
Abstract
Recently, administration of calcium supplements for the prevention and treatment of osteoporosis has become a highly controversial issue. The findings of epidemiological studies are not necessarily supportive of the practice and are also open to different interpretations. In this article, we attempt to broaden the discussion and provide evidence that calcium supplementation may fail to compensate for renal calcium loss, and also that the resultant increased calcium load in the circulation could lead to extraskeletal deposition, including in the coronary arteries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
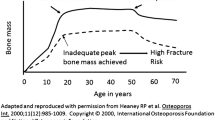
Osteoporotic fractures, particularly in the hip, significantly increase morbidity and mortality and are devastating to those affected. Calcium supplements are universally given in combination with first line therapies for the prevention and treatment of osteoporosis, but recently, their use has been questioned in the light of findings from meta-analyses primarily concerning their possible cardiovascular adverse effects [1]. As expected, these concerns have been disputed with significant criticism regarding the validity of the methods used in the analyses and, more recently, the lack of a clear biological mechanism explaining such an outcome. In an attempt to advance the discussion on this important topic, we describe the anticipated effects of calcium (and vitamin D) supplementation prescribed to compensate for increased calcium availability and excretion secondary to high bone turnover, otherwise known as renal calcium leak [2] and provide evidence for a physiological mechanism that could force the system to deposit the increased load of calcium in places other than the skeleton.
The pathophysiology of calcium handling in patients with osteoporosis
Interestingly, the simplistic view of replacing the excreted calcium has been enough to justify indiscriminate calcium administration. As of yet, a comprehensive recognition of the pathophysiology has not entered into the discussion of the current controversy of calcium supplementation. Based on our current understanding of calcium and phosphate homeostasis, evidence suggests that supplemental calcium could fail to compensate for renal calcium loss, and the resultant increased calcium load in the circulation could lead to extraskeletal deposition, including in the coronary arteries.
Estrogen maintains the steady state of calcium and phosphate (Pi) homeostasis. In menopause, particularly early in its course, the withdrawal of estrogen lifts an inhibitory effect on cytokines including IL-1, IL-6, and TNF-α, causing acceleration in the rate of bone resorption by osteoclasts. [3, 4] As a result, more calcium and Pi become available in the circulation inducing parathyroid hormone (PTH) to respond to the changes in their concentration. While on the one hand, increasing calcium levels provoke a decrease in PTH, the elevation in Pi, however, will raise the demand for more phosphaturic action from PTH and therefore antagonistically increase levels. Simultaneously, elevations in Pi will increase the levels of FGF-23, which in turn will both decrease the release of PTH to prevent the release of additional Pi and calcium from the bone, and will also decrease the levels of 1,25(OH)2D3 to restrict the absorption of both calcium and Pi from the intestine (Fig. 1). Thus, following the withdrawal of estrogens, this concerted action will effectively keep the PTH concentration unchanged [5], despite increased bone resorption liberating additional calcium and Pi. The ensuing elevations in calcium result in its increased excretion through the kidneys, otherwise known as renal calcium leak.

Simplified schematic presentation of the effects of menopause on calcium and Pi concentrations and their regulating hormones. In light brown the inhibitory effects of increased calcium concentrations on the production/release of PTH; in dark brown the stimulatory effects of 1,25(OH)2D3 on the calcium and phosphate absorption in the intestine; in dark blue the stimulating effects of increased Pi concentrations on the production/release of PTH; and in light blue the inhibitory effects of FGF-23 on the production of 1,25(OH)2D3 in the kidney and PTH in the parathyroid glands
By providing calcium (and vitamin D) supplementation, we force more calcium and Pi into the circulation with the assumption that it will be preferentially shunted to bone. However, even in the high bone turnover state characteristic of postmenopausal osteoporosis, the capacity for bone to buffer the additional calcium is restricted due to the inability of osteoblasts to maintain rates of bone formation equivalent to those of resorption. Indeed, early menopausal women (≤5 years menopausal) did not benefit from calcium supplementation [6], and neither calcium nor vitamin D alleviates bone resorption during the early stages of change in estrogen status [7]. Furthermore, in patients taking antiresorptives, if the same amount of calcium is administered, the possible detrimental effects could be clinically relevant. Following the use of potent antiresorptives, such as nitrogen containing bisphosphonates or denosumab, an anti-RANKL binding monoclonal antibody (with denosumab being the more “aggressive” of the two), the rate of bone resorption by osteoclasts is effectively decelerated, as is the rate of bone formation by osteoblasts as well. As a result, the capacity of the bone for buffering calcium is limited further. This loss of skeletal space for calcium storage will force greater excretion through the kidneys and seek extraskeletal locations for deposition [8]. In patients on commonly prescribed thiazide diuretics, which are able to reduce calcium excretion by as much as 50–150 mg, the renal route will be compromised to an even greater extent, inevitably making soft tissues and vessels one of the alternatives for the deposition of the circulating calcium surplus.
In reality, administration of calcium and vitamin D supplementation may be simply increasing the amount of circulating calcium and Pi, which will increase their product (Ca × Pi) and the risk of extraskeletal calcification. As far as the bone is concerned, increased calcium availability could lower PTH levels and decrease the rate of bone resorption, although to a lesser degree than that caused by the action of the cytokines mentioned above. Simultaneously, the decrease in PTH action will also reduce the rate of new bone formation. Therefore, calcium supplementation could not only have no effects on substituting the calcium leaked through the kidneys but it could also be increasing the risk of extraskeletal deposition in soft tissues including the coronary arteries.
A group of patients that could be at a higher risk of vascular calcification could be those with reduced renal function. In a recently published analysis of the 2005–2008 National Health and Nutrition Examination Survey (NHANES) USA data, nearly a quarter of women with osteoporosis (23.54 ± 2.02 %; 2.9 million) had moderate renal impairment defined as GFR 30–59 mL/min [9]. These patients are expected to be treated with calcium supplements as a routine.
The debate on the benefits and risks of “forcing” the entry of calcium into the circulation via the co-administration of vitamin D (another issue that should be scrutinized rigorously) will take time to reach a consensus. However, indiscriminate prescription of calcium supplementation to all postmenopausal women should be reconsidered.
References
I.R. Reid, M.J. Bolland, Calcium risk-benefit updated–new WHI analyses. Maturitas. 77(1), 1–3 (2014). doi:10.1016/j.maturitas.2013.10.003
W.R. McKane, S. Khosla, M.F. Burritt, P.C. Kao, D.M. Wilson, S.J. Ory, B.L. Riggs, Mechanism of renal calcium conservation with estrogen replacement therapy in women in early postmenopause–a clinical research center study. J. Clin. Endocrinol. Metab. 80(12), 3458–3464 (1995)
S. Khosla, Pathogenesis of age-related bone loss in humans. J. Gerontol. A Biol. Sci. Med. Sci. 68(10), 1226–1235 (2013)
G. Passeri, G. Girasole, R.L. Jilka, S.C. Manolagas, Increased interleukin-6 production by murine bone marrow and bone cells after estrogen withdrawal. Endocrinology 133(2), 822–828 (1993)
R.L. Prince, I. Dick, P. Garcia-Webb, R.W. Retallack, The effects of the menopause on calcitriol and parathyroid hormone: responses to a low dietary calcium stress test. J. Clin. Endocrinol. Metab. 70(4), 1119–1123 (1990)
B. Dawson-Hughes, G.E. Dallal, E.A. Krall, L. Sadowski, N. Sahyoun, S. Tannenbaum, A controlled trial of the effect of calcium supplementation on bone density in postmenopausal women. N. Engl. J. Med. 323(13), 878–883 (1990)
C.Y. Park, W.H. Lee, J.C. Fleet, M.R. Allen, G.P. McCabe, D.M. Walsh, C.M. Weaver, Calcium and vitamin D intake maintained from preovariectomy independently affect calcium metabolism and bone properties in Sprague Dawley rats. Osteoporos. Int. 25(7), 1905–1915 (2014)
A.M. Parfitt, Renal bone disease: a new conceptual framework for the interpretation of bone histomorphometry. Curr. Opin. Nephrol. Hypertens. 12(4), 387–403 (2003)
R. Lubwama, A. Nguyen, A. Modi, C. Diana, P.D. Miller, Prevalence of renal impairment among osteoporotic women in the USA, NHANES 2005-2008: is treatment with bisphosphonates an option? Osteoporos. Int. 25(5), 1607–1615 (2014)
Conflict of interest
No competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Paziana, K., Pazianas, M. Calcium supplements controversy in osteoporosis: a physiological mechanism supporting cardiovascular adverse effects. Endocrine 48, 776–778 (2015). https://doi.org/10.1007/s12020-015-0550-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-015-0550-9