, and gender were added as time-invariant predictors of the intercept and linear time slope (see Table 2). Gender was negatively associated with the random intercept and positively associated with the linear time slope, such that boys exhibited lower initial levels of depressive symptoms and more stable patterns of symptoms over time as compared to girls. Further, higher levels of hope were related to lower concurrent depressive symptoms, whereas higher levels of peer victimization were related to higher concurrent depressive symptoms. Neither hope nor peer victimization were associated with the linear time slope. Relative to the previous unconditional model for change, the main effects model accounted for an additional 33% of the level-2 random intercept variance and 7% of the level-1 residual variance for a total R 2 = 0.20.
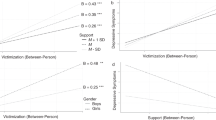
A two-way interaction between peer victimization and hope predicting the intercept and linear time slope (see Table 2) was then added to the model. Hope significantly moderated peer victimization in predicting the linear time slope, but not the random intercept. As shown in Fig. 1a, peer victimization predicted smaller decreases in depressive symptoms over time for children with hope ≤ − 0.50 SD (lower bound) and greater decreases in depressive symptoms over time for children with hope ≥ + 2.71 SD (upper bound); it should be noted, however, that the upper bound fell beyond the limits of the current data. This model accounted for an additional 2% of the level-2 random intercept variance and 2% of the level-1 residual variance for a total ΔR 2 = 0.02.

Interactive Effects of Peer Victimization and Hope on Depressive and Anxiety Symptoms
Anxiety Symptoms
When time-invariant predictors were added to the model (see Table 3), gender was negatively associated with the random intercept, but not the linear time slope, such that boys exhibited lower initial levels of anxiety symptoms as compared to girls. Neither peer victimization nor hope was associated with the random intercept or the linear time slope. This model accounted for an additional 20% of the level-2 random intercept variance and 1% of the level-1 residual variance for a total R 2 = 0.12.
When the two-way interaction was added to the model (see Table 3), hope significantly moderated peer victimization in predicting the linear time slope, but not the random intercept. As shown in Fig. 1b, peer victimization predicted smaller decreases in anxiety symptoms over time for children with hope ≤ − 0.90 SD (lower bound) and greater decreases in anxiety symptoms over time for children with hope ≥ + 1.37 SD (upper bound). This model accounted for an additional 1% of the level-2 random intercept variance and 3% of the level-1 residual variance for a total ΔR 2 = 0.02.
Self-Esteem
When time-invariant predictors were added to the model (see Table 4), race, but not gender, was significantly associated with the random intercept; specifically, Black/African American participants exhibited higher levels of self-esteem over time as compared to participants who self-identified as another race. Higher levels of hope were related to higher levels of self-esteem over time, whereas higher levels of peer victimization were related to lower levels of self-esteem over time. This model accounted for an additional 38% of the random intercept variance for a total R 2 = 0.19. When the two-way interaction was added to the model (see Table 4), hope did not significantly moderate peer victimization in predicting the random intercept. This model accounted for an additional 1% of the random intercept variance for a total ΔR 2 = 0.01.
Discussion
Ample research suggests that peer victimization is an adverse experience that contributes to poor psychosocial outcomes, including increased symptoms of depression and anxiety (e.g., Halliday et al., 2021; Reijntjes et al., 2010) and lower self-esteem (e.g., Tsaousis, 2016). However, less work has been done to identify factors that might protect youth from these harmful outcomes. This study aimed to address this gap in the literature by being the first study to investigate whether the prospective associations between peer victimization and internalizing problems would differ depending on adolescents’ trait hope. The current findings provide initial support for the notion that hope may serve as an individual-level protective factor against the deleterious effects of peer victimization. Further, the current sample was comparable on all of the variables of interest to a number of other samples drawn from large cities across the United States, which suggests that the current findings could be generalizable to other adolescent samples.
In line with past research (McDougal & Vaillancourt, 2015; Reijntjes et al., 2010; Valle et al., 2006; Visser et al., 2013), we found that peer victimization was associated with higher concurrent depressive symptoms, whereas hope was associated with lower concurrent depressive symptoms. Additionally, we found that depressive and anxiety symptoms decreased over the course of the semester. These findings mirror previous work that has shown that the vast majority of youth experience low levels of internalizing symptoms, which tend to decrease over time (Allan et al., 2014; Hatoum et al., 2018). Further, consistent with expectations and previous work demonstrating that hope buffers the negative effects associated with stressful life events (Valle et al., 2006; Visser et al., 2013), we found that hope mitigated the longitudinal impact of peer victimization on depressive and anxiety symptoms. That is, peer victimization was not associated with increases in depressive or anxiety symptoms for adolescents with moderate to high levels of hope, whereas victimization predicted more stable and problematic patterns of symptoms over time for those with low levels of hope. Further, among adolescents with very high levels of hope (i.e., greater than 1.52 standard deviations above the mean), peer victimization actually predicted greater decreases in anxiety symptoms over time. Contrary to our hypothesis, hope did not moderate the link between peer victimization and self-esteem. However, in line with previous work (e.g., Dixon et al., 2017; Halama & Dedova, 2007; Tsaousis, 2016), we found that hope was uniquely associated with higher levels of self-esteem, whereas peer victimization was uniquely associated with lower levels of self-esteem over time.
These findings can be understood through a framework of resilience. More specifically, Luthar and colleagues (2000) suggest that certain personality characteristics or attributes may confer protective effects for individuals in the face of adversity, and they theorized that there were four patterns of protective factors in terms of risk status and adjustment. The first pattern, simply termed “protective,” describes a factor with a direct positive effect on adjustment that is independent from, and does not interact with, risk status. In the second pattern, labeled “protective-stabilizing,” high levels of the protective factor serve to prevent a change in functioning across both high and low levels of risk; that is, the personality attribute provides a stabilizing function regardless of the intensity of the stressor. The third pattern, “protective-enhancing,” refers to an interactive process in which adjustment difficulties decrease with increasing risk at high levels of the protective factor (i.e., the factor yields added benefits at higher levels of risk). The fourth pattern is termed “protective-reactive” and describes a factor that confers advantages primarily at low levels of risk.
In the current study, hope served as a protective factor for self-esteem. Specifically, youth who had higher levels of hope exhibited higher self-esteem over time, regardless of their experiences of peer victimization. In contrast, hope had a protective-stabilizing effect on depressive and anxiety symptoms, whereby peer victimization did not confer risk for adolescents with moderate to high levels of this factor; instead, these individuals exhibited declines in symptoms over time. Surprisingly, very high levels of hope provided a protective-enhancing effect for anxiety symptoms, such that peer victimization predicted greater decreases in symptoms over time.
Why might youth with higher levels of hope not be adversely impacted by peer victimization? Previous research has shown that youth who are the targets of peer aggression may be more likely to develop self-blaming attributions when trying to explain the causes of their victimization (e.g., “It must be something about me”; Graham & Juvonen, 1998). According to attribution theory (Weiner, 1985), causes of events that are perceived as being internal, stable, and uncontrollable are more likely to contribute to poor psychosocial outcomes. In fact, prior work has shown that self-blaming attributions help explain the link between peer victimization and internalizing problems (Betts et al., 2017; Chen & Graham, 2012; Graham & Juvonen, 1998). On the other hand, when the causes of events are perceived as being external, they are more likely to be perceived as controllable, which can increase motivation to address and resolve the situation (Graham & Juvonen, 1998; Weiner, 1985).
Snyder (2002) posited that high-hope individuals are more likely to persist in the pursuit of a goal when presented with external obstacles. In addition, high levels of hope are characterized by the development of multiple pathways to achieve a goal (Snyder, 2002). It may be the case that youth with higher levels of hope are more likely to view peer victimization as an obstacle that is caused by external factors (e.g., characteristics of the perpetrator) and not an internal characteristic. Therefore, hope may protect individuals from developing self-blaming attributions for experiences of victimization, which subsequently lead to symptoms of depression and anxiety. The benefits of hope may also be due to the fact that individuals with higher hope are more likely to identify and engage in adaptive coping strategies when faced with stressors (Hagen et al., 2005); this could explain why such youth exhibited greater decreases in anxiety symptoms over time at higher levels of peer victimization.
Limitations and Directions for Future Research
These findings must be considered in light of the study’s limitations. First, the reliance on self-report measures could contribute to shared method variance. Prior work has shown that adolescents are reliable informants of their experiences of victimization because they are able to identify instances that others might not be aware of (Olweus, 1991); however, other work suggests that teacher- and peer-reports of peer victimization provide additional information (e.g., Branson & Cornell, 2009; Graham et al., 2003). Thus, future research should utilize a multi-informant approach to bolster the validity of findings. Second, despite the longitudinal design of the study, the time period under investigation (i.e., 4 months) was relatively brief. It would be informative for future investigations to examine the influence of hope on the prospective associations between peer victimization and internalizing problems over longer intervals and during different developmental periods, such as early adolescence. Future research should also extend these results by examining the protective role of other psychological strengths (e.g., humor, gratitude, etc.).
Summary
In conclusion, findings of the current study suggests that hope may serve as a protective factor in the context of peer victimization. That is, adolescents who experienced more frequent victimization and had lower levels of hope showed more stable patterns of depressive and anxiety symptoms over time. In contrast, peer victimization was not prospectively associated with depressive or anxiety symptoms for adolescents who had moderate to high levels of hope; these youth saw a decline in symptoms over time. Adolescents with very high levels of hope, however, showed greater declines in anxiety symptoms when they experienced more frequent peer victimization. Finally, more frequent experiences of victimization were uniquely associated with lower self-esteem, whereas higher levels of hope predicted higher self-esteem over time.
These findings build on previous work by identifying an individual trait (i.e., hope) that serves as a psychological strength and might confer benefits for youth who are experiencing peer victimization. This is important because youth who experience this interpersonal stressor are at an increased risk for a multitude of negative psychosocial outcomes (e.g., Halliday et al., 2021). A better understanding of factors that might reduce these risks could be important for interventions designed to address the mental health needs of peer-victimized youth. Although hope is considered dispositional in nature, evidence suggests that changes in hopeful thinking can occur through prevention programs (e.g., Marques et al., 2011) and mental health interventions (e.g., Ritschel et al., 2016). Additional research is needed to investigate whether efforts to foster hopeful thinking might contribute to a reduction in depressive and anxiety symptoms for adolescents who experience peer victimization.
Availability of data and material
The data for the current project are available from the authors upon request.
Code Availability
Not applicable.
Notes
Participation in the information sessions on goal setting did not predict change in depressive symptoms (b = –0.01, SE = 0.02, p = .68), anxiety symptoms (b = –0.02, SE = 0.02, p = .31), or self-esteem (b = –0.06, SE = 0.07, p = .38).
Given that systematic change in self-esteem was not observed, a series of alternative covariance structure models were evaluated according to the procedures outlined by Hoffman (2015). Specifically, compound symmetry, first-order auto-regressive, and Toeplitz models were sequentially estimated. At the request of a reviewer, fixed effect analyses were re-run using unstructured covariance models, and the pattern of findings remained unchanged.
References
Adrian, M., Jenness, J. L., Kuehn, K. S., Smith, M. R., & Mclaughlin, K. A. (2019). Emotion regulation processes linking peer victimization to anxiety and depression symptoms in adolescence. Development and Psychopathology, 31(3), 999–1009. https://doi.org/10.1017/s0954579419000543
Allan, N. P., Capron, D. W., Lejuez, C. W., Reynolds, E. K., Macpherson, L., & Schmidt, N. B. (2014). Developmental trajectories of anxiety symptoms in early adolescence: The influence of anxiety sensitivity. Journal of Abnormal Child Psychology, 42(4), 589–600. https://doi.org/10.1007/s10802-013-9806-0
Arbuckle, J. L. (1996). Full information estimation in the presence of incomplete data. In G. A (a. Marcoulides, & Shumaker, R. E. (Eds.). Advanced structural equation modeling: Issues and techniques (pp.243–277).Lawrence Erlbaum Associates, Inc>The reference: (Arbuckle 1996) is present in the reference section but not in the text. Could you please check? There was a typo in the name. It has been corrected. This citation can be found in the Analytic Method section.
Babyak, M. A., Snyder, C. R., & Yoshinobu, L. (1993). Psychometric properties of the Hope Scale: A confirmatory factor analysis. Journal of Research in Personality, 27(2), 154–169. https://doi.org/10.1006/jrpe.1993.1011
Bagley, C., & Mallick, K. (2001). Normative Data and Mental Health Construct Validity for the Rosenberg Self-Esteem Scale in British Adolescents. International Journal of Adolescence and Youth, 9(2–3), 117–126. https://doi.org/10.1080/02673843.2001.9747871
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavior change. Psychological Review, 84, 191–215. https://doi.org/10.1016/0146-6402(78)90002-4
Bandura, A. (1989). Human agency in social cognitive theory. American Psychologist, 44, 1175–1184. https://doi.org/10.1037/0003-066X.44.9.1175
Barnum, D. D., Snyder, C. R., Rapoff, M. A., Mani, M. M., & Thompson, R. (1998). Hope and social support in psychological adjustment of children who have survived burn injuries and their matched controls. Children’s Health Care, 27(1), 15–30. https://doi.org/10.1207/s15326888chc2701_2
Bauer, D., & Curran, P. J. (2005). Probing interactions in fixed and multilevel regression. (a. Inferential and graphical techniques.Multivariate Behavioral Research, 40(3),373–400, b. https://doi.org/10.1207/s15327906mbr4003_5
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II. San Antonio: Psychological Corporation
Betts, L. R., Houston, J. E., Steer, O. L., & Gardner, S. E. (2017). Adolescents’ experiences of victimization: The role of attribution style and generalized trust. Journal of School Violence, 16(1), 25–48. https://doi.org/10.1080/15388220.2015.1100117
Bogart, L. M., Elliott, M. N., Klein, D. J., Tortolero, S. R., Mrug, S., Peskin, M. F. … Schuster, M. A. (2014). Peer victimization in fifth grade and health in tenth grade. Pediatrics, 133(3), 440–447. https://doi.org/10.1542/peds.2013-3510
Boulton, M. J., Smith, P. K., & Cowie, H. (2010). Short-term longitudinal relationships between children’s peer victimization/bullying experiences and self-perceptions. School Psychology International, 31(3), 296–311. https://doi.org/10.1177/0143034310362329
Branson, C. E., & Cornell, D. G. (2009). A comparison of self and peer reports in the assessment of middle school bullying. Journal of Applied School Psychology, 25(1), 5–27. https://doi.org/10.1080/15377900802484133
Casper, D. M., & Card, N. A. (2016). Overt and relational victimization: A meta-analytic review of their overlap and associations with psychological adjustment. Child Development, 88(2), 466–483. https://doi.org/10.1111/cdev.12621
Chang, E. C. (1998). Hope, problem-solving ability, and coping in a college student population: Some implications for theory and practice. Journal of Clinical Psychology, 54(7), 953–962. https://doi.org/10.1002/(SICI)1097-4679(199811)54:7<953::AID-JCLP9>3.0.CO;2-F
Chen, X., & Graham, S. (2012). Close relationships and attributions for peer victimization among late adolescents. Journal of Adolescence, 35(6), 1547–1556. https://doi.org/10.1016/j.adolescence.2012.06.003
Copeland, W. E., Wolke, D., Angold, A., & Costello, E. J. (2013). Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry, 70(4), 419. https://doi.org/10.1001/jamapsychiatry.2013.504
Crick, N. R., & Grotpeter, J. K. (1996). Children’s treatment by peers: Victims of relational and overt aggression. Development and Psychopathology, 8(2), 367–380. https://doi.org/10.1017/S0954579400007148
Crick, N. R., Casas, J. F., & Ku, H. C. (1999). Relational and physical forms of peer victimization in preschool. Developmental Psychology, 35(2), 376–385. https://doi.org/10.1037/0012-1649.35.2.376
Curry, L. A., Snyder, C. R., Cook, D. L., Ruby, B. C., & Rehm, M. (1997). Role of hope in academic and sport achievement. Journal of Personality and Social Psychology, 73(6), 1257–1267. https://doi.org/10.1037/0022-3514.73.6.1257
De Los Reyes, A., & Prinstein, M. J. (2004). Applying depression-distortion hypotheses to the assessment of peer victimization in adolescents. Journal of Clinical Child & Adolescent Psychology, 33(2), 325–335. https://doi.org/10.1207/s15374424jccp3302_14
Dixson, D. D., Worrell, F. C., & Mello, Z. (2017). Profiles of hope: How clusters of hope relate to school variables. Learning and Individual Differences, 59, 55–64. https://doi.org/10.1016/j.lindif.2017.08.011
Federal Bureau of Investigation (2010–2014). FBI Uniform Crime Reporting Program. https://www.fbi.gov/services/cjis/ucr
Feldman, J. S., Zhou, Y., Krug, W., Wilson, C., Lemery-Chalfant, M. N., K., & Shaw, D. S. (2021). Extracurricular involvement in the school-age period and adolescent problem behavior among low-income youth. Journal of Consulting and Clinical Psychology, 89(11), 947–955. https://doi.org/10.1037/ccp0000685. https://doi-org.lib-e2.lib.ttu.edu/
Fu, X., Padilla-Walker, L. M., & Brown, M. N. (2017). Longitudinal relations between adolescents’ self-esteem and prosocial behavior toward strangers, friends and family. Journal of Adolescence, 57, 90–98. https://doi.org/10.1016/j.adolescence.2017.04.002
Graham, S., Bellmore, A., & Juvonen, J. (2003). Peer victimization in middle school: When self- and peer views diverge. Journal of Applied School Psychology, 19(2), 117–137. https://doi.org/10.1300/j008v19n02_08
Graham, S., & Juvonen, J. (1998). Self-blame and peer victimization in middle school: An attributional analysis. Developmental Psychology, 34(3), 587–599. https://doi.org/10.1037/0012-1649.34.3.587
Hagen, K. A., Myers, B. J., & Mackintosh, V. H. (2005). Hope, social support, and behavior problems in at-risk children. American Journal of Orthopsychiatry, 75(2), 211–219. https://doi.org/10.1037/0002-9432.75.2.0
Halama, P., & Dedová, M. (2007). Meaning in life and hope as predictors of positive mental health: Do they explain residual variance not predicted by personality traits? Studia Psychologica, 49(3), 191–200. https://www.proquest.com/scholarly-journals/meaning-life-hope-as-predictors-positive-mental/docview/226905080/se-2?accountid=7098
Halliday, S., Gregory, T., Taylor, A., Digenis, C., & Turnbull, D. (2021). The impact of bullying victimization in early adolescence on subsequent psychosocial and academic outcomes across the adolescent period: A systematic review. Journal of School Violence, 20(3), 351–373. https://doi.org/10.1080/15388220.2021.1913598
Hatoum, A. S., Rhee, S. H., Corley, R. P., Hewitt, J. K., & Friedman, N. P. (2018). Etiology of stability and growth of internalizing and externalizing behavior problems across childhood and adolescence. Behavior Genetics, 48(4), 298–314. https://doi.org/10.1007/s10519-018-9900-8
Hoffman, L. (2015). Longitudinal analysis: Modeling within-person fluctuation and change New York, NY:Routledge
Hong, J. S., Choi, J., Albdour, M., Willis, T. M., Kim, J., & Voisin, D. R. (2021). Future orientation and adverse outcomes of peer victimization among African American adolescents. Journal of Aggression, Maltreatment, & Trauma, 30(4), 528–546. https://doi.org/10.1080/10926771.2020.1759747
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Queen, B. … Ethier, K. A. (2018). Youth Risk Behavior Surveillance - United States, 2017. MMWR Surveillance Summaries, 67(8), 1–114. https://doi-org.lib-e2.lib.ttu.edu/https://doi.org/10.15585/mmwr.ss6708a1
Kwon, P. (2002). Hope, defense mechanisms, and adjustment: Implications for false hope and defensive hopelessness. Journal of Personality, 70(2), 207–231. https://doi.org/10.1111/1467-6494.05003
Ladd, G. W., Ettekal, I., & Kochenderfer-Ladd, B. (2017). Peer victimization trajectories from kindergarten through high school: Differential pathways for children’s school engagement and achievement. Journal of Educational Psychology, 109(6), 826–841. https://doi.org/10.1037/edu0000177
Lewis, G., & Araya, R. (2014). Peer victimization during adolescence and risk for anxiety disorders in adulthood: A prospective cohort study. Depression and Anxiety, 31(7), 574–582. https://doi.org/10.1002/da.22270
Lewis, H. A., & Kliewer, W. (1996). Hope, coping, and adjustment among children with sickle cell disease: Tests of mediator and moderator models. Journal of Pediatric Psychology, 21(1), 25–41. https://doi.org/10.1093/jpepsy/21.1.25
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–562. https://www.jstor.org/stable/1132374
Malecki, C. K., Demaray, M. K., Coyle, S., Geosling, R., Rueger, S. Y., & Becker, L. D. (2015). Frequency, power differential, and intentionality and the relationship to anxiety, depression, and self-esteem for victims of bullying. Child & Youth Care Forum, 44(1), 115–131. https://doi.org/10.1007/s10566-014-9273-y
March, J. S. (1997). MASC: multidimensional anxiety scale for children. New York: Multi-Health Systems Inc
March, J. S., Sullivan, K., & Parker, J. (1999). Test-retest reliability of the multidimensional anxiety scale for children. Journal of Anxiety Disorders, 13(4), 349–358. https://doi.org/10.1016/s0887-6185(99)00009-2
Marques, S. C., Lopez, S. J., & Pais-Ribeiro, J. L. (2011). “Building hope for the future”: A program to foster strengths in middle-school students. Journal of Happiness Studies: An Interdisciplinary Forum on Subjective Well-Being, 12(1), 139–152. https://doi.org/10.1007/s10902-009-9180-3
Marques, S. C., Lopez, S. J., Fontaine, A. M., Coimbra, S., & Mitchell, J. (2015). How much hope is enough? Levels of hope and students’ psychological and school functioning. Psychology in the Schools, 52(4), https://doi.org/10.1002/pits.21833
McDougall, P., & Vaillancourt, T. (2015). Long-term adult outcomes of peer victimization in childhood and adolescence: Pathways to adjustment and maladjustment. American Psychologist, 70(4), 300–310. https://doi.org/10.1037/a0039174. https://doi-org.lib-e2.lib.ttu.edu/
Nishina, A., & Juvonen, J. (2005).Daily reports of witnessing and experiencing peer harassment in middle school. Child Development, 76, 435–450 https://doi.org/10.1111/j.1467-8624.2005.00855.x
Nylund, K., Bellmore, A., Nishina, A., & Graham, S. (2007). Subtypes, Severity, and Structural Stability of Peer Victimization: What Does Latent Class Analysis Say? Child Development, 78(6), 1706–1722. https://doi.org/10.1111/j.1467-8624.2007.01097.x
Olweus, D. (1991). Bully/victim problems among schoolchildren: Basic facts and effects of a school-based intervention program. In D. Pepler & K. Rubin (Eds.) The development and treatment of childhood aggression (1st ed., pp. 411–448). Psychology Press. https://doi.org/10.4324/9780203771693
Oncioiu, S. I., Orri, M., Boivin, M., Geoffrow, M. C., Arseneault, L., Brendgen, M. … Cote, S. M. (2020). Early childhood factors associated with peer victimization trajectories from 6 to 17 years of age. Pediatrics, 145(5), 1–12. https://doi.org/10.1542/peds.2019-2654
Osman, A., Williams, J. E., Espenschade, K., Gutierrez, P. M., Bailey, J. R., & Chowdhry, O. (2009). Further evidence of the reliability and validity of the Multidimensional Anxiety Scale for Children (MASC) in psychiatric inpatient samples. Journal of Psychopathology and Behavioral Assessment, 31(3), 202–214. https://doi.org/10.1007/s10862-008-9095-z
Overbeek, G., Zeevalkink, H., Vermulst, A., & Scholte, R. H. (2010). Peer victimization, self-esteem, and ego resilience types in adolescents: A prospective analysis of person‐context interactions. Social Development, 19(2), 270–284. https://doi.org/10.1111/j.1467-9507.2008.00535.x
Prinstein, M. J., Boergers, J., & Vernberg, E. M. (2001). Overt and relational aggression in adolescents: Social-psychological adjustment of aggressors and victims. Journal of Clinical Child & Adolescent Psychology, 30(4), 479–491. https://doi.org/10.1207/s15374424jccp3004_05
Queirós, A. N., & Vagos, P. (2016). Measures of aggression and victimization in Portuguese adolescents: Cross-cultural validation of the Revised Peer Experience Questionnaire. Psychological Assessment, 28(10), e141–e151. https://doi.org/10.1037/pas0000363
Rausch, E., Racz, S. J., Augenstein, T. M., Keeley, L., Lipton, M. F., Szollos, S. … De Los Reyes, A. (2017). A multi-informant approach to measuring depressive symptoms in clinical assessments of adolescent social anxiety using the Beck Depression Inventory-II: Convergent, incremental, and criterion-related validity. Child & Youth Care Forum, 46(5), 661–683. https://doi.org/10.1007/s10566-017-9403-4
Reijntjes, A., Kamphuis, J. H., Prinzie, P., & Telch, M. J. (2010). Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse & Neglect, 34(4), 244–252. https://doi.org/10.1016/j.chiabu.2009.07.009
Ritschel, L. A., Ramirez, C. L., Cooley, J. L., & Craighead, W. E. (2016). Behavioral activation for major depression in adolescents: Results from a pilot study. Clinical Psychology: Science and Practice, 23(1), 39–57. https://doi.org/10.1111/cpsp.12140
Rosenberg, M. (1965). Society and the adolescent child. Princeton, NJ: Princeton University Press
Rudolph, K. D., Troop-Gordon, W., Monti, J. D., & Miernicki, M. E. (2014). Moving against and away from the world: The adolescent legacy of peer victimization. Development and Psychopathology, 26(3), 721–734. https://doi.org/10.1017/s0954579414000340
Saint-Georges, Z., & Vaillancourt, T. (2020). The temporal sequence of depressive symptoms, peer victimization, and self-esteem across adolescence: Evidence for an integrated self-perception driven model. Development and Psychopathology, 32(3), 975–984. https://doi.org/10.1017/S0954579419000865
Salmivalli, C., & Isaacs, J. (2005). Prospective relations among victimization, rejection, friendlessness, and children’s self-and peer‐perceptions. Child Development, 76(6), 1161–1171. https://doi.org/10.1111/j.1467-8624.2005.00841.x-i1
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4, 219–247. https://doi.org/10.1037/0278-6133.4.3.219
Scheier, M. F., & Carver, C. S. (1987). Dispositional optimism and physical well-being: The influence of generalized outcome expectancies on health. Journal of Personality, 55, 169–210. https://doi.org/10.1111/j.1467-6494.1987.tb00434.x
Schmitt, D. P., & Allik, J. (2005). Simultaneous administration of the Rosenberg Self-Esteem Scale in 53 nations: Exploring the universal and culture-specific features of global self-esteem. Journal of Personality and Social Psychology, 89(4), 623–642. https://doi.org/10.1037/0022-3514.89.4.623
Snyder, C. R. (1994). Psychology of hope: You can get there from here. Simon & Schuster
Snyder, C. R. (1995). Conceptualizing, measuring, and nurturing hope. Journal of Counseling and Development: JCD, 73(3), 355. https://doi.org/10.1002/j.1556-6676.1995.tb01764.x
Snyder, C. R. (2002). Hope theory: Rainbows in the mind. Psychological Inquiry, 13(4), 249–275. https://doi.org/10.1207/S15327965PLI1304_01
Snyder, C. R., Cheavens, J., & Sympson, S. C. (1997). Hope: An individual motive for social commerce. Group Dynamics: Theory, Research, and Practice, 1(2), 107–118. https://doi.org/10.1037/1089-2699.1.2.107
Snyder, C. R., Harris, C., Anderson, J. R., Holleran, S. A., Irving, L. M., Sigmon, S. T. … Harney, P. (1991). The will and the ways: Development and validation of an individual-differences measure of hope. Journal of Personality and Social Psychology, 60(4), 570–585. https://doi.org/10.1037/0022-3514.60.4.570
Snyder, C. R., Lopez, S. J., Shorey, H. S., Rand, K. L., & Feldman, D. B. (2003). Hope theory, measurements, and applications to school psychology. School Psychology Quarterly, 18(2), 122–139. https://doi.org/10.1521/scpq.18.2.122.21854
Sowislo, J. F., & Orth, U. (2013). Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychological Bulletin, 139, 213–240. https://doi.org/10.1037/a0028931
Stapinski, L. A., Araya, R., Heron, J., Montgomery, A. A., & Stallard, P. (2015). Peer victimization during adolescence: Concurrent and prospective impact on symptoms of depression and anxiety. Anxiety, Stress, & Coping, 28(1), 105–120. https://doi.org/10.1080/10615806.2014.962023
Steiger, A. E., Fend, H. A., & Allemand, M. (2015). Testing the vulnerability and scar models of self-esteem and depressive symptoms from adolescence to middle adulthood and across generations. Developmental Psychology, 51, 236–247. https://doi.org/10.1037/a0038478
Tsaousis, I. (2016). The relationship of self-esteem to bullying perpetration and peer victimization among schoolchildren and adolescents: A meta-analytic review. Aggression and Violent Behavior, 31, 186–199. https://doi.org/10.1016/j.avb.2016.09.005
U. S. Department of Commerce, U. S. Census Bureau. (2011). QuickFacts. https://www.census.gov/quickfacts/fact/table/US/PST045219The reference: (Department of Commerce) is present in the reference section but not in the text. Could you please check?This citation is located in the Participants Section (US Census Bureau, 2011)
Vacek, K. R., Coyle, L. D., & Vera, E. M. (2010). Stress, self-esteem, hope, optimism, and well-being in urban, ethnic minority adolescents. Journal of Multicultural Counseling and Development, 38(2), 99–11. https://doi.org/10.1002/j.2161-1912.2010.tb00118.x
Valle, M. F., Huebner, S., & Suldo, S. M. (2006). An analysis of hope as a psychological strength. Journal of School Psychology, 44, 393–406. https://doi.org/10.1016/j.jsp.2006.03.005
Van Geel, M., Goemans, A., Zwaanswijk, W., Gini, G., & Vedder, P. (2018). Does peer victimization predict low self-esteem, or does low self-esteem predict peer victimization? Meta-analyses on longitudinal studies. Developmental Review, 49, 31–40. https://doi.org/10.1016/j.dr.2018.07.001
Van Ryzin, M. J. (2011). Protective factors at school: Reciprocal effects among adolescents’ perceptions of the school environment, engagement in learning, and hope. Journal of Youth and Adolescence, 40(12), 1568–1580. https://doi.org/10.1007/s10964-011-9637-7
Visser, P. L., Loess, P., Jeglic, E. L., & Hirsch, J. K. (2013). Hope as a moderator of negative life events and depressive symptoms in a diverse sample. Stress and Health: Journal of the International Society for the Investigation of Stress, 29(1), 82–88. https://doi.org/10.1002/smi.2433The reference: (Visser et al. 2013) is present in the reference section but not in the text. Could you please check?The year of this citation was listed incorrectly throughout the text. It was previously cited as Visser et al., 2012, but has since been updated to the correct citation, which is Visser et al., 2013.
Weiner, B. (1985). An attributional theory of achievement motivation and emotion. Psychological Review, 92(4), 548–573. https://doi.org/10.1037/0033-295X.92.4.548
Acknowledgements
The authors would like to thank all students, teachers, and school administrators who gave their time to participate in this study. We are also grateful to the many individuals involved with the Child and Adolescent Mood Program at the Emory University School of Medicine who assisted with the project.
Funding
This research was supported by a grant from the Emory Office of University-Community Partnerships and by the Brock Family Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed parental consent and youth assent were obtained from all individual participants included in the study.
Consent for publication
All authors consent to publication of this work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ricker, B.T., Cooley, J.L., Sanchez, C.R. et al. Prospective Associations Between Peer Victimization and Internalizing Symptoms in Adolescence: The Protective Role of Hope. J Psychopathol Behav Assess 44, 649–662 (2022). https://doi.org/10.1007/s10862-022-09966-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-022-09966-8