
Abstract
Copper is an essential trace element in animals and humans. However, excessive intake of copper can cause copper ions to accumulate in tissues and organs of animals, leading to copper toxicity. Copper ions induce apoptosis and autophagy through oxidative stress–mediated mitochondrial dysfunction. In addition, copper induces cell death by targeting lipoylated tricarboxylic acid (TCA) cycling proteins, termed cuproptosis. In recent years, copper cytotoxicity studies have attracted attention. In addition, the number of cases of copper toxicity in animals has been increasing over the past years due to environmental pollution and overdose from copper feed supplements. Therefore, a comprehensive understanding of copper toxicity and the metabolism of copper ions can aid in devising strategies for preventing copper toxicity. This review introduces the tissue and organ toxicity and cytotoxicity caused by copper toxicity and reviews the metabolism of copper ions in tissues, organs, and cells. The paper also reviews the clinical cases and animal experiments of copper toxicity in recent years. Finally, the preventive and curative measures for copper toxicity and the future challenges are also discussed. The general objective of this paper is to provide a reliable reference for copper toxicity prevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Copper is a trace element found in nature [1]. In 1921, scientists identified the occurrence of copper in animals and insects [2]. Since then, scientists have gradually begun to explore the function of copper in animals [3]. Nowadays, people are much more aware of copper. Copper is distributed in various tissues and organs in the animal body, such as the liver, kidney, heart, bones, nerve cells, and hair [4]. Copper participates in hematopoiesis, the growth, and development of nerve cells in animals. It is also a cofactor of many metalloenzymes, including cytochrome C oxidase [5] and phosphodiesterase [6]. Furthermore, copper participates in maintaining normal metabolism in the animal body by binding to enzymes [7].
Studies have shown that copper deficiency can lead to some animal diseases. Copper deficiency in small ruminants leads to delayed estrus, abortion, congenital ataxia, and infertility. Copper deficiency in layers affects the formation of lysine-derived cross-links, which constitute the biochemical and mechanical properties of eggshell membranes [8]. But excessive copper can lead to copper toxicity in animals [9]. In 1948, Marston et al. experimentally studied the effects of copper excess on mature Merino and Border-Leicester sheep. The results of the experiments showed significant differences in the response of the two breeds to copper overdose, with Border-Leicester sheep dying almost entirely after the first hemolytic crisis, while Merino sheep were better tolerant of copper excess intake [10]. After years of studies, in 1969, scientists recognized chronic copper toxicity as a nutritionally harmful animal disease [11]. However, the specific doses for different animals and the causative mechanisms of copper toxicity were unknown.
Copper Toxicity
Copper toxicity can cause diarrhea, abdominal pain, liver dysfunction, and hemolysis in animals [12]. In 1970, researchers conducted experiments on sheep and observed that excess copper caused gastrointestinal lesions [13]. The mechanisms of toxicity by trace elements include causing protein aggregation, which could affect biological processes [14]. Copper toxicity can be chronic or acute, depending on the degree of exposure. Reported cases of acute copper toxicity are mainly through accidental ingestion of copper-containing preparations (copper sulfate, basic copper chloride) [15]. Chronic copper toxicity is mainly through excessive intake of copper in the diet, feeding errors in the diet, overuse of copper supplements, and the presence of genetic diseases with gene mutations.
Chronic Copper Toxicity
Chronic copper toxicity is caused by excessive intake of copper in animals over a long time [16]. It is divided into two phases. The first is the copper accumulation period, which spans from a few weeks to more than a year, and the animals have no obvious poisoning symptoms. In the second stage, the animal appears to refuse to eat for a short period of time, moves slowly, has sunken eyes, and develops a yellowish discoloration of the visible mucous membranes [17]. In 1976, Soil et al. were the first to discover morphological changes in the erythrocytes of sheep with chronic copper toxicity, confirming the plausibility of the phenomenon of hemolysis [18]. Chronic copper toxicity primarily affects the liver [19, 20]. When the liver’s ability to process copper is overwhelmed, chronic copper toxicity occurs, manifesting itself as an acute hemolytic crisis in which the liver releases excess copper, causing hemolysis of red blood cells [20].
Cooper et al. performed autopsies on four rabbits, three females and one male, suffering from copper toxicity. The researchers observed fresh blood in the abdominal cavity, ruptured liver hemorrhage in the male, and acute intravascular hemolysis and hemoglobinuric nephropathy in two females. The highest copper residue in the liver of the rabbits was 1250 mg/kg, and the lowest concentration was 532 mg/kg [21]. Giadinis et al. found signs of hemolytic disease with neurological involvement in sheep diagnosed with chronic copper toxicity. Treatment involved regulating copper intake, while sodium sulfate and ammonium molybdate were added to the sheep’s diet to alleviate the copper toxicity symptoms [22]. In one study in Israel, an intake of 250 mg/kg copper caused classical clinical signs of copper toxicity in several cows, and 20 cows died within 4 days [23].
Chronic copper toxicity is characterized by a group nature, with a long incubation period, but no obvious symptoms are observed in the early stages of chronic copper toxicity. If the source of the excess copper cannot be identified in time in animals, group illnesses can easily occur, resulting in serious economic losses.
Acute Copper Toxicity
Acute copper toxicity is rare and is usually seen when large amounts of copper-containing compounds, such as copper sulfate and copper acetate, are ingested over a short time. The severity of acute copper toxicity is closely related to the amount of copper ingested. Mild cases present with gastrointestinal symptoms. In severe cases, gastrointestinal bleeding, endogenous hemolysis, acute kidney injury, and death may occur [24]. Giergiel et al. investigated a case of copper toxicity due to ingestion of bedding soaked in copper sulfate solution, a disinfectant, in 2-day-old turkeys. Necropsy revealed the presence of wood chips in the gastrointestinal contents, numerous lesions in the digestive tract, erosion, deep ulcers, and severe congestion on the surface of the muscularis propria. The copper levels in the liver were more than seven times the normal level [15]. Dash and other autopsies have found that acute copper toxicity causes acute renal failure, and excessive copper intake is directly toxic to renal tubular cells. Acute copper toxicity causes gastrointestinal bleeding and circulatory failure [25]. Some studies have found that whole-blood copper concentrations strongly correlate with the severity of acute copper toxicity. However, no strong correlation exists between serum copper concentrations and the severity of the toxicity [26].
Over the past nearly 100 years, there have been different animal clinical cases and animal experiments reporting chronic copper toxicity and acute copper toxicity, which are summarized in Table 1. It can be seen that most of the research reports are chronic copper toxicity. The pathological changes of copper toxicity in different types of animals are mostly liver and kidney lesions, and clinical symptoms mainly include developmental delay and diarrhea. Up to now, only a few cases of acute copper toxicity in animals have been reported. In intensive farming farms, animal feeds are managed carefully; thus, the probability of sudden excessive intake of copper is low.
Toxicity Analysis
The reasons for copper toxicity in animals include copper intake and the animal’s own factors such as species, age, and genetics [33]. Accumulation of copper in tissues causes several damages, including hepatotoxicity, nephrotoxicity, neurotoxicity, and cytotoxicity [34].
Hepatotoxicity
The liver is the main organ for storing copper and plays an important role in maintaining copper homeostasis. The same ingested copper by the animal organism is mainly distributed by the liver, which acts as a copper center. When the ingested copper exceeds the hepatic threshold, it triggers the release of hepatic copper, allowing it to further affect other organs. The main reason for hepatotoxicity is that the accumulation of Cu in the liver may lead to oxidative damage by overproduction of reactive oxygen species (ROS) which induces a variety of cell deaths such as autophagy, apoptosis, and necrosis. Further, the changes that occur in the cells can further affect the function of the liver. Copper accumulation in the liver also may cause liver fibrosis [35]. Excess copper in the body accumulates in the central lobe area of the liver. The hepatotoxicity of copper has been demonstrated in several studies in different animals. Chronic exposure to elemental copper has been found to induce significant hepatotoxicity in animal studies [36,37,38]. Copper exposure–induced hepatotoxicity also involves multiple signaling pathways and several types of cell death, such as mitochondrial dysfunction apoptosis and cuproptosis [39, 40]. Li et al. experimentally confirmed that copper exposure leads to mitochondrial dysfunction and hepatotoxicity by inducing oxidative stress and PERK/ATF4-mediated endoplasmic reticulum stress [41]. Zhong et al. reported that FDX1-mediated proteolipid acylation and proteotoxic stress were indeed involved in copper-induced hepatotoxicity in chickens.
The experimental results showed that the mRNA and protein levels of FDX1 were significantly up-regulated and the levels of lipoylated-DLAT and oligomerization of lipoylated-DLAT were significantly increased under the treatment of a high-copper environment, which corroborated the idea of cuproptosis proposed by Tsvetkov et al. [36]. In addition, Sutunkova et al. noticed significant dystrophic and progressive necrotic changes in liver hepatocytes of mice exposed to copper oxide nanoparticles [42].
Nephrotoxicity
The kidney is involved in the circulation and excretion of toxins, including excess copper [43]. Copper excretion mainly occurs in the bile; only a small amount of copper is excreted in the urine [44]. In 1989, Fuentealba et al. used 6-week-old male mice in a 16-week high-copper feeding experiment. At week 4, copper ions accumulated rapidly in the kidneys of the mice, and irreversible nuclear damage occurred after a threshold was reached. Also, this experiment demonstrated nephrotoxicity due to copper overdose [45]. In addition to the common copper oxide particles, copper nanoparticles are also widely used as livestock and poultry feed additives. In 2012, Liao et al. found that copper nanoparticles induced extensive renal proximal tubular necrosis in rat kidneys, accompanied by elevated blood urea nitrogen and creatinine [46]. Elevated serum creatinine and urea levels are indicators of nephrotoxicity [47]. Regarding the molecular mechanism of CuSO4-induced nephrotoxicity, Dai et al. showed that CuSO4 exposure up-regulated the activity and mRNA expression of some enzymes [37]. Currently, researchers have experimentally demonstrated that resveratrol, among others, has a positive effect on copper-induced nephrotoxicity [47]. Sara et al. experimentally demonstrated using chickens that excessive copper intake causes nephrotoxicity and that intake of cinnamon extract and probiotics ameliorate copper-induced nephrotoxicity [48]. Gopinath et al. designed experiments and found that in copper-poisoned sheep, the copper content in the kidneys rose during the prehemolytic phase, and necrosis, degeneration, and changes in enzyme activity occurred in renal tubular cells during the hemolytic phase. A large amount of hemoglobin appeared in the renal tubular cells [49]. Khalid et al. found that gavage intake of 300 mg/kg of copper oxide nanoparticles caused hepatotoxicity and nephrotoxicity in Wistar rats. However, resveratrol protects against CuONPs-induced hepatotoxicity and nephrotoxicity. The results showed that copper oxide significantly increased ALT, AST, creatinine, and urea levels and caused kidney injury [47]. Copper accumulation in the kidney leads to glomerular and tubular dysfunction, causing hemoglobinuria [49].
Neurotoxicity
Copper is well-known to be necessary for the development and function of the nervous system. Several studies have suggested that excess copper may have neurotoxic effects, but the mechanism of neurotoxicity is unknown. Zhu et al. detected the relationship between ROS and mitochondrial autophagy in the hypothalamus of mice treated with high copper. The experimental results showed that high concentrations of copper sulfate caused histopathological and neuronal alterations in the hypothalamus of mice, produced a large amount of ROS, induced mitochondrial autophagy, and led to an imbalance in mitochondrial division or fusion [50]. Yu et al. explored the effects of long-term exposure to basic copper chloride (TBCC) on neurotoxicity, using Sprague–Dawley rats grouped to give different doses of TBCC treatment. The results showed that excessive TBCC induced cognitive dysfunction in rats; at 12 weeks, the number of nidus vesicles in the hippocampus was decreased, and the balance of neuronal mitochondrial division or fusion was disrupted [51]. Through microscopic examination, Howell et al. found that astrocytes in sheep suffering from chronic copper toxicity were deformed, while neuroglial disorganization was observed in the brain, reflecting the neurological damage of copper toxicity [52].
Cytotoxicity
ROS are a by-product of normal mitochondrial metabolism within the cell and homeostasis in vivo. It is also a signal molecule, but when its levels are elevated, it causes lipid, protein, and DNA damage [53]. Excess intracellular copper will induce ROS production via the Fenton and Haber–Weiss reactions [43]. Tchounwou et al. found that excess copper induces stress genes and also causes mitochondrial dysfunction by reducing mitochondrial transmembrane potential and ATP levels [54]. In 2022, Tsvetkov et al. demonstrated that copper-induced cell death is regulated by mitochondrial ferredoxin 1 (FDX-1)-mediated lipid acylation of proteins. Copper can induce cell death by targeting lipoylated tricarboxylic acid (TCA) cyclins, which is a newly discovered form of cell death that the researchers named cuproptosis [55]. Autophagy is a catabolic mechanism associated with lysosomes. The main role of autophagy in cells under normal conditions is to maintain intracellular trophic homeostasis, whereas transitory autophagy leads to autophagic cell death [56]. Copper has been found to bind to the autophagy-regulated kinases ULK1 and ULK2, and this binding is required for kinase activity. In addition, altering intracellular copper levels can modulate the kinase activities of ULK1 and ULK2, thereby affecting the autophagic process [57].
Copper Absorption and Metabolism
Copper Absorption and Metabolism in Ruminants
The rumen microbiological system of ruminants has an important influence on copper absorption [58]. The presence of Cu–Mo–S interactions in ruminants affects copper absorption [59]. In the rumen of ruminants, only 5% of copper is absorbed, of which more than 90% is excreted [60]. In addition, Van Beest et al. measured essential trace elements in the blood, liver, kidney, and hair of red deer (Cervus elaphus). Copper and zinc concentrations were found to be positively correlated with metallothionein 1 (MT1) mRNA expression levels in red deer liver and with the age of the red deer [61]. In 1995, researchers studied copper metabolism in cattle using Angus, Simmental, and Charolais cattle. The study found that Angus cattle had higher plasma copper concentrations and ceruloplasmin activity than Charolais and Simmental cattle in the absence of copper supplementation and that Angus bulls performed better in terms of copper uptake and retention [62]. Different breeds of sheep have different copper tolerance levels [63]. It can also be concluded from the analyses of the case reports that sheep are the animals most likely to suffer from copper toxicity. Worldwide, more cases of copper toxicity in sheep have been reported, resulting in heavy economic losses. In addition, ruminants are most susceptible at a young age, when the milk does not pass through the rumen, so copper is absorbed more efficiently, accumulates more quickly, and is more likely to occur [64]. The production of sulfide in the rumen of ruminants reduces the availability of copper in forage [58]. Sheep cannot increase bile secretion to promote copper excretion in response to increased copper intake. Sheep are intolerant to excess dietary copper due to an impaired ability to excrete copper in bile, leading to accumulation of copper in the liver and, eventually, hepatotoxicity [63]. Oruc et al. found widespread jaundice, yellow liver, kidney hypertrophy, and hemorrhage in sheep following autopsy. Serologic examination of the animals revealed high concentrations of copper in the serum. The farmer described the existence of a factory in the vicinity of the sheep house, and the investigators highly suspected that the sheep had inhaled dust or ingested copper-contaminated vegetation, which led to copper toxicity [65]. Early stages of copper toxicity in ruminants have no obvious clinical signs, and there is a risk of mass outbreaks if they are not detected in time.
Copper Absorption and Metabolism in Non-ruminant Animals
Non-ruminants including pigs, poultry, and dogs have a higher tolerance for copper than ruminants including cattle, sheep, and deer. Copper toxicity is not likely to occur under normal feeding conditions. At present, a case report of a 2-year-old male mongrel dog suffering from acute copper toxicity has been reported, and laboratory investigations have revealed significantly elevated copper levels in the liver of 3530 ppm, well above the laboratory reference interval of 120 to 400 ppm [29]. Huang and other researchers experimentally administered copper sulfate orally to chicks and observed changes in the cecum depending on the length of time. Specifically, there was detachment of the cecum mucosa from 90 days of copper sulfate intake [66]. Hashem et al. set up an experiment on copper toxicity in broiler chickens. The chickens were divided into five groups, one was fed 300 mg/kg of copper sulfate in basal ration for 7 weeks. No death occurred during the experimental period. However, some of the chickens showed mild diarrhea, decreased appetite, and pallor [67]. Copper is a highly effective supplement for swine, but long-term intake of copper feeds causes toxic copper accumulation [68]. Li et al. experimentally investigated copper toxicity dosage in porcine testes and showed that, on the one hand, copper exposure promoted apoptosis and induced autophagy. On the other hand, apoptosis caused a decrease in the antioxidant capacity in the testes [69]. Even though a high copper diet promotes piglet growth, excessive copper intake can lead to color changes in the pig’s intestines, mostly darkening. Ma and other researchers found that copper levels in intestinal pig samples significantly exceeded the national standard [70].
Organ and Tissue Copper Metabolism
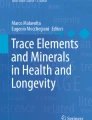
The process of copper absorption and metabolism is similar across different animals. Copper is absorbed from the stomach to the distal small intestine [71]. The most important site of absorption is the first section of the small intestine, the duodenum. Only a small fraction of the copper in food is fully soluble in the stomach, while most copper ions are absorbed in the small intestine. After entering the small intestine through the enterohepatic circulation, copper ions are transported to the liver via the hepatic portal vein [72]. Copper is mainly stored in the liver, and excess copper is excreted from the body mainly through bile or feces [53]. A small portion is excreted in sweat and urine. The flow of copper metabolism in tissues and organs is shown in Fig. 1.

The process of absorption and metabolism of copper ions. Copper ions are absorbed through the epithelial cells of the small intestine and pass through the portal circulation into the liver for storage and utilization, where they reach distant tissues via the circulation. Excess copper ions enter the bile ducts and are excreted through the bile
Intercellular Metabolism
The process of copper transport between tissues is shown in Fig. 1. Intercellular transport of copper ions is facilitated by a number of enzymes and copper-binding proteins [55, 73, 74].
Ceruloplasmin is a key target of mammalian copper homeostasis and copper-related copper ion transporter carriers. CTR 1 transports monovalent copper ions into the cell [75]. CTR1, present in both yeast and mammalian cells, is a high-affinity copper transporter characterized by high structural and functional stability [76]. Cytb converts divalent copper ions to monovalent copper ions [77]. Atox-1 is responsible for the translocation of copper to ATP7a and ATP7b in the trans-Golgi [78]. COX can use copper for oxidative phosphorylation and mitochondrial function [5]. Plasma copper cyano-proteins (CP) are the main carriers of copper transported in the blood. Other carriers of copper in the circulation include amino acids and albumin, which transport copper for use in individual tissue cells [75].
Copper ions are not directly absorbed in the small intestine but need to bind to the enzyme metalloreductase (STEAP), where they are first converted to cuprous ions before absorption [79]. Cuprous ions enter small intestinal epithelial cells via members of the solute carrier family, copper transporter carrier (CTR1), or copper transporter carrier (CTR2) [80]. CTR1 is a homo-trimeric protein that transports copper across the plasma membrane with high affinity and specificity, driving copper absorption in the animal intestine [81]. In addition, copper ions can be transported to small intestinal cells via the divalent metal transporter (DMT1), a compensatory mechanism when copper uptake by CTR1 is insufficient [82]. After entering the cell, copper or cuprous ions bind to copper chaperone proteins, which transport copper to various locations such as the cytoplasm, mitochondria, Golgi apparatus, and nucleus [73]. In mitochondria, copper ions are required for the production of ATP by the respiratory chain. COX17 is a mitochondrial copper chaperone that assembles cytochrome oxidase in mitochondria and has an important role in maintaining mitochondrial copper homeostasis [50]. ATOX1 binds to cuprous ions in hepatocytes and transports them to the copper-transporting ATPase in the Golgi apparatus [83]. In the Golgi, cuprous ions bind to ATP7A/ATP7B and later expel copper ions from the cell via ATP7A/ATP7B [84, 85]. Copper efflux from cells is dependent on the copper efflux carriers ATP7A and ATP7B, both of which are critical in maintaining copper homeostasis [78]. Mutations in ATP7A and ATP7B cause Menkes disease and Wilson disease. ATP7A and ATP7B are regulated by a variety of factors. Copper metabolism MURR1 structural domain 1 (COMMD1) is an independent system that regulates ATPase quality control and promotes the degradation of ATP7A and ATP7B. On the other hand, COMMMD1 can bind to the N-terminus of ATP7B to promote copper excretion from hepatocytes [86]. Intracellular metallothionein and glutathione chelate copper ions to promote intracellular copper efflux [87]. Copper transport from the epithelial cells of the small intestine to the biliary tract is shown in Fig. 2, and the specific metabolism of copper in hepatocytes is shown in Fig. 3.

The specific process of copper absorption and systemic metabolism in animals. ATOX1, antioxidant 1 copper chaperone; CCS, copper chaperone for superoxide dismutase; Cox17, cytochrome C oxidase assembly protein 17; CP, ceruloplasmin; CU + , copper (I); CU2 + , copper (II); Cyt B, cytochrome B; DMT1, divalent metal transporter 1; SOD1, copper-zinc superoxide dismutase; STEAP, six transmembrane epithelial antigen of the prostate; TGN, trans-Golgi network; CTR1, copper transporter 1; MT, metallothionein; GSH, glutathione

Transport of copper ions in hepatocytes. Copper ions enter the cell via CTR1 and bind to different intracellular proteins such as ATOX1, COX17, and SOD. The ions are excreted via ATP7B. Copper metabolism is a very complex process, and this diagram only shows some of the processes. However, it is worth noting that, unlike small intestinal epithelial cells, ATP7B is mainly expressed in hepatocytes
Clinical Diagnosis
Clinical symptoms of acute copper toxicity are nausea, vomiting, epigastric pain, and diarrhea. Chronic copper toxicity presents with mental depression, anorexia, and jaundice, among other symptoms. Hemolysis occurs in both acute and chronic copper toxicity [88]. By analyzing cases of copper toxicity with hemolysis and hemoglobinuria nephropathy in Boer goats, Bozynski and other researchers found that chronic copper toxicity remains subclinical until the copper content exceeds the hepatic reserve threshold, where it is released from the surrounding tissues. At the same time, external stimuli such as traveling for a long distance, pregnancy, and strenuous exercise can lead to the rupture of copper lysosomes, releasing copper from the liver. Clinical symptoms of acute copper toxicity include abdominal pain, diarrhea, vomiting, anorexia, dewatering, and shock. Pathologic autopsy revealed dark brown changes in the kidneys of the goats, and the bladder contained dark reddish-brown urine [23]. Hemolysis due to chronic copper toxicity has also been studied. Fernandes et al. found that when excess copper in plasma enters and binds to hemoglobin, it causes the formation of methemoglobin and lipid peroxidation, resulting in hemolysis [89].
The clinical signs of acute and chronic copper toxicity are partially similar. Acute copper toxicity has a short course, and cattle can die in a short time after ingesting too much copper. There is an incubation period for chronic copper toxicity, with no obvious clinical symptoms in the early stages of the disease. In clinical diagnosis, copper toxicity needs to be differentiated from other events, such as aflatoxin or cotton phenol intake toxicity. A common diagnostic method for copper toxicity is the determination of copper concentrations in the serum or plasma of poisoned animals. Chronic copper toxicity only occurs when large amounts of copper are released into the serum when copper levels exceed the critical level, and this is accompanied by an increase in liver enzyme activity. Therefore, the monitoring and diagnosis of early chronic copper toxicity is very difficult, and better diagnostic methods still need to be further explored.
Prevention and Treatment
Prevention
The prevention of copper toxicity in animals mainly relies on limiting copper intake. In addition, some researchers have also found experimentally that regulating the ratio of relevant elements in the feed can also prevent copper toxicity. Harker et al. designed feeding experiments with high-copper diets incorporating molybdenum salts, which revealed that the addition of ammonium molybdate to concentrate feeds may be an effective method of reducing the risk of nutritional copper toxicity in housed sheep [90]. Dietary zinc supplementation effectively prevents copper toxicity in sheep arising from feeding [33]. Gooneratne et al. used sheep in their experiments and found that copper toxicity could be prevented or treated by intravenous injection of thiomolybdate in moderate doses [91]. In addition, zinc acetate was applied to a case of hepatic copper toxicity in dogs, where a significant decrease in the concentration of copper in the liver was observed [92].
Treatment
By 1981, whether and how various mineral elements interact with the body of ruminants had not yet been demonstrated. The hypothesis that molybdate reacts with sulfides in the rumen to form thiomolybdate was put forward by Gooneratne et al., who investigated whether thiomolybdate could be used to prevent and treat copper toxicity in sheep by intravenous injection. The results showed that a weekly intake of 100 mg of thiomolybdate is safe [91]. However, exceeding this dose causes diarrhea. Humann-Ziehank et al. designed a long-term copper overdose experiment to observe changes in subclinical outcomes caused by chronic copper toxicity. The results showed that chronic copper toxicity occurred in sheep at 3.7 mg/kg for 84 days. The researchers also observed an increase in the liver’s ability to store copper in response to excessive copper intake. Thiomolybdate intake itself does not cause harmful effects in animals [93].
The clinical diagnosis of copper toxicity is based on elevated copper concentrations in the liver and kidneys. Measuring copper concentrations in tissues of animals with hemolytic disease can further define the cause of the disease and exclude other causative factors. Researchers have suggested that measuring molybdenum concentrations in tissues can further determine whether copper toxicity is secondary or primary. Clinical cases of copper toxicity in sheep are common, and severe copper toxicity is associated with low cure rates and severe economic losses. Detecting subclinical forms of copper toxicity can prevent the risk of outbreaks of copper toxicity in populations. Minervino et al. found that 300 mg/kg dry matter (DM) of zinc helped to prevent excessive accumulation of copper in the liver of sheep [94]. Hidiroglou et al. treated sheep with chronic copper toxicity by supplementing the feed with 0.1 g ammonium molybdate plus 1 g sodium sulfate in regimen I and penicillamine sulfate 50 mg/kg orally in regimen II. Copper excretion was monitored during the treatment period. The results showed a significant and sustained increase in copper excretion during the supplementation period. Feed supplementation with molybdenum and sulfur was very effective in promoting copper excretion and significantly reduced mortality [95]. Dietary supplementation with zinc and copper reduces copper accumulation in the liver of animals. High concentrations of molybdenum, selenium, and iron in feed reduce the absorption of copper in ruminants [96].
In conclusion, the prevention and treatment of chronic copper toxicity depends on the monitoring of hepatic copper during animal feeding; if copper accumulation or copper overload is detected at an early stage, the feed structure needs to be adjusted in a timely manner, and in severe cases, penicillamine can be ingested to detoxify the animal. The duration for acute copper toxicity is short, the mortality rate is high, and because there is no reliable therapeutic solution, treatment of acute copper toxicity still needs further exploration.
Future and Outlook
In the extended sense of copper toxicity, the occurrence of copper toxicity in food animals is a food safety concern. Dairy products or meat from copper-poisoned cows can lead to copper toxicity in humans. Scientists are constantly developing safer copper-containing additives, such as lysine and glutamic acid-copper chelates, to avoid copper toxicity or environmental pollution. Current research on the monitoring and accumulation of trace elements in animals has shed light on the mechanisms of toxicity caused by excess trace elements. Accompanying research can provide effective prediction and prevention of toxicity caused by the accumulation of trace elements. However, the mechanisms behind the pathological changes and clinical symptoms caused by excess trace elements in the body are poorly understood. In addition, research on the metabolic mechanisms of copper toxicity will improve not only the understanding and knowledge of copper toxicity in animals but also in studying diseases related to copper metabolism disorders, such as Wilson’s disease and Menk’s disease. The pathogenic mechanisms of copper toxicity remain to be explored further.
Data Availability
No datasets were generated or analyzed during the current study.
References
Wang Y, Zhang W, Yao Q (2021) Copper-based biomaterials for bone and cartilage tissue engineering. J Orthop Transl 29:60–71. https://doi.org/10.1016/j.jot.2021.03.003
Muttkowski RA (1921) Copper: its occurrence and role in insects and other animals. Trans Am Microsc Soc 40:144. https://doi.org/10.2307/3221584
Hart EB, Steenbock H, Waddell J et al (1928) Iron in nutrition. J Biol Chem 77:797–812. https://doi.org/10.1016/S0021-9258(20)74028-7
Francque SM, Marchesini G, Kautz A et al (2021) Non-alcoholic fatty liver disease: a patient guideline. JHEP Rep 3:100322. https://doi.org/10.1016/j.jhepr.2021.100322
Nývltová E, Dietz JV, Seravalli J et al (2022) Coordination of metal center biogenesis in human cytochrome c oxidase. Nat Commun 13:3615. https://doi.org/10.1038/s41467-022-31413-1
Xue Q, Kang R, Klionsky DJ et al (2023) Copper metabolism in cell death and autophagy. Autophagy 19:2175–2195. https://doi.org/10.1080/15548627.2023.2200554
Cai D, Tu M, Wan D (2022) Editorial: The actions of trace element metabolism and epigenetics on animal health and disease. Front Vet Sci 9:1086322. https://doi.org/10.3389/fvets.2022.1086322
Ogbuewu IP, Mbajiorgu CA (2023) Review of selected trace element contained in tropical medicinal plants utilised in animal production. Appl Ecol Environ Res 21:3791–3805. https://doi.org/10.15666/aeer/2105_37913805
Ruiz LM, Jensen EL, Rossel Y et al (2016) Non-cytotoxic copper overload boosts mitochondrial energy metabolism to modulate cell proliferation and differentiation in the human erythroleukemic cell line K562. Mitochondrion 29:18–30. https://doi.org/10.1016/j.mito.2016.04.005
Marston HR, Lee HJ (1948) The effects of copper deficiency and of chronic overdosage with copper on Border-Leicester and Merino sheep. J Agric Sci 38:229–241. https://doi.org/10.1017/S0021859600005487
Todd JR (1969) Chronic copper toxicity of ruminants. Proc Nutr Soc 28:189–198. https://doi.org/10.1079/PNS19690037
Belli CB, Fernandes WR, Torres LN et al (2021) Copper toxicity in horses: does it exist? J Equine Vet Sci 106:103752. https://doi.org/10.1016/j.jevs.2021.103752
Macleod NS, Watt JA (1970) Experimental copper poisoning in sheep. Vet Rec 86:375–376. https://doi.org/10.1136/vr.86.13.375
Alhazmi HA, Ahsan W, Ibrahim AMM et al (2021) Investigation of bovine serum albumin aggregation upon exposure to silver(i) and copper(ii) metal ions using Zetasizer. Open Chem 19:987–997. https://doi.org/10.1515/chem-2021-0089
Giergiel M, Durkalec MM, Nawrocka A et al (2019) Ingestion of bedding material as a cause of acute copper sulfate poisoning in turkey poults. Poult Sci 98:707–711. https://doi.org/10.3382/ps/pey430
García-Fernández AJ, Motas-Guzmán M, Navas I et al (1999) Sunflower meal as cause of chronic copper poisoning in lambs in southeastern Spain. Can Vet J Rev Veterinaire Can 40:799–801
Johnsen IV, Aaneby J (2024) Accumulation of copper and lead in ruminants grazing on a contaminated shooting range in Nordland County, Norway. Environ Sci Pollut Res Int 31:11026–11036. https://doi.org/10.1007/s11356-023-31609-y
Soli NE, Nafstad I (1976) Chronic copper poisoning in sheep. Structural changes in erythrocytes and organs. Acta Vet Scand 17:316–327. https://doi.org/10.1186/BF03547912
Maryam T, Rana NF, Alshahrani SM et al (2023) Silymarin encapsulated liposomal formulation: an effective treatment modality against copper toxicity associated liver dysfunction and neurobehavioral abnormalities in Wistar rats. Molecules 28:1514. https://doi.org/10.3390/molecules28031514
Yamkate P, Gold RM, Xenoulis PG et al (2021) Assessment of copper accumulation in archived liver specimens from cats. J Feline Med Surg 23:526–533. https://doi.org/10.1177/1098612X20961350
Cooper GL, Bickford AA, Charlton BR et al (1996) Copper poisoning in rabbits associated with acute intravascular hemolysis. J Vet Diagn Invest 8:394–396. https://doi.org/10.1177/104063879600800323
Giadinis ND, Papaioannoy N, Kritsepi-Konstantinou M et al (2009) Acute encephalopathy and clinical pathology findings in a sheep with chronic copper poisoning. Turk J Vet Anim Sci. https://doi.org/10.3906/vet-0809-21
Shimon Barel O, Cuneah JS (2019) Chronic copper toxicosis in dairy cows first case of chronic copper toxicosis in dairy cows in Israel and its remedial management. Isr J Vet Med 74:39–43
Gupta A, Puri S, Aggarwal N et al (2023) Intravascular hemolysis, methemogolbinemia and acute renal failure in a young female. Indian J Nephrol 33:136. https://doi.org/10.4103/ijn.ijn_410_21
Dash SC (1989) Copper sulphate poisoning and acute renal failure. Int J Artif Organs 12:610–610. https://doi.org/10.1177/039139888901201002
Sinkovič A, Strdin A, Svenšek F (2008) Severe acute copper sulphate poisoning: a case report. Arch Ind Hyg Toxicol 59:31–35. https://doi.org/10.2478/10004-1254-59-2008-1847
Abu Damir H, Eldirdiri NI, Adam SE et al (1993) Experimental copper poisoning in the camel (Camelus dromedarius). J Comp Pathol 108:191–208. https://doi.org/10.1016/s0021-9975(08)80221-6
Brooks JW, Whary MT, Hattel AL et al (2006) Clostridium piliforme infection in two farm-raised white-tailed deer fawns (Odocoileus virginianus) and association with copper toxicosis. Vet Pathol 43:765–768. https://doi.org/10.1354/vp.43-5-765
Giudice E, Crinò C, Lanzafame P et al (2017) Acute hypoxemic respiratory failure with hemoptysis in a dog exposed to copper sulfate powder. Top Companion Anim Med 32:36–40. https://doi.org/10.1053/j.tcam.2017.05.004
Ramirez CJ, Kim DY, Hanks BC, Evans TJ (2013) Copper toxicosis in New Zealand White rabbits (Oryctolagus cuniculus). Vet Pathol 50:1135–1138. https://doi.org/10.1177/0300985813490756
Wiederanders RE, Evans GW, Wasdahl WW (1968) Acute and chronic copper poisoning in the rat. J Lancet 88:286–291
Bidewell CA, Drew JR, Payne JH et al (2013) Case study of copper poisoning in a British dairy herd. Vet Rec Case Rep 1:e100267. https://doi.org/10.1136/vetreccr.100267rep
Bremner I (1998) Manifestations of copper excess. Am J Clin Nutr 67:1069S-1073S. https://doi.org/10.1093/ajcn/67.5.1069S
Alkhouri N, Gonzalez-Peralta RP, Medici V (2023) Wilson disease: a summary of the updated AASLD Practice Guidance. Hepatol Commun 7. https://doi.org/10.1097/HC9.0000000000000150
Balemi S, Grace N, West D et al (2010) Accumulation and depletion of liver copper stores in dairy cows challenged with a Cu-deficient diet and oral and injectable forms of Cu supplementation. N Z Vet J 58:137–141. https://doi.org/10.1080/00480169.2010.67515
Zhong G, Li L, Li Y et al (2023) Cuproptosis is involved in copper-induced hepatotoxicity in chickens. Sci Total Environ 866:161458. https://doi.org/10.1016/j.scitotenv.2023.161458
Zhong G, Li Y, Ma F et al (2024) Copper exposure induced chicken hepatotoxicity: involvement of ferroptosis mediated by lipid peroxidation, ferritinophagy, and inhibition of FSP1-CoQ10 and Nrf2/SLC7A11/GPX4 axis. Biol Trace Elem Res 202:1711–1721. https://doi.org/10.1007/s12011-023-03773-2
Alhusaini A, Fadda L, Hassan I et al (2018) Liposomal curcumin attenuates the incidence of oxidative stress, inflammation, and DNA damage induced by copper sulfate in rat liver. Dose-Response Publ Int Hormesis Soc 16:1559325818790869. https://doi.org/10.1177/1559325818790869
Jiang T, Guo H, Xia Y-N et al (2021) Hepatotoxicity of copper sulfide nanoparticles towards hepatocyte spheroids using a novel multi-concave agarose chip method. Nanomed 16:1487–1504. https://doi.org/10.2217/nnm-2021-0011
Huo Y, Ma F, Li L et al (2023) Effect of copper exposure on the cholesterol metabolism in broiler liver. Biol Trace Elem Res 201:5747–5755. https://doi.org/10.1007/s12011-023-03609-z
Li M, Tang S, Velkov T et al (2024) Copper exposure induces mitochondrial dysfunction and hepatotoxicity via the induction of oxidative stress and PERK/ATF4-mediated endoplasmic reticulum stress. Environ Pollut 352:124145. https://doi.org/10.1016/j.envpol.2024.124145
Sutunkova MP, Ryabova YV, Minigalieva IA et al (2023) Features of the response to subchronic low-dose exposure to copper oxide nanoparticles in rats. Sci Rep 13:11890. https://doi.org/10.1038/s41598-023-38976-z
Wang L, Guan T, Wang G et al (2023) Effects of copper on gill function of juvenile oriental river prawn (Macrobrachium nipponense): stress and toxic mechanism. Aquat Toxicol 261:106631. https://doi.org/10.1016/j.aquatox.2023.106631
Pantic S, Skodric SR, Loncar Z, Pantic I (2019) Neurotoxocity, nephrotoxicity, and hepatotoxicity of copper-based nanoparticles: potential implications in molecular medicine and neurosciences. Rev Adv Mater Sci 58:201–205. https://doi.org/10.1515/rams-2019-0032
Fuentealba IC, Haywood S, Foster J (1989) Cellular mechanisms of toxicity and tolerance in the copper-loaded rat. III. Ultrastructural changes and copper localization in the kidney. Br J Exp Pathol 70:543–556
Liao M, Liu H (2012) Gene expression profiling of nephrotoxicity from copper nanoparticles in rats after repeated oral administration. Environ Toxicol Pharmacol 34:67–80. https://doi.org/10.1016/j.etap.2011.05.014
Khalid S, Afzal N, Khan JA et al (2018) Antioxidant resveratrol protects against copper oxide nanoparticle toxicity in vivo. Naunyn Schmiedebergs Arch Pharmacol 391:1053–1062. https://doi.org/10.1007/s00210-018-1526-0
Elazab ST, Elshater NS, Kishaway ATY, EI-Emam HA, (2021) Cinnamon extract and probiotic supplementation alleviate copper-induced nephrotoxicity via modulating oxidative stress, inflammation, and apoptosis in broiler chickens. Animals 11:1609. https://doi.org/10.3390/ani11061609
Gopinath C, Hall GA, Howell JM (1972) The effects of experimental chronic copper poisoning on the kidneys of sheep. J Pathol 106:P8
Zhu S, Wu H, Cui H et al (2023) Induction of mitophagy via ROS-dependent pathway protects copper-induced hypothalamic nerve cell injury. Food Chem Toxicol Int J Publ Br Ind Biol Res Assoc 181:114097. https://doi.org/10.1016/j.fct.2023.114097
Yu W, Chang X, Liao J et al (1987) (2023) Long-term oral tribasic copper chloride exposure impedes cognitive function and disrupts mitochondrial metabolism by inhibiting mitophagy in rats. Environ Pollut Barking Essex 336:122474. https://doi.org/10.1016/j.envpol.2023.122474
Howell JM, Blakemore WF, Gopinath C et al (1974) Chronic copper poisoning and changes in the central nervous system of sheep. Acta Neuropathol (Berl) 29:9–24. https://doi.org/10.1007/BF00684387
Chen L, Min J, Wang F (2022) Copper homeostasis and cuproptosis in health and disease. Signal Transduct Target Ther 7:378. https://doi.org/10.1038/s41392-022-01229-y
Tchounwou PB, Newsome C, Williams J, Glass K (2008) Copper-induced cytotoxicity and transcriptional activation of stress genes in human liver carcinoma (HepG(2)) cells. Met Ions Biol Med Proc Int Symp Met Ions Biol Med Held Ions Met En Biol En Med Symp Int Sur Ions Met 10:285–290
Tsvetkov P, Coy S, Petrova B et al (2022) Copper induces cell death by targeting lipoylated TCA cycle proteins. Science 375:1254–1261. https://doi.org/10.1126/science.abf0529
Levine B, Kroemer G (2019) Biological functions of autophagy genes: a disease perspective. Cell 176:11–42. https://doi.org/10.1016/j.cell.2018.09.048
Tsang T, Posimo JM, Gudiel AA et al (2020) Copper is an essential regulator of the autophagic kinases ULK1/2 to drive lung adenocarcinoma. Nat Cell Biol 22:412–424. https://doi.org/10.1038/s41556-020-0481-4
Suttle NF (2012) Copper imbalances in ruminants and humans: unexpected common ground. Adv Nutr 3:666–674. https://doi.org/10.3945/an.112.002220
Nederbragt H, Van Den Ingh TSGAM, Wensvoort P (1984) Pathobiology of copper toxicity. Vet Q 6:179–235. https://doi.org/10.1080/01652176.1984.9693935
Kurek Ł, Kurek Ł, Olech M et al (2017) Long-term subclinical copper deficiency and it is influence on functions of parenchymal organs and the serum macro-element deficiency in dairy cows. J Elem. https://doi.org/10.5601/jelem.2017.22.1.1417
Van Beest FM, Schmidt NM, Frederiksen ML et al (2024) Direct and indirect linkages between trace element status and health indicators - a multi-tissue case-study of two deer species in Denmark. Biol Trace Elem Res 202:3623–3638. https://doi.org/10.1007/s12011-023-03926-3
Ward JD, Spears JW, Gengelbach GP (1995) Differences in copper status and copper metabolism among Angus, Simmental, and Charolais cattle. J Anim Sci 73:571–577. https://doi.org/10.2527/1995.732571x
Haywood S, Simpson DM, Ross G, Beynon RJ (2005) The greater susceptibility of North Ronaldsay sheep compared with cambridge sheep to copper-induced oxidative stress, mitochondrial damage and hepatic stellate cell activation. J Comp Pathol 133:114–127. https://doi.org/10.1016/j.jcpa.2005.02.001
Borobia M, Villanueva-Saz S, Ruiz De Arcaute M et al (2022) Copper poisoning, a deadly hazard for sheep. Animals 12:2388. https://doi.org/10.3390/ani12182388
Oruc HH, Cengiz M, Beskaya A (2009) Chronic copper toxicosis in sheep following the use of copper sulfate as a fungicide on fruit trees. J Vet Diagn Invest 21:540–543. https://doi.org/10.1177/104063870902100420
Huang C, Shi Y, Zhou C et al (2021) Effects of subchronic copper poisoning on cecal histology and its microflora in chickens. Front Microbiol 12:739577. https://doi.org/10.3389/fmicb.2021.739577
Hashem MA, Abd El Hamied SS, Ahmed EMA et al (2021) Mitigating the growth, biochemical changes, genotoxic and pathological effects of copper toxicity in broiler chickens by supplementing vitamins C and E. Animals 11:1811. https://doi.org/10.3390/ani11061811
Gao Y, Yang W, Che D et al (2020) Advances in the mechanism of high copper diets in restraining pigs growth. J Anim Physiol Anim Nutr 104:667–678. https://doi.org/10.1111/jpn.13213
Li Y, Chen H, Liao J et al (2021) Long-term copper exposure promotes apoptosis and autophagy by inducing oxidative stress in pig testis. Environ Sci Pollut Res 28:55140–55153. https://doi.org/10.1007/s11356-021-14853-y
Ma Z, Li Y, Han Z et al (2021) Excessive copper in feed not merely undermines animal health but affects food safety. J Vet Sci 22:e31. https://doi.org/10.4142/jvs.2021.22.e31
Van Den Berghe PV, Klomp LW (2009) New developments in the regulation of intestinal copper absorption. Nutr Rev 67:658–672. https://doi.org/10.1111/j.1753-4887.2009.00250.x
Wapnir R (1998) Copper absorption and bioavailability. Am J Clin Nutr 67:1054S-1060S. https://doi.org/10.1093/ajcn/67.5.1054S
Liu T, Liu Y, Zhang F, Gao Y (2023) Copper homeostasis dysregulation promoting cell damage and the association with liver diseases. Chin Med J (Engl) 136:1653–1662. https://doi.org/10.1097/CM9.0000000000002697
Liu Y, Miao Ji (2022) An emerging role of defective copper metabolism in heart disease. Nutrients 14:700. https://doi.org/10.3390/nu14030700
Linder MC (2016) Ceruloplasmin and other copper binding components of blood plasma and their functions: an update. Metallomics 8:887–905. https://doi.org/10.1039/C6MT00103C
Puig S, Thiele DJ (2002) Molecular mechanisms of copper uptake and distribution. Curr Opin Chem Biol 6:171–180. https://doi.org/10.1016/S1367-5931(02)00298-3
Georgatsou E, Mavrogiannis LA, Fragiadakis GS, Alexandraki D (1997) The yeast Fre1p/Fre2p cupric reductases facilitate copper uptake and are regulated by the copper-modulated Mac1p activator. J Biol Chem 272:13786–13792. https://doi.org/10.1074/jbc.272.21.13786
Lutsenko S, Barnes NL, Bartee MY, Dmitriev OY (2007) Function and regulation of human copper-transporting ATPases. Physiol Rev 87:1011–1046. https://doi.org/10.1152/physrev.00004.2006
Ohgami RS, Campagna DR, McDonald A, Fleming MD (2006) The Steap proteins are metalloreductases. Blood 108:1388–1394. https://doi.org/10.1182/blood-2006-02-003681
Wu G, Peng H, Tang M, et al (2021) ZNF711 down-regulation promotes CISPLATIN resistance in epithelial ovarian cancer via interacting with JHDM2A and suppressing SLC31A1 expression. eBioMedicine 71:103558. https://doi.org/10.1016/j.ebiom.2021.103558
Nose Y, Kim B-E, Thiele DJ (2006) Ctr1 drives intestinal copper absorption and is essential for growth, iron metabolism, and neonatal cardiac function. Cell Metab 4:235–244. https://doi.org/10.1016/j.cmet.2006.08.009
Tsai C-Y, Liebig JK, Tsigelny IF, Howell SB (2015) The copper transporter 1 (CTR1) is required to maintain the stability of copper transporter 2 (CTR2). Metallomics 7:1477–1487. https://doi.org/10.1039/C5MT00131E
Jomova K, Makova M, Alomar SY et al (2022) Essential metals in health and disease. Chem Biol Interact 367:110173. https://doi.org/10.1016/j.cbi.2022.110173
Fodor I, Yañez-Guerra LA, Kiss B et al (2023) Copper-transporting ATPases throughout the animal evolution – from clinics to basal neuron-less animals. Gene 885:147720. https://doi.org/10.1016/j.gene.2023.147720
Polishchuk EV, Concilli M, Iacobacci S et al (2014) Wilson disease protein ATP7B utilizes lysosomal exocytosis to maintain copper homeostasis. Dev Cell 29:686–700. https://doi.org/10.1016/j.devcel.2014.04.033
de Bie P, van de Sluis B, Klomp L, Wijmenga C (2005) The many faces of the copper metabolism protein MURR1/COMMD1. J Hered 96:803–811. https://doi.org/10.1093/jhered/esi110
Corbee RJ, Penning LC (2021) COMMD1 exemplifies the power of inbred dogs to dissect genetic causes of rare copper-related disorders. Animals 11:601. https://doi.org/10.3390/ani11030601
Gunay N, Yildirim C, Karcioglu O et al (2006) A series of patients in the emergency department diagnosed with copper poisoning: recognition equals treatment. Tohoku J Exp Med 209:243–248. https://doi.org/10.1620/tjem.209.243
Fernandes A, Mira ML, Azevedo MS, Manso C (1988) Mechanisms of hemolysis induced by copper. Free Radic Res Commun 4:291–298. https://doi.org/10.3109/10715768809066894
Harker DB (1976) The use of molybdenum for the prevention of nutritional copper poisoning in housed sheep. Vet Rec 99:78–81. https://doi.org/10.1136/vr.99.5.78
Gooneratne SR, Howell JM, Gawthorne JM (1981) Intravenous administration of thiomolybdate for the prevention and treatment of chronic copper poisoning in sheep. Br J Nutr 46:457–467. https://doi.org/10.1079/BJN19810054
Brewer GJ, Dick RD, Schall W et al (1992) Use of zinc acetate to treat copper toxicosis in dogs. J Am Vet Med Assoc 201:564–568
Humann-Ziehank E, Coenen M, Ganter M, Bickhardt K (2001) Long-term observation of subclinical chronic copper poisoning in two sheep breeds. J Vet Med Ser A 48:429–439. https://doi.org/10.1046/j.1439-0442.2001.00376.x
Minervino A, López-Alonso M, Barrêto Júnior R et al (2018) Dietary zinc supplementation to prevent chronic copper poisoning in sheep. Animals 8:227. https://doi.org/10.3390/ani8120227
Hidiroglou M, Heaney DP, Hartin KE (1984) Copper poisoning in a flock of sheep. Copper excretion patterns after treatment with molybdenum and sulfur or penicillamine. Can Vet J Rev Veterinaire Can 25:377–382
Spears JW (2000) Micronutrients and immune function in cattle. Proc Nutr Soc 59:587–594. https://doi.org/10.1017/S0029665100000835
Funding
This research was funded by the National Natural Science Foundation of China (grant nos. 32273074, 31972746, 31772809, and 31872538) and through a Key Grant Project of Liaoning Provincial Department of Education (grant no. LJKZ0632).
Author information
Authors and Affiliations
Contributions
Writing—original draft preparation, Yudong Wang; writing—review and editing, Qiushi Yan and Yang Shi; Supervision, Miao Long.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, Y., Yan, Q., Shi, Y. et al. Copper Toxicity in Animals: A Review. Biol Trace Elem Res (2024). https://doi.org/10.1007/s12011-024-04345-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12011-024-04345-8