
Abstract
To compare circular stapler (CS) with linear stapler (LS) in a meta-analysis concerning operative time, anastomotic leaks, wound infections, strictures, and length of stay. Pubmed, Medline, and Scopus were searched for articles published since 2006. Four hundred and five articles were assessed, and 13 articles of which only one was a randomized controlled trial were included in all 49,331 patients from different regions of the world. The pooled analysis shows that operative time was shorter in LS than in CS (weighted mean difference 36.2 min; 95% CI 34.7–37.6.; p < 0.0001). No difference was seen concerning leaks or strictures. The relative risk (RR) of leakage after LS was 80% of the risk after CS; however, the 95% confidence interval (CI) showed overlap (0.58–1.11). The RR of anastomotic stricture after LS was 74% of the risk after CS; however, 95% CI (0.52–1.05) showed overlap. Wound infections were less common after LS than after CS; RR was 27% (95% CI 0.21–0.33). Length of stay (LOS) was 0.65 days shorter after LS than after CS (95% CI 0.51–0.78). LS compared with CS results in shorter operative time, less wound infections, and shorter length of stay, but no difference was seen concerning risks of leaks or strictures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Sleeve gastrectomy has gained popularity in the recent years and is now the most common bariatric procedure, making laparoscopic Roux-en-Y gastric bypass (LRYGB) the second most common bariatric procedure [1]. When performing LRYGB, a pouch is created from the cardia region of the stomach and joined with the jejunum through a gastro-jejunostomy. The gastro-jejunostomy may be performed using a stapler (circular or linear) or entirely hand-sewn. When the gastro-jejunostomy is done using circular stapler, the anastomosis is complete immediately after the stapler has been fired. When a linear stapler is used, the remaining defect is closed with a running suture after the stapler has been fired; this can be swiftly and safely done with a barbed suture [2]. Opinions on which of these mechanical techniques is superior differ. In some European countries such as Germany and Sweden, using a linear stapler (LS) is the most common method [3, 4], while applying a circular stapler (CS) is a more common method in the USA [5]. A meta-analysis comparing circular and linear stapler was published in 2011 involving 1300 patients; linear stapler was associated to shorter operative time, fewer strictures, and fewer postoperative superficial infections [6]. Since then, several large studies have been published providing the incentive to perform a new meta-analysis comparing circular to linear stapler with regard to outcomes [3, 4]. This study compares CS with LS; hand-sewn gastro-jejunostomies are omitted because of the infrequency [3]. Since bariatric surgery has increased in the recent years, also a small difference in outcomes between techniques would have a large impact on the bariatric population [1].
The outcomes studied were operative time, anastomotic leaks, wound infections, strictures, and length of stay.
Method
In Pubmed, a search was performed using the search term “linear,” “circular,” and “stapling technique” with the Boolean “OR” function. The set was then combined with the search term “gastric bypass” and further narrowed down limiting the result to English articles. Since staplers have undergone considerable improvement in the last decade, studies published before 2006 were excluded.
In all, 405 abstracts were assessed.
All articles were assessed in a structured manner by the author but without a formalized protocol and non-comparative studies; non-published studies and non-English studies were excluded. PRISMA statement for reporting meta-analysis [7] was followed. The references of the articles were scanned, and additional studies suitable for analysis were added. After the full-text articles were retrieved, data was extracted for the outcomes previously noted. Thirteen articles were included in one or more of the outcome analyses.
Statistics
Heterogeneity was assessed by using I2 statistic. Publication bias was assessed through funnel plot. Data was analyzed using Stata® version 14.1 (Statacorp LP, TX, USA). A p < 0.05 was considered statistically significant. A fixed-effects model with inverse variance method was used for summary–effect calculation.
Results
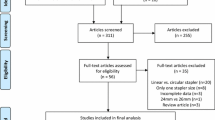
The literature search yielded 405 articles; 392 articles were excluded because they were not comparative between LS and CS, non-published, or not written in english. The flow chart for the study selection is shown in Fig. 1. In all, 13 articles were included (one RCT, three prospective cohorts, and nine retrospective cohorts; Table 1 [3,4,5, 8,9,10,11,12,13,14,15,16,17]). The studies included were found to be from Europe, North America, South America, and Middle East. In total, 49,331 patients were included, of which 40,281 underwent surgery with LS and 9050 with CS; the majority of patients were included from one cohort study with mostly LS patients [4].

Flow chart of literature search and extraction of relevant studies
Operative time was included in nine of the studies (Fig. 2). The pooled analysis showed that operative time was shorter in LS than in CS (weighted mean difference 36 min; 95% CI 35–36; p < 0.0001). In all but one of included studies [17], the mean operative time was shorter in LS than in CS. The mean operative time in the studies ranged from 73 to 156 min for LS and from 114 to 169 min for CS.

Data on operative time were reported in nine studies, favoring linear stapler by 36 min
No difference was seen concerning leaks; data on leaks was included in 12 of the studies (Fig. 3). The relative risk of leakage after LS was 80% of the risk after CS; however, the 95% CI showed overlap (0.58–1.11); thus, no significant difference in leak rate was found.

Data on leaks were reported in 12 studies; no significant different was seen between stapler techniques
Eight of the studies included data on wound infections (Fig. 4). In all studies except one, wound infections were more common after CS than after LS. The relative risk of wound infections after LS was 27% of the risk after CS 95% CI (0.21–0.34).

Data on wound infections were reported in 11 studies, favoring linear stapler realtive risk 0.27 (95% CI 0.21–0.33)
Strictures were reported in 11 of the studies (Fig. 5). The relative risk of anastomotic stricture after LS was 74% of the risk after CS; however, 95% CI (0.52–1.05) showed overlap; thus, no significant difference in the risk of stricture was found.

Data on anastomotic stricture was noted in 11 of included studies, showing no significant advantage for either technique
LOS was reported in eight of the included studies (Fig. 6). LOS was 0.65 days shorter after LS than after CS (95% CI 0.51–0.78); thus, LOS was significantly shorter for LS patients than for CS patients. Funnel plots were performed for all the studied outcomes and did not indicate publication bias.

Data on length of stay was noted in eight of included studies, favoring linear stapler by 0.65 days (95% CI 0.51–0.78 days)
Discussion
This study represents the largest meta-analysis to date comparing LS with CS for creating the gastro-jejunostomy, favoring LS concerning operative time, wound infections, and LOS but with no difference concerning leaks and strictures.
Operative time could be considered of secondary interest when choosing operative technique. However, operative time is of interest as surgeons with long operative time has been linked to increased risks of postoperative complications [18]. It is possible that a long operative time increases the risk for example pulmonary embolus and may also be a proxy for perioperative difficulties. In all studies, but one, the operative time was shorter with LS than with CS; consequently, the findings were consistent and the results are likely to be reproducible. There are several explanations why LS requires less operative time. First, introducing the circular stapler into the abdomen may be time consuming. The CS device is wider than a port so the porthole needs to be dilated before allowing the CS to pass through. Second, inserting the CS into the bowel may be challenging as the small bowel may also require dilating before allowing the stapler to enter. Third, when removing the stapler, many surgeons choose to close the dilated opening in the fascia with stitches which adds to operative time. In addition, the dilated port hole may result in leakage of insufflated carbon dioxide during the remainder of the procedure. These factors affect operative time to such a degree that although LS requires the remaining defect in the anastomosis after stapling to be closed manually, LS still requires less time. Major et al. estimated the costs of LS to be 20% lower than the cost of CS [17]. In addition, the shorter operative time makes LS considerably more economical.
Leak is the most feared complication after LRYGB. Leaks may require reoperation, treatment in an intensive care unit, and patients may die as a result of a leak. More than 49,000 patients were analyzed (40,281 LS and 9050 CS patients) in this meta-analysis, yet no difference was shown regarding the primary outcome leakage. In spite of the two techniques being distinct in how the anastomosis is formed, there is no difference in the leak rates. This raises many questions, if the techniques have similar outcomes yet are so different, what does this imply concerning the etiology of leaks? Patient specific factors such as age may be more important than which technique is used to create the anastomosis [19] as long as certain basic aspects of surgery is respected such as adequate stitches, knots, and blood circulation to involved tissue.
Increased risk of wound infections have been linked to CS [6]. In all but one of the studies included, the risk of wound infections was increased in CS compared to LS. After firing the stapler, the stapler is retracted through the abdominal wall and the circular rings from the gastric pouch and the jejunum may be inspected. Retrieving contaminated tissue and stapler through the abdominal wall is believed to increase the risk of wound infections. This risk can be reduced by using a plastic sheath to protect the subcutaneous tissue from the contaminated stapler [20]. In none of the included studies has the use of the protective sheath been documented, though it is possible that some of the cohort studies included patients in which the protective sheath was used. Inserting the anvil the transoral route as described by Wittgrove et al. is a common route [21] and Medtronic Orvil® which is an anvil fixed to a nasogastric tube could be used to facilitate this [22]. Another possibility is to first insert the anvil of the stapler through the abdominal wall and then into an opening in gastric pouch. A tobacco pouch suture may then be applied to pull the edges of the gastric pouch snug to the anvil. This technique might cause fewer wound infections since the anvil is not contaminated by being pulled through the mouth and esophagus. Choice and dosage of perioperative antibiotics may also have affected the risk of developing wound infections; however, regimens for antibiotics were generally not stated in the included studies.
Strictures may be underreported as a study by Csendes et al. found strictures to be present in 29% of asymptomatic patients [23]. It could also be argued that the definition of stricture is too broad if patients are given the diagnosis in spite of not having any symptoms. However, it is important that the same follow-up and defintion is used for CS and LS patients for the data on strictures to remain valid. It is established that CS with a diameter of 21 mm is associated to an increased risk of developing anastomotic strictures compared to CS with 25 mm diameter [24]. Only three of the studies included patients in which 21 mm CS had been used. This should be taken into account when interpreting the results concerning anastomotic strictures. In addition, the two larger cohorts included lacked data on strictures [4, 5].
Length of stay was shorter in CS than in LS. The dilatation of the abdominal wall needed to introduce the circular stapler may cause postoperative pain, and in addition, the higher incidence of wound infections could contribute to the prolonged length of stay. In seven of eight studies which included data on length of stay had longer length of stay for CS patients than for LS patients. This implies that the difference is related to the stapler and not related to different postoperative management between centers.
Strengths of the current analysis are that these studies are from different regions and the differences are likely attributed to stapler method rather than an individual surgeon’s proficiency in using a particular method. The funnel plot showed little asymmetry implying that publication bias is not influencing the results of the study (see Supplementary data).
Limitations are the following, 12 of the studies were comparative studies and only one was a randomized controlled trial, with 40 patients in each arm from 2008 [16]. In addition, staplers are high-tech products undergoing continuous development and the staplers used in the earlier cohorts may be less reliable than the staplers used in the more recent studies. Nevertheless, the comparison is unbiased as in each cohort, LS is compared to contemporary CS staplers. CS are now available with three rows of staplers which have been the norms for LS for some time.
Conclusion
LS is associated to shorter operative time, fewer wound infections, and shorter length of stay. No difference was found regarding leaks or strictures.
References
Angrisani L, Santonicola A, Iovino P, et al. IFSO Worldwide Survey 2016: primary, endoluminal, and revisional procedures. Obes Surg. 2018;28(12):3783–94.
Vidarsson B, Sundbom M, Edholm D. Shorter overall operative time when barbed suture is used in primary laparoscopic gastric bypass: a cohort study of 25,006 cases. Surg Obes Relat Dis. 2017;13(9):1484–8.
Stroh C, Nesterov G, Weiner R, et al. Circular versus linear versus hand-sewn gastrojejunostomy in Roux-en-Y-gastric bypass: data analysis from a quality assurance study of the surgical treatment of obesity in Germany. Surg Sci. 2014;2014(5):280–9.
Edholm D, Sundbom M. Comparison between circular-and linear-stapled gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass—a cohort from the Scandinavian Obesity Registry. Surg Obes Relat Dis. 2015;11(6):1233–6.
Finks JF, Carlin A, Share D, et al. Effect of surgical techniques on clinical outcomes after laparoscopic gastric bypass—results from the Michigan Bariatric Surgery Collaborative. Surg Obes Relat Dis. 2011;7(3):284–9.
Giordano S, Salminen P, Biancari F, et al. Linear stapler technique may be safer than circular in gastrojejunal anastomosis for laparoscopic Roux-en-Y gastric bypass: a meta-analysis of comparative studies. Obes Surg. 2011;21(12):1958–64.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
Bohdjalian A, Langer FB, Kranner A, et al. Circular- vs. linear-stapled gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2010;20(4):440–6.
Giordano S, Tolonen P, Victorzon M. Comparison of linear versus circular stapling techniques in laparoscopic gastric bypass surgery—a pilot study. Scand J Surg. 2010;99(3):127–31.
Bendewald FP, Choi JN, Blythe LS, et al. Comparison of hand-sewn, linear-stapled, and circular-stapled gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2011;21(11):1671–5.
Qureshi A, Podolsky D, Cumella L, et al. Comparison of stricture rates using three different gastrojejunostomy anastomotic techniques in laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2015;29(7):1737–40.
Schneider R, Gass J-M, Kern B, et al. Linear compared to circular stapler anastomosis in laparoscopic Roux-en-Y gastric bypass leads to comparable weight loss with fewer complications: a matched pair study. Langenbeck’s Arch Surg. 2016;401(3):307–13.
Vines L, Frick T, Aczél S, et al. Linear stapled gastrojejunostomy results in fewer strictures compared to circular stapled gastrojejunostomy in laparoscopic gastric bypass surgery. Langenbeck’s Arch Surg. 2017;402(6):911–6.
Khalayleh H, Pines G, Imam A, et al. Anastomotic stricture rates following Roux-en-Y gastric bypass for morbid obesity: a comparison between linear and circular-stapled anastomosis. J Laparoendosc Adv Surg Tech A. 2018;28(6):5.
Lee S, Davies AR, Bahal S, et al. Comparison of gastrojejunal anastomosis techniques in laparoscopic Roux-en-Y gastric bypass: gastrojejunal stricture rate and effect on subsequent weight loss. Obes Surg. 2014;24(9):1425–9.
Leyba JL, Llopis SN, Isaac J, et al. Laparoscopic gastric bypass for morbid obesity—a randomized controlled trial comparing two gastrojejunal anastomosis techniques. JSLS. 2008;12(4):385–8.
Major P, Janik MR, Wysocki M, et al. Comparison of circular- and linear-stapled gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass: a multicenter study. Wideochir Inne Tech Maloinwazyjne. 2017;12(2):140–6.
Reames BN, Bacal D, Krell RW, et al. Influence of median surgeon operative duration on adverse outcomes in bariatric surgery. Surg Obes Relat Dis. 2015;11(1):207–13.
Stenberg E, Szabo E, Agren G, et al. Early complications after laparoscopic gastric bypass surgery: results from the Scandinavian Obesity Surgery Registry. Ann Surg. 2013;260:1040–7.
Chen J, Miller M, Ibele A, et al. Dual ring wound protector reduces circular stapler related surgical site infections in patients undergoing laparoscopic Roux-En-Y gastric bypass. Obes Surg. 2018;28(10):3352–9.
Wittgrove AC, Clark GW, Tremblay LJ. Laparoscopic gastric bypass, Roux-en-Y: preliminary report of five cases. Obes Surg. 1994;4(4):353–7.
Nguyen NT, Hinojosa MW, Smith BR, et al. Advances in circular stapling technique for gastric bypass: transoral placement of the anvil. Obes Surg. 2008;18(5):611–4.
Csendes A, Burgos AM, Burdiles P. Incidence of anastomotic strictures after gastric bypass: a prospective consecutive routine endoscopic study 1 month and 17 months after surgery in 441 patients with morbid obesity. Obes Surg. 2009;19(3):269–73.
Fisher BL, Atkinson JD, Cottam D. Incidence of gastroenterostomy stenosis in laparoscopic Roux-en-Y gastric bypass using 21-or 25-mm circular stapler: a randomized prospective blinded study. Surg Obes Relat Dis. 2007;3(2):176–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The author received funding from Swedish medical council.
Ethical Approval
For this type of study, formal consent is not required.
Informed Consent
Does not apply.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Edholm, D. Systematic Review and Meta-analysis of Circular- and Linear-Stapled Gastro-jejunostomy in Laparoscopic Roux-en-Y Gastric Bypass. OBES SURG 29, 1946–1953 (2019). https://doi.org/10.1007/s11695-019-03803-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-03803-w