
Abstract
Purpose of the Review
Polymyalgia rheumatica (PMR) is one of the most common inflammatory rheumatologic condition occurring in older adults. It is characterized by proximal pain and stiffness in the shoulders, neck, and/or pelvic girdle in individuals over 50 years of age along with evidence of an intense systemic inflammatory response. Although the above clinical symptoms are very characteristic for the condition, it can be mimicked by other autoimmune, infectious, malignant, and endocrine disorders chief among which are giant cell arteritis (GCA) and elderly-onset rheumatoid arthritis (EORA). Recently, PMR was reported in relation to treatment with immune checkpoint inhibitors.
Current treatment of PMR consists of low-to-medium doses of glucocorticosteroids (GC) with variable response rates and disease recurrence estimated to occur in 50% of patients while tapering down GC doses. In addition, GC-based regimens cause much of the morbidity associated with PMR in older adults, requiring close monitoring for GC-induced toxicity during therapy and highlighting the need for novel therapeutic strategies. Here, we review the latest findings in the field regarding specific etiologic factors, genetic associations, diagnostic methods, and advancements in treatment strategies and disease monitoring indices.
Recent Findings
Recent discoveries involving novel therapeutic targets in GCA have accelerated the study of PMR pathophysiology and have advanced treatment strategies in PMR management leading to current trials in IL-6 blocking agents.
Summary
PMR remains an enigmatic inflammatory condition affecting older adults, with current treatment approach causing much morbidity in this patient population. Advancements in our understanding of novel immunopathologic targets can serve as a solid foundation for future treatment strategies in the field.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Epidemiology and Immunopathogenesis
Polymyalgia rheumatica, a condition first reported in 1888 and later named by Barber in 1957 [1], is one of the most common inflammatory disorder affecting senior adults. It most commonly occurs in women of Northern European ancestry but can occur in any ethnic group. Peak incidence occurs at age 70–75 years with 66–75% of patients being female with lifetime risk of 2.4% for women and 1.7% for men [2,3,4]. PMR almost never occurs in patients younger than 50 years. While the etiology of PMR remains unclear, its occurrence seems to stem from an interplay between genetic and environmental factors with a role for immunosenescence.
Unlike the overlapping condition giant cell arteritis (GCA), where HLA-DRB1*04 genotype is a known risk factor for disease development, no clear HLA association has been shown in PMR [5]. However, even in PMR, genetic polymorphisms may play a role, especially polymorphisms of interleukin (IL)-6, intercellular adhesion molecule 1, and IL-1 receptor antagonist, as recent reports show relevance of these mediators in PMR immunopathogenesis (see below).
Additional immunopathogenic factors involve the aging immune system, with a decrease in production of new immune cells, including a decrease in T cell production due to thymic involution. This, in turn, causes a reduction in the output of thymic regulatory T cells, leading to increased Th1 and Th17 responses, immune dysregulation, and autoimmunity [6]. A consequence of immune dysregulation is an increase in pro-inflammatory cytokine production such as IL-6 and IL-1 beta in older adults [7, 8]. Interestingly, gout, a well-known inflammatory arthritis associated with IL-1 activation, was recently found to be associated with a greater than 2-fold higher risk of incident PMR in older adults [9]. Given its stimulation of Th17 responses, IL-17 has also recently been implicated in both PMR and GCA [10]. In addition, elevated IL-6 levels have been shown to correlate with PMR disease activity [5] and IL-6 blocking agents are currently being trialed in PMR after having shown efficacy in GCA [11].
Aside from genetic factors, environmental factors are also purported to play a role in PMR development. The risk of GCA is known to increase during the winter months in the setting of mycoplasma, chlamydia pneumonia, and parvovirus B19 epidemics [12], and herpes zoster occurrence was recently found to be associated with an increased risk of GCA in two large GCA patient cohorts [13]. However, no infectious organism has been clearly associated with PMR occurrence to date [12].
Clinical and Laboratory Manifestations
Clinical signs and symptoms of PMR typically include abrupt onset (ranging between 2 weeks to 2 months, though a more subtle, progressive course can also occur) of pain and stiffness typically affecting the neck and one or both proximal girdles—the shoulder girdle, and less commonly, the pelvic girdle. Although symptoms may be unilateral on initial presentation, clinical manifestations are later bilateral [14]. Stiffness is particularly debilitating and is typically present for more than 30 min in the morning, making it difficult for patients to lift their arms to complete their activities of daily living (ADLs). Similarly, it may be difficult for patients affected by pelvic girdle stiffness to get out of bed or rise from a chair without assistance. Resting stiffness, (also known as “jellying” phenomenon) may also occur. In some patients, the pain in the shoulder and pelvic regions may radiate to the elbows, hips and even to the knees. Characteristic clinical signs of systemic inflammation, such as low-grade fever, anorexia and weight loss, and/or malaise and fatigue occur in approximately 40–50% of patients and are particularly common in patients over 70 years of age [4].
On clinical examination, the clinician may observe reduced active and passive ranges of motion on shoulder elevation or hip flexion. It is noteworthy that while patients may experience a sensation of proximal muscle weakness, actual muscle weakness or findings supporting myopathy are lacking. Distal musculoskeletal manifestations may occur in 25–50% of patients, most frequently as transient, nonerosive asymmetrical arthritis primarily affecting the knee or wrist in about 40% of patients [14,15,16]. Tenosynovitis is also common and may lead to carpal tunnel syndrome [4, 16]. Pitting edema can affect the hands, wrists, ankles, and feet, and occasionally is the presenting finding.
Among laboratory signs of inflammation, elevated erythrocyte sedimentation rate (ESR) typically over 40 mm/h, and elevated C-reactive protein (CRP) level are highly characteristic of PMR and are detected in more than 90% of patients, but both ESR and CRP may be normal in a small percentage of patients [4, 17, 18]. Additional common laboratory markers of inflammation, including anemia of chronic disease, thrombocytosis, or elevated ferritin level can also be seen. Mild elevation of liver enzymes, especially alkaline phosphatase, occurring in one-third to one-half of patients, may also occur [18]. Elevated anticardiolipin antibody titers have also been described in PMR patients and appear to be associated with increased risk of developing vascular complications including GCA [18, 19].
Diagnosis
The diagnosis of PMR does not pose a significant challenge for an experienced clinician when typical signs and symptoms and elevated inflammatory markers are present. However, PMR may be over- or underdiagnosed by less experienced clinicians in cases of mimicking conditions or multiple comorbidities especially given lack of a gold standard for diagnosis and the non-specificity of signs and symptoms as well as laboratory studies associated with this condition [20, 21]. Especially notable in this regard is elderly-onset rheumatoid arthritis (EORA, discussed at length below) as well as rotator cuff pathology or osteoarthritis (OA) of the cervical or lumbar spine, which should normally be excluded when diagnosing PMR but which commonly co-exist with PMR in elderly patients [20].
The 2015 European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) management guidelines recommend to conduct a basic workup to exclude alternative diagnoses of PMR and to establish a baseline for monitoring of therapy. This basic workup should include complete blood count, inflammatory markers, thyroid function tests, bone profile (vitamin D, calcium, alkaline phosphatase levels), kidney and liver function tests, creatine kinase level, rheumatoid factor (RF) and/or anti-citrullinated protein antibodies (ACPA), urinalysis, and protein electrophoresis. Depending on clinical signs and symptoms and likelihood of alternative diagnoses, additional testing such as anti-nuclear antibodies (ANA), anti-cytoplasmic neutrophil antibodies (ANCA) or tuberculosis testing may be warranted [22]. Ultrasonography can be particularly useful in patients with typical proximal symptoms but normal inflammatory markers.
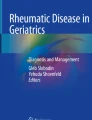
In 2012, EULAR and ACR jointly developed the Provisional Classification Criteria for Polymyalgia Rheumatica for research purposes consisting of a weighted scoring system for classifying PMR (Table 1) [23]. Ultrasonographic findings of shoulder or hip inflammation can be used to enhance specificity of these criteria (Fig. 1). Among shoulder ultrasonographic findings are subdeltoid bursitis, biceps tenosynovitis, and/or glenohumeral synovitis and hip findins include joint synovitis and/or trochanteric bursitis. Of note, ultrasonographic pathologic findings chracteristic of PMR must be present in at least one shoulder for such findings to be used in classification of PMR, while isolated hip joint-related findings do not suffice on their own for such classification. Unfortunately, these most up-to-date EULAR/ACR criteria only have 66–68% sensitivity and 65–88% specificity (though better with ultrasound data) and cannot readily distinguish between PMR and other conditions that might occur in seniors [21, 24, 25].

a Biceps tenosynovitis (represented by a double asterisk) and b subacromial subdeltoid bursitis (represented by an arrow) as representative inflammatory findings on shoulder ultrasonography of PMR patients
Differential Diagnosis of PMR
Several categories of illnesses can present in a similar manner to PMR (Table 2). In addition, because of the overlap between PMR and GCA, this form of large vessel vasculitis must be considered in every patient presenting with PMR.
Several studies to date examine the reasons for initial misdiagnosis of PMR. In a retrospective case series by González-Gay et al., the most common clue to a misdiagnosis of PMR was lack of rapid response to GC treatment and in most of these cases, alternative diagnoses were not initially considered [26]. In a retrospective study by Ceccato et al. consisting of 200 Argentinian patients from three different hospitals diagnosed with PMR from 2004 to 2009, over the next 4.5 ± 3 months on average, 16/200 (8%) of patients were eventually found to have alternative diagnoses [27]. The most common missed diagnoses were malignancies and rheumatologic conditions other than PMR. Other entities which were initially missed were infective endocarditis, narrow cervical canal, Parkinson’s disease, statin-related myalgia, hypothyroidism, vitamin D deficiency, and CPPD. It is of interest that about 63% of patients initially thought to have PMR had no response to GC treatment, and 12.5% of patients had persistently elevated ESR as clues to an alternative diagnosis [27]. Overall, these data are reassuring in that the vast majority of patients who have signs and symptoms of PMR are correctly classified and lack of response of symptoms to GC and/or persistent elevation of inflammatory markers should serve as indicators to search for alternative diagnoses.
Comorbidities in PMR
As previously noted, current clinical guidelines suggest that in order to diagnose PMR, a large number of medical conditions which may mimic the symptoms of PMR should be excluded, such as inflammatory arthritis and endocrine, infective, and neoplastic conditions [22]. However, comorbidities are very common in various rheumatologic conditions as well as in the older age group affected by PMR so that several recent studies have examined the co-occurrence of various medical conditions with PMR. A recent systematic review on such comorbid conditions by Partington et al. which included 41 pertinent studies highlighted the wide variations in study design and the studied populations in these publications, but found a positive associations between PMR diagnosis and cardiovascular disease (CVD) including incidence of stroke, myocardial infarction, heart failure, and peripheral vascular disease in PMR patients relative to population controls [28••]. Of these studies, the study by Hancock et al. found that the magnitude of excess risk of vascular events in PMR patients (adjusted HR 2.6, 95% CI 2.4–2.9 irrespective of vascular disease end point examined), was higher in early disease and in patients younger than 60 years at diagnosis [29]. Another systematic review and meta-analysis on CVD risk in PMR patients conducted by Ungprasert et al. and which examined some of the same studies which were evaluated by Partington et al. also found a significantly increased excess CVD risk among patients with PMR relative to controls with a pooled risk ratio of 1.72 (95% CI 1.21–2.45) [30]. Notably, a study by Kremers et al. included in both meta-analyses found that PMR patients receiving GC therapy did not have an increase in risk of vascular events relative to untreated PMR patients [31].
The evidence of association of other comorbidities with PMR, including thyroid disease [28, 32, 33] and Parkinson’s disease [28, 34], remains controversial, especially given the risk of clustering of diagnoses in this older population. Similar controversy also exists regarding any association between PMR and malignancy risk [28••, 35]. Several studies regarding possible association between PMR and overall malignancy rate as well as the possible association of PMR with specific types of cancer such as leukemia, lymphoma, myeloproliferative disease and various solid tumors have been published to date. One retrospective, general practice database-centered population-matched cohort study by Muller et al. from the United Kingdom found a HR of 1.69 (1.18–2.42, 95% CI) of cancer diagnosis in the first 6-months following PMR diagnosis with higher prevalence of cancers involving the hematopoietic, lymphatic, female reproductive, genitourinary, and central nervous systems [36]. Similarly, a Swedish study on hospitalized PMR and GCA patients with matched population controls found a marginally increased standardized incidence ratio (1.19 for cancers diagnosed < 1 year and 1.06 for cancers diagnosed > 1 year of follow-up) of similar cancer types noted by Muller et al. though also including squamous cell carcinoma and melanoma [37]. Contrary to these studies, a 30-year-long population-based cohort study of PMR patients with a comparator group of non-PMR subjects from Olmsted County, Minnesota, conducted by Pfeifer et al. found no significant difference in the prevalence of malignancy prior to PMR incidence date/index date or in the cumulative incidence of malignancy at 10 years of follow-up between PMR patients and population controls [38]. Similarly, a study by Myklebust et al. conducted in Norway on PMR and GCA patients with population-matched controls found no differences in frequencies or types of malignant neoplasms between these two groups [39]. Notably, regardless of findings involving malignancy in “typical” PMR cases, the literature does suggest that the presence of atypical features of PMR may hint at presence of occult malignancy [35]. For instance, a case series reported by Naschitz et al. showed that atypical features of PMR such as age younger than 40 years, limited or asymmetric involvement of typical sites, ESR < 40 mm/h or > 100 mm/h, and poor or delayed response to steroid treatment may be suggestive of the presence of occult malignancy [40]. Similar findings were also reported in a study by González-Gay et al. [41], with kidney, lung, and colorectal cancer and multiple myeloma most often found in patients presenting with atypical PMR features in both of these studies.
Taken together, current data on comorbidities in PMR suggests that while certain conditions should be excluded prior to considering the diagnosis of PMR, the coexistence of comorbid conditions with PMR should note necessarily exclude or invalidate this diagnosis.
Co-occurring Conditions in PMR
Giant Cell Arteritis
Giant cell arteritis (GCA), a form of large and medium vessel vasculitis, shares both epidemiological and immunological similarities with PMR. The clinical connections between PMR and GCA suggest that they may be different manifestations of the same disease process: both conditions have similar age and sex distributions and both present with increased levels of serum acute-phase reactants with swift response to GC [15]. Population-based studies show that PMR is two to three times more common than GCA (PMR incidence 52.5/100,000 aged 50+ in Olmsted County, Minnesota, where GCA incidence is 20/100,000) [12]. Importantly, 16–21% of PMR patients present with clinical features of GCA; conversely, about 40% of patients with GCA have symptoms of PMR before, concomitantly, or following diagnosis of GCA [15]. Interestingly, both pathology and imaging studies reveal that subclinical vasculitis without clinical features of GCA may be detected in a subset of patients with PMR. A positive temporal artery biopsy was demonstrated in up to 9% of patients with PMR [42], and evidence of vasculitis was found in up to 31% of PMR patients undergoing 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) at diagnosis [43]. Signs of vasculitis were also found on ultrasound examination of the temporal arteries in 8% of patients with PMR [44]. Based on these findings, it has been suggested that PMR may represent GCA with incompletely developed vascular involvement [45]. Because patients with pure manifestations of PMR do not develop the characteristic clinical complications of GCA, no universal screening recommendations for subclinical vasculitis currently exist [42], but patients with PMR should be educated about signs and symptoms of GCA and asked about symptoms of GCA during follow-up.
Several studies to date report on clinical features which distinguish between PMR and GCA [4] or increase the likelihood of a clinical diagnosis of GCA [46]. While older age, female sex, short (< 6 weeks) duration of symptoms, and increase in acute-phase reactants are present in both conditions [46], some clinical features do suggest the diagnosis of GCA over isolated PMR (Table 3). Notably, patients with isolated PMR have in general lower values of ESR and less frequently have anemia and thrombocytosis than patients with PMR with concomitant GCA [47]. In addition, clinical signs and symptoms of vasculitis involving vision changes, temporal artery abnormalities, jaw or limb claudication, or differential pulses or blood pressures in the extremities point to vasculitis [4, 46].
Remitting Seronegative Symmetrical Synovitis with Pitting Edema and Elderly-Onset Rheumatoid Arthritis
PMR, EORA, and remitting seronegative symmetrical synovitis with pitting edema (RS3PE) are clinically overlapping inflammatory conditions affecting individuals over 60 years of age. Importantly, both PMR and EORA can initially present as RS3PE and both PMR and RS3PE can be initial presentations of EORA [4]. By definition, RS3PE is a symmetrical polyarthritis in which pitting edema of the hands and/or feet is a prominent feature [48]. The hand swelling results from diffuse extensor more than flexor tendon tenosynovitis of the hands with inflammation of surrounding soft tissues [49] (Fig. 2). As in PMR, IL-6 has been implicated in the pathogenesis of RS3PE. Also as in PMR, RS3PE is accompanied by elevated acute-phase reactants and negative RA serologic tests [48], though a recent study suggests that CRP levels are typically higher in PMR [50]. RS3PE has been reported as an isolated syndrome, as a paraneoplastic syndrome in solid and hematologic malignancies, or in association with infectious agents or rheumatologic conditions [35, 49]. In the case of EORA first presenting as PMR or RS3PE, it usually has sudden onset and is typically accompanied by elevated acute-phase reactants and negative RF and ACPA [48]. Any one of these three conditions can be treated by GC doses varying between 10 and 20 mg/day with gradual taper. However, when difficulty arises in tapering down GC, the clinician should consider the onset of EORA as less than two-thirds of EORA patients report significant clinical benefit following 1 month of GC treatment vs 97.6% of PMR patients [50]. Importantly, when occurring as a paraneoplastic syndrome, RS3PE responds poorly to treatment other than treatment of the underlying malignancy.

Examples of diffuse tenosynovitis of the hands with inflammation of surrounding soft tissues characteristic of Remitting Seronegative Symmetrical Synovitis with Pitting Edema (RS3PE)
Association of Immune Checkpoint Inhibitor Therapy and PMR Onset
Immune checkpoint inhibitors (ICIs) targeting cytotoxic T lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1) are currently being successfully used to increase survival in many cancers. However, this treatment is associated with immune-related adverse events (IrAE). Recently, several case series reported PMR occurring following ICI treatment [51, 52, 53•]. These reported cases suggest that ICI-related PMR generally meets the 2012 EULAR/ACR Provisional Classification Criteria for PMR and responds to GC therapy, rarely requiring additional immunosuppressive therapy [51, 52, 54]. However, a recent case series of ICI-related PMR showed that some cases do present atypically, with 37% of patients requiring higher doses of prednisone than traditionally recommended for PMR treatment (20 mg/d up to 60 mg/day) [53•].
Several mechanisms have been proposed for ICI-related PMR. In some cases of ICI-related PMR, the IL-6 inhibitor tocilizumab (TCZ) was successfully used to treat PMR as a GC-sparing agent, suggesting a possible pathogenic role of IL-6 and Th17 cell activation in IrAEs [53•]. Another proposed mechanism for the occurrence of PMR/GCA following ICI therapy lies in the recent discovery that dendritic cells from GCA-affected blood vessel walls show low expression of the inhibitory ligand of PD-1 (PD-L1) suggesting a breakdown of the tissue-protective PD1/PD-L1 immunoinhibitory checkpoint which thus unleashes arterial wall inflammation and remodeling [55].
Management of PMR in the Elderly
In contrast to GCA, where GC therapy is started immediately because of possible risk of vision loss, patients with apparently isolated PMR should have a basic diagnostic workup prior to starting therapy.
Goals of therapy in patients with PMR in the short term are to control chronic PMR symptoms and prevent disease relapse, to optimize and preserve activity level, and to optimize musculoskeletal function and improve quality of life with minimal adverse effects from medications. Long-term treatment goals include reduction in decline of mobility over time and reduction of possible cardiovascular complications associated with PMR itself and involving long-term GC use [14, 20].
Non-pharmacologic Interventions
While evidence for physical therapy in PMR in lacking, individualized exercise programs consisting of range-of-motion exercises for the shoulder and hips are recommended for maintaining good physical function and mobility in PMR patients [22]. Patient education on PMR and side effects of GC therapy is essential to good quality of patient care. Influenza and pneumococcal vaccinations are recommended for all patients receiving immunosuppressive medications, including PMR patients [56]. In addition, live viral vaccinations should be avoided with the exception of measles-mumps-rubella, varicella, and herpes zoster, which might be administered to patients with mild immunosuppression (such as prednisone equivalent dose < 20 mg/day, MTX < 0.4 mg/kg per week, or azathioprine < 3.0 mg/kg per day) but should be avoided in patients receiving biologic disease-modifying antirheumatic drugs (bDMARDs) [56, 57].
Pharmacologic Interventions
Glucocorticosteroids
Glucocorticosteroids (GC) therapy with slow taper is considered the mainstay of PMR treatment, with mean length of treatment of 1.8 years [16]. Response to GC is usually rapid, occurring within days of initiation of therapy. The British Society for Rheumatology Guidelines define a rapid response to GC as a patient-reported global improvement of ≥ 70% within a week of starting GC treatment with normalization of inflammatory markers within 4 weeks [58]. However, response may also be more gradual with studies showing that about one-third of patients have incomplete response at 4 weeks [59]. Because steroid responsiveness is not unique to PMR, an empirical GC “test of treatment” is not recommended to aid in PMR diagnosis.
The 2015 EULAR/ACR recommendations for PMR management emphasize that there is no ideal GC regimen suitable for all patients, so that GC dosing and tapering schedule should be based on individual patient characteristics, including disease severity, comorbidities, other prescribed medications, risk of GC-related adverse events, and patient preference. Clinicians should generally aim at the minimum effective starting single-daily dose of GC within a range of 12.5–25-mg prednisone equivalent, as studies show no clinical benefit of higher starting doses with greater risk of adverse events and prolongation of therapy [22, 60]. While the 2015 EULAR/ACR recommendations for PMR management emphasize using a single rather than divided daily doses of GC [22], it is the authors’ experience that splitting the dose in partially responsive patients can be very useful. Providing one-fourth to one-third of the total dose in the evening can in some patients provide significant AM relief not provided by a single AM dosing. Not all patients have the expected 24-h response from a single AM dose of GC.
Prednisone dose should be tapered to an oral dose of 10 mg/day prednisone equivalent within 4–8 weeks with progressive taper when response seems favorable. Relapse is common, occurring in about 50% of patients [4, 5], with female sex, ESR > 40 mm/h and peripheral arthritis indicating a higher risk for relapse [4, 22]. When relapse occurs, oral prednisone dose should be increased to the pre-relapse dose (not necessarily to the initial response dose) with gradual decrease within 4–8 weeks to the dose at which the relapse occurred. Once remission is achieved, prednisone should be tapered by 1 mg every 4 weeks (alternate day schedules can be used) until discontinuation when the patient is asymptomatic from their polymyalgic symptoms [22]. A more rapid tapering regimen is often associated with a high relapse rate and should thus be avoided [20, 60].
The use of intramuscular (IM) methylprednisolone acetate was only evaluated in one randomized controlled trial (RCT), in which methylprednisolone acetate 120 mg IM every 3 weeks was administered for 12 weeks followed by monthly injections with dose reductions of 20 mg every 3 months, and was found to be associated with similar remission rates to patients receiving an oral prednisone taper starting at 15 mg/ day with lower cumulative GC dose, fewer fractures, and lower weight gain [4, 61]. However, due to limited availability of IM methylprednisolone and limited studies with this agent, its use is not universally recommended for PMR [4, 61].
Novel studies on optimizing the benefit/risk ratio of GC use currently focus on development of innovative GC preparations such as selective GC receptor agonists and modulators (SEGRMs) which are aimed at enhancing anti-inflammatory cellular pathways selectively while minimizing GC-induced adverse events. Some of these novel compounds may modulate the activity of a GC receptor agonist and may also not classically bind the GC receptor ligand-binding pocket in order to exert their effects [62]. Ongoing studies also examine the use of selective delivery of GC to inflamed tissues using nanometer-sized liposomes, and recent studies have already been carried out with these drug delivery systems in RA [63] so that their use in PMR might be trialed in the future. Last, the bedtime administration of modified-release (MR) prednisone aimed at optimal chronotherapy around 2:00 AM. has already been trialed successfully in a small feasibility study in new-onset GCA with comparable efficacy and safety to immediate-release (IR) prednisone [64] and might be trialed in PMR in the future.
Conventional Disease-Modifying Antirheumatic Drugs
Because of need for long-term treatment of PMR with GC, GC-sparing agents have been trialed in PMR management. Of cDMARDs, methotrexate (MTX) is the only immunosuppressive agent that has been evaluated in RCTs [4, 65, 66], with most studies showing benefit with regard to relapse rate, cumulative GC dose used (for instance, in the highest-quality RCT by Caporali et al., a median dose of 2.1 g was used in the MTX plus prednisone group vs 3.0 g in prednisone plus placebo group, p = 0.003) and ability to discontinue GC after 76 weeks of treatment (88% for MTX plus prednisone vs 53% for prednisone alone, p = 0.003) [4, 65, 66]. Accordingly, EULAR/ACR recommendations call for early use of MTX in individual patients at high risk of relapse (female patients, ESR > 40 mm/h, peripheral arthritis), in relapsing disease, or in patients with GC-related adverse events or comorbidities that might be exacerbated by GC use [22]. There are also reports of using azathioprine (AZA) [67] and leflunomide (LEF) [68, 69] in PMR patients. A RCT is currently being conducted on use of LEF in PMR (www.clinicaltrials.gov).
Biologic Disease-Modifying Antirheumatic Drugs
Unlike GCA, the use of novel bDMARDs in PMR has been challenging due to the lack of proper animal model for PMR. In recent years, several bDMARDs have been successfully trialed in GCA and given the overlap between GCA and PMR, these agents are currently being examined in PMR.
The first bDMARDs trialed in PMR, the tumor necrosis factor alpha blockers (anti-TNF alpha agents) infliximab and etanercept, were not found to be effective so that their use in PMR should be discouraged [70, 71]. Unlike these agents, the interleukin-6 (IL-6) blocking agent TCZ which has recently been approved for management of GCA [11], has yielded promising results in terms of relapse-free remission without GC in several case reports and two open-label studies in PMR [72, 73]. The most common adverse event associated with TCZ in these studies was transient leukopenia and neutropenia [73]. Following these initial promising results, the IL-6 blocking agents TCZ and sarilumab are currently being evaluated for use in PMR in several RCTs (www.clinicaltrials.gov). Because IL-1 and IL-17 are presumed to play a role in PMR immunopathogenesis, the IL-17 blocking agent secukinumab and the IL-1 blocking agent canakinumab have both been trialed in a two-week, single-blind, randomized three-arm proof of concept study in PMR patients, showing rapid improvement in pain but only moderate improvement in movement so that the use of these agents requires further study [14]. Abatacept, which blocks the interaction of CD80/CD86 with CD28 leading to a decrease of T cell activation, has been used in a clinical trial in GCA showing improved relapse-free survival at 12 months and longer median duration of remission compared to placebo following discontinuation of GC at week 28 [74] but has yet to be trialed in PMR. Current ongoing studies on relapsing GCA treatment also involve Janus kinase/signal transducers and activators of transcription (JAK/STAT inhibitors) baricitinib and upadacitinib following successful completion of several animal model studies on GCA showing suppression of T cell accumulation in blood vessel walls with reduction in interferon-gamma production by tofacitinib [14, 75, 76]. However, their role in PMR management is still unknown. A single center, open-label, prospective 15-patient study of low-dose IL-2 is currently also underway for PMR treatment as well (www.clinicaltrials.gov).
Monitoring PMR Disease Activity
Clinicians should closely monitor patients with PMR for clinical and laboratory signs of disease activity and evidence of GC-related toxicity. Monitoring is suggested every 4–8 weeks in the 2–4 months after treatment is started and then every 4–12 weeks during the first year of disease. In the second year, monitoring should be done every 8–12 weeks and as indicated in cases of relapse during tapering of GC or other immunosuppressive agents [4].
Currently, there is no generally accepted definition of remission or relapse in PMR, but the absence of PMR symptoms, particularly morning stiffness, in conjunction with normal ESR and CRP, has often been used to define remission in clinical studies [77]. Conversely, the reappearance of clinical signs of PMR, with or without ESR or CRP elevation, is considered to indicate relapse as a PMR flare in the absence of an increase in markers of inflammation may be observed in up to 25% of patients even if these markers were abnormal at time of diagnosis [4, 77].
In some studies, a composite PMR disease activity score has been used to determine disease activity level in PMR patients [4, 78] (Table 4). As in the generally accepted definitions of remission and relapse in PMR, this composite disease activity score relies on markers of inflammation to determine PMR disease activity. Notably, the advent of IL-6 inhibitors in the treatment of PMR poses a unique challenge in this regard because IL-6 inhibitors may affect ESR and CRP independently of disease control. This, in turn, may necessitate the development of alternative disease activity measures when utilizing these agents in PMR management.
Prognosis
Epidemiological studies attest to PMR having a benign course without affecting patient survival, with median duration of the disease running up to 11 months (range, 2–54 months) [79]). Three studies to date showed no differences in mortality rates among patients diagnosed with PMR without co-existing GCA compared with population controls [80,81,82], including CVD-related deaths [82], with a study by Myklebust et al. showing reduced cancer mortality rate among PMR patients relative to population controls (RR = 0.59, 95% CI 0.3–1.17) [82]. Similarly, a study by Gran et al. found increased survival among PMR patients without co-existing GCA relative to controls (RR = 0.70, 95% CI 0.52–0.95) [80], attributing improved medical surveillance in this population to higher patient survival.
Importantly, current literature suggests that the main morbidity related to PMR actually involves complications of GC therapy, and not PMR itself, with GC-induced complications occurring in up to 65% of patients [83]. Studies show that three variables independently increase the risk of adverse events among PMR patients: age at PMR diagnosis, a cumulative dose of prednisone ≥ 1800 mg, and female sex [83]. Indeed, population studies reveal that long-term GC treatment in PMR patients carries with it a 2–5 times greater risk of diabetes mellitus, osteoporotic fractures (vertebral fractures, femoral neck fractures, and hip fractures) compared with age- and sex-matched individuals [83]. Therefore, patients being treated for PMR should be monitored regularly not only for disease activity, but also for GC-related toxicity. Management of comorbidities including CVD risks such as hypertension, diabetes, and hyperlipidemia as well as osteoporosis is necessary throughout the entire course of disease. In the case of osteoporosis, prophylaxis should be initiated along with initiation of GC treatment [84]. Because of the high morbidity associated with long-term GC use, the GC toxicity index (GTI) was recently devised as a composite measure score in GC toxicity and has already been used in clinical trials, focusing on measuring changes in specific domains related to GC-related toxicity over the treatment period [85•] (Table 5). In this scoring system, evaluation of two time points is required for scoring to show change in GC-related toxicity over time. In any domain, the most severe item is scored, with score reported as both a total score and a domain-specific score.
Conclusion (Key Points)
-
The majority of patients who present with PMR are correctly classified but it is important to remember mimicking conditions.
-
Increased CVD risk and several conditions such as EORA and GCA may overlap with PMR and should be considered in every patient.
-
PMR may occur following ICI therapy and may present atypically in these patients.
-
GC therapy remains the cornerstone of PMR treatment, though due to its myriad detrimental side effects, patients should be monitored for GC-induced toxicity.
-
MTX is accepted as a GC-sparing agent in PMR, but additional conventional and biologic DMARDs are currently being trialed in PMR management, most notably IL-6 blocking agents.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Barber HS. Myalgic syndrome with constitutional effects; polymyalgia rheumatica. Ann Rheum Dis. 1957;16:230–7.
Michet CJ, Matteson EL. Polymyalgia rheumatica. BMJ. 2008;336:765–9.
Crowson CS, Matteson EL, Myasoedova E, Michet CJ, Ernste FC, Warrington KJ, et al. The lifetime risk of adult-onset rheumatoid arthritis and other inflammatory autoimmune rheumatic diseases. Arthritis Rheum. 2011;63:633–9.
Matteson EL, Dejaco C. Polymyalgia Rheumatica. Ann Intern Med. 2017;166:ITC65–80.
Dejaco C, Duftner C, Buttgereit F, Matteson EL, Dasgupta B. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology. 2017;56:506–15.
Dejaco C, Duftner C, Schirmer M. Are regulatory T-cells linked with aging? Exp Gerontol. 2006;41:339–45.
Franceschi C, Bonafè M, Valensin S, Olivieri F, De Luca M, Ottaviani E, et al. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann N Y Acad Sci. 2000;908:244–54.
Mohan SV, Liao YJ, Kim JW, Goronzy JJ, Weyand CM. Giant cell arteritis: immune and vascular aging as disease risk factors. Arthritis Res Ther. 2011;13:231.
Singh JA, Cleveland JD. The risk of polymyalgia rheumatica in older adults with gout: a Medicare claims study. Rheumatol Adv Pract. 2018;2.
Samson M, Audia S, Fraszczak J, Trad M, Ornetti P, Lakomy D, et al. Th1 and Th17 lymphocytes expressing CD161 are implicated in giant cell arteritis and polymyalgia rheumatica pathogenesis. Arthritis Rheum. 2012;64:3788–98.
Stone JH, Klearman M, Collinson N. Trial of Tocilizumab in Giant-cell arteritis. N Engl J Med. 2017;377:1494–5.
Salvarani C, Gabriel SE, O’Fallon WM, Hunder GG. The incidence of giant cell arteritis in Olmsted County, Minnesota: apparent fluctuations in a cyclic pattern. Ann Intern Med. 1995;123:192–4.
England BR, Mikuls TR, Xie F, Yang S, Chen L, Curtis JR. Herpes zoster as a risk factor for incident giant cell arteritis. Arthritis Rheum. 2017;69:2351–8.
Castañeda S, García-Castañeda N, Prieto-Peña D, Martínez-Quintanilla D, Vicente EF, Blanco R, et al. Treatment of polymyalgia rheumatica. Biochem Pharmacol. 2019;165:221–9.
Salvarani C, Macchioni PL, Tartoni PL, Rossi F, Baricchi R, Castri C, et al. Polymyalgia rheumatica and giant cell arteritis: a 5-year epidemiologic and clinical study in Reggio Emilia, Italy. Clin Exp Rheumatol. 1987;5:205–15.
Caylor TL, Perkins A. Recognition and management of polymyalgia rheumatica and giant cell arteritis. Am Fam Physician. 2013;88:676–84.
Wise CM, Agudelo CA, Chmelewski WL, McKnight KM. Temporal arteritis with low erythrocyte sedimentation rate: a review of five cases. Arthritis Rheum. 1991;34:1571–4.
Hazleman B. Laboratory investigations useful in the evaluation of polymyalgia rheumatica (PMR) and giant cell arteritis (GCA). Clin Exp Rheumatol. 2000;18:S29–31.
Chakravarty K, Pountain G, Merry P, Byron M, Hazleman B, Scott DG. A longitudinal study of anticardiolipin antibody in polymyalgia rheumatica and giant cell arteritis. J Rheumatol. 1995;22:1694–7.
Patil P, Dasgupta B. Polymyalgia rheumatica in older adults. Aging Health. 2013;9:483–95.
Camellino D, Cimmino MA. Are the new ACR/EULAR criteria the ultimate answer for polymyalgia rheumatica classification? J Rheumatol. 2016;43:836–8.
Dejaco C, Singh YP, Perel P, Hutchings A, Camellino D, Mackie S, et al. 2015 recommendations for the management of polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum. 2015;67:2569–80.
Dasgupta B, Cimmino MA, Maradit-Kremers H, Schmidt WA, Schirmer M, Salvarani C, et al. 2012 provisional classification criteria for polymyalgia rheumatica: a European league against rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis. 2012;71:484–92.
Macchioni P, Boiardi L, Catanoso M, Pazzola G, Salvarani C. Performance of the new 2012 EULAR/ACR classification criteria for polymyalgia rheumatica: comparison with the previous criteria in a single-centre study. Ann Rheum Dis. 2014;73:1190–3.
Ozen G, Inanc N, Unal AU, Bas S, Kimyon G, Kisacik B, et al. Assessment of the new 2012 EULAR/ACR clinical classification criteria for polymyalgia rheumatica: a prospective multicenter study. J Rheumatol. 2016;43:893–900.
González-Gay, García-Porrúa, Salvarani, Olivieri, Hunder. Polymyalgia manifestations in different conditions mimicking polymyalgia rheumatica. Clin Exp Rheumatol. 2000;18:755–9.
Ceccato F, Uña C, Regidor M, Rillo O, Babini S, Paira S. Conditions mimicking polymyalgia rheumatica. Reumatol Clin. 2011;7:156–60.
•• Partington R, Helliwell T, Muller S, Abdul Sultan A, Mallen C. Comorbidities in polymyalgia rheumatica: a systematic review. Arthritis Res Ther. 2018;20:258 This study is an excellent systematic review on the literature examining the prevalence of comorbidities associated with PMR.
Hancock AT, Mallen CD, Muller S, Belcher J, Roddy E, Helliwell T, et al. Risk of vascular events in patients with polymyalgia rheumatica. Can Med Assoc J. 2014;186:E495–501.
Ungprasert P, Koster MJ, Warrington KJ, Matteson EL. Polymyalgia rheumatica and risk of coronary artery disease: a systematic review and meta-analysis of observational studies. Rheumatol Int. 2017;37:143–9.
Maradit Kremers H, Reinalda MS, Crowson CS, Davis JM, Hunder GG, Gabriel SE. Glucocorticoids and cardiovascular and cerebrovascular events in polymyalgia rheumatica. Arthritis Rheum. 2007;57:279–86.
Bowness P, Shotliff K, Middlemiss A, Myles AB. Prevalence of hypothyroidism in patients with polymyalgia rheumatica and giant cell arteritis. Br J Rheumatol. 1991;30:349–51.
Juchet H, Labarthe MP, Ollier S, Vilain C, Arlet P. Prevalence of hypothyroidism and hyperthyroidism in temporal arteritis and rhizomelic pseudopolyarthritis. A controlled study of 104 cases. Rev Rhum Ed Fr. 1993;60:493–8.
Li X, Sundquist J, Sundquist K. Subsequent risks of Parkinson disease in patients with autoimmune and related disorders: a nationwide epidemiological study from Sweden. Neurodegener Dis. 2012;10:277–84.
Chakravarty E, Genovese MC. Rheumatic syndromes associated with malignancy. Curr Opin Rheumatol. 2003;15:35–43.
Muller S, Hider SL, Belcher J, Helliwell T, Mallen CD. Is cancer associated with polymyalgia rheumatica? A cohort study in the General Practice Research Database. Ann Rheum Dis. 2014;73:1769–73.
Ji J, Liu X, Sundquist K, Sundquist J, Hemminki K. Cancer risk in patients hospitalized with polymyalgia rheumatica and giant cell arteritis: a follow-up study in Sweden. Rheumatology. 2010;49:1158–63.
Pfeifer EC, Crowson CS, Major BT, Matteson EL. Polymyalgia rheumatica and its association with cancer. Rheumatology (Sunnyvale). 2015;Suppl 6.
Myklebust G, Wilsgaard T, Jacobsen BK, Gran JT. No increased frequency of malignant neoplasms in polymyalgia rheumatica and temporal arteritis. A prospective longitudinal study of 398 cases and matched population controls. J Rheumatol. 2002;29:2143–7.
Naschitz JE, Slobodin G, Yeshurun D, Rozenbaum M, Rosner I. Atypical polymyalgia rheumatica as a presentation of metastatic cancer. Arch Intern Med. 1997;157:2381.
Gonzalez-Gay MA, Garcia-Porrua C, Salvarani C, Olivieri I, Hunder GG. The spectrum of conditions mimicking polymyalgia rheumatica in northwestern Spain. J Rheumatol. 2000;27:2179–84.
Gonzalez-Gay MA. Giant cell arteritis and polymyalgia rheumatica: two different but often overlapping conditions. Semin Arthritis Rheum. 2004;33:289–93.
Blockmans D, De Ceuninck L, Vanderschueren S, Knockaert D, Mortelmans L, Bobbaers H. Repetitive 18-fluorodeoxyglucose positron emission tomography in isolated polymyalgia rheumatica: a prospective study in 35 patients. Rheumatology. 2007;46:672–7.
Schmidt WA, Gromnica-Ihle E. Incidence of temporal arteritis in patients with polymyalgia rheumatica: a prospective study using colour Doppler ultrasonography of the temporal arteries. Rheumatology. 2002;41:46–52.
Salvarani C, Cantini F, Hunder G. Polymyalgia rheumatica and giant-cell arteritis. Lancet. 2008;372:234–45.
Laskou F, Coath F, Mackie SL, Banerjee S, Aung T, Dasgupta B. A probability score to aid the diagnosis of suspected giant cell arteritis. Clin Exp Rheumatol. 2019;37(Suppl 117):104–8.
González-Gay MA, García-Porrúa C, Vázquez-Caruncho M. Polymyalgia rheumatica in biopsy proven giant cell arteritis does not constitute a different subset but differs from isolated polymyalgia rheumatica. J Rheumatol. 1998;25:1750–5.
McCarty DJ, O’Duffy JD, Pearson L, Hunter JB. Remitting seronegative symmetrical synovitis with pitting edema. RS3PE syndrome. JAMA. 1985;254:2763–7.
Varshney AN, Singh NK. Syndrome of remitting seronegative symmetrical synovitis with pitting edema: a case series. J Postgrad Med. 2015;61:38–41.
Belloli L, Massarotti M, Marasini B. Polymyalgia rheumatica and elderly onset rheumatoid arthritis. J Clin Rheumatol. 2008;14:59.
Goldstein BL, Gedmintas L, Todd DJ. Drug-associated polymyalgia rheumatica/giant cell arteritis occurring in two patients after treatment with ipilimumab, an antagonist of ctla-4. Arthritis Rheum. 2014;66:768–9.
Garel B, Kramkimel N, Trouvin A-P, Frantz C, Dupin N. Pembrolizumab-induced polymyalgia rheumatica in two patients with metastatic melanoma. Joint Bone Spine. 2017;84:233–4.
• Calabrese C, Cappelli LC, Kostine M, Kirchner E, Braaten T, Calabrese L. Polymyalgia rheumatica-like syndrome from checkpoint inhibitor therapy: case series and systematic review of the literature. RMD Open. 2019;5:e000906 This systematic review is unique in highlighting atypical clinical features of ICI-related PMR.
Belkhir R, Burel SL, Dunogeant L, Marabelle A, Hollebecque A, Besse B, et al. Rheumatoid arthritis and polymyalgia rheumatica occurring after immune checkpoint inhibitor treatment. Ann Rheum Dis. 2017;76:1747–50.
Zhang H, Watanabe R, Berry GJ, Vaglio A, Liao YJ, Warrington KJ, et al. Immunoinhibitory checkpoint deficiency in medium and large vessel vasculitis. Proc Natl Acad Sci U S A. 2017;114:E970–9.
van Assen S, Agmon-Levin N, Elkayam O, Cervera R, Doran MF, Dougados M, et al. EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis. 2011;70:414–22.
Singh JA, Furst DE, Bharat A, Curtis JR, Kavanaugh AF, Kremer JM, et al. 2012 update of the 2008 American College of Rheumatology recommendations for the use of disease-modifying antirheumatic drugs and biologic agents in the treatment of rheumatoid arthritis. Arthritis Care Res. 2012;64:625–39.
Dasgupta B, Borg FA, Hassan N, Barraclough K, Bourke B, Fulcher J, et al. BSR and BHPR guidelines for the management of polymyalgia rheumatica. Rheumatology. 2010;49:186–90.
Matteson EL, Maradit-Kremers H, Cimmino MA, Schmidt WA, Schirmer M, Salvarani C, et al. Patient-reported outcomes in polymyalgia rheumatica. J Rheumatol. 2012;39:795–803.
Hernández-Rodríguez J, Cid MC, López-Soto A, Espigol-Frigolé G, Bosch X. Treatment of polymyalgia rheumatica: a systematic review. Arch Intern Med. 2009;169:1839–50.
Dasgupta B, Dolan AL, Panayi GS, Fernandes L. An initially double-blind controlled 96 week trial of depot methylprednisolone against oral prednisolone in the treatment of polymyalgia rheumatica. Br J Rheumatol. 1998;37:189–95.
Sundahl N, Bridelance J, Libert C, De Bosscher K, Beck IM. Selective glucocorticoid receptor modulation: new directions with non-steroidal scaffolds. Pharmacol Ther. 2015;152:28–41.
van den Hoven JM, Van Tomme SR, Metselaar JM, Nuijen B, Beijnen JH, Storm G. Liposomal drug formulations in the treatment of rheumatoid arthritis. Mol Pharm. 2011;8:1002–15.
Raine C, Stapleton PP, Merinopoulos D, Maw WW, Achilleos K, Gayford D, et al. A 26-week feasibility study comparing the efficacy and safety of modified-release prednisone with immediate-release prednisolone in newly diagnosed cases of giant cell arteritis. Int J Rheum Dis. 2018;21:285–91.
Ferraccioli G, Salaffi F, De Vita S, Casatta L, Bartoli E. Methotrexate in polymyalgia rheumatica: preliminary results of an open, randomized study. J Rheumatol. 1996;23:624–8.
Caporali R, Cimmino MA, Ferraccioli G, Gerli R, Klersy C, Salvarani C, et al. Prednisone plus methotrexate for polymyalgia rheumatica: a randomized, double-blind, placebo-controlled trial. Ann Intern Med. 2004;141:493–500.
De Silva M, Hazleman BL. Azathioprine in giant cell arteritis/polymyalgia rheumatica: a double-blind study. Ann Rheum Dis. 1986;45:136–8.
Adizie T, Christidis D, Dharmapaliah C, Borg F, Dasgupta B. Efficacy and tolerability of leflunomide in difficult-to-treat polymyalgia rheumatica and giant cell arteritis: a case series. Int J Clin Pract. 2012;66:906–9.
Diamantopoulos AP, Hetland H, Myklebust G. Leflunomide as a corticosteroid-sparing agent in giant cell arteritis and polymyalgia rheumatica: a case series. Biomed Res Int. 2013;2013:120638.
Salvarani C, Macchioni P, Manzini C, Paolazzi G, Trotta A, Manganelli P, et al. Infliximab plus prednisone or placebo plus prednisone for the initial treatment of polymyalgia rheumatica: a randomized trial. Ann Intern Med. 2007;146:631–9.
Kreiner F, Galbo H. Effect of etanercept in polymyalgia rheumatica: a randomized controlled trial. Arthritis Res Ther. 2010;12:R176.
Lally L, Forbess L, Hatzis C, Spiera R. Brief report: a prospective open-label phase IIa trial of tocilizumab in the treatment of polymyalgia rheumatica. Arthritis Rheum. 2016;68:2550–4.
Devauchelle-Pensec V, Berthelot JM, Cornec D, Renaudineau Y, Marhadour T, Jousse-Joulin S, et al. Efficacy of first-line tocilizumab therapy in early polymyalgia rheumatica: a prospective longitudinal study. Ann Rheum Dis. 2016;75:1506–10.
Langford CA, Cuthbertson D, Ytterberg SR, Khalidi N, Monach PA, Carette S, et al. A randomized, double-blind trial of abatacept (CTLA-4Ig) for the treatment of giant cell arteritis. Arthritis Rheum. 2017;69:837–45.
O’Shea JJ, Kontzias A, Yamaoka K, Tanaka Y, Laurence A. Janus kinase inhibitors in autoimmune diseases. Ann Rheum Dis. 2013;72(Suppl 2):ii111–5.
Zhang H, Watanabe R, Berry GJ, Tian L, Goronzy JJ, Weyand CM. Inhibition of JAK-STAT signaling suppresses pathogenic immune responses in medium and large vessel vasculitis. Circulation. 2018;137:1934–48.
Dejaco C, Duftner C, Cimmino MA, Dasgupta B, Salvarani C, Crowson CS, et al. Definition of remission and relapse in polymyalgia rheumatica: data from a literature search compared with a Delphi-based expert consensus. Ann Rheum Dis. 2011;70:447–53.
Leeb BF, Bird HA. A disease activity score for polymyalgia rheumatica. Ann Rheum Dis. 2004;63:1279–83.
Chuang TY, Hunder GG, Ilstrup DM, Kurland LT. Polymyalgia rheumatica: a 10-year epidemiologic and clinical study. Ann Intern Med. 1982;97:672–80.
Gran JT, Myklebust G, Wilsgaard T, Jacobsen BK. Survival in polymyalgia rheumatica and temporal arteritis: a study of 398 cases and matched population controls. Rheumatology. 2001;40:1238–42.
Doran MF, Crowson CS, O’Fallon WM, Hunder GG, Gabriel SE. Trends in the incidence of polymyalgia rheumatica over a 30 year period in Olmsted County, Minnesota, USA. J Rheumatol. 2002;29:1694–7.
Myklebust G, Wilsgaard T, Jacobsen BK, Gran JT. Causes of death in polymyalgia rheumatica. A prospective longitudinal study of 315 cases and matched population controls. Scand J Rheumatol. 2003;32:38–41.
Gabriel SE, Sunku J, Salvarani C, O’Fallon WM, Hunder GG. Adverse outcomes of antiinflammatory therapy among patients with polymyalgia rheumatica. Arthritis Rheum. 1997;40:1873–8.
Buckley L, Guyatt G, Fink HA, Cannon M, Grossman J, Hansen KE, et al. 2017 American College of Rheumatology Guideline for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Rheum. 2017;69:1521–37.
• Miloslavsky EM, Naden RP, Bijlsma JWJ, Brogan PA, Brown ES, Brunetta P, et al. Development of a glucocorticoid toxicity index (GTI) using multicriteria decision analysis. Ann Rheum Dis. 2017;76:543–6 This study is the official report delineating the development and outcome measures incorporated into the GTI.
Slobodin G, Rimar D, Boulman N, Kaly L, Rozenbaum M, Rosner I, et al. Acute sacroiliitis. Clin Rheumatol. 2016;35:851–6.
Gazitt T, Kibari A, Nasrallah N, Abu Elhija M, Zisman D. Polymyalgia rheumatica: the great imitator. Isr Med Assoc J. 2019;21:627–8.
Mallia C, Coleiro B, Crockford M, Ellul B. Raynaud’s phenomenon caused by giant cell arteritis. A case report. Adv Exp Med Biol. 1999;455:517–20.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Human and Animal Rights and Informed Consent
The patient’s written consent was obtained for the figures found in this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Rheumatoid Arthritis
Electronic supplementary material
ESM 1
(DOC 115 kb)
Rights and permissions
About this article

Cite this article
Gazitt, T., Zisman, D. & Gardner, G. Polymyalgia Rheumatica: a Common Disease in Seniors. Curr Rheumatol Rep 22, 40 (2020). https://doi.org/10.1007/s11926-020-00919-2
Published:
DOI: https://doi.org/10.1007/s11926-020-00919-2