
Abstract
Commercially available polypropylene mesh is preferred in the developed countries during inguinal hernioplasty. Whereas, the mosquito net mesh is a safe and effective alternative in the developing countries such as India. To evaluate the safety and efficacy of mosquito net mesh as prosthesis in comparison with polypropylene mesh in inguinal hernia repair by Lichtenstein tension-free technique. A total of 60 patients presented with uncomplicated inguinal hernia were randomized into two groups: group A (mosquito net mesh) and group B (polypropylene mesh). Postoperatively, the Southampton scoring system was employed to assess the level of infection at the surgical site on days 3, 5, 7, and 10. The data obtained were analyzed using SPSS 20.0. The data were compared using Fisher’s exact test, chi-square test, and independent sample t test. P ≤ 0.05 was considered statistically significant. All the patients were men and majority were in the age-group of 51–60 years. Right-sided inguinal hernia was reported in most (30) of the patients. The rate of surgical site infection on postoperative day 3 (P = 1.000), 5 (P = 0.704), 7 (P = 0.612), and 10 (P = 1.000) were comparable in both groups A and B. The baseline characteristics, clinical presentations, and assessment of surgical site infection in both groups were comparable. Therefore, mosquito net mesh, as prosthesis for inguinal hernia repair, is equally safe and efficacious as polypropylene mesh.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Inguinal hernioplasty is a common procedure performed in adult men. Conventional surgical methods for the repair of hernias have a higher recurrence rate (15%). Whereas, the Lichtenstein tension-free repair with the use of a prosthetic mesh is associated with < 5% recurrence rates. In addition, the tension-free hernia repair substantially improves the patient’s health in particular and lifestyle in general [1].
Inguinal hernias constitute for 75% of the total abdominal wall hernias. Lifetime risk of inguinal hernia is reported to be 27% in men and 3% in women [2, 3]. The incidence rates with respect to the age of the patients is reported to be 11 per 10,000 cases between 16 and 24 years, and 200 per 10,000 cases in patients aged 75 years and more [2, 4]. The prevalence of inguinal hernia in India is estimated to be 1.79% [5].
Of late, the surgical procedures of choice include the Shouldice layered repair, Lichtenstein tension-free mesh repair, and laparoscopic repair [3]. The Lichtenstein tension-free mesh repair is considered to be the gold standard for hernioplasty in which the prosthetic mesh reinforces the area of weakness. The mesh aids in minimizing the amount of tension required to be applied on the abdominal wall to cover the hernia, thus leading to lower recurrence rates [6]. The commercially available polypropylene mesh is preferred in the developed countries [7, 8]. The mosquito net mesh (MNM) is as effective and safe alternative in the developing countries including India and Africa [9]. MNM is a copolymer of polypropylene and polyethylene, which are medically approved materials for human use [10].
Despite proven efficacy, worldwide use of MNM warrants more studies to support and encourage its use. Accordingly, the present study was intended to assess the safety of MNM as prosthesis in comparison with polypropylene mesh for Lichtenstein’s tension-free inguinal hernia repair with respect to infection rates.
Materials and Methods
Study Design
The study was conducted at the Department of General Surgery KLE’s Dr. Prabhakar Kore Hospital and Medical Research Centre, Belagavi. It was a hospital-based randomized controlled trial performed for 1 year from January 2015 to December 2015.
A total of 60 patients admitted to the Department of General Surgery were enrolled in the study. Patients aged 18–60 years presenting with uncomplicated inguinal hernia requiring mesh repair consenting for surgery were included in the study. Patients aged less than 18 years and more than 60 years, with history of recurrent inguinal hernia, chronic kidney disease, HIV, and other immunocompromized states were excluded from the study. Before the commencement of study, ethical clearance was obtained from the Institutional Ethical Committee. After explaining the purpose, procedures, risks, and benefits of the study, a written informed consent was obtained from all the participants. The data including, age, clinical signs and symptoms, and type of hernia were recorded in a predesigned and pretested proforma.
Instrumentation
At admission, all the patients were subjected to investigations such as complete blood count, random blood sugar, renal function tests, HIV/HbsAg, chest X-ray, and ECG. Patients were randomized sequentially into two groups of 30, groups A and B. Prior to the surgical intervention, intravenous (IV) ciprofloxacin 500 mg single dose was administered to patients. The surgical procedure employed in both groups was Lichtenstein tension-free mesh repair under spinal anesthesia. In group A, the patients underwent inguinal hernia repair with mosquito net mesh (Fig. 1a), whereas the inguinal hernia repair with commercially available polypropylene mesh was subjected in group B patients (Fig. 1b). The MNM was obtained from Bangalore Monofilaments Pvt. Ltd., and was cut into 7 1/2 cm × 15 cm size. Ethylene oxide was used to sterilize the mesh. The mesh was fixed by polypropylene 2-0 suture to reflected portion of inguinal ligament and conjoined tendon in both groups.

a Mosquito net mesh. b Polypropylene mesh
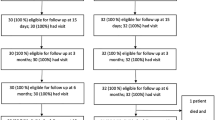
Postoperatively, all the patients were administered IV ciprofloxacin Q12th hourly for 1 day. Later on, the route of antibiotic administration was switched from IV to oral, and the patients received tablet ciprofloxacin 500 mg Q12th hourly for 3 days. In case of surgical site infection (SSI) development, patients were treated with antibiotics for a longer duration until the SSI subsided (Figs. 2 and 3).

Normal wound healing

Wound with surgical site infection
Postoperatively, the Southampton scoring system [11, 12] was employed to assess the level of infection at the surgical site on days 3, 5, 7, and 10. In infected patients, prolonged antibiotic administration was employed for the treatment.
Statistical Analysis
The data obtained were coded and entered in Microsoft excel spreadsheet, and analyzed using SPSS 20.0. The categorical data were expressed as rates, ratios, and percentages, and compared using Fisher’s exact test and chi-square test. Continuous data were expressed as mean ± standard deviation and compared using independent sample t test. P ≤ 0.050 was considered statistically significant.
Results and Discussion
All the patients in the study were men and majority were in the age-group 51–60 years. The patients were thoroughly examined on admission for duration of hernia, respiratory rate, pulse rate, systolic, and diastolic blood pressure (Table 1). With respect to the clinical presentation, swelling in the groin region was present in all the patients (60). Pain was observed in only some of the patients (17), whereas pallor was seen in majority of the patients (54). Mental retardation, as part of central nervous system functioning assessment, was absent in most of the patients (58); however, it was present in two of the patients. Majority of the patients had right-sided inguinal hernia (30), followed by left (21) and bilateral (9) hernias. Hypertension (7) and diabetes mellitus (4) were the comorbidities observed in the patients (Table 1).
Based on the Southampton scoring system, the level of surgical site infection was assessed. The grading was defined as bruising (grade Ia), mild erythema (grade Ic), erythema plus other signs of inflammation at only one point (grade IIa), erythema plus other signs of inflammation around sutures (grade IIb), clear or haemoserous discharge at only one point (< 2 cm; grade IIIa). The assessment of surgical site infection in the study population was recorded as shown in Table 2. Majority of the patients in both the study groups were free of SSIs on postoperative day 3 (86.67% vs. 83.33%; p = 1.000), 5 (86.67% vs. 86.67%; p = 0.704), 7 (96.67% vs. 90%; p = 0.6012), and 10 (100% vs. 96.67%; p = 1.000).
Postoperative SSI in group A and B was compared. It was observed that the rate of SSI in Leichtenstein tension-free mesh repair with MNM and polypropylene mesh was statistically comparable at days 3, 5, 7, and 10.
The present study has used the validated Southampton scoring system; however, previous studies have used different definitions of SSIs—superficial and deep SSIs. A randomized double-blind study by Freudenberg et al. [13] reported comparable results with no significant difference in the short-term clinical outcome of hernia treatment with MNM and the commercial mesh prosthesis, which holds resemblance to the present study.
In a study including 70 patients treated with MNM and nylon mesh, the findings were indicative of no evidence of immediate prosthesis infection or any medical condition postsurgery. However, hematoma of the surgical scar (4%) and incidence of superficial infection (3%) were reported in some of the patients. A 30-day follow-up demonstrated no major infection or rejection [14]. In another study, despite antibiotic prophylaxis, patients developed wound infection (5–8%) and hematoma (7%) 3 months after hernia treatment with Lichtenstein repair using commercial prosthetic mesh in developed countries such as Scotland [15].
Furthermore, Tongaonkar et al. in their 10-year experience of performing Lichtenstein hernia repair with MNM validated long-term safety and efficacy of MNM when compared with commercially available mesh, provided it is adequately sterilized [10]. Recently, Darokar et al. reported that the incidence of the serous discharge was more prominent in patients treated with polypropylene mesh (11.11%) when compared with MNM (5.41%). There was no incidence of superficial and deep infection, hematoma formation, and seroma formation in both the intervention groups. Sterilized MNM was determined as a safe and cost-effective alternative to commercial mesh [8].
In conclusion, MNM as prosthesis for Lichtenstein tension-free inguinal hernia mesh repair is safe in comparison with polypropylene mesh in terms of incidence of postoperative surgical site infection rates. However, further studies with respect to the long-term outcomes such as chronic pain, complications, and recurrence rates are required in large sample size for a longer study period.
References
Neumayer L, Giobbie-Hurder A, Jonasson O, Fitzgibbons R Jr, Dunlop D, Gibbs J, Reda D, Henderson W, Veterans Affairs Cooperative Studies Program 456 Investigators (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350(18):1819–1827
Jenkins JT, O’Dwyer PJ (2008) Inguinal hernias. Br Med J 336(7638):269–272
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362(9395):1561–1571
Devlin H (1995) Trends in hernia surgery in the land of Astley Cooper. Problems in Gen Surg 12:85–92
Kumar B, Madhusoodhanan N, Balaji A, Poornima M (2014) Prevalence and risk factors of inguinal hernia: a hospital based observational study. Int J Med Appl Sc 3(4):191–198
Gandhi D, Marcin S, Xin Z, Asha B, Kaswala D, Zamir B (2011) Chronic abdominal pain secondary to mesh erosion into cecum following incisional hernia repair: a case report and literature review. Ann Gastroenterol 24(4):321–324
Adesunkanmi ARK, Badmus TA, Ogundoyin O (2004) Determinants of outcome of inguinal herniorrhaphy in Nigerian patients. Surg Pract 8(1):14–21
Darokar A, Bele K, Mulmule R, Qazi R (2016) Study of open inguinal hernia repair by mosquito net mesh versus polypropylene mesh. Int J Res Med Sci 4(1):126–130
Stephenson B, Kingsnorth A (2011) Inguinal hernioplasty using mosquito net mesh in low income countries an alternative and cost effective prosthesis. Surgery: Br Med J 18:1237–1247
Tongaonkar RR, David L, Kingsnorth AN (2013) Ten-year personal experience of using low density polyethylene (LDPE) mesh for inguinal hernia repair. Trop Med Surg 1:136. https://doi.org/10.4172/2329-9088.1000136
Williams NS, Bailey H, Bulstrode CJ, Love RM, O’Connell PR (2008) Bailey & Love’s short practice of surgery. Crc Press, Boca Raton
Gottrup F, Melling A, Hollander DA (2005) An overview of surgical site infections: aetiology, incidence and risk factors. EWMA Journal 5(2):11–15
Freudenberg S, Sano D, Ouangré E, Weiss C, Wilhelm TJ (2006) Commercial mesh versus nylon mosquito net for hernia repair. A randomized double-blind study in Burkina Faso. World J Surg 30(10):1784–1789
Kiss A, Corona D, Kiss O (2012) The use of mosquito-net cloths as prosthesis in inguinal hernia repair: an experience in Southern Sudan. Surgical Science 3(03):155
Hair A, Duffy K, McLean J, Taylor S, Smith H, Walker A, Macintyre IMC, O'Dwyer PJ (2000) Groin hernia repair in Scotland. Br J Surg 87(12):1722–1726
Author information
Authors and Affiliations
Contributions
All authors contributed in the development of the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Pradhan, R., Pangi, A. Use of Mosquito Net Mesh Versus Polypropylene Mesh in Tension-Free Repair of Inguinal Hernia: a 1-Year Randomized Controlled Trial. Indian J Surg 82, 1063–1066 (2020). https://doi.org/10.1007/s12262-020-02216-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-020-02216-9