
Abstract
Magnesium (Mg) is an essential nutrient as a structural constituent of bone and regulator of >300 enzymes. However, studies on intake and urinary excretion of Mg are limited. The purpose of this study was to evaluate Mg intake and its relation to 24-h urinary excretion in healthy adults. Anthropometric measurements and dietary intake by the 24-h recall method were conducted in 80 adults aged 21–69 (average 44.3) years. Urine was collected for 24 h on the day following the dietary survey. Dietary assessment and 24-h urine collection were repeated 3 days later. Daily intake and urinary excretion of Mg were analyzed using Can-Pro and ICP-OES, respectively. The statistical analysis was conducted using SAS program. Mg intake of the subjects was 319 ± 129 mg/day for men and 277 ± 94 mg/day for women and the proportion of subjects who did not meet the estimated average requirement was 50 and 67.5 % for men and women, respectively. Urinary Mg excretion was 30.3 % of the daily Mg intake. Urinary Mg excretion was not significantly correlated with the daily Mg intake. Korean adults are not meeting the recommended intake of Mg, but its urinary excretion suggests homeostasis is not compromised.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The content of magnesium (Mg) is the sixth highest within the body after calcium, phosphorus, potassium, sodium, and chloride and its content is the second highest after potassium as a cation of intracellular fluid [1]. Mg maintains bone integrity as a component of bone and teeth, stabilizes cell membranes, is a coenzyme of diverse enzymes within our body, delivers neural stimulation, takes part in synthesis of fat, protein, nucleic acid, etc. [1]. There have been consistent findings that adequate intake of Mg plays an important role not only for bone health, but also for prevention of non-communicable diseases, particularly that of cardiovascular disease [2–4]. The DASH diet for hypertension prevention recommends sufficient intake of Mg and other cations [5].
Since Mg exists as a compound of the chlorophyll porphyrin within plants, its content is high in green leafy vegetables. However, when food is processed and cooked, Mg is lost. During refinement of grain, as much as 80 % of Mg is lost and 50 % is lost during cooking of some vegetables [6, 7]. Food groups with the highest contributions of Mg intake for Koreans are grains and vegetables; the three top sources are rice, tofu, and kimchi [8]. Based on an analysis of the 2007–2008 Korea National Health and Nutrition Examination Survey (KNHANES), Mg intake of adults over age 19 years averaged 321 mg/day for men and, for women, 247 mg/day [9]. These intakes are over 80 % of the recommended intake (RI). In contrast, in another study [8], women of average age 20.2 years consumed 186 mg Mg/day or 63 % of the RI. Similarly, low Mg intakes were reported for both adult men and women at 187 and 189 mg/day, respectively [10]. The intake of Mg was sufficient when vegetables were the center of the dietary life of Koreans in which meat intake was traditionally low [11]. Mg deficiency may become a problem with the current trends of increased meat intake and relative decrease in vegetable intake [12, 13].
Mg is well absorbed through the intestinal tract, mainly by simple diffusion and active transport in the jejunum and ileum. Mg absorption is disproportionate to intake in that it is usually 40–60 % from regular meals, but up to 75 % for Mg-deficient individuals and 25 % for Mg-replete individuals [14]. Homeostasis of Mg within the body is mainly regulated by the kidney [15]. Mg control in the kidney is mostly by filtration and reabsorption and there rarely is tubule secretion. About 65 % of filtered Mg is reabsorbed at Henle’s loop, 20–30 % absorbed at the tubule, and the remaining 3–5 % is excreted via urine [15]. Serum Mg is a less reliable indicator of Mg status because only approximately 0.3 % of the body Mg is in that body pool [16]. Most studies only report intake of Mg and do not assess urinary excretion level or their relation. Therefore, the purpose of this study was to assess the daily intake and urinary excretion of Mg on self-selected diets in Korean adults and relate excretion to Mg intake.
Materials and Methods
Subjects
The subjects of this study were 80 adults on self-selected diets. Since the age range of adults is wide, 80 men and women were recruited into each of five age groups, i.e., 19–29, 30–39, 40–49, 50–59, and 60–69 years. The volunteers were recruited by posting a study subject recruitment announcement on the websites of self-governing society organization. Among study volunteers, those with a diagnosis of hypertension, cardiac failure, diabetes, kidney disease, cancer, or other diseases could affect validity of data; those under medication and diet control and pregnant lactating women were excluded. This study was approved by the Institutional Review Board of Kyungbuk National University (IRB 2014–0053) and it was conducted upon reception of consent from study participants.
Anthropometric Measurement
Height of the subjects was measured using an extensometer without shoes. Weight was measured with the use of In Body (X-SCAN PLUS II, Biospace, Seoul, Korea) with minimal clothing. Body mass index (BMI) was calculated as weight in kilograms divided by squared height in meters. Blood pressure was measured with the use of automatic sphygmomanometer (Microlife WatchBP Home 3MX1–1, Switzerland) after the subjects rested for 10 min in sitting posture. When outside the normal range of blood pressure, subjects were excluded. All measurements were repeated twice and the averaged value of two-time measurements was reported.
Dietary Intake Survey and Analysis
Dietary assessment was conducted twice at intervals of 3 days with both food records and modified 24-h recalls. Dietary sheets were provided to the subjects in advance so that subjects could directly record food intake followed by 24-h recall interviews. Interviews were conducted by a researcher based on the diet record. Dietary intake surveys were conducted for meals from rising in the morning until bedtime on week days excluding weekends and holidays. In order to increase the accuracy of intake, auxiliary tools including actual photo of ingredients and food, tape measure, food replicas, and containers were utilized. Also, the subjects were instructed to take a photo of each meal during the assessment to be utilized for diet record corrections and the 24-h recall interview. During the 24-h recall interview, researchers recorded the name and quantity of food intake by the subject and the name and quantity of ingredients in the food. In the case of processed food, the name of the product and manufacturer was recorded. Also, the type and quantity of dietary supplement and health functional food were examined. Quantity of intake on the day of the survey was examined in comparison with normal intake. This was accomplished by asking subjects to select if intake was more, similar, or less than normal intake. Intake of not only beverage such as coffee, tea, or others but also water was recorded. Based on the findings of the 24-h recall, the analysis on energy and nutrient intakes were conducted using CAN-Pro 4.0 (Computer Aided Nutritional Analysis program version 4.0, Korea Nutrition Society, 2010). The subjects of this study consumed 465 food items based on 24-h dietary recall data. Regarding food intake, 31.6 % of the items had information on Mg contents in the database of CAN-Pro 4.0, which is very low. Therefore, Mg intakes of the subjects were calculated using Mg content databases produced by previous studies [17] and the food composition table of the National Rural Living Science Institute, Korea [18]. Mg content of foods not included in the Mg content database was calculated by replacing it with similar food in the database.
Urine Collection and Analysis
Urine collection for 24 h was conducted twice after a 1-day lag following diet assessment. The subjects were instructed to collect urine in 500-mL urine beakers at every urination and to record the quantity of urination. Then, all urine during each 24-h time period was transferred to a urine bag. Urine collection time was 24 h from the start of urine collection between 6 and 9 a.m. on the day of the 24-h urine collection to the next day. The subjects were instructed to throw away the first urine after the start of urine collection and begin collection from the next urine. The urine at the end of urine collection was to be collected. When there was a necessity to adjust the test date due to difficulties such as urine loss or menstrual period of women participants, a minimum interval of 3 days was required between the first and second 24-h urine collection. Compliance with 24-h urine collections was confirmed when the value of [collected urine quantity/(weight × 21)] was over 0.7. When the value was lower than 0.7, the data were excluded from the analysis target and also when the creatinine concentration of 24-h urine was lower than reference (value estimated based on sex, age, and weight of subject) [19]. The quantity of 24-h urine was measured with the use of a mass cylinder and a sample of about 20 ml urine was separated in order to analyze creatinine and Mg concentration. Urinary creatinine was analyzed by colorimetric assay and Mg content was analyzed by inductively coupled plasma optical emission spectroscopy (ICP-OES, Optima 5300 DV, PerkinElmer, MA, USA) after centrifugation of urine at ×400 g for 15 min. The relative standard deviation gained from three repeated analyses of the urine sample was within 3 %.
Statistical Analysis
Statistical analysis was conducted using SAS program (Ver. 9.4, SAS Institute Inc., Cary, NC, USA). Means and standard deviations were calculated. Differences in the variables between men and women were assessed using the unpaired Student’s t test. For determining mean differences for all variables for each age group, post hoc analysis using Duncan’s test was conducted when indicated by ANOVA test. The correlation between each variable was evaluated for its significance using Pearson’s correlation test and then partial correlation was conducted after adjusting sex, age, BMI, and food intake as potential confounding factors that have potential impacts on daily intake and excretion of Mg. Significance verification of all statistical analysis was conducted at a level of p < 0.05.
Results
General Characteristics of the Subjects
Age and anthropometric measurements of the subjects are shown in Table 1. The average age of all subjects was 44.3 years and there was no significant difference between men and women. Although height, weight, BMI, and systolic blood pressure were significantly higher in men compared to women, there was no significant difference in diastolic blood pressure.
Daily Mg Intake of the Subjects
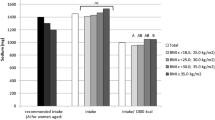
Daily energy intake was significantly higher in men at 2129 kcal compared to 1732 kcal for women (p < 0.01), and carbohydrate, fat, and protein intakes were significantly higher in men compared to women (Table 2). For Mg intake, there was no significant difference between men and women at 319 and 277 mg/day, respectively. These intakes represented 87.3 and 75.7 % of the RI. The proportion of subjects below the estimated average requirement (EAR) was 50 and 67.5 % for men and women, respectively, and the proportion of subjects falling below 75–125 % of the RI was 52.5 and 37.5 % for men and women, respectively (Table 2). Mg intake from each food group was indicated in Table 3 and there was no significant difference between men and women. Mg intake from the vegetable group was the highest at 24.7 % of total intake followed by grains (14.8 %), fish and shellfish (12 %), and beans (11.7 %). The rank of foods contributing to Mg intake was tofu, kimchi, and rice; about 50 % of the total Mg intake was from 20 types of food (Fig. 1).

Major food sources of dietary magnesium of the Korean participants
Comparison of Daily Intake and Urinary Excretion of Mg According to Age Group
Mg intake and urinary excretion during 24 h according to sex and age of the subjects are shown in Table 4. Mg intake was highest in women in their 50s at 394 mg/day and lowest in men in their 50s at 251 mg/day (p < 0.05). Urinary excretion of Mg was significantly higher in men compared to women (p < 0.01); it was highest in women in their 50s at 106 mg. However, there was no significant difference in the proportion of urinary Mg excretion per daily Mg intake by sex and age. The relation between Mg intake and urinary Mg excretion for the entire population is shown in Fig. 2. Average Mg excretion was 30.3 % of intake.

Relation between magnesium intake and urinary magnesium excretion of the participants
Correlation Among Urinary Mg Excretion, Energy and Mg Intakes
There was no significant correlation between urinary Mg excretion and total daily Mg intake (Table 5). Urinary Mg excretion was significantly positively correlated with carbohydrate intake (p < 0.05), Mg intake from grains (p < 0.05), and Mg intake from seasoning (p < 0.05). However, after adjusting for confounding factors of sex, height, BMI, and food intake, urinary Mg excretion was significantly positively correlated only with Mg intake from grains (p < 0.05).
Discussion
This study was conducted to evaluate daily Mg intake and urinary excretion of Mg and their relation in adults on self-selected diets. Daily Mg intake of the subjects was 319 mg/day for men and 277 mg/day for women, representing 87.3 and 75.7 % levels of the RI, respectively. The proportion of subjects below the EAR was relatively high at 50 % for men and 67.5 % for women. Daily Mg excretion in urine was 30.3 % of the daily Mg intake. Urinary Mg excretion was not significantly correlated with daily Mg intake.
Mg is an essential nutrient, and its adequate intake plays an important role in not only skeletal structure but also cell function and general metabolism in the body. Mg is contained in various foods including cereals and vegetables as main food groups so should not be deficient. However, the recent decrease of plant foods and increased intake of processed foods and animal foods in the Korean diet leads to concern over inadequate Mg intake [12].
In previous studies on Mg intake conducted in Korea, it has been reported that intake of Mg is 239–350 mg/day in adults which is more than 80 % of the RI [9, 17, 20–24]. In ten European countries, Mg intake determined with the 24-h recall method varied by country from 347 mg/day in Sweden to 467 mg/day in Germany for males and from 258 mg/day in Greece to 402 mg/day in France for females [25]. Papanikolaosu et al. [26] who analyzed 2007–2010 NHANES data reported that Mg intake of adults at the age of 19 or older was 272 mg/day in non-Hispanic black and 346 mg/day in non-Hispanic white. Mg intake of the subjects in our study was 319 mg/day for males and 277 mg/day for females. These levels were a little lower than those of previous studies, but were about 87.3 and 75.7 % of the RI, respectively. This is encouraging as a group. However, when Mg intake of the subjects in this study was evaluated by individuals, the proportion of persons who did not meet the EAR was 50 % for males and 67.5 % for females. The proportion of persons who did not reach 75 % of the RI was 40 % for males and 60 % for females. Similarly, Papanikolaou et al. [26] reported that participants’ average intake of Mg was satisfactory, but the proportion of participants who did not meet the EAR was high at 68.7 % for non-Hispanic blacks and 42.8 % for non-Hispanic whites. When bone health and cardiovascular disease prevention are affecting large portions of society, screening intake of Mg and other important minerals for nutritional management to increase intake is prudent.
Dietary patterns influence Mg intake which can be influenced by culture. In a study conducted in the USA on various races, non-Hispanic blacks were found to consume more cholesterol and less K, cellulose, dairy products, fruits, and vegetables than non-Hispanic whites [27–29]. Newby et al. [30] reported that non-Hispanic blacks ate a smaller average amount of minerals and vitamins including Mg than non-Hispanic whites. Kim et al. [8] reported that food groups making the largest contribution to Mg intake in young adult women were cereals, followed by vegetables, and food sources making the largest contribution to Mg intake were rice, tofu, and kimchi. The percentage of Mg intake from food groups in our study was high in vegetables (24.7 %), cereals (14.8 %), fish and shellfishes (12 %), and beans (11.7 %). The food item making the largest contribution was tofu, followed by kimchi and rice. Mg content is high in green leafy vegetables, and a large amount of Mg is contained in various plant foods such as unrefined cereals, beans, nuts, and seeds [31]. In particular, tofu is high in Mg content due to Mg in brine used in manufacturing tofu. Tofu is one of the major food sources making a contribution to Mg intake in the Korean diet [12]. As mentioned in the assessment of Mg intake, it is thought that participants low in Mg intake ate a small amount of these food sources of Mg. Therefore, nutritional management should target increased intake of food groups such as vegetables, cereals, and beans.
We compared Mg intake and urinary excretion according to gender and age group in order to investigate the relation between Mg intake and urinary excretion. For a normal glomerular filtration rate, approximately 2000–2400 mg/day of Mg is filtered. Approximately 95 % of filtered Mg is reabsorbed. The other 3–5 % or so is excreted in the urine [32]. For subjects in this study, urinary excretion of Mg was 61–106 mg/day, and was in the normal range. This study did not analyze fecal Mg excretion of the subjects, from which Mg absorption rate could be estimated. So, it is not possible to discuss Mg balance. In this study, the amount of Mg in the urine was shown on average about 30 % of Mg intake, but urinary Mg did not reflect intake on an individual level.
Assessment of Mg status is difficult as there is no simple, rapid, and accurate test to indicate total body Mg status [33]. Mg transfer among some body pools is slow and not accessible in humans. Mg concentration in a certain tissue cannot accurately reflect Mg status in the body [34]. At present, the Mg loading test is a gold standard for assessing the nutritional status of Mg. However, the Mg loading test can only be applied to people whose kidney and intestine functions are normal [35]. Mg in the urine should represent recent diet, but because of rapid adaptation of the kidney to the diet, urinary Mg cannot reflect Mg status in the body [34]. This study evaluated the strength of 24-h urinary excretion of Mg in representing the previous daily Mg intake. However, Mg in the urine was not significantly correlated with Mg intake. Klevay and Milne [36] reported that restriction of Mg intake, 130 mg/day, for 81 days resulted in decreased urinary loss. Some studies [37–39] also reported low urinary Mg as an early sign of depletion. However, in our study, Mg intake of 298 mg/day was relatively higher than previous studies that reported Mg-deficient status. When this intake level was applied in the model of Hunt and Johnson [40], neutral Mg balance was predicted and Mg output represented 94 % of the previous day’s intake. This indicates that the average Mg intake of 298 mg/day is higher than the intake level to maintain neutral Mg balance. Even though the daily Mg intake of the subjects with self-selected diets was not sufficient in some individuals, their Mg intakes were not low enough to trigger physiological homeostatic adaptations to conserve Mg at the kidney. Nevertheless, urinary Mg showed significant positive correlations with Mg intake from grains. This should be further evaluated.
This study has the following limitations. In analyzing Mg intake, the Mg food composition database was not sufficient. So, an analysis was made with database coverage of 88.6 %. Accordingly, there is a possibility that Mg intake may be underestimated. Second, fecal excretion of Mg was not measured, so it was not possible to consider Mg absorption rate or balance status. Finally, the number of study participants is small. However, this study has the following strengths. In order to accurately analyze Mg intake and excretion, the 24-h recall method was improved and used for dietary evaluation with two assessments. It is expected that the results of this study can be utilized in various Mg-related studies in the future by closely examining the relation between 24-h urinary excretion and intake of Mg in the situation when there is difficulty in assessing the nutritional status of Mg.
Conclusion
Daily Mg intake of adults with self-selected diets was 319 mg for men and 277 mg for women, representing 87.3 and 75.7 % of the RI. The proportion of subjects below the EAR was relatively higher at 50 % for men and 67.5 % for women. Urinary Mg excretion was 30.3 % of the daily Mg intake, regardless of the intake, so it did not reflect the status in this population. Urinary Mg reflects status only at lower Mg intake than in this Korean cohort.
References
Wester PO (1987) Magnesium. Am J Clin Nutr 45:1305–1312
Touyz RM (2003) Role of magnesium in the pathogenesis of hypertension. Mol Asp Med 24:107–136
Ford ES, Li C, McGuire LC, Mokdad AH, Liu S (2007) Intake of dietary magnesium and the prevalence of the metabolic syndrome among U.S. adults. Obesity 15:1139–1146
Hruby A, O’Donnell CJ, Jacques PF, Meigs JB, Hoffmann U, McKeown NM (2014) Magnesium intake is inversely associated with coronary artery calcification: the Framingham Heart Study. JACC Cardiovasc Imaging 7:59–69
Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MM, Lin PH, Karanja N (1997) A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med 336:1117–1124
Schroeder HA, Nason AP, Tipton IH (1969) Essential metals in man: magnesium. J Chronic Dis 21:815–841
Severi S, Bedogni CT, Manzieri AM, Poli M, Battistini N (1997) Effects of cooking and storage methods on the micronutrient content of foods. Eur J Cancer Prev 6:S21–S24
Kim MH, Yeon JY, Choi MK, Bae YJ (2011) Evaluation of magnesium intake and its relation with bone quality in healthy young Korean women. Biol Trace Elem Res 144:109–117
Choi MK, Bae YJ (2013) Relationship between dietary magnesium, manganese, and copper and metabolic syndrome risk in Korean adults: the Korea National Health and Nutrition Examination Survey(2007-2008). Biol Trace Elem Res 156:56–66
Son SM, Huh GY (2006) Dietary risk factors associated with hypertension in patients. Korean J Comm Nutr 11:661–672
Sung CJ (1990) A study of Mg status in adult Korean rural women on self-selected diet. Korean J Nutr 23:25–36
The Ministry of Health and Welfare, Korean Center for Disease Control and Prevention (20.1.3) National health statistics. Korea Center for Disease Control and Prevention, Seoul
Marier JR (1986) Magnesium content of the food supply in the modern-day world. Magnesium 5:1–8
Kayne LH, Lee DB (1993) Intestinal magnesium absorption. Miner Electrolyte Metab 19:210–217
Quamme GA, Dirks JH (1986) The physiology of renal magnesium handling. Renal Physiol 9:257–269
Jahnen-Dechent W, Ketteler M (2012) Magnesium basics. Clin Kidney J 5:i3–i14
Bae YJ, Kim MH, Choi MK (2010) Analysis of magnesium contents in commonly consumed foods and evaluation of its daily intake in Korean independent-living subjects. Biol Trace Elem Res 135:182–199
Rural Development Administration, National Institute of Agricultural Science (2011) Food composition table. Kwangmundang Press, Seoul
Blackburn GL, Bistrian BR, Maini BS, Schlamm HT, Smith MF (1977) Nutritional and metabolic assessment of the hospitalized patient. JPEN 1:11–22
Sung CJ, Rho SN, Kim AJ, Choi MK, Lee JH (1993) Relationship among dietary intakes, blood levels, and urinary excretions of Ca, P, Mg and serum lipid levels in Korean rural adult men and women. J Korean Soc Food Nutr 22:709–712
Sung CJ, Choi YH, Kim MH, Choi SH, Cho KO (2002) A study of nutrient intake and serum levels of osteocalcin, Ca, P, and Mg and their correlation to bone mineral density in Korean postmenopausal women residing in rural area. Korean J Community Nutr 7:111–120
Kim SK, Sunwoo JG, Lee EJ (2006) Relation of mineral nutrition status and climacteric symptoms in pre- and postmenopausal women. Korean J Nutr 39:121–132
Yun ME, Lee DH, Kim MH (2008) Effects of soy isoflavones supplementation and exercise on urinary calcium, magnecium, copper and zinc excretion in postmenopausal women. Korean J Nutr 41:612–620
Yeon JY, Sung CJ (2011) A study on dietary mineral intakes, urinary mineral excretions, and bone mineral density in Korean postmenopausal women. Korean J Comm Nutr 16:569–579
Welch AA, Fransen H, Jenab M, Boutron-Ruault MC, Tumino R, Agnoli C, Ericson U, Johansson I, Ferrari P, Engeset D, Lund E, Lentjes M, Key T, Touvier M, Niravong M, Larrañaga N, Rodríguez L, Ocké MC, Peeters PHM, Tjønneland A, Bjerregaard L, Vasilopoulou E, Dilis V, Linseisen J, Nöthlings U, Riboli E, Slimani N, Bingham S (2009) Variation in intakes of calcium, phosphorus, magnesium, iron and potassium in 10 countries in the European Prospective Investigation into Cancer and Nutrition study. Eur J Clin Nutr 63:S101–S121
Papanikolaou Y, Brooks J, Reiders J, Fulgoni VL (2015) Comparison of inadequate nutrient intakes in non-Hispanic blacks vs. non-Hiapanic whites: an analysis of NHANES 2007-2010 in U.S. children and adults. J Health Care for the Poor and Underserved 26:726–736
Diaz VA, Mainous AG 3rd, Koopman RJ, Carek PJ, Geesey ME (2005) Race and diet in the overweight: association with cardiovascular risk in a nationally representative sample. Nutrition 21:718–725
McCabe-Sellers BJ, Bowman S, Stuff JE, Champagne CM, Bogle ML (2007) Assessment of the diet quality of US adults in the lower Mississippi Delta. Am J Clin Nutr 86:697–706
Kimmons J, Gillespie C, Seymour J, Serdula M, Blanck HM (2009) Fruit and vegetable intake among adolescents and adults in the United States: percentage meeting individualized recommendations. Medscape J Med 11:26
Newby PK, Noel SE, Grant R, Judd S, Shikany JM, Ard J (2011) Race and region are associated with nutrient intakes among black and white men in the United States. J Nutr 141:296–303
McNeill DA, Ali PS, Song YS (1985) Mineral analyses of vegetarian, health, and conventional foods: magnesium, zinc, copper, and manganese content. J Am Diet Assoc 85:569–572
Blaine J, Chonchol M, Levi M (2015) Renal control of calcium, phosphate, and magnesium homeostasis. Clin J Am Soc Nephrol 10:1257–1272
Elin RJ (1991) Laboratory tests for the assessment of magnesium status in humans. Magnes Trace Elem 92:172–181
Arnaud MJ (2008) Update on the assessment of magnesium status. Br J Nutr 99:S24–S36
Gullestad L, Midtvedt K, Dolva LO, Norseth J, Kjekshus J (1994) The magnesium loading test: reference values in healthy subjects. Scan J Clin Lab Invest 54:23–31
Klevay LM, Milne DB (2002) Low dietary magnesium increases supraventricular ectopy. Am J Clin Nutr 75:550–554
Wälti MK, Walcyyk T, Wimmermann MB, Fortunato G, Weber M, Spinas GA, Hurrell RF (2006) Urinary excretion of an intravenous 26Mg dose as an indicator of marginal magnesium deficiency in adults. Eur J Clin Nutr 60:147–154
Nielsen FH, Milne DB, Gallagher S, Johnson L, Hoverson B (2007) Moderate magnesium deprivation results in calcium retention and altered potassium and phosphorus excretion by postmenopausal women. Magnes Res 20:19–31
Nielsen FH, Milne DB (2003) Some magnesium status indicators and oxidative metabolism responses to low-dietary magnesium are affected by dietary copper in postmenopausal women. Nutrition 19:617–626
Hunt CD, Johnson LK (2006) Magnesium requirements: new estimations for men and women by cross-sectional statistical analyses of metabolic magnesium balance data. Am J Clin Nutr 84:843–852
Acknowledgments
This work was supported by the research grant of the Kongju National University in 2016.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the Institutional Review Board of Kyungbuk National University (IRB 2014–0053) and it was conducted upon reception of consent from study participants.
Rights and permissions
About this article

Cite this article
Choi, MK., Weaver, C.M. Daily Intake of Magnesium and its Relation to Urinary Excretion in Korean Healthy Adults Consuming Self-Selected Diets. Biol Trace Elem Res 176, 105–113 (2017). https://doi.org/10.1007/s12011-016-0822-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-016-0822-0