
Abstract
Some genetic alterations of glutathione S-transferase omega 2 (GSTO2) have been reported to increase the risk of many malignancies, including hepatocellular carcinoma (HCC); however, their prognostic capability remained unresolved in HCC patients treated with transarterial chemoembolization (TACE). To fill this gap, we genotyped three well-defined polymorphisms in GSTO2 to assess whether they can predict overall survival among 228 HCC patients under TACE treatment. The median follow-up time and survival time were 22.0 months (range 3.0–60.0) and 19.2 months, respectively. Only one of three polymorphisms examined, rs157077, was significantly associated with overall survival of TACE-treated HCC (P = 0.003), and its mutant allele conferred a higher risk of death than its wild homozygotes (hazard ratio 1.58, 95 % confidence interval 1.17–2.14). Moreover, carriers of this mutant allele had higher tissue GSTO2 expression, reinforcing the prognostic capability of GSTO2 rs157077 for HCC, especially in combination with age and tumor–node–metastasis (TNM) stage. Taken together, we for the first time provided evidence supporting the prognostic role of GSTO2 in the progression of TACE-treated HCC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is one of the most common malignancies worldwide, especially in China, and it largely remains incurable [1]. As estimated, only 10–37 % of HCC patients with advanced tumor or poor hepatic functional reserve are suitable for surgery [2], and it is a high priority to adopt nonsurgical local therapy in routine clinical practice to improve survival and palliation of HCC patients [3]. Transarterial chemoembolization (TACE), as a minimally invasive treatment, has been recommended as a first-line palliative therapy for nonsurgical cases with large or multifocal lesions and no vascular invasion of distant metastasis [4]. However, the prognosis for HCC patients treated with TACE varied greatly according to host characteristics [5, 6] and disease status [7]. Traditional clinicopathological features such as tumor stage, histological grade, and concentration of serum alpha-fetoprotein (AFP) seem to insufficiently predict clinical outcomes in HCC patients. Therefore, there is an urgent need to develop novel discriminatory biomarkers for HCC patients with different clinical outcomes. The recent decade has witnessed extraordinary advances in investigating imaging and serological markers to predict survival and response to TACE treatment [8–11]. However, very few studies so far have explored the prognostic capability of potential genetic markers.
Glutathione S-transferases (GSTs) are a family of phase II isoenzymes that detoxify toxicant [12], and its dysfunction has been documented to be closely related with chemotherapeutic response [13–15]. Glutathione S-transferase omega 2 (GSTO2) belongs to the omega class of GSTs, and its detoxifying property is partially genetically determined [16]. Several lines of supportive evidence indicated that genetic alterations in GSTO2 were associated with significant risks of many digestive cancers, such as hepatocellular carcinoma, gastric cancer, and colorectal cancer [17, 18]. However, evidence for the prognostic capability of genetic alterations in GSTO2 for cancer is sparse. To address this issue, in this study, we explored three polymorphisms in GSTO2 and assessed the associations of these polymorphisms with overall survival in a cohort of 228 Chinese HCC patients under TACE therapy.
Materials and methods
Study participants
All study participants were consecutively recruited at the Department of Hepatobiliary Surgery and Department of Cardiology and Periphery Vascular Medicine, the First Affiliated Hospital of Xi’an Jiaotong University in Xi’an, China, and they were newly diagnosed and histopathologically confirmed HCC patients. All study patients received TACE treatment and had no previous history of other cancers or cancer-related treatments. Participants received other treatments (such as chemotherapy, interventional therapy, or biological target therapy) after surgical operation was excluded for further analysis. Ethics committee of the First Affiliated Hospital of Xi’an Jiaotong University approved this study. Written informed consent was obtained from each participant before enrollment.
Demographic and clinical data
For each participant, demographic data included age at diagnosis, gender, hepatitis B surface antigen (HBsAg) status, liver cirrhosis, Child–Pugh score, serum AFP level, and tumor–node–metastasis (TNM) stage (I, II, or III) and were recorded. Venous blood was stored in Vacutainer tubes at 4 °C. Genomic DNA was extracted from peripheral blood leukocytes using E.Z.N.A. Blood DNA Midi Kit (Omega Bio-Tek, Norcross, GA, USA), according to the manufacturer’s instructions. All participants were followed up postoperatively at 3-month intervals in the 1st year, 6-month intervals in the 2nd year, and annually thereafter. The survival time was defined as the period from the date of first treatment to the date of death or last follow-up.
Polymorphism selection and genotyping
Three examined polymorphisms (rs156699, rs157077, and rs7085725) within GSTO2 were selected from NIEHS, a set of web-based single nucleotide polymorphism (SNP) selection toll (National Institute of Environmental Health Sciences, http://snpinfo.niehs.nih.gov/snpinfo/snptag.htm). They were common polymorphisms with a minor allele frequency ≥0.05 in a population of Chinese Han in Beijing (CHB) and a design score cutoff ≥0.6. Genotyping was performed using the Sequenom MassARRAY iPLEX genotyping system (Sequenom Inc., San Diego, CA, USA). Data management and analyses were performed using Sequenom Typer 4.0 software.
Statistical analysis
All statistical analyses were performed using the SPSS software version 21.0 statistical package for Microsoft Windows (SPSS, Chicago, IL, USA). Study power was computed using the Power and Sample Size Calculation (PS) software version 3.0.7. Each genotype of examined polymorphisms was examined in a logistic regression model. Risk estimates are expressed as hazard ratios (HRs) and its 95 % confidence interval [95 % confidence interval (CI)] as estimated from multivariate Cox proportional hazard model. Multivariate analysis was adjusted by age and TNM stage. Kaplan–Meier curves and log-rank tests were used to assess the overall survival associated with different genotypes. All statistical tests were two-sided, and P < 0.05 was accepted as statistically significant.
Results
Clinical characteristics of study participants
Clinical characteristics of all 228 HCC patients treated with TACE are shown in Table 1. For all the patients, the median age at the time of HCC diagnosis was 55 years (range 21–87). The majority of patients were males (83.3 %) and complicated by HBsAg positive (75.9 %) and liver cirrhosis (84.2 %) status, 66.7 % of patients were classified as Child A, and 56.1 % of patients presented with tumor size ≥5 cm. More than half of the patients (57.5 %) had low serum AFP level (<200 ng/mL). The percentages of patients with TNM stages I, II, and III were 18.4, 14.9, and 66.7 %, respectively. At the end of follow-up, 14.0 % (n = 32) of patients were dead, and the median survival time was 19.2 months. Furthermore, Cox regression analyses showed poorer overall survival in patients with older age [adjusted HR (95 % CI) = 1.48 (1.01–2.18); P < 0.001] and advanced TNM stage [adjusted HR (95 % CI) = 1.38 (1.13–1.67); P < 0.001].
Association of rs157077 with overall survival
The influences of the three examined polymorphisms in GSTO2 were assessed on overall survival of HCC patients treated with TACE (Table 2). Under the dominant model, rs157077 was significantly associated with the overall survival. Patients carrying the mutant allele of rs157077 had a significantly increased risk of death [adjusted HR (95 % CI) = 1.58 (1.17–2.14)], compared with those homozygous for the wild type (P = 0.003). Kaplan–Meier analysis showed a significantly shorter median survival time in rs157077 mutant allele carriers than those homozygous for the wild type (17.0 vs. 21.2 months; log rank P = 0.001) (Fig. 1a).

Kaplan–Meier curves for HCC patients carrying the rs157077 mutant allele. a In all patients. b In HBV-positive patients. c in AFP-negative (<200 ng/mL) patients
The effect of rs157077 on the overall survival in HCC patients was further stratified by demographic and clinicopathological characteristics. As shown in Table 3, the significant increased death risk conferred by rs157077 was observed in younger patients [HR (95 % CI) = 1.71 (1.05–2.81); P = 0.033], HBsAg-positive patients [HR (95 % CI) = 1.65 (1.16–2.35), P = 0.006], and AFP-negative patients [HR (95 % CI) = 1.72 (1.12–2.65); P = 0.014]. Log-rank test further indicated significant shorter OS time of mutant allele carriers in those patients with abovementioned factors (Fig. 1b, c).
Association of rs157077 with GSTO2 expression
The expression quantitative trait locus (eQTL) analysis was conducted to explore whether rs157077 have functional relevance using Genevar software. Genevar analysis showed that the mutant allele (G) was consistently correlated with higher expression of GSTO2 in adipose and skin tissues obtained from healthy female twins (Fig. 2).

Association between the rs157077 genotype and the GSTO2 expression in tissues from healthy female twins based on an eQTL analysis in the Genevar database of SNP–gene associations. a, c Adipose tissue. b, d Skin tissue; rho correlation value, Pemp non-parametric permutation P value for 10,000 reiterations
Survival tree analysis
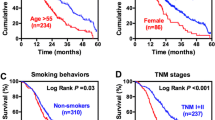
A survival tree analysis was performed to explore the potential prognostic capability of rs157077. The top splitting factor was TNM stage, followed by age and rs157077, resulting in a four-terminal node tree (Fig. 3a). The median survival time was 15.8 months for terminal node 1 (HCC patients with TNM stage III) and 18.7 months for terminal node 2 (patients with TNM stage I + II and age >55 years). In those HCC patients with younger age (≤55 years), TNM stage I + II and carrying the rs157077 homozygous wild type had a better clinical outcome with a median survival time of 45.6 months, when compared with those mutant allele carriers (P < 0.001; Fig. 3b).

Classification and regression tree analysis of rs157077. a Survival tree analysis of rs157077 with HCC overall survival. The number under each node represents a median survival time. b Overall survival according to different risk groups identified by survival tree analysis
Discussion
In the present study, we evaluated the prognostic capability of the three polymorphisms within GSTO2 among 228 TACE-treated HCC patients. We found that only rs157077 was significantly associated with the overall survival of HCC patients. To the best of our knowledge, this is the first study to investigate the prognostic value of GST genetic alterations for the TACE-treated HCC.
TACE is a widely used therapy in clinical practice for mid-stage HCC, and its anti-tumoral effect is mainly achieved through the occlusion-related hypoxia and chemotherapy-induced cytotoxicity, implicating in the induction of oxidative damage and cell death after DNA damage. As an important oxygen free radical-scavenging enzyme, GSTO2 protects normal hepatocytes against oxidative damage induced by chemical toxicant [19, 20]. Considering that GSTO2 activity is under genetic control [16], it is therefore reasonable to assume that GSTO2 genetic alterations might affect cancer risk and prognosis. Indeed, previous case–control studies have demonstrated that some GSTO2 polymorphisms were associated with an increased risk of cancer [18, 21–24], possibly by modulating GSTO2 gene expression level [25]. However, the genetic effect of GSTO2 on cancer prognosis is still largely unknown. In the present study, we, for the first time, identified a common polymorphism, rs157077, in GSTO2 as a primary factor to predict the clinical outcome of HCC patients either in overall or in stratified analysis. The potential contribution of rs157077 to overall survival was also consolidated by survival tree analysis. When combining rs157077 with age and TNM stage, two important prognosis factors, our risk prediction model exhibited strong prognostic capability for TACE-treated HCC patients.
To date, little is known about the functional role of GSTO2 in carcinogenesis. It has been observed that the GSTO1 gene, which was a paralog gene and exhibited very similar biological function to GSTO2, was over-expressed in chemo- and radio-resistant cancer cells [26, 27] and was involved in cancer cell invasion and metastasis [28]. On the basis of these observations, GSTO2 is believed to play an important role in cancer progression and alteration of GSTO2 which determine cancer patients’ survival. In the present study, we found that the mutant allele of rs157077 in GSTO2 was significantly correlated with GSTO2 expression in tissues, the finding serving as a potential explanation that rs157077 mutant allele carriers had shorter survival time after TACE treatment, compared with the wild homozygotes, which might be due to their higher GSTO2 expression.
Another important finding of our study was that GSTO2 rs157077 was identified to be significantly associated with overall survival in AFP-negative patients. AFP, the only universally recognized tumor marker for HCC [29], served as a marker for prognosticating response to TACE therapy for a long time. However, estimates of the prognostic value of serum AFP level between studies differed widely [30, 31]. Considering that approximately 70 % of TACE-treated HCC patients are AFP negative [32], new prognostic biomarkers are needed to improve treatment efficacy. Our findings supported the use of rs157077 as an ancillary method to predict TACE response in AFP-negative HCC patients.
Several possible limitations should be acknowledged for this study. First, the moderate sample size might limit the validity of some stratified analyses. Second, only three polymorphisms within GSTO2 were examined. It is highly encouraged to incorporate other polymorphisms, especially the low-penetrance polymorphisms in GSTO2 and other relevant genes. Third, the fact that our study participants were of northwestern Han Chinese descent limited the generalizability of our findings, calling for further evaluation to determine whether these findings can be generalized to other ethnic groups.
In conclusion, this study provided the first epidemiological evidence in favor of a role of rs157077 in the prognostic prediction of a Chinese population of HCC patients under TACE therapy. If validated, this genetic polymorphism may potentially be developed as a simple non-invasive predictive biomarker.
References
Jemal A et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90.
Burroughs A, Hochhauser D, Meyer T. Systemic treatment and liver transplantation for hepatocellular carcinoma: two ends of the therapeutic spectrum. Lancet Oncol. 2004;5:409–18.
Lencioni R, Crocetti L. Local-regional treatment of hepatocellular carcinoma. Radiology. 2012;262:43–58.
Bruix J, Sherman M, American Association for the Study of Liver, D. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–2.
Llovet JM et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359:1734–9.
Lo CM et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35:1164–71.
European Association for Study of, L., European Organisation for, R. & Treatment of, C. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Eur J Cancer. 2012;48:599–641.
Chung JC et al. Diffusion-weighted magnetic resonance imaging to predict response of hepatocellular carcinoma to chemoembolization. World J Gastroenterol. 2010;16:3161–7.
Mannelli L, Kim S, Hajdu CH, Babb JS, Taouli B. Serial diffusion-weighted MRI in patients with hepatocellular carcinoma: prediction and assessment of response to transarterial chemoembolization. Preliminary experience. Eur J Radiol. 2013;82:577–82.
Cho E et al. Serum insulin-like growth factor-1 predicts disease progression and survival in patients with hepatocellular carcinoma who undergo transarterial chemoembolization. PLoS One. 2014;9:e90862.
Zheng YB et al. Prognostic value of serum vascular endothelial growth factor receptor 2 response in patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Med Oncol. 2014;31:843.
Chasseaud LF. The role of glutathione and glutathione S-transferases in the metabolism of chemical carcinogens and other electrophilic agents. Adv Cancer Res. 1979;29:175–274.
Lee WH et al. Cytidine methylation of regulatory sequences near the pi-class glutathione S-transferase gene accompanies human prostatic carcinogenesis. Proc Natl Acad Sci U S A. 1994;91:11733–7.
Niu D, Zhang J, Ren Y, Feng H, Chen WN. HBx genotype D represses GSTP1 expression and increases the oxidative level and apoptosis in HepG2 cells. Mol Oncol. 2009;3:67–76.
Zhang YJ et al. Silencing of glutathione S-transferase P1 by promoter hypermethylation and its relationship to environmental chemical carcinogens in hepatocellular carcinoma. Cancer Lett. 2005;221:135–43.
Mukherjee B et al. Glutathione S-transferase omega 1 and omega 2 pharmacogenomics. Drug Metab Dispos. 2006;34:1237–46.
Marahatta SB et al. Polymorphism of glutathione S-transferase omega gene and risk of cancer. Cancer Lett. 2006;236:276–81.
Masoudi M, Saadat I, Omidvari S, Saadat M. Genetic polymorphisms of GSTO2, GSTM1, and GSTT1 and risk of gastric cancer. Mol Biol Rep. 2009;36:781–4.
Board PG et al. Identification, characterization, and crystal structure of the omega class glutathione transferases. J Biol Chem. 2000;275:24798–806.
Whitbread AK et al. Characterization of the omega class of glutathione transferases. Methods Enzymol. 2005;401:78–99.
Masoudi M, Saadat I, Omidvari S, Saadat M. Association between N142D genetic polymorphism of GSTO2 and susceptibility to colorectal cancer. Mol Biol Rep. 2011;38:4309–13.
Pongstaporn W et al. Genetic alterations in chromosome 10q24.3 and glutathione S-transferase omega 2 gene polymorphism in ovarian cancer. J Exp Clin Cancer Res. 2006;25:107–14.
Pongstaporn W, Pakakasama S, Sanguansin S, Hongeng S, Petmitr S. Polymorphism of glutathione S-transferase omega gene: association with risk of childhood acute lymphoblastic leukemia. J Cancer Res Clin Oncol. 2009;135:673–8.
Xu YT et al. Genetic polymorphisms in glutathione S-transferase omega (GSTO) and cancer risk: a meta-analysis of 20 studies. Sci Rep. 2014;4:6578.
Allen M et al. Glutathione S-transferase omega genes in Alzheimer and Parkinson disease risk, age-at-diagnosis and brain gene expression: an association study with mechanistic implications. Mol Neurodegener. 2012;7:13.
Giri U, Terry NH, Kala SV, Lieberman MW, Story MD. Elimination of the differential chemoresistance between the murine B-cell lymphoma LY-ar and LY-as cell lines after arsenic (As2O3) exposure via the overexpression of gsto1 (p28). Cancer Chemother Pharmacol. 2005;55:511–21.
Yan XD, Pan LY, Yuan Y, Lang JH, Mao N. Identification of platinum-resistance associated proteins through proteomic analysis of human ovarian cancer cells and their platinum-resistant sublines. J Proteome Res. 2007;6:772–80.
Liu L, Zhao L, Zhang Y, Zhang Q, Ding Y. Proteomic analysis of Tiam1-mediated metastasis in colorectal cancer. Cell Biol Int. 2007;31:805–14.
Xu XS et al. Highlights for alpha-fetoprotein in determining prognosis and treatment monitoring for hepatocellular carcinoma. World J Gastroenterol. 2012;18:7242–50.
O’Suilleabhain CB et al. Factors predictive of 5-year survival after transarterial chemoembolization for inoperable hepatocellular carcinoma. Br J Surg. 2003;90:325–31.
Tsai YJ et al. Early identification of poor responders to transarterial chemoembolization for hepatocellular carcinoma. Hepatol Int (2011) (in press).
Takayasu K et al. Prospective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8510 patients. Gastroenterology. 2006;131:461–9.
Acknowledgments
This work was financially supported by the National Natural Science Foundation of China (Grant Nos. 81201549 and 81272644) and the project of Innovative Research Team for Key Science and Technology in Xi’an Jiaotong University (No. 2003KCJ-23).
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding authors
Additional information
Zhixin Wang, Kai Qu and Zhichao Huang contributed equally to this work.
Rights and permissions
About this article

Cite this article
Wang, Z., Qu, K., Huang, Z. et al. Glutathione S-transferase O2 gene rs157077 polymorphism predicts response to transarterial chemoembolization in hepatocellular carcinoma. Tumor Biol. 36, 6463–6469 (2015). https://doi.org/10.1007/s13277-015-3336-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-3336-z