
Abstract
Purpose of the Review
Results from epidemiological studies suggest that vitamin D (VD) deficiency (VDD) may be a cause of hypertension (HTN). However, the results of randomized clinical trials (RCTs) designed to address the impact of VD supplementation on reducing blood pressure (BP) remain equivocal. To determine whether VD might serve as a beneficial treatment option for a specific subset of hypertensive patients, we performed a stratified analysis of RCT data and addressed problems associated with some methodological issues.
Recent Findings
HTN is caused by multiple factors. VDD may be one of the factors contributing to the development of this disorder. There are more than 70 RCTs that examined the impact of VD supplementation on BP. These RCTs can be classified into four groups based on their respective study populations, including participants who are (1) VD-sufficient and normotensive, (2) VD-deficient and normotensive, (3) VD-sufficient and hypertensive, and (4) VD-deficient and hypertensive.
Summary
Our evaluation of these studies demonstrates that VD supplementation is ineffective when used to reduce BP in VD-sufficient normotensive subjects. VD supplementation for five years or more may reduce the risk of developing HTN specifically among those with VDD. Interestingly, findings from 12 RCTs indicate that daily or weekly supplementation, as opposed to large bolus dosing, results in the reduction of BP in VD-deficient hypertensive patients. Our ongoing research focused on elucidating the mechanisms of VDD-induced HTN will ultimately provide evidence to support the development of etiology-specific prevention and treatment strategies focused on HTN in the VD-deficient population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Uncontrolled hypertension (HTN) is a major risk factor for stroke, cardiovascular disease, renal failure, and increased maternal mortality [1]. Although several different types of antihypertensive medications are currently available [2], ~50% of hypertensive patients in the USA have blood pressure (BP) that is poorly controlled. Furthermore, approximately five million patients with HTN are resistant to therapy [3]. A recent publication in the Journal of the American Medical Association [4••] reported that in 2017–2018, only 43.7% of adults diagnosed with HTN exhibited adequate BP control (age-adjusted rate); this represented a decline from 53.8% reported for the years 2013–2014. Among the major problems limiting effective treatment of this disorder, more than 95% of these patients have been diagnosed with essential HTN of unknown cause with no etiology-specific therapies. The less effective yet lifelong therapies available for these patients have become a severe burden for our society [5]. Thus, efforts to identify causal factors and therapeutic targets are urgently needed in promoting the development of etiology-specific prevention and treatment of HTN.
Vitamin D deficiency (VDD) is commonly defined as serum 25-hydroxy vitamin D (25[OH]D) levels <20 ng/ml [6, 7]. The well-characterized sequelae of VDD include nutritional rickets in children, osteomalacia in women, and increased severity of fractures secondary to falls in the elderly. Over the past 20 years, large-scale cross-sectional and cohort analyses, as well as Mendelian randomization and prospective studies, have demonstrated that serum 25[OH]D levels are inversely related to elevated BP, HTN, and adverse cardiovascular events [8]. These findings are supported by the results of studies using genetic and nutrient-depleted VD-deficient animal models that display hypertensive phenotypes [9]. Collectively, the results of these studies suggest that VDD may also contribute to human HTN and that VD supplementation may be effective means for its prevention and treatment. Well-designed RCTs are powerful tools that might be used to assess the contributions of VD in HTN. Although RCTs are currently considered the gold standard, studies that are poorly designed, conducted, analyzed, and reported can provide highly misleading results. When designing RCTs to address the impact of VD, which has been identified as a threshold nutrient [10] (described further below), clarity with respect to the participants’ baseline BP and serum 25[OH]D levels, as well as the specific dosing regimens is critical to their ultimate success (see below in detail).
At this time, findings are available from more than 70 RCTs that were designed to evaluate the role of VD in reducing BP. These can be classified into four groups based on baseline levels of serum 25[OH]D and BP in selected study populations; of note, several of the earliest RCTs are without serum 25[OH]D data. As a group, these studies include participants that are (1) VD-sufficient and normotensive, (2) VD-deficient and normotensive, (3) VD-sufficient and hypertensive, and (4) VD- deficient and hypertensive. We have also re-evaluated these findings based on the recent changes in the guidelines used to diagnose HTN. While the new guidelines, which have reduced the threshold for diagnosing HTN [11], may benefit some patients at high risk of developing cardiovascular disease, most individuals are identified as hypertensive at a BP of 140/90 mmHg or greater [12]. Many of the clinical trials discussed in this review were completed before the release of the new guidelines. Thus, for this review, “normotensive” denotes BP < 140/90 mmHg and “hypertensive” refers to BP ≥ 140/90 mmHg.
VD Supplementation is Ineffective in Reducing BP in VD-Sufficient Normotensive Subjects
In 1998, Krause et al. [13] used ultraviolet B (UVB) irradiation to treat a group of patients with otherwise untreated essential HTN and VDD. The treatment resulted in a 162% increase in serum levels of 25[OH]D and a significant reduction (6 mmHg) in both systolic and diastolic BP (SBP/DBP). While this finding has led some investigators to perform clinical trials using VD to treat this specific cohort of hypertensive patients, other investigators have gone forward to examine the use of VD to reduce BP in the general population. This direction was largely based on the theory that VD could suppress basal expression of the endogenous hormone, renin [14]. Since that time, many lines of evidence have emerged that suggest that a modest increase in renin levels has little to no impact on VDD-associated HTN [8, 9].
In contrast to exogenous BP-reducing drugs (for example, the renin inhibitor, aliskiren), VD is synthesized in skin exposed to sunlight and can also be obtained from dietary sources (e.g., milk). VD is a well-known threshold nutrient, meaning that physiological responses (e.g., promoting calcium absorption) are dose-dependent at low concentrations; once a threshold value is reached, higher levels of the given nutrient promote limited beneficial effects [10, 15••, 16••]. Thus, it will be critical to have a clear understanding of endogenous VD levels in participants selected for this type of study. One is unlikely to see a great benefit from VD supplementation of normotensive study participants if their baseline serum 25[OH]D levels are already above the threshold level. These observations can explain the negative outcomes from many of the RCTs that demonstrated no effect of VD supplementation on BP in the general population, including those who are normotensive and VD- sufficient [8, 17–19].
The ongoing vitamin D and Omega-3 HTN trial (VITAL HTN; NCT01653678) was designed to examine long-term VD supplementation (2000 UI daily for five years) as a means to prevent HTN in participants aged ≥ 50 years who presented with normal BP. VITAL researchers have already published one report [20], stating that VD supplementation did not reduce the incidence of cardiovascular events among the participants who presented with adequate mean levels of VD (only 12.7% of participants were VD-deficient). These preliminary results suggest that VD supplementation is unlikely to have a significant impact on the incidence of HTN in participants who were VD-sufficient at baseline.
A Five-Year Trial of VD Supplementation May Reduce the Risk of Developing HTN in Vulnerable Normotensive Populations Presenting with VDD
Low serum VD levels have been associated with an increased risk of developing HTN [8, 9]. Thus, VD supplementation should reduce the incidence of HTN in susceptible subjects with VDD and normotension at baseline. Because HTN is an age-dependent, chronic disease with a long induction period, it may be essential to provide long-term VD supplementation to this target treatment group. Recent advances from large RCTs suggest that VD supplementation should be provided over a five-year period in order to determine its effects on the incidence of chronic diseases (e.g., HTN) [15••, 16••]. Thus, the negative results from previous studies in which VD supplementation was time limited (≤18 months) may need to be re-evaluated, as the study period was not long enough to record a sufficient number of events [21–27].
Results from a recent clinical trial revealed that two years of VD supplementation at 800 IU and 2000 IU per day reduced mean SBP by 3.94 and 2.75 mmHg, respectively, in a VD-deficient cohort of patients ≥60 years of age [28•]. Unfortunately, this study did not include a placebo group, and thus, the findings presented do not permit us to conclude that VD supplementation effectively reduces BP. Future RCTs that include placebo groups should determine whether a similar or more reduction in BP can achieved with these doses of VD over five years in vulnerable VD-deficient patients. These findings would be of substantial clinical significance because every 10-mmHg reduction in SBP has been associated with reduction of 20% in major cardiovascular disease events, 17% in coronary heart disease, 27% in stroke, 28% in heart failure, and 13% in all-cause mortality [29]. It is critical to note that there were no statistically significant differences between the responses to 800 IU and 2000 IU [28•]; this observation suggests that the maximum impact of VD on reducing BP in a normotensive population may be achieved via a regimen of 800 IU per day for two years or longer. Subsequently, the same group published the results of the DO-HEALTH RCT which demonstrated that daily supplementation with 2000 IU or control (i.e., a lower dose of VD) over three years reduced SBP by 8.6 and 7.9 mmHg, respectively, in hypertensive elderly cohort with VD insufficiency [30]. Since all participants were allowed to take 800 IU VD daily in the DO-HEALTH RCT [31], one assumes that the “no VD” control group [30] was taking this lower dose. Reductions in BP among those treated with 2000 IU VD per day were no different from the responses of the control group, suggesting that daily 800 IU of VD for three years provided the maximum benefit in reducing BP in elderly patients with both HTN and VD insufficiency.
At baseline, BP is regulated by interactions between genetic, epigenetic, and environmental factors that maintain a stable balance between vasocontraction and vasodilation [8]. While VDD may also result in elevated BP in those <40 years of age, these younger individuals may have the capacity to maintain normal BP and vascular tone due to sufficient compensatory mechanisms (e.g., endothelial nitric oxide synthase [eNOS]-dependent signaling pathways). Thus, younger people with VDD may not develop HTN [32].
VD Supplementation has a Modest Effect on Some Hypertensive Patients Who are VD-Sufficient
Many different factors including single gene mutation (e.g., Liddle syndrome) and environmental factors (e.g., high-salt diet) can cause HTN. VDD is potentially one of the causal factors for HTN. Unlike nutritional rickets caused by a single factor (VDD) and cured by VD repletion, VD supplementation is unlikely to be an effective treatment for all types of HTN caused by multiple factors. For example, Larsen et al. [33] treated 112 hypertensive patients with 3000 IU VD or placebo daily for 20 weeks. In this study, supplementation with VD resulted in increased serum levels of VD levels but had no significant impact on BP evaluated over a 24-h period. However, a post hoc analysis of 92 study participants who presented with VDD or VD insufficiency at baseline revealed dramatic reductions in SBP/DBP specifically in this subgroup. These results suggest that patients who develop HTN secondary to other causes other than VDD may not benefit substantially from VD supplementation.
As we noted earlier in this review, VD provided at levels above a specific threshold may not lead to additional beneficial effects under normal physiologic conditions. However, during the development of some types of HTN, the threshold level for VD can be increased, a phenomenon in which enhanced VD signaling acts as a negative feedback hormonal regulator to inhibit an excessively high BP level. Animal studies have revealed that administration of VD or its analogs can result in modest, but significant reductions in BP in spontaneously hypertensive rats (SHRs) [34, 35] and in cases of angiotensin II (Ang II)-induced HTN in mice [36], while they have no impact on high-salt induced HTN [37]. These findings suggest that boosting VD signaling may result in reductions in BP in certain types of HTN with normal VD levels at baseline and that VD exerts its antihypertensive role partly via its capacity to reduce Ang II-induced vasocontraction and enhance atrial natriuretic peptide-induced vasodilation (Chen S et al. submitted). While an appropriate dose and dose interval of VD may result in reductions in BP in some, but not all VD-sufficient hypertensive patients, the results from the clinical trials that recruited hypertensive cohorts who are VD sufficient may not be fully consistent.
VD Supplementation Reduces BP in Hypertensive Patients with VDD
An ideal RCT designed to determine whether VD can be an effective treatment for HTN should target hypertensive patients with VDD. The experimental group should be treated with a constant, non-intermittent physiological dose of VD, while the controls should be treated with either placebo or VD at an ineffective low dose. To date, more than 10 trials developed using this design (including ours in which the key methods and findings were described [8]) have revealed that daily supplementation with VD (800–4000 IU), VD analogs, or UVB radiation restored serum 25[OH]D levels and resulted in a significant reduction in BP in VD-deficient hypertensive subjects [13, 33, 38–44]. These findings are consistent with the results of two earlier RCTs that also found that daily administration of a VD analog could reduce BP in hypertensive patients in which 25[OH]D levels were not known [45, 46]. Another two RCTs demonstrated that weekly doses of VD resulted in effective reductions in BP in hypertensive patients with VDD [47, 48]. Despite the comparatively small sample sizes in these trials, these outcomes consistently demonstrate that daily or weekly administration of appropriate doses of VD or its analogs can significantly reduce BP in VD-deficient hypertensive populations. These data provide the rationale for studies designed to elucidate the cellular and molecular mechanisms underlying VDD-induced HTN. The results of these mechanistic studies will provide a molecular basis and evidence to support large RCTs in which VD supplementation is used for etiology-specific prevention or treatment of HTN. Toward this end, our group has shown that cell-specific deletion of the VD receptor in vascular smooth cells results in HTN which may be due to a concomitant increase in the expression of modulatory calcineurin-interacting protein 1 (Chen S et al., submitted). The results of this study suggest that VD signaling in vascular smooth muscle cells may play a critical role in the pathogenesis of VDD-induced HTN.
Some of the trials in this group reported negative results, many of which might be attributed to problems with the study designs. The use of intermittent large bolus doses [49–53] leads to wide fluctuations in circulating VD levels and does not provide the steady and effective dose required by the vascular system [15••, 54–56]. Large boluses of VD may even have a toxic effect on the vascular walls (discussed below).
VD Supplementation Via Intermittent Large Bolus Doses has no Impact on BP in Hypertensive Patients with VDD
VD is an essential nutrient that supports bone health [7]. While administration of VD (e.g., 800–2000 IU daily) reduces the risk of fractures secondary to falls in the elderly [57], monthly or yearly administration of large bolus doses (e. g., 60,000–100,000 IU monthly or 300,000–500,000 IU annually) has no effect or may even increase the risk of fracture [58–62]. By contrast, daily doses of more appropriate concentrations of VD (e.g., 800–4000 IU daily) or its active forms are effective antihypertensive treatments for patients with both HTN and VDD [13, 33, 38–43]. Several trials have examined the impact of intermittent large bolus doses (e.g.,100,000 IU VD at 1–3 times per year) and reported that this regimen does not reduce BP in VD-deficient patients with HTN [49–53], most notably in those >70 years of age [49, 51, 52]. Interestingly, two previous small RCTs reported that large bolus doses of VD reduced SBP in patients with type 2 diabetes (T2D) and HTN after 8 weeks [63, 64], but not at 16 weeks of treatment [64]. The transient hypotensive role of VD administered in this fashion may be related to its toxic effect on patients with T2D and HTN who frequently exhibit larger blood volumes due to high serum glucose levels. Consistent with this interpretation, we found administration of high-dose VD to rats led to a significant increase in daily urine volume and a decrease in body weight (Chen S et al., unpublished data).
At this time, we have no clear understanding of the mechanisms underlying the vascular toxicity mediated by large bolus doses of VD or the lack of response among hypertensive patients with VDD. Several lines of evidence may be introduced that might clarify this scenario. Heaney et al. [54] found that a bolus injection of 100,000 IU VD in a group of healthy adults (n = 30) led to the elevation of plasma mean VD levels of 521 pmol/L. This concentration, which was 100-fold higher than the basal level evaluated over the previous 24 h, returned to near baseline in seven days. The injection resulted in a slow rise in serum 25[OH]D; these levels reached a peak at 515 nmol/L at seven days and returned to baseline (~68 nmol/L) after about four months. The active form of VD, 1,25-dihydroxyvitamin D (calcitriol) is synthesized by 25-hydroxylation of VD in the liver and subsequent 1-hydroxylation in the kidney and can also be generated locally in specific tissues [8]. VD-25-hydroxylase (also known as sterol 27-hydroxylase) is expressed in vascular endothelial cells [65, 66]; 25[OH]D 1-alpha-hydroxylase is expressed in both vascular endothelial and smooth muscle cells [67, 68]. The high concentration of VD introduced by bolus injection may result in the overproduction of calcitriol specifically in vascular endothelial and smooth muscle cells. In several animal models (e. g., pigs, rats, goats, and mice), large doses of VD can induce an osteoblastic phenotype in vascular smooth muscle cells that ultimately results in vascular calcification [69]. Elderly individuals (≥70 years old) frequently suffer from vascular stiffness; isolated systolic HTN is believed to be the direct result of vascular stiffness and calcification. Thus, the high doses of VD (e. g., 100,000 IU) administered in several of the aforementioned trials [49, 51–53] may actually promote vascular calcification, thereby counteracting any of its beneficial antihypertensive effects. Furthermore, while two studies demonstrated that large bolus doses of VD resulted in serum 25[OH]D levels that were similar to those reported in response to daily doses of VD, the levels obtained in response to the large bolus doses dropped significantly at the completion of the trials [70, 71]. Given that (1) vascular tissue cells can synthesize calcitriol and (2) circulating 25[OH]D levels do not reflect the full extent of VD activity in target tissues [72, 73], serum VD levels have been considered more important than serum 25[OH]D for the evaluation of VD activity in target tissues [55, 56]. Intermittent large bolus doses of VD that result in a rapid rise in serum VD levels followed by a similarly rapid return to basal levels may also contribute to the observed lack of effect of VD supplementation in several trials that included VD-deficient hypertensive populations. Finally, as described above [54], intermittent large bolus doses of VD produce wide fluctuations in circulating VD and 25[OH]D levels. These levels may change the physiological functioning of VD so that it will have no effect on the prevention of overall mortality due to fractures and falls among the elderly [74]. This treatment regimen may not be beneficial in patients with VDD-induced HTN because its impact is dramatically different from that of the daily dose schedule (e.g., 800–4000 IU per day) that generates a steady, more physiologic increase in serum VD and 25[OH]D levels over a longer period [75].
Further research will be required to elucidate the underlying mechanisms via which large bolus doses of VD promote vascular calcification. Additional studies will also be needed to determine why VD administered in this fashion either has no therapeutic efficacy or a detrimental impact on VDD-induced HTN. Nevertheless, a consensus of recent reviews has concluded that a constant physiological dose of VD results in steady levels of serum VD and 25[OH]D with optimal benefits. By contrast, intermittent large bolus doses of VD do not achieve steady or effective levels of VD and 25[OH]D and should not be used in these treatment regimens [15••].
Re-Evaluation of Meta-Analyses of Several RCTs
Meta-analyses aim to provide a more precise estimate of the effects of a specific situation or intervention as they can increase sample size and power by a combined review of primary studies with similar populations, controls, interventions, and outcomes. However, it has become clear that administration of VD to subjects in each of the four different aforementioned groups (i.e., VD-sufficient and normotensive, VD-deficient and normotensive, VD-sufficient and hypertensive, and VD-deficient and hypertensive) results in dramatically different outcomes. Furthermore, large intermittent bolus doses of VD are ineffective in reducing BP, even in hypertensive VD-deficient patient cohorts. Thus, pooling data from the four different groups will introduce a considerable amount of heterogeneity. Likewise, meta-analyses that do not consider the specific dosing regimens will also provide mistaken support for the null hypothesis. While none of the published meta-analyses designed to evaluate the role of VD supplementation in reducing BP have provided uniformly positive results, several recent reviews do conclude that VD supplementation can reduce BP in VD-deficient hypertensive patients [76, 77]. The conclusions from these two meta-analyses [76, 77] are supported by evidence from seven RCTs [33, 40, 42, 63, 64, 78, 79] that included 242 participants with an average age of 58.4 years who were recruited to the VD supplementation arm with mean baseline SBP/DBP ± SD of 134.7 ± 6.6/79 ± 4.9 mmHg. The administration of VD for 8–24 weeks reduced mean SBP/DBP by 5.5/2.6 mmHg (95% CIs, 5.2–5.8/2.4–2.8). All seven trials included patients undergoing treatment with HTN medication; however, the percentage of patients undergoing treatment and the types of HTN medication used varied widely. Co-administration of a calcium channel blocking agent had relatively little impact on the antihypertensive effect of VD [40]. However, VD supplementation alone resulted in minor and insignificant reductions in BP compared with the administration of placebo in one trial in which 85–90% and 70–85% of the participants were treated with angiotensin-converting enzyme/Ang II receptor inhibitors or diuretics, respectively [78]. As we noted above, VD exerts its antihypertensive effects partly via reductions in enhanced Ang II-induced vasoconstriction and recovery of impaired atrial natriuretic peptide-induced vasodilation. Administration of agents that block increases in Ang II and its downstream signaling molecules and/or the use of diuretics will mask the antihypertensive effects of VD in VDD hypertensive patients. Although all of these agents can reduce BP in these patients, VD may be an effective treatment that is also etiology-specific. By contrast, Ang II signaling blockers and diuretics are non-specific treatments that require lifelong administration. Patient age and ethnicity do not seem to have an impact on the results reported in these trials.
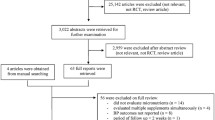
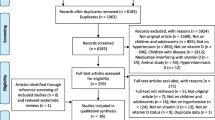
Other meta-analyses [80, 81] have not focused on problems with study methodology and have thus generated data that are not consistent with those that document the benefits of VD administration. One such study was performed by Beveridge et al. [80]. This meta-analysis included 46 clinical trials that were selected based on their use of VD supplementation for a minimum of 4 weeks and reported BP measurements. In 17 of these trials, participants had a mean baseline SBP ≥140 mmHg (based on findings shown in Fig. 2 and Table 1 of this publication); in seven of these trials, administration of VD or VD analogs results in a significant reduction in BP [41, 43, 45, 46, 63, 64, 82]. Of note, one trial reported that VD had no effect overall, but significantly reduced BP in the hypertensive subgroup with baseline 25[OH]D levels less than 32 ng/ml [33]. Another trial included in the meta-analysis reported that, when combined with several antihypertensive medications, administration of both VD and placebo resulted in significant decreases in BP [83]. Among the eight trials that reported no response to VD, one used a lower daily dose (400–600 IU) [84] and five administered large bolus doses [49, 51,52,53, 50]. Four studies in the latter group administered 100,000 IU VD to the elderly or patients with resistant HTN at intervals of 1–3 times in one year [49, 51,52,53] which is a treatment regimen that does not achieve steady or effective levels of VD and 25[OH]D [15••]. The large bolus dosing strategy used in each of these five trials may have led to the overall negative results. However, the authors of the meta-analysis did not specifically analyze treatment regimens and baseline VD levels in the relevant subgroup. Instead, they combined the subgroup data with those from the other 29 trials that recruited normotensive participants, from which they had concluded previously that VD supplementation did not affect BP in normotensive cohorts [85]. Thus, it is no surprise that pooling the data from all 46 trials, regardless of VD and hypertensive status revealed no significant reduction in BP from VD or its analogs.
Of note, at the end of the Results section of this meta-analysis and review, Beveridge et al. [80] reported that they analyzed data from a small group of patients (n = 60) with HTN and severe baseline VDD (25[OH]D at <10 ng/mL and parathyroid hormone >217 pg/ml). They stated that administration of VD was without benefit in these patients, but no references to primary studies were provided. Thus, we have no way of knowing whether these 60 patients received daily or intermittent large bolus doses of VD. Although we understand that this meta-analysis and review was published seven years ago before the data from the most recent RCTs were available, it is helpful to highlight the potential for misinterpretation that can be introduced when one pools data from heterogeneous trials without a clear assessment of potential errors in methodology. In this case, the meta-analysis led to a false conclusion regarding VD and its effectiveness in reducing BP. It is important to correct these conclusions as the field progresses.
Summary
Unlike pharmaceutical agents (e. g., prazosin or captopril), VD is an endogenous nutrient with a specific threshold that limits its therapeutic efficacy in lowering BP. It is critical to recognize that VD is not a panacea as it is not effective in reducing BP in the VD-sufficient normotensive population. However, an appropriate VD regimen (e. g., 800–4000 IU per day) can reduce BP in patients diagnosed with some types of HTN, most notably HTN secondary to VDD. Long-term VD supplementation (five years) may also reduce the risk of developing HTN in VD-deficient susceptible populations. Our ongoing studies focused on the molecular and cellular links between VDD and HTN will support the development of etiology-specific therapeutics for and prevention of HTN in this critical patient subgroup.
References
The articles published recently with particular interests, have been highlighted as: • Of importance •• Of major importance
Adams JM, Wright JS. A National Commitment to Improve the Care of Patients With Hypertension in the US. JAMA. 2020;324(18):1825–6. https://doi.org/10.1001/jama.2020.20356.
Ferdinand KC, Nasser SA. Management of Essential Hypertension. Cardiol Clin. 2017;35(2):231–46. https://doi.org/10.1016/j.ccl.2016.12.005.
Egan BM, Zhao Y, Axon RN, Brzezinski WA, Ferdinand KC. Uncontrolled and apparent treatment resistant hypertension in the United States, 1988 to 2008. Circulation. 2011;124(9):1046–58. https://doi.org/10.1161/CIRCULATIONAHA.111.030189.
•• Muntner P, Hardy ST, Fine LJ, Jaeger BC, Wozniak G, Levitan EB, et al. Trends in Blood Pressure Control Among US Adults With Hypertension, 1999–2000 to 2017–2018. JAMA. 2020;324(12):1190–200. https://doi.org/10.1001/jama.2020.14545. This study shows the HTN control trends among US adult patients recently.
Chen S. Essential hypertension: perspectives and future directions. J Hypertens. 2012;30(1):42–5. https://doi.org/10.1097/HJH.0b013e32834ee23c.
Mogire RM, Mutua A, Kimita W, Kamau A, Bejon P, Pettifor JM, et al. Prevalence of vitamin D deficiency in Africa: a systematic review and meta-analysis. Lancet Glob Health. 2020;8(1):e134–42. https://doi.org/10.1016/S2214-109X(19)30457-7.
Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53–8. https://doi.org/10.1210/jc.2010-2704.
Chen S, Sun Y, Agrawal DK. Vitamin D deficiency and essential hypertension. J Am Soc Hypertens. 2015;9(11):885–901. https://doi.org/10.1016/j.jash.2015.08.009.
Chen S. Effect of Vitamin D on the Treatment and Prevention of Essential Hypertension. Drug Designing: Open Access. 2017. https://doi.org/10.4172/2169-0138.1000147.
Heaney RP. Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutr Rev. 2014;72(1):48–54. https://doi.org/10.1111/nure.12090.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):1269–324. https://doi.org/10.1161/HYP.0000000000000066.
Bakris G, Sorrentino M. Redefining Hypertension - Assessing the New Blood-Pressure Guidelines. N Engl J Med. 2018;378(6):497–9. https://doi.org/10.1056/NEJMp1716193.
Krause R, Buhring M, Hopfenmuller W, Holick MF, Sharma AM. Ultraviolet B and blood pressure. Lancet. 1998;352(9129):709–10. https://doi.org/10.1016/S0140-6736(05)60827-6.
Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest. 2002;110(2):229–38. https://doi.org/10.1172/JCI15219.
•• Giustina A, Adler RA, Binkley N, Bollerslev J, Bouillon R, Dawson-Hughes B, et al. Consensus statement from 2(nd) International Conference on Controversies in Vitamin D. Rev Endocr Metab Disord. 2020;21(1):89–116. https://doi.org/10.1007/s11154-019-09532-w. A statement from the second VD International Conference emphasizes that low or high doses of VD may be inefficient because a U-shape relationship exists between VD doses and its outcomes, and that a non-intermittent regimen is important for a successful intervention.
•• Giustina A, Bouillon R, Binkley N, Sempos C, Adler RA, Bollerslev J, et al. Controversies in Vitamin D: A Statement From the Third International Conference. JBMR Plus. 2020;4(12):e10417. https://doi.org/10.1002/jbm4.10417. A statement from the Third VD International Conference highlights that the conclusion that VD has no effect on cardiovascular system and cancer from recent large RCTs is not evidence-based to claim because the trials did not target the populations who were VD-deficient.
Gepner AD, Haller IV, Krueger DC, Korcarz CE, Binkley N, Stein JH. A randomized controlled trial of the effects of vitamin D supplementation on arterial stiffness and aortic blood pressure in Native American women. Atherosclerosis. 2015;240(2):526–8. https://doi.org/10.1016/j.atherosclerosis.2015.04.795.
Jorde R, Sneve M, Torjesen P, Figenschau Y. No improvement in cardiovascular risk factors in overweight and obese subjects after supplementation with vitamin D3 for 1 year. J Intern Med. 2010;267(5):462–72. https://doi.org/10.1111/j.1365-2796.2009.02181.x.
Kunutsor SK, Burgess S, Munroe PB, Khan H. Vitamin D and high blood pressure: causal association or epiphenomenon? Eur J Epidemiol. 2014;29(1):1–14. https://doi.org/10.1007/s10654-013-9874-z.
Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, Mora S, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380(1):33–44. https://doi.org/10.1056/NEJMoa1809944.
Arora P, Song Y, Dusek J, Plotnikoff G, Sabatine MS, Cheng S, et al. Vitamin D therapy in individuals with prehypertension or hypertension: the DAYLIGHT trial. Circulation. 2015;131(3):254–62. https://doi.org/10.1161/CIRCULATIONAHA.114.011732.
Bressendorff I, Brandi L, Schou M, Nygaard B, Frandsen NE, Rasmussen K, et al. The Effect of High Dose Cholecalciferol on Arterial Stiffness and Peripheral and Central Blood Pressure in Healthy Humans: A Randomized Controlled Trial. PLoS ONE. 2016;11(8):e0160905. https://doi.org/10.1371/journal.pone.0160905.
Nagpal J, Pande JN, Bhartia A. A double-blind, randomized, placebo-controlled trial of the short-term effect of vitamin D3 supplementation on insulin sensitivity in apparently healthy, middle-aged, centrally obese men. Diabet Med. 2009;26(1):19–27. https://doi.org/10.1111/j.1464-5491.2008.02636.x.
Schleithoff SS, Zittermann A, Tenderich G, Berthold HK, Stehle P, Koerfer R. Vitamin D supplementation improves cytokine profiles in patients with congestive heart failure: a double-blind, randomized, placebo-controlled trial. Am J Clin Nutr. 2006;83(4):754–9. https://doi.org/10.1093/ajcn/83.4.754.
Scragg R, Wishart J, Stewart A, Ofanoa M, Kerse N, Dyall L, et al. No effect of ultraviolet radiation on blood pressure and other cardiovascular risk factors. J Hypertens. 2011;29(9):1749–56. https://doi.org/10.1097/HJH.0b013e328349666d.
Seibert E, Lehmann U, Riedel A, Ulrich C, Hirche F, Brandsch C, et al. Vitamin D3 supplementation does not modify cardiovascular risk profile of adults with inadequate vitamin D status. Eur J Nutr. 2017;56(2):621–34. https://doi.org/10.1007/s00394-015-1106-8.
Zittermann A, Frisch S, Berthold HK, Gotting C, Kuhn J, Kleesiek K, et al. Vitamin D supplementation enhances the beneficial effects of weight loss on cardiovascular disease risk markers. Am J Clin Nutr. 2009;89(5):1321–7. https://doi.org/10.3945/ajcn.2008.27004.
• Abderhalden LA, Meyer S, Dawson-Hughes B, Orav EJ, Meyer U, de Godoi Rezende Costa Molino C, et al. Effect of daily 2000 IU versus 800 IU vitamin D on blood pressure among adults age 60 years and older: a randomized clinical trial. Am J Clin Nutr. 2020;112(3):527–37. https://doi.org/10.1093/ajcn/nqaa145. The results from this uncontrolled clinical trial suggest that VD supplementation at 800 IU per day for two years may reduce mean SBP in a VD-deficient cohort of patients ≥60 years of age.
Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957–67. https://doi.org/10.1016/S0140-6736(15)01225-8.
Bischoff-Ferrari HA, Vellas B, Rizzoli R, Kressig RW, da Silva JAP, Blauth M, et al. Effect of Vitamin D Supplementation, Omega-3 Fatty Acid Supplementation, or a Strength-Training Exercise Program on Clinical Outcomes in Older Adults: The DO-HEALTH Randomized Clinical Trial. JAMA. 2020;324(18):1855–68. https://doi.org/10.1001/jama.2020.16909.
Bischoff-Ferrari HA, de Godoi Rezende Costa Molino C, Rival S, Vellas B, Rizzoli R, Kressig RW, et al. DO-HEALTH: Vitamin D3 - Omega-3 - Home exercise - Healthy aging and longevity trial - Design of a multinational clinical trial on healthy aging among European seniors. Contemp Clin Trials. 2021;100:106124. https://doi.org/10.1016/j.cct.2020.106124.
Tiosano D, Schwartz Y, Braver Y, Hadash A, Gepstein V, Weisman Y, et al. The renin-angiotensin system, blood pressure, and heart structure in patients with hereditary vitamin D-resistance rickets (HVDRR). J Bone Miner Res. 2011;26(9):2252–60. https://doi.org/10.1002/jbmr.431.
Larsen T, Mose FH, Bech JN, Hansen AB, Pedersen EB. Effect of cholecalciferol supplementation during winter months in patients with hypertension: a randomized, placebo-controlled trial. Am J Hypertens. 2012;25(11):1215–22. https://doi.org/10.1038/ajh.2012.111.
Borges AC, Feres T, Vianna LM, Paiva TB. Effect of cholecalciferol treatment on the relaxant responses of spontaneously hypertensive rat arteries to acetylcholine. Hypertension. 1999;34(4 Pt 2):897–901.
Wong MS, Delansorne R, Man RY, Svenningsen P, Vanhoutte PM. Chronic treatment with vitamin D lowers arterial blood pressure and reduces endothelium-dependent contractions in the aorta of the spontaneously hypertensive rat. Am J Physiol Heart Circ Physiol. 2010;299(4):H1226–34. https://doi.org/10.1152/ajpheart.00288.2010.
Chen S, Gardner DG. Liganded vitamin D receptor displays anti-hypertrophic activity in the murine heart. J Steroid Biochem Mol Biol. 2013;136:150–5. https://doi.org/10.1016/j.jsbmb.2012.09.007.
Thierry-Palmer M, Cephas S, Muttardy FF, Al-Mahmoud A. High dietary cholecalciferol increases plasma 25-hydroxycholecalciferol concentration, but does not attenuate the hypertension of Dahl salt-sensitive rats fed a high salt diet. J Steroid Biochem Mol Biol. 2008;111(1–2):7–12. https://doi.org/10.1016/j.jsbmb.2008.04.002.
Bernini G, Carrara D, Bacca A, Carli V, Virdis A, Rugani I, et al. Effect of acute and chronic vitamin D administration on systemic renin angiotensin system in essential hypertensives and controls. J Endocrinol Invest. 2013;36(4):216–20. https://doi.org/10.1007/BF03347275.
Bricio-Barrios JAR, Palacios-Fonseca AJM, Del Toro-Equihua MP, Sanchez-Ramirez CAP. Effect of calcitriol supplementation on blood pressure in older adults. J Nutr Gerontol Geriatr. 2016;35(4):243–52. https://doi.org/10.1080/21551197.2016.1206499.
Chen WR, Liu ZY, Shi Y, Yin DW, Wang H, Sha Y, et al. Vitamin D and nifedipine in the treatment of Chinese patients with grades I-II essential hypertension: a randomized placebo-controlled trial. Atherosclerosis. 2014;235(1):102–9. https://doi.org/10.1016/j.atherosclerosis.2014.04.011.
de Zeeuw D, Agarwal R, Amdahl M, Audhya P, Coyne D, Garimella T, et al. Selective vitamin D receptor activation with paricalcitol for reduction of albuminuria in patients with type 2 diabetes (VITAL study): a randomised controlled trial. Lancet. 2010;376(9752):1543–51. https://doi.org/10.1016/S0140-6736(10)61032-X.
Forman JP, Scott JB, Ng K, Drake BF, Suarez EG, Hayden DL, et al. Effect of vitamin D supplementation on blood pressure in blacks. Hypertension. 2013;61(4):779–85. https://doi.org/10.1161/HYPERTENSIONAHA.111.00659.
Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C. Effects of a short-term vitamin D(3) and calcium supplementation on blood pressure and parathyroid hormone levels in elderly women. J Clin Endocrinol Metab. 2001;86(4):1633–7. https://doi.org/10.1210/jcem.86.4.7393.
Qasemi R, Ghavamzadeh S, Faghfouri AH, Valizadeh N, Mohammadi A, Sayyadi H. The effect of vitamin D supplementation on flow-mediated dilatation, oxidized LDL and intracellular adhesion molecule 1 on type 2 diabetic patients with hypertension: A randomized, placebo-controlled, double-blind trial. Diabetes Metab Syndr. 2021;15(4):102200. https://doi.org/10.1016/j.dsx.2021.102200.
Lind L, Lithell H, Skarfors E, Wide L, Ljunghall S. Reduction of blood pressure by treatment with alphacalcidol. A double-blind, placebo-controlled study in subjects with impaired glucose tolerance. Acta Med Scand. 1988;223(3):211–7.
Lind L, Wengle B, Wide L, Sorensen OH, Ljunghall S. Hypertension in primary hyperparathyroidism–reduction of blood pressure by long-term treatment with vitamin D (alphacalcidol). A double-blind, placebo-controlled study. Am J Hypertens. 1988;1(4 Pt 1):397–402. https://doi.org/10.1093/ajh/1.4.397.
Panahi Y, Namazi S, Rostami-Yalmeh J, Sahebi E, Khalili N, Jamialahmadi T, et al. Effect of Vitamin D Supplementation on the Regulation of Blood Pressure in Iranian Patients with Essential Hypertension: A Clinical Trial. Adv Exp Med Biol. 2021;1328:501–11. https://doi.org/10.1007/978-3-030-73234-9_35.
Sheikh V, Mozaianimonfared A, Gharakhani M, Poorolajal J, Ph D. Effect of vitamin D supplementation versus placebo on essential hypertension in patients with vitamin D deficiency: a double-blind randomized clinical trial. J Clin Hypertens (Greenwich). 2020;22(10):1867–73. https://doi.org/10.1111/jch.13926.
Scragg R, Khaw KT, Murphy S. Effect of winter oral vitamin D3 supplementation on cardiovascular risk factors in elderly adults. Eur J Clin Nutr. 1995;49(9):640–6.
Strobel F, Reusch J, Penna-Martinez M, Ramos-Lopez E, Klahold E, Klepzig C, et al. Effect of a randomised controlled vitamin D trial on insulin resistance and glucose metabolism in patients with type 2 diabetes mellitus. Horm Metab Res. 2014;46(1):54–8. https://doi.org/10.1055/s-0033-1358453.
Witham MD, Crighton LJ, Gillespie ND, Struthers AD, McMurdo ME. The effects of vitamin D supplementation on physical function and quality of life in older patients with heart failure: a randomized controlled trial. Circ Heart Fail. 2010;3(2):195–201. https://doi.org/10.1161/CIRCHEARTFAILURE.109.907899.
Witham MD, Dove FJ, Khan F, Lang CC, Belch JJ, Struthers AD. Effects of vitamin D supplementation on markers of vascular function after myocardial infarction–a randomised controlled trial. Int J Cardiol. 2013;167(3):745–9. https://doi.org/10.1016/j.ijcard.2012.03.054.
Witham MD, Ireland S, Houston JG, Gandy SJ, Waugh S, Macdonald TM, et al. Vitamin D therapy to reduce blood pressure and left ventricular hypertrophy in resistant hypertension: randomized, controlled trial. Hypertension. 2014;63(4):706–12. https://doi.org/10.1161/HYPERTENSIONAHA.113.02177.
Heaney RP, Armas LA, Shary JR, Bell NH, Binkley N, Hollis BW. 25-Hydroxylation of vitamin D3: relation to circulating vitamin D3 under various input conditions. Am J Clin Nutr. 2008;87(6):1738–42. https://doi.org/10.1093/ajcn/87.6.1738.
Hollis BW, Wagner CL. Clinical review: The role of the parent compound vitamin D with respect to metabolism and function: Why clinical dose intervals can affect clinical outcomes. J Clin Endocrinol Metab. 2013;98(12):4619–28. https://doi.org/10.1210/jc.2013-2653.
Jorde R, Grimnes G. Serum cholecalciferol may be a better marker of vitamin D status than 25-hydroxyvitamin D. Med Hypotheses. 2018;111:61–5. https://doi.org/10.1016/j.mehy.2017.12.017.
Bischoff-Ferrari HA, Willett WC, Orav EJ, Lips P, Meunier PJ, Lyons RA, et al. A pooled analysis of vitamin D dose requirements for fracture prevention. N Engl J Med. 2012;367(1):40–9. https://doi.org/10.1056/NEJMoa1109617.
Bischoff-Ferrari HA, Dawson-Hughes B, Orav EJ, Staehelin HB, Meyer OW, Theiler R, et al. Monthly high-dose vitamin D treatment for the prevention of functional decline: a randomized clinical trial. JAMA Intern Med. 2016;176(2):175–83. https://doi.org/10.1001/jamainternmed.2015.7148.
Ginde AA, Blatchford P, Breese K, Zarrabi L, Linnebur SA, Wallace JI, et al. High-dose monthly vitamin D for prevention of acute respiratory infection in older long-term care rsidents: a randomized clinical trial. J Am Geriatr Soc. 2017;65(3):496–503. https://doi.org/10.1111/jgs.14679.
Khaw KT, Stewart AW, Waayer D, Lawes CMM, Toop L, Camargo CA Jr, et al. Effect of monthly high-dose vitamin D supplementation on falls and non-vertebral fractures: secondary and post-hoc outcomes from the randomised, double-blind, placebo-controlled ViDA trial. Lancet Diabetes Endocrinol. 2017;5(6):438–47. https://doi.org/10.1016/S2213-8587(17)30103-1.
Sanders KM, Stuart AL, Williamson EJ, Simpson JA, Kotowicz MA, Young D, et al. Annual high-dose oral vitamin D and falls and fractures in older women: a randomized controlled trial. JAMA. 2010;303(18):1815–22. https://doi.org/10.1001/jama.2010.594.
Smith H, Anderson F, Raphael H, Maslin P, Crozier S, Cooper C. Effect of annual intramuscular vitamin D on fracture risk in elderly men and women–a population-based, randomized, double-blind, placebo-controlled trial. Rheumatology (Oxford). 2007;46(12):1852–7. https://doi.org/10.1093/rheumatology/kem240.
Sugden JA, Davies JI, Witham MD, Morris AD, Struthers AD. Vitamin D improves endothelial function in patients with Type 2 diabetes mellitus and low vitamin D levels. Diabet Med. 2008;25(3):320–5. https://doi.org/10.1111/j.1464-5491.2007.02360.x.
Witham MD, Dove FJ, Dryburgh M, Sugden JA, Morris AD, Struthers AD. The effect of different doses of vitamin D(3) on markers of vascular health in patients with type 2 diabetes: a randomised controlled trial. Diabetologia. 2010;53(10):2112–9. https://doi.org/10.1007/s00125-010-1838-1.
Reiss AB, Martin KO, Rojer DE, Iyer S, Grossi EA, Galloway AC, et al. Sterol 27-hydroxylase: expression in human arterial endothelium. J Lipid Res. 1997;38(6):1254–60.
Theodoropoulos C, Demers C, Petit JL, Gascon-Barre M. High sensitivity of rat hepatic vitamin D3–25 hydroxylase CYP27A to 1,25-dihydroxyvitamin D3 administration. Am J Physiol Endocrinol Metab. 2003;284(1):E138–47. https://doi.org/10.1152/ajpendo.00303.2002.
Somjen D, Weisman Y, Kohen F, Gayer B, Limor R, Sharon O, et al. 25-hydroxyvitamin D3–1alpha-hydroxylase is expressed in human vascular smooth muscle cells and is upregulated by parathyroid hormone and estrogenic compounds. Circulation. 2005;111(13):1666–71. https://doi.org/10.1161/01.CIR.0000160353.27927.70.
Zehnder D, Bland R, Chana RS, Wheeler DC, Howie AJ, Williams MC, et al. Synthesis of 1,25-dihydroxyvitamin D(3) by human endothelial cells is regulated by inflammatory cytokines: a novel autocrine determinant of vascular cell adhesion. J Am Soc Nephrol. 2002;13(3):621–9. https://doi.org/10.1681/ASN.V133621.
Wang J, Zhou JJ, Robertson GR, Lee VW. Vitamin D in vascular calcification: a double-edged sword? Nutrients. 2018. https://doi.org/10.3390/nu10050652.
Meekins ME, Oberhelman SS, Lee BR, Gardner BM, Cha SS, Singh RJ, et al. Pharmacokinetics of daily versus monthly vitamin D3 supplementation in non-lactating women. Eur J Clin Nutr. 2014;68(5):632–4. https://doi.org/10.1038/ejcn.2013.278.
Oberhelman SS, Meekins ME, Fischer PR, Lee BR, Singh RJ, Cha SS, et al. Maternal vitamin D supplementation to improve the vitamin D status of breast-fed infants: a randomized controlled trial. Mayo Clin Proc. 2013;88(12):1378–87. https://doi.org/10.1016/j.mayocp.2013.09.012.
Dusso A, Brown A, Slatopolsky E. Extrarenal production of calcitriol. Semin Nephrol. 1994;14(2):144–55.
Haussler MR, Whitfield GK, Haussler CA, Hsieh JC, Thompson PD, Selznick SH, et al. The nuclear vitamin D receptor: biological and molecular regulatory properties revealed. J Bone Miner Res. 1998;13(3):325–49. https://doi.org/10.1359/jbmr.1998.13.3.325.
Zheng YT, Cui QQ, Hong YM, Yao WG. A meta-analysis of high dose, intermittent vitamin D supplementation among older adults. PLoS ONE. 2015;10(1):e0115850. https://doi.org/10.1371/journal.pone.0115850.
DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr. 2004;80(6 Suppl):1689S-S1696. https://doi.org/10.1093/ajcn/80.6.1689S.
Farapti F, Fadilla C, Yogiswara N, Adriani M. Effects of vitamin D supplementation on 25(OH)D concentrations and blood pressure in the elderly: a systematic review and meta-analysis. F1000Res. 2020;9:633. https://doi.org/10.12688/f1000research.24623.3.
He S, Hao X. The effect of vitamin D3 on blood pressure in people with vitamin D deficiency: A system review and meta-analysis. Medicine (Baltimore). 2019;98(19):e15284. https://doi.org/10.1097/MD.0000000000015284.
Dalbeni A, Scaturro G, Degan M, Minuz P, Delva P. Effects of six months of vitamin D supplementation in patients with heart failure: a randomized double-blind controlled trial. Nutr Metab Cardiovasc Dis. 2014;24(8):861–8. https://doi.org/10.1016/j.numecd.2014.02.015.
Mozaffari-Khosravi H, Loloei S, Mirjalili MR, Barzegar K. The effect of vitamin D supplementation on blood pressure in patients with elevated blood pressure and vitamin D deficiency: a randomized, double-blind, placebo-controlled trial. Blood Press Monit. 2015;20(2):83–91. https://doi.org/10.1097/MBP.0000000000000091.
Beveridge LA, Struthers AD, Khan F, Jorde R, Scragg R, Macdonald HM, et al. Effect of Vitamin D Supplementation on Blood Pressure: A Systematic Review and Meta-analysis Incorporating Individual Patient Data. JAMA Intern Med. 2015;175(5):745–54. https://doi.org/10.1001/jamainternmed.2015.0237.
Zhang D, Cheng C, Wang Y, Sun H, Yu S, Xue Y, et al. Effect of vitamin D on blood pressure and hypertension in the general population: an update meta-analysis of cohort studies and randomized controlled trials. Prev Chronic Dis. 2020;17:E03. https://doi.org/10.5888/pcd17.190307.
Lind L, Wengle B, Ljunghall S. Blood pressure is lowered by vitamin D (alphacalcidol) during long-term treatment of patients with intermittent hypercalcaemia. A double-blind, placebo-controlled study. Acta Med Scand. 1987;222(5):423–7.
Breslavsky A, Frand J, Matas Z, Boaz M, Barnea Z, Shargorodsky M. Effect of high doses of vitamin D on arterial properties, adiponectin, leptin and glucose homeostasis in type 2 diabetic patients. Clin Nutr. 2013;32(6):970–5. https://doi.org/10.1016/j.clnu.2013.01.020.
Muldowney S, Lucey AJ, Hill TR, Seamans KM, Taylor N, Wallace JM, et al. Incremental cholecalciferol supplementation up to 15 mug/d throughout winter at 51–55 degrees N has no effect on biomarkers of cardiovascular risk in healthy young and older adults. J Nutr. 2012;142(8):1519–25. https://doi.org/10.3945/jn.111.154005.
Witham MD, Nadir MA, Struthers AD. Effect of vitamin D on blood pressure: a systematic review and meta-analysis. J Hypertens. 2009;27(10):1948–54. https://doi.org/10.1097/HJH.0b013e32832f075b.
Acknowledgements
We are grateful for the support of The Bakar Foundation and The Leone-Perkins Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interests
The authors declare no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Nutrition and Hypertension
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, S., Gemelga, G. & Yeghiazarians, Y. Is Vitamin D Supplementation an Effective Treatment for Hypertension?. Curr Hypertens Rep 24, 445–453 (2022). https://doi.org/10.1007/s11906-022-01204-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11906-022-01204-6