
Abstract
Experimental and epidemiologic studies indicated that calcium-sensing receptor (CaSR) polymorphisms were associated with cancer risk, yet no data are available for candidate gene and hepatocellular carcinoma (HCC) risk. To address this, we evaluated whether CaSR rs17251221 polymorphism is associated with HCC susceptibility, clinicopathological parameters, and prognosis in HCC patients treated by TACE. A TaqMan assay was used to genotype rs17251221 SNP in this case (n = 843)–control (n = 783) study. A significant increased risk of HCC was observed in patients carrying rs17251221 GG (adjusted OR 1.355, 95 % CI 1.024–1.793, P = 0.033), AG/GG genotype (adjusted OR 1.254, 95 % CI 1.007–1.561, P = 0.043), and G allele (adjusted OR 1.163, 95 % CI 1.013–1.335, P = 0.032). Furthermore, a significant association was found between Child-Pugh class, serum BCLC stage, and AFP level and rs17251221 genotypes. More importantly, individuals carrying rs17251221 AG, GG genotype showed significantly longer MST than AA genotype and significant hazard ration (AG: adjusted HR 0.484, 95 % CI 0.406–0.577, P < 0.001; GG: adjusted HR 0.633, 95 % CI 0.575–0.697, P < 0.001, respectively). Meanwhile, we found a favorable HR for AG/GG genotype carriers (adjusted HR 0.645, 95 % CI 0.542–0.768, P < 0.001). These results indicated that CaSR rs17251221 polymorphism is associated with susceptibility to HCC, and rs17251221 G allele genotype showed significant independent better prognosis of HCC patients treated with TACE.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related death and is the fifth most common malignant tumor that accounts for ~80 % of all liver cancer cases worldwide [1, 2]. Etiologically, hepatocarcinogenesis is a multistep, multifactor, complex process [3]. Currently, the multiple risk factors mainly included hepatitis B virus (HBV) or hepatitis C virus (HCV) infection, cirrhosis, carcinogen exposure, and especially genetic factors [4, 5]. Thus, substantial efforts should been made to identify genetic biomarkers as prognostic factors for improving therapeutic effect and prognosis prediction of HCC patients.
Calcium-sensing receptor (CaSR) was originally cloned from the bovine parathyroid gland in 1993 [6]. Subsequently, Canaff et al. [7] identified its expression in liver tissue and primary cultured hepatocytes. CASR gene located on chromosome 3p13.3–21, and encoded protein is a typical G protein coupled receptor with an extracellular domain, include a domain of seven membrane spanning and an unusually long intracellular carboxyl terminal tail [8, 9]. Generally, CaSR plays an important role in calcium homeostasis through regulation of parathyroid hormone secretion and calcium reabsorption [10, 11]. The rs17251221 SNP is located in the intron of the CaSR gene, and previous study revealed that rs17251221 polymorphism was strongly associated with serum calcium regulation in individuals of European and Indian-Asian descent [12]. Moreover, Chou et al. [13] revealed that the rs17251221 polymorphism was a susceptibility marker for stone multiplicity in nephrolithiasis. To data, only two studies investigated the association of CaSR rs17251221 genotypes with the susceptibility and survival of malignancies [14, 15]. One of the report found that CaSR (rs17251221) was strongly associated with prostate cancer [14]. Recent study further demonstrated that the genetic variations in the intron of CaSR gene rs17251221, a risk factor associated with breast cancer susceptibility, as well as a prognostic indicator [15]. However, the genetic effect of CaSR rs17251221 polymorphism on the susceptibility and prognosis of HCC is still unclear. Therefore, in this large prospective cohort, we analyzed the functional genetic polymorphisms of CaSR rs17251221 and attempted to elucidate the association between the polymorphisms and HCC susceptibility and clinical outcomes after FEM regimens treated with TACE. This study provides a theoretic basis for personalized chemotherapy in the treatment of HCC patients.
Materials and methods
Study subjects
We recruited 843 HCC patients newly diagnosed by cancer specialists consecutively from Shengjing Hospital of China Medical University and First Hospital of Dalian Medical University. This cohort of HCC patients was diagnosed based on histologic, combined with at least one positive HCC image on computed tomography (CT) or magnetic resonance imaging (MRI) and combined with serum AFP analysis (>400 ng/mL), and all HCC patients were untreated and shown not to have other cancers by an initial screening examination.
In this study, HCC typically are followed and monitored through their treatment regularly scheduled clinical and radiographic examinations. Preoperative serum tumor markers level included alpha fetoprotein (AFP). Clinical data were collected from medical records including sex, age, serum AFP, HBsAg marker, cirrhosis, tumor size, Child-Pugh class, TNM stage, and BCLC stage. All the patients (n = 843) received FEM (5-fluorouracil, epirubicin, mitomycin-C) regimen by transcatheter hepatic arterial chemoembolization (TACE) therapy. The FEM regimen consists of 5-fluorouracil (330 mg/m2, every week), adriamycin (30 mg/m2, every 4 weeks), and mitomycin (30 mg/m2, every 2 weeks). The treatment was given or switched to other chemotherapy until disease progression, or patient’s refusal to continue treatment.
We also included 783 unrelated healthy controls matched by gender and age. The controls had no known medical illness or hereditary disorders and were not taking any medications. The controls were recruited from individuals who visited the same hospitals for a health check-up. Before its commencement, this study was approved by the Research Ethics Committee of China Medical University and Dalian Medical University, and informed consent was obtained from each participant.
Genotyping assay
Genomic DNA was extracted from a leukocyte cell pellet of each blood sample using the TIANGEN DNA Blood Mini Kit (TIANGEN BIOTECH (Beijing) CO., LTD, Beijing, China) according to the manufacturer’s instructions. CaSR rs17251221 polymorphism was genotyped by TaqMan SNP Genotyping Assays on the ABI 7500 fast Real-Time PCR platform (Applied Biosystems, ABI Technologies, Carlsbad, CA, USA). The TaqMan probes were synthesized by Life Technology (Shanghai, China). The following amplification conditions were used: 95 °C for 10 min, 45 cycles of 92 °C for 15 s, 60 °C for 60 s, and 60 °C for 30 s. Samples and 10 % duplicate s were randomized and blinded for both cases and controls. There was 100 % concordance for both interplate and intraplate duplicates for rs17251221.
Statistical analysis
SPSS software package version 16.0 (SPSS Inc., Chicago, Illinois, USA) was used to analyze the data in this study. All tests were two-sided, and the criteria of statistical significance were set at P < 0.05. The chi-square (Pearson’s χ 2 test) or Fisher’s exact test was used to determine the differences in distributions of demographic, epidemiologic, and clinical variables between groups, and Hardy–Weinberg equilibrium test. Unconditional logistic regression models were used to analyze the association between the rs17251221 genotypes and HCC susceptibility, as well as clinicopathological parameters. The Disease-free survival (DFS) was taken from the date of diagnosis to the date of disease recurrence, progression, death without progression, or last follow-up. The overall survival (OS) was calculated as the time from diagnosis to liver cancer-related death or the date of last follow-up. The Kaplan–Meier method and the log-rank test were used to analyze the associations of the survival time with demographic characteristics, clinical features, and polymorphism. Multivariate Cox proportional hazards regression models were performed to obtain the adjusted hazard ratio (HR) and 95 % CI for potential prognostic factors for the survival in HCC patients.
Results
Demographic and baseline characteristics of the study subjects
The demographic characteristics and clinical variables of the HCC patients are summarized in Table 1. Totally, 843 patients with pathologically confirmed HCC and a group of 783 age- and gender-matched cancer-free healthy controls were included in this study. There were no significant differences in the distributions of gender and age between HCC patients and controls (P = 0.693 and P = 0.732, respectively). The age was matched between HCC patients (range 28–73 years; median 50 years) and controls (range 27–75 years; median 50 years). Among 843 patients, most of the patients were males (86.5 %), while 75.0 % of them had a chronic HBV infection. The vast majority of HCC patients (80.7 %) who had cirrhosis, and 69.8 % of the patients was classified into Child-Pugh A. All the HCC patients underwent the treatment of TACE. The variables of age, gender were adjusted for any residual confounding effects in later logistic regression analyses.
Association of CaSR rs17251221 polymorphism and HCC risk
The frequencies of allelic and genotype distribution for rs17251221 genetic variant in CaSR gene for both HCC patients and controls are shown in Table 2. The rs17251221 genotype frequency distribution in control group fit well to Hardy–Weinberg equilibrium (P = 0.738). We observed that the alleles and genotypes from rs17251221 genetic variant were statistically associated with the risk of HCC. There was statistically increased risk of HCC in the homozygote comparison (GG vs. AA: adjusted OR 1.355, 95 % CI 1.024–1.793, P = 0.033), recessive model (AG/GG vs. AA: adjusted OR 1.254, 95 % CI 1.007–1.561, P = 0.043), and allele comparison (G vs. A: adjusted OR 1.163, 95 % CI 1.013–1.335, P = 0.032). No significant difference was detected for HCC risk in heterozygote comparison (GA vs. AA: adjusted OR = 0.894, 95 % CI = 0.697–1.147, P = 0.379) and dominant model (GA/AA vs. GG: adjusted OR 0.837, 95 % CI 0.661–1.059, P = 0.137).
Interaction of CaSR rs17251221 polymorphism with different clinical parameters in HCC patients
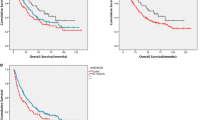
In case-only analysis (n = 843), we further investigated the interaction of CaSR rs17251221 polymorphism with clinicopathological characteristics or environmental risk factors such as HBsAg status, Cirrhosis using χ 2 test, and adjusted unconditional logistic regression adjusted by age and gender, shown in Table 3. We found that the distribution frequency of CaSR rs17251221 polymorphism was significantly associated with Child-Pugh class, BCLC stage, and serum AFP level. The frequency (81.2 %) of rs17251221 variants (AG/GG genotypes) in HCC patients with Child-Pugh class B was significantly higher than that (74.5 %) in those with Child-Pugh class A (adjusted OR 1.457, 95 % CI 1.010–2.100, P = 0.044), as shown in Table 3 and Fig. 1a. Furthermore, a higher frequency of rs17251221 AA genotype was observed in HCC patients with BCLC stage C (26.6 %) in comparison with those patients with BCLC stage A (67.5 %) (adjusted OR 0.389, 95 % CI 0.205–0.738, P = 0.004) (Table 3, Fig. 1b). There was a higher distribution frequency (26.8 %) of rs17251221 AA genotype was observed in serum AFP level (>400 ng/mL) than those HCC patients with lower serum AFP level (≤400 ng/mL) (adjusted OR 0.721, 95 % CI 0.523–0.995, P = 0.046) (Table 3; Fig. 1d). Moreover, the frequency distribution of rs17251221 genotypes in patients with different tumor size (cm) was shown in Fig. 1c, however, there was no association detected between the rs17251221 and tumor size (>5 vs. ≤5 cm) (adjusted OR 1.284, 95 % CI 0.930–1.772, P = 0.128). No significant interaction of rs17251221 polymorphism was found with other clinical characteristics.

Histogram and box plots illustrating the frequency distribution of rs17251221 genotypes and stratified clinicopathological characteristics. a Frequency distribution of rs17251221 genotypes classified by Child-Pugh classes (a, b). b Frequency distribution of rs17251221 genotypes classified by BCLC stage (a, b, c). c Mean tumor size (cm) (95 % CI) of HCC patients with rs17251221 genotypes (AG/GG, GG, AG, AA). d Median serum AFP level of HCC patients with rs17251221 genotypes (AG/GG, GG, AG, AA)
Effects of CaSR rs17251221 polymorphism on HCC survival
Kaplan–Meier method and log-rank test, multivariate Cox regression analysis were performed to further evaluate the correlations of CaSR rs17251221 polymorphism with the prognosis of HCC patients treated with FEM regimen by TACE therapy (n = 843).
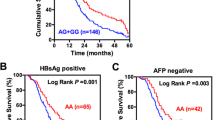
As shown in Fig. 2, a significant difference was observed between the OS of HCC patients and genotypes of rs17251221 (log-rank test: P < 0.001 in the different genotype and P < 0.001 in the recessive model, respectively). HCC patients carrying rs17251221 AG or GG genotype survived significantly longer OS time (AG genotype: median survival time, MST 22 months, 95 % CI 19–25 months, GG genotype: MST 31 months, 95 % CI 26–36 months, respectively) in comparison to the carriers who had AA genotype (MST 12 months, 95 % CI 8–14 months), as illustrated in Fig. 2a. Furthermore, multivariate Cox regression analysis also established that rs17251221 AG, GG genotypes as prognostic factors for longer OS time (AG genotype: adjusted HR 0.484, 95 % CI 0.406–0.577, P < 0.001; GG genotype: adjusted HR 0.633, 95 % CI 0.575–0.697, P < 0.001, respectively) adjusted by age, gender, child-Pugh class, tumor size, clinical stage, lymph node metastasis, serum tumor marker AFP level, outlined in Table 4. Then, in the recessive model, rs17251221 AG/GG genotype carriers (MST 27 months, 95 % CI 24–30 months; Fig. 2b) showed significantly prolonged OS time and also verified in multivariate Cox regression analysis (adjusted HR 0.645, 95 % CI 0.542–0.768, P < 0.001), as illustrated in Table 4. Moreover, after adjusted multivariate Cox regression analysis, we found that rs17251221 GG genotype showed predictive of better prognosis in DFS (adjusted HR 0.815, 95 % CI 0.668–0.995, P = 0.045), although there was no association in log-rank test. In addition, multivariate Cox regression analysis identified that tumor size (>5 cm), clinical stages (III or IV), lymph node metastasis status (Node-positive), and serum AFP level (>400 ng/mL) of HCC patients was found to be predictive of worse prognosis in PFS or OS (Table 4).

The relationship between the CaSR rs17251221 polymorphism and HCC prognosis according to Kaplan–Meier analysis. a CaSR rs17251221 AG, GG genotype had longer overall survival in HCC patients after FEM regimens treated with TACE (log-rank test: P < 0.001). b CaSR rs17251221 AG/GG genotypes had longer overall survival in HCC patients after FEM regimens treated with TACE (log-rank test: P < 0.001)
Discussion
The calcium-sensing receptor (CaSR), as an important regulator of calcium homeostasis, is expressed in all of the organs including liver [16, 17]. The inactivation or mutation of the CaSR gene usually leads to one of the several disorders of calcium metabolism [18–20]. Recent study further demonstrated that high dietary Ca2+ stimulate CaSR activation and could down-regulate cell proliferation, invasion, inhibit tumor development, and increase the chemotherapeutic sensitivity of cancer cells [21–24]. Furthermore, epidemiological study revealed the CaSR polymorphisms contribute to susceptibility for breast cancer [15]. Therefore, rs17251221 polymorphism may be a potential candidate functional SNP in HCC.
To further confirm the above hypothesis, we for the first time performed a case–control study to explore systematically the correlation of CaSR rs17251221 polymorphism with the susceptibility, clinicopathological parameters, and clinical outcomes of HCC patients after FEM regimen by TACE therapy. We found that rs17251221 AG/GG genotypes were associated with increased HCC susceptibility. These results are similar with the recent study [15] on breast cancer, reporting that patients with rs17251221 GG + AG genotypes were more likely to be increased risk for breast cancer than AA genotype carriers. More importantly, we further analyzed the relationship between rs17251221 polymorphism with clinicopathological parameters or environmental risk factors (HBsAg status, Cirrhosis status) and found that CaSR rs17251221 polymorphism was significantly associated with Child-Pugh class, BCLC stage, and serum AFP level, suggesting that rs17251221 polymorphism may be involved in the development of Child-Pugh class- and BCLC stage-associated HCC. This polymorphism may be used as a potential marker for identification of the malignant and invasive Child-Pugh class- and BCLC stage-associated HCC patients. However, we did not found any interaction with environmental risk factors such as HBsAg status and Cirrhosis status.
Little is known about regarding the CaSR rs17251221 polymorphism in terms of the potential impact on the cancer clinical outcomes. Thereafter, we further investigated the association of CaSR rs17251221 polymorphism with the survival time of HCC patients treated with TACE. It is worth to note that CaSR rs17251221 AG/GG genotypes were related to a significantly longer OS in our study, and multivariate analysis confirmed an independent favorable prognostic value of rs17251221 polymorphism in HCC patients treated by TACE. Similarly, in breast cancer [15], rs17251221 GG + AG genotypes were observed as prognostic indicators for both DFS and OS. However, further investigations are warranted to understand the precise mechanism of this polymorphism involved in different tumors in other areas or ethnicities.
To the best of our knowledge, our results firstly provide evidence that CaSR rs17251221 polymorphism is associated with susceptibility and therapeutic outcome in HCC patients treated with FEM chemotherapy by TACE therapy in a large and well-characterized cohort. These data suggest that CaSR rs17251221 polymorphism may play an important role in the development of HCC, and therefore, may be a vital prognostic indicator for HCC, and employed as a potential adjuvant in HCC patients for TACE therapy in the future.
Abbreviations
- CaSR :
-
Calcium-sensing receptor
- SNPs:
-
Single-nucleotide polymorphisms
- HCC:
-
Hepatocellular carcinoma
- HBV:
-
Hepatitis B virus
- HBsAg:
-
Hepatitis B surface antigen
- AFP:
-
Alpha fetoprotein
- MST:
-
Median survival time
- DFS:
-
Disease-free survival
- OS:
-
Overall survival
- FEM:
-
Regimen, 5-fluorouracil, epirubicin, and mitomycin-C
- TACE:
-
Transhepatic arterial chemotherapy and embolization
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
References
Njei B, Rotman Y, Ditah I, Lim JK. Emerging trends in hepatocellular carcinoma incidence and mortality. Hepatology. 2014. doi:10.1002/hep.27388.
Chen JG, Zhu J, Zhang YH, Chen YS, Ding LL, Lu JH, Zhu YR. Trends in the mortality of liver cancer in Qidong, China: an analysis of fifty years. Zhonghua Zhong Liu Za Zhi. 2012;34(7):532–7.
Ding J, Wang H. Multiple interactive factors in hepatocarcinogenesis. Cancer Lett. 2014;346(1):17–23.
Yang Y, Zhang D, Feng N, Chen G, Liu J, Chen G, Zhu Y. Increased intake of vegetables, but not fruit, reduces risk for hepatocellular carcinoma: a meta-analysis. Gastroenterology. 2014. doi:10.1053/j.gastro.
Fernández-Rodríguez CM, Gutiérrez-García ML. Prevention of hepatocellular carcinoma in patients with chronic hepatitis B. World J Gastrointest Pharmacol Ther. 2014;5(3):175–82.
Brown EM, Gamba G, Riccardi D, Lombardi M, Butters R, Kifor O, Sun A, Hediger MA, Lytton J, Hebert SC. Cloning and characterization of an extracellular Ca2+-sensing receptor from bovine parathyroid. Nature. 1993;366:575–80.
Canaff L, Petit JL, Kisiel M, Watson PH, Gascon-Barre M, Hendy GN. Extracellular calcium- sensing receptor is expressed in rat hepatocytes. Coupling to intracellular calcium mobilization and stimulation of bile flow. J Biol Chem. 2001;276:4070–9.
Cifuentes M, Rojas CV. Antilipolytic effect of calcium-sensing receptor in human adipocytes. Mol Cell Biochem. 2008;319:17–21.
Bai M. Structure and function of the extracellular calcium-sensing receptor (review). Int J Mol Med. 1999;4:115–25.
Xie R, Tang B, Yong X, Luo G, Yang SM. Roles of the calcium sensing receptor in digestive physiology and pathophysiology (review). Int J Oncol. 2014. doi:10.3892/ijo.2014.2560.
Xing WJ, Kong FJ, Li GW, Qiao K, Zhang WH, Zhang L, Bai SZ, Xi YH, Li HX, Tian Y, Ren H, Wu LY, Wang R, Xu CQ. Calcium-sensing receptors induce apoptosis during simulated ischaemia-reperfusion in Buffalo rat liver cells. Clin Exp Pharmacol Physiol. 2011;38(9):605–12.
Kapur K, Johnson T, Beckmann ND, Sehmi J, Tanaka T, Kutalik Z, Styrkarsdottir U, Zhang W, Marek D, Gudbjartsson DF, Milaneschi Y, Holm H, Diiorio A, Waterworth D, Li Y, Singleton AB, Bjornsdottir US, Sigurdsson G, Hernandez DG, Desilva R, Elliott P, Eyjolfsson GI, Guralnik JM, Scott J, Thorsteinsdottir U, Bandinelli S, Chambers J, Stefansson K, Waeber G, Ferrucci L, Kooner JS, Mooser V, Vollenweider P, Beckmann JS, Bochud M, Bergmann S. Genome-wide meta-analysis for serum calcium identifies significantly associated SNPs near thecalcium-sensing receptor (CASR) gene. PLoS Genet. 2010;6(7):e1001035.
Chou YH, Woon PY, Chen WC, Hsu YW, Chang JM, Hwang DY, Chiu YC, Kuo HC, Chang WP, Hou MF, Liu ME, Chang JG, Chang WC. A genetic polymorphism (rs17251221) in the calcium- sensing receptor gene (CASR) is associated with stonemultiplicity in calcium nephrolithiasis. PLoS One. 2011;6(9):e25227.
Jorde R, Schirmer H, Njølstad I, Løchen ML, Bøgeberg ME, Kamycheva E, Figenschau Y, Grimnes G. Serum calcium and the calcium-sensing receptor polymorphism rs17251221 in relation to coronary heart disease, type 2 diabetes, cancer and mortality: the Tromsø Study. Eur J Epidemiol. 2013;28(7):569–78.
Li X, Kong X, Jiang L, Ma T, Yan S, Yuan C, Yang Q. A genetic polymorphism (rs17251221) in the calcium-sensing receptor is associated with breast cancer susceptibility and prognosis. Cell Physiol Biochem. 2014;33(1):165–72.
Singh N, Promkan M, Liu G, Varani J, Chakrabarty S. Role of calcium sensing receptor (CaSR) in tumorigenesis. Best Pract Res Clin Endocrinol Metab. 2013;27:455–63.
Chakrabarty S, Radjendirane V, Appelman H, Varani J. Extracellular calcium and calcium sensing receptor function in human colon carcinomas: Promotion of e-cadherin expression and suppression of beta-catenin/tcf activation. Cancer Res. 2003;63:67–71.
O’Seaghdha CM, Yang Q, Glazer NL, Leak TS, Dehghan A, Smith AV, Kao WH, Lohman K, Hwang SJ, Johnson AD, GEFOS Consortium, Hofman A, Uitterlinden AG, Chen YD, GEFOS Consortium, Siscovick DS, Harris TB, Psaty BM, Coresh J, Gudnason V, Witteman JC, Liu YM, Kestenbaum BR, Fox CS, Köttgen A. Common variants in the calcium-sensing receptor gene are associated with total serumcalcium levels. Hum Mol Genet. 2010;19(21):4296–303.
Liu G, Hu X, Chakrabarty S. Calcium sensing receptor down-regulates malignant cell behavior and promotes chemosensitivity in human breast cancer cells. Cell Calcium. 2009;45(3):216–25.
Pollak MR, Brown EM, Chou YH, Hebert SC, Marx SJ, Steinmann B, Levi T, Seidman CE, Seidman JG. Mutations in the human Ca2+ -sensing receptor gene cause familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. Cell. 1993;5:1297–303.
Brown EM, MacLeod RJ. Extracellular calcium sensing and extracellular calcium signaling. Physiol Rev. 2001;81:239–97.
Magno AL, Ward BK, Ratajczak T. The calcium-sensing receptor: A molecular perspective. Endocr Rev. 2011;32:3–30.
Reh CM, Hendy GN, Cole DE, Jeandron DD. Neonatal hyperparathyroidism with a heterozygous calcium-sensing receptor (CASR) R185Q mutation: clinical benefit from cinacalcet. J Clin Endocrinol Metab. 2011;96:E707–12.
Pidasheva S, Grant M, Canaff L, Ercan O, Kumar U, Hendy GN. Calcium-sensing receptor dimerizes in he endoplasmic reticulum: biochemical and biophysical characterization of casr mutants retained intracellularly. Hum Mol Genet. 2006;15:2200–9.
Acknowledgments
The authors gratefully acknowledge the efforts and contributions of doctors, nurses and technical staff at the Shengjing Hospital of China Medical University and First Hospital of Dalian Medical University.
Conflict of interest
None of the authors have any financial or other interests that could be construed as a conflict of interest with regard to the submitted manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tang, Q., Zhao, Y., Wang, Y. et al. A genetic variant (rs17251221) in the calcium-sensing receptor relates to hepatocellular carcinoma susceptibility and clinical outcome treated by transcatheter hepatic arterial chemoembolization (TACE) therapy. Med Oncol 31, 267 (2014). https://doi.org/10.1007/s12032-014-0267-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12032-014-0267-2