
Abstract
Previous studies have reported that silicon (Si) has a positive effect on bone health, immune response, and cognitive health. However, basic and important studies on evaluating dietary intake and urinary excretion of Si are limited. The aim of this study was to evaluate dietary Si intake and urinary excretion according to gender and age in healthy and free-living Korean adults and to investigate the relationship between them with gender. In this cross-sectional study, anthropometric measurements, dietary assessment using a food record, and a 24-h urine collection were conducted in 80 healthy Korean adults (40 males and 40 females; groups of 8 subjects representing each decade of life [20s to 60s]) with self-selected diet. The dietary assessment and 24-h urine collection were performed twice at intervals of 3 days. Daily intake of Si was estimated using a Si database of food composition. Urinary excretion of Si was analyzed using ICP-OES. The mean dietary Si intake was 22.8 mg/day for men and 19.3 mg/day for women without significant difference according to their gender and age. Si intake was the highest from vegetables both in men and women, followed by grains, beverages, and fruits in men and by grains, fruits, and milks in women. Urinary Si excretion was significantly higher in men (9.8 mg/day) than women (9.3 mg/day), and significantly increased with age only in women. Regarding the relationship between dietary Si intake and urinary Si excretion, a significantly positive correlation was found in men, but not in women. Longitudinal and balance studies to elucidate gender differences in Si nutrition are needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Silicon (Si), distributed in the form of alumino silicate (Al2O5Si) and silicon dioxide (SiO2, silica), is the next abundant element after oxygen on Earth [1]. Previous studies reported that Si, as a trace mineral, is essential for the development of bone and connective tissue [2, 3] and has a positive effect on immune response and cognitive health, in addition to bone health [4, 5].
Si content is abundant in vegetables and beverages such as drinking water and beer and higher in vegetables than meat and/or dairy products [6, 7]. The daily intake of Si was reported to be 20–50 mg for the Western diet [8,9,10] and 140–204 mg for China and India [11, 12], which showed differences in each country with different dietary patterns. Differences were also reported according to gender and age [8, 13].
Dietary Si is mainly absorbed in the gastrointestinal tract and most is excreted into urine [8]. Urinary Si excretion is an important factor to correlate with dietary intake and is a biomarker for estimating bioavailability [8, 14]. Several studies reported that the urinary excretion of Si during 0–6 h of ingestion was about 45% of dietary intake and 24-h Si excretion was about 57% [14,15,16]. However, studies on evaluating dietary Si intake and its relationship to urinary Si excretion are still limited.
In order to establish the dietary reference intakes (DRIs) of certain nutrients, sufficient scientific evidence to prove the requirement of and harmfulness to the body should be obtained; therefore, studies evaluating the nutrient intake and excretion level are needed [17]. The dietary patterns vary by country, and the food contents of trace minerals such as Si vary greatly depending on the type of soil and food variety. To obtain research data for establishing DRI of Si in a certain country, it is necessary to conduct research considering usual and actual dietary patterns of subjects and their age and gender [18].
The aim of this study was to evaluate the dietary Si intake and urinary Si excretion and investigate their relationship according to gender and age in Korean healthy adults with self-selected diet, which can be used as evidence data for accelerating Si research and establishing its RI for Koreans. In this study, a dietary intake survey and a 24-h urine collection were conducted in 80 Korean healthy adults, grouped based on their gender and age. And then, dietary intake and urinary excretion of Si were evaluated and the relationship between them was analyzed.
Materials and Methods
Subjects
The subjects of this study were 80 healthy males and females aged 20–69 years who were selected after volunteering in Chungnam, Korea. The volunteers were recruited by posting a study subject recruitment announcement on the websites of self-governing organizations of the region. The exclusion criteria disallowing volunteers from participating included having hypertension, heart failure, diabetes, kidney disease, or cancer, being under any medication and diet control, and for women, being pregnant and lactating. Regarding gender and age, the 80 subjects were selected as 8 males and 8 females for each age group in their 20s, 30s, 40s, 50s, and 60s.
Anthropometric Measurements
On the first day of the survey, trained staff members performed anthropometric measurements. Body weight and height of the subjects were measured twice to the nearest 0.1 kg and 0.1 cm, respectively, using a height–weight meter (DS-102, Dong Sahn Jenix Co., Seoul, Korea) while subjects were barefoot and wearing light indoor clothing. Body mass index (BMI) was calculated as weight in kilograms divided by squared height in meters.
Dietary Assessment
After anthropometric measurements, the dietary assessment was conducted for two days at intervals of 3 days on weekdays using the method of a food record. After completing the anthropometric measurement, subjects were instructed to maintain a usual diet and to record on a dietary sheet the type and amount of all food and beverages (e.g., coffee, tea, alcoholic beverages) consumed for 24 h on the day before urine collection, and if a camera was available, they were instructed to take a photo of food before consumption. A trained and registered dietician validated the dietary records through a direct interview with the subjects. In order to increase the accuracy of the dietary intake survey, the dietician used food containers, food models, measuring cups, weighing spoons, rulers, and measuring tape. Food and nutrient intakes were calculated using CAN-Pro 4.0 (Computer Aided Nutritional Analysis Program for Professionals, The Korean Nutrition Society, Seoul, Korea) based on the dietary intake survey sheet. Si intakes of the subjects were calculated using a Si content database produced by a previous study [19] and the food composition table of Japan [20]. The Si database covered 85.5% for the number of food consumed by the subjects and 96.8% for food intake.
Twenty-four-Hour Urine Collection and Analysis
Twenty-four-hour urine samples were collected twice during the study. Each collection started at 7:00 am on the day after the dietary intake assessments. The first voided urine was discarded, and thereafter, all urine was collected for 24 h. In order to determine the accuracy of the urine collection, [urine volume collected/(body weight × 21)] was calculated, and if it was more than 0.7, then it was judged to be accurate. And when it was lower than 0.7 and urinary creatinine concentration was lower than the reference value estimated based on the subject’s gender, age, and body weight, it was judged to be inaccurate [21]. In this case, urine and dietary intake data were collected again at intervals of at least 3 days. The collected urine was measured as total volume, and 10 mL of the urine was dispensed into a disposable transfer pipette and stored at − 70 °C until analysis. Urinary creatinine was analyzed by kinetic colorimetry assay. Si concentration in the urine sample was analyzed using inductively coupled plasma optical emission spectroscopy (ICP-OES; Optima 5300 DV, PerkinElmer, MA, USA) after urine was centrifuged at 400 g for 15 min based on a previous study [22]. The urine sample was prepared for analysis by diluting (1 + 1) with 1% (w/v) nitric acid and warming to room temperature prior to analysis for Si by ICP-OES. To measure the Si concentrations in urine samples, calibration standard solutions (Si concentrations of 0 to 10 mg/L) were prepared by diluting the stock standard solution (Kanto Chemical Co., Tokyo, Japan) with 1% nitric acid. The ICP-OES system was operated at 1150 W forward power with a plasma flow of 8 L/min, sample uptake rate of 49 rpm, auxiliary gas flow rate of 0.2 L/min, and nebulizer gas flow rate of 0.8 L/min with PFA nebulizer. The analytical wavelength used for Si was 251.611 nm. The relative standard deviation (%RSD) was maintained within 3% for each urine sample.
Statistical Analysis
Statistical analysis was performed using the SAS program (Ver. 9.3 SAS Institute, Cary, NC, USA). Data of dietary intake and urinary excretion for two days were used for statistical analysis after calculating the average for each subject. Data of all continuous variables were calculated as mean and standard deviation. To check normal distribution of all continuous variables, a Shapiro–Wilk test was conducted. Variable differences according to gender and age were tested using Student’s t test and ANOVA test with post hoc analysis of Tukey’s test. The correlation between each variable was evaluated for its significance using Pearson’s correlation test. Significance verification of all statistical analyses was set at the level of p < 0.05.
Results
Anthropometric Characteristics
No significant difference was found in the height, weight, and BMI of men according to age. In women, however, height significantly decreased (p < 0.001) while BMI increased (p < 0.05) with age (Table 1).
Daily Energy and Nutrient Intakes
Daily energy, carbohydrate, protein, and Si intakes were not significantly different according to age both in men and women. Dietary Si intake was 22.8 mg/day for men and 19.3 mg/day for women without significant difference in gender and age (Table 2).
Dietary Si Intake from Food Groups
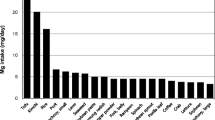
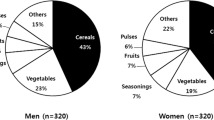
Figure 1 shows food and Si intakes from each food group in men and women. Food intake was the highest from beverages in men and vegetables in women. However, Si intake was the highest from vegetables both in men and women, followed by grains, beverages, and fruits in men and grains, fruits, and milks in women. Especially in beverages, men had a higher intake of Si from beer than women (data not shown).

Daily food and silicon intakes from food groups of the subjects
Dietary Intake and Urinary Excretion of Si
Figure 2 shows dietary Si intake and urinary excretion of the subjects according to age. Dietary Si intake was not significantly different between men and women. However, urinary Si excretion was significantly higher in men at 9.8 mg/day than women at 9.3 mg/day. In men, dietary Si intake and urinary excretion increased with age without significant difference. In women, there was no significant difference in dietary Si intake according to age, but urinary Si excretion significantly increased (p < 0.05).

Silicon intake and urinary excretion of the subjects according to gender and age. Eight subjects for each age group. Different letters over the graph indicate significant difference among age groups at p < 0.05 by Tukey’s multiple-range test after significant difference at p < 0.05 by ANOVA test
Relationship Between Dietary Si Intake and Urinary Excretion
Relationships between dietary Si intake and urinary Si excretion in men and women are shown in Fig. 3. Dietary Si intake was significantly correlated with urinary Si excretion in men (p < 0.01), but not in women.

Correlation between dietary intake and urinary excretion of silicon in the subjects
Discussion
In this study, we evaluated the dietary Si intake and urinary Si excretion and the relationship between them in free-living Korean adult men and women in order to provide evidence data required to accelerate Si research and to establish its DRI for Koreans. The main results showed no significant difference in dietary Si intake and urinary excretion according to age in men. In women, there was no significant difference in dietary Si intake with age, but urinary Si excretion was significantly increased. Dietary Si intake was significantly correlated with urinary Si excretion in men, but not women.
In the present study, the daily intake of Si was 22.8 mg for men and 19.3 mg for women, similar to 20–50 mg reported in the Western diet [7, 8, 23]. Adequate intake of Si is estimated to be 10–25 mg based on 24-h urinary excretion [24, 25]. Dietary Si intake in this study was within this range. Daily Si intake of men was reported as 20–30% [8] and 100% [6] higher than that of women. This study also showed that the intake of men was higher than that of women without significance, which is consistent with previous studies [6, 8]. However, Si intake per 1000 kcal was 10.8 mg/1000 kcal for men and 11.4 mg/1000 kcal for women. This is also consistent with the results of Kim [19], in which Si was 15.0 mg/1000 kcal for men and 16.3 mg/1000 kcal for women. These results show that women consume a more high-density Si diet than men.
Major food groups that contributed to the consumption of Si both in men and women were vegetables and grains. Choi and Kim [26] reported that Si intakes from grains and vegetables were 25.6% and 22.7% of total Si intake, respectively. In the present study, Si intakes through grains and vegetables were 22.3% and 26.6%, respectively, indicating that these were the main sources of Si. Grains have been reported as foods high in Si because of silicification of flower bracts and matured grain husk containing silica [27]. Vegetables also contain high Si by permeating Si into trichomes or microtriches of their surface from the soil [28]. In addition to vegetables and grains, beverages were also a major source of Si in this study. Si intake from beverages especially beer was significantly higher in men than women. Robberecht et al. [23] reported that beer and coffee were major sources of Si. It has been reported that the reason for higher Si intake of men than women is beer consumption [6, 8]. Beer is produced from barley and hops with high Si content. During the beer production, Si compound is used as a cleaning agent and cytolytic silica is decomposed into water soluble orthosilicic acid during the glycation, so that the Si content of beer is high and its absorption rate is also as high as 50% [7, 29, 30].
Ingested Si from food is absorbed mostly in the gastrointestinal track after digestion into orthosilicic acid, and most of the Si in serum is quickly filtered in the kidney glomeruli and excreted through the urine [15, 30, 31]. Based on studies evaluating urinary Si excretion, Jugdaohsingh et al. [8] reported that 41% of the ingested dose was excreted in the urine in 0–9 h. Pruksa et al. [16] reported that 57% of the ingested dose was excreted in the urine in 24 h, and the amount of Si absorption in healthy persons was the same as Si excretion in urine in 24 h. Although the absorption of Si in this study was not measured, and Si intake and urinary excretion were not measured on the same day, the ratio of urinary Si excretion to dietary Si intake was 47.2% for males and 53.6% for females (data not shown). These results are similar to those of previous studies that indicated that 40–75% of the ingested Si was excreted in the urine in 4–8 h [31] or that urinary excretion of Si in 24 h accounted for 57% of the intake [16]. However, this study has a limitation to emphasize the ratio of urinary Si excretion to dietary Si intake because Si intake and urinary excretion were analyzed through uncontrolled diet. However, this result may be interpreted as a ratio of usual urinary Si excretion to usual dietary Si intake. Further study to assess Si balance based on metabolic experiments with diet control is required.
In females of this study, although dietary intake of Si was not significantly different according to age, urinary excretion significantly increased with age. However, urinary Si excretion of males increased with increasing dietary intake according to age without significant difference. These results on gender difference in urinary Si excretion according to age can be interpreted from the following two perspectives. The first is difference in eating patterns between males and females, as mentioned in previous results. The contribution rate of beer to total Si intake was 10.0% for males and 1.5% for females. It is reported that beer is one of the major sources of Si and about 50% of Si ingested from beer is excreted in the urine [15, 29]. Jugdaohsingh [8] reported that about 49% of Si from grains and 21% from fruits and vegetables were excreted in the urine. Therefore, there is a possibility that urinary Si excretion may be different due to different eating patterns between men and women. The second perspective is the physiological difference between males and females, especially menopause in women. Numerous studies have shown that Si appears to have a beneficial effect on bone formation and bone health but not on bone resorption [2, 3, 32, 33]. Jugdaohsingh et al. [34] reported a difference in Si effects between postmenopausal women and either men or premenopausal women, interpreting the effect of Si would not be expected in postmenopausal women because their bone mineral density is driven by the resorption process. From these perspectives, we interpret that absorption and utilization of Si are high during the fertile period, but as they decrease after menopause, urinary excretion may increase with age. The current study also found that Si urinary excretion of women significantly increased from their 50s, which is a common menopausal age. Macdonald et al. reported that estrogen status is important for Si metabolism in bone health [3]. However, this study has some limitations to interpret the results because we did not analyze bone metabolism or physiological indices of the subjects and the variance in the Si intake data collected was large, so further studies including these biomarkers and a larger study population are needed.
To establish mineral RIs, scientific evidence obtained from balance studies on the intake, absorption, excretion, and equilibrium status is needed [35,36,37]. Urinary excretion of minerals can be an important index for estimating the intake and setting the requirement. In the results of correlation analysis between Si intake and urinary Si excretion, a significantly positive correlation was found in men, but not in women. Other studies reported that dietary Si intake was significantly correlated with urinary Si excretion without difference between men and women [8, 13]. Factors affecting Si absorption include dietary fiber, calcium, magnesium, and steroid hormones [38, 39]. As discussed earlier, there is a possibility that the dietary patterns or physiological characteristics of women that are different from those of men may interfere in the relationship between dietary Si intake and urinary Si excretion. Future study is required to investigate the relationship between Si intake and urinary Si excretion and its gender difference considering interference factors.
This study has several limitations to generalize the results. In estimating Si intake, drinking water was not included and the Si database on food composition was not sufficient, suggesting a possibility of underestimating Si intake. Also, the number of study participants was small and the study area was limited to some parts of Korea. Although urinary Si excretion was assessed the day after Si intake examination, the diet on this day was not controlled, which could have weakened the relationship between dietary intake and urinary excretion of Si. However, this is the first study to evaluate dietary Si intake and urinary Si excretion and to investigate the relationship between them according to gender and age in Korean adults with self-selected diet. This research data can be used for establishing the DRI for Si and evaluating the nutritional status of Si.
Conclusion
Dietary Si intakes of Korean adults with self-selected diet were 22.8 mg/day for men and 19.3 mg/day for women without significant difference with respect to their age. Urinary Si excretion was significantly higher in men at 9.8 mg/day than women at 9.3 mg/day and significantly increased with age only in women. In the relation between dietary Si intake and urinary Si excretion, a significantly positive correlation between them was found in men, but not in women.
References
Sjöberg S (1996) Silica in aqueous environments. J Non-Cryst Solids 196:51–57
Calomme M, Geusens P, Demeester N, Behets G, D’Haese P, Sindambiwe J, Van Hoof V, Berghe DV (2006) Partial prevention of long-term femoral bone loss in aged ovariectomized rats supplemented with choline-stabilized orthosilicic acid. Calcif Tissue Int 78:227–232
Macdonald HM, Hardcastle AC, Jugdaohsingh R, Fraser WD, Reid DM, Powell JJ (2012) Dietary silicon interacts with oestrogen to influence bone health: evidence from the Aberdeen prospective osteoporosis screening study. Bone 50:681–687
Gillette Guyonnet S, Andrieu S, Vellas B (2007) The potential influence of silica present in drinking water on Alzheimer’s disease and associated disorders. J Nutr Health Aging 11:119–124
Nielsen FH (2008) A novel silicon complex is as effective as sodium metasilicate in enhancing the collagen-induced inflammatory response of silicon-deprived rats. J Trace Elem Med Biol 22(1):39–49
Pennington J (1991) Silicon in foods and diets. Food Addit Contam 8:97–118
Powell J, McNaughton S, Jugdaohsingh R, Anderson S, Dear J, Khot F, Mowatt L, Gleason K, Sykes M, Thompson R (2005) A provisional database for the silicon content of foods in the United Kingdom. Br J Nutr 94:804–812
Jugdaohsingh R, Anderson S, Tucker K, Elliott H, Kiel D, Thompson R, Powell J (2002) Dietary silicon intake and absorption. Am J Clin Nutr 75:887–893
Becker W, Branca F, Brasseur D, Bresson JL, Flynn A, Jackson A (2004) Opinion of the scientific panel on dietetic products, nutrition and allergies on a request from the commission related to the tolerable upper intake level of silicon. EFSA J 60:1–11
McNaughton S, Bolton-Smith C, Mishra G, Jugdaohsingh R, Powell J (2005) Dietary silicon intake in post-menopausal women. Br J Nutr 94:813–817
Anasuya A, Bapurao S, Paranjape P (1996) Fluoride and silicon intake in normal and endemic fluorotic areas. J Trace Elem Med Biol 10:149–155
Chen F, Cole P, Wen L, Mi Z, Trapido E (1994) Estimates of trace element intakes in Chinese farmers. J Nutr 124:196–201
Trumbo P, Yates A, Schlicker S, Poos M (2001) Dietary reference intakes: vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. J Am Diet Assoc 101:294–301
Jugdaohsingh R, Sripanyakorn S, Powell JJ (2013) Silicon absorption and excretion is independent of age and sex in adults. Br J Nutr 110:1024–1030
Sripanyakorn S, Jugdaohsingh R, Elliott H, Walker C, Mehta P, Shoukru S, Thompson RP, Powell JJ (2004) The silicon content of beer and its bioavailability in healthy volunteers. Br J Nutr 91:403–409
Pruksa S, Siripinyanond A, Powell JJ, Jugdaohsingh R (2014) Silicon balance in human volunteers; a pilot study to establish the variance in silicon excretion versus intake. Nutr Metab 11:4
Ministry of Health and Welfare (2015) Dietary reference intakes for Koreans 2015. Ministry of Health & Welfare, Seoul
Ma JF, Yamaji N (2006) Silicon uptake and accumulation in higher plants. Trends Plant Sci 11:392–397
Kim HJ (2016) Development of database on silicon content in common foods and assessment of its daily intake in Korean. Kongju National University, Master thesis
Suzuki Y, Tanushi S (1993) Table of trace element contents in Japanese foodstuffs. Daiichi-shuppan, Tokyo
Blackburn GL, Thornton PA (1979) Nutritional assessment of the hospitalized patient. Med Clin North Am 63:1103–1115
Burden TJ, Whithead MW, Thomson RPH, Powell JJ (1998) Preparation of urine samples for trace metal determination: a study with aluminum analysis by inductively coupled plasma optical emission spectrometry. Ann Clin Biochem 35:245–253
Robberecht H, Van Cauwenbergh R, Van Vlaslaer V, Hermans N (2009) Dietary silicon intake in Belgium: sources, availability from foods, and human serum levels. Sci Total Environ 407:4777–4782
Calomme M, Cos P, D’Haese P, Vingerhoets R, Lamberts L, De Broe M, Van Hoorebeke C, Van den Berghe D (1998) Absorption of silicon in healthy subjects. Met Ions Biol Med 5:228–232
Carlisle EM (1982) The nutritional essentiality of silicon. Nutr Rev 40:193–198
Choi M, Kim M (2016) Dietary silicon intake of Korean young adult males and its relation to their bone status. Biol Trace Elem Res 176:89–104
Hayward D, Parry D (1980) Scanning electron microscopy of silica deposits in the culms, floral bracts and awns of barley. Ann Bot 46:541–548
Parry D, Hodson M, Sangster A, Jones W, O’Neill C (1984) Some recent advances in studies of silicon in higher plants. Phil Trans R Soc Lond 304:537–549
Bellia J, Birchall J, Roberts N (1994) Beer: a dietary source of silicon. Lancet 343:235
Reffitt DM, Jugdaohsingh R, Thompson RP, Powell JJ (1999) Silicic acid: its gastrointestinal uptake and urinary excretion in man and effects on aluminium excretion. J Inorg Biochem 76:141–147
Van Dyck K, Van Cauwenbergh R, Robberecht H, Deelstra H (1999) Bioavailability of silicon from food and food supplements. Fresenius J Anal Chem 363:541–544
Nielsen FH, Poellot R (2004) Dietary silicon affects bone turnover differently in ovariectomised and sham-operated growing rats. J Trace Elem Exp Med 17:137–149
Macdonald HM, Hardcastle AE, Jugdaohsingh R, Reid DM, Powell JJ (2005) Dietary silicon intake is associated with bone mineral density in premenopasual women and postmenopausal women taking HRT. J Bone Miner Res 20:S393
Jugdaohsingh R, Tucker KL, Qiao N, Cupples LA, Kiel DP, Powell JJ (2004) Dietary silicon intake is positively associated with bone mineral density in men and premenopausal women of the Framingham Offspring cohort. J Bone Miner Res 19:297–307
Offenbacher EG, Spencer H, Dowling HJ, Pi-Sunyer FX (1986) Metabolic chromium balances in men. Am J Clin Nutr 44:77–82
Schwartz R, Apgar BJ, Wien EM (1986) Apparent absorption and retention of Ca, Cu, Mg, Mn, and Zn from a diet containing bran. Am J Clin Nutr 43:444–455
Nishimuta M, Kodama N, Shimada M, Yoshitake Y, Matsuzaki N, Morikuni E (2012) Estimated equilibrated dietary intakes for nine minerals (Na, K, Ca, mg, P, Fe, Zn, Cu, and Mn) adjusted by mineral balance medians in young Japanese females. J Nutr Sci Vitaminol 58:118–128
Kelsay JL, Behall KM, Prather ES (1979) Effect of fiber from fruits and vegetables on metabolic responses of human subjects, II. Calcium, magnesium, iron, and silicon balances. Am J Clin Nutr 32:1876–1880
Nielsen FH (1991) Nutritional requirements for boron, silicon, vanadium, nickel, and arsenic: current knowledge and speculation. FASEB J 5:2661–2667
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the Institutional Review Board of Kyungpook National University (IRB 2014-0053) and was conducted according to the Helsinki declaration; all subjects were explained in detail the purpose and contents of the study, and each signed an informed consent form.
Conflict of Interest
The authors declare that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kim, YY., Kim, MH. & Choi, MK. Relationship Between Dietary Intake and Urinary Excretion of Silicon in Free-Living Korean Adult Men and Women. Biol Trace Elem Res 191, 286–293 (2019). https://doi.org/10.1007/s12011-018-1619-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-018-1619-0