
Abstract
Background
Stricture is a common complication of gastrointestinal (GI) anastomoses, associated with impaired quality of life, risk of malnutrition, and further interventions. This systematic review and meta-analysis aimed to determine the association between circular stapler diameter and anastomotic stricture rates throughout the GI tract.
Methods
A systematic literature search of EMBASE, MEDLINE and Cochrane Library was performed. The primary outcome was the rate of radiologically or endoscopically confirmed anastomotic stricture. Pooled odds ratios (OR) were calculated using random-effects models to determine the effect of circular stapler diameter on stricture rates in different regions of the GI tract.
Results
Twenty-one studies were identified: seven oesophageal, twelve gastric, and three lower GI. Smaller stapler sizes were strongly associated with higher anastomotic stricture rates throughout the GI tract. The oesophageal anastomosis studies showed; 21 versus 25 mm circular stapler: OR 4.39 ([95% CI 2.12, 9.07]; P < 0.0001); 25 versus 28/29 mm circular stapler: OR 1.71 ([95% CI 1.15, 2.53]; P < 0.008). Gastric studies showed; 21 versus 25 mm circular stapler: OR 3.12 ([95% CI 2.23, 4.36]; P < 0.00001); 25 versus 28/29 mm circular stapler: OR 7.67 ([95% CI 1.86, 31.57]; P < 0.005). Few lower GI studies were identified, though a similar trend was found: 25 versus 28/29 mm circular stapler: pooled OR 2.61 ([95% CI 0.82, 8.29]; P = 0.100).
Conclusions
The use of larger circular stapler sizes is strongly associated with reduced risk of anastomotic stricture in the upper GI tract, though data from lower GI joins are limited.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Stricture is a common late complication of anastomoses in both the upper and lower gastrointestinal (GI) tract [1,2,3]. Anastomotic stricture has been reported to occur in 1.6–40% of patients, depending on anastomotic location, surgical technique, and other patient factors [4]. Upper GI tract strictures can be associated with dysphagia, reflux, inability to tolerate diet, and secondary complications such as pulmonary aspiration. Lower GI tract strictures can be associated with abdominal pain, bloating, constipation, and frank obstruction. Strictures all along the GI tract can result in impaired quality of life, risk of malnutrition, and the need for endoscopic or surgical intervention with risk of further complications such as anastomotic rupture [3, 5, 6].
Anastomotic stricture may occur regardless of the technique used, and previous meta-analyses have compared hand-sewn anastomosis with circular or linear stapled techniques [7,8,9,10]. The use of circular staplers has a well-established role in both upper and lower GI surgery, and numerous published studies have investigated the effect of stapler diameter on subsequent anastomotic stricture rates [11,12,13,14,15]. However, only one systematic review to date has synthesised these results, which looked primarily at bariatric surgery [11].
Therefore, to guide clinical practice, the aim of this systematic review and meta-analysis was to assess the impact of circular stapler diameter on anastomotic stricture rates throughout the GI tract.
Methods
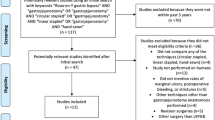
A systematic review and meta-analysis were performed in accordance with the PRISMA guidelines [16] (Fig. 1). The MEDLINE, EMBASE, and Cochrane Library databases were searched from 1980 to January 2017 using the search terms “circular stapler”, “anastomosis”, “stapler”, “size”, “millimeters”, “diameter”, “stricture”, “stenosis”, and MeSH headings “surgical stapling” (MeSH), “surgical staplers” (MeSH), “surgical anastomosis” (MeSH), “pathologic constriction” (MeSH) in combination with the Boolean operators “AND” or “OR”. Other articles were identified by hand-searching reference lists from retrieved articles. Identified titles and abstracts were then scrutinized by two independent reviewers (WA and CW) to determine eligibility for full-text review. Any discrepancies between the two reviewers were settled by discussion and consensus, with arbitration by a third reviewer (GOG) if necessary.

PRISMA flow diagram, illustrating the identification, screening and exclusion process
Studies investigating patients undergoing circular stapled GI anastomoses were included, regardless of the operation or location of the anastomosis. Both randomized and non-randomized comparative studies were included, provided at least two circular stapler diameters were compared. Studies that included patients with sutured or linear stapled anastomoses were included, provided they also compared two or more circular stapler diameters. Papers available only as conference abstracts and non-English language articles were excluded. For studies investigating more than one region of the GI tract, results for each anastomotic location were analysed separately. Both cervical and thoracic anastomoses post-oesophageal resection were included. Patients undergoing either oncological or benign resections were included. The quality of observational studies was assessed using the Newcastle–Ottawa Scale [17], while the Jadad scoring system was used for randomized trials [18]. A sensitivity analysis was performed on studies scoring 5 or below in the Newcastle–Ottawa Scale to assess for inclusion into the statistical analysis.
One reviewer (WA) extracted data points from the acquired full texts and a second reviewer (CW) confirmed these. The data points extracted were: year of study, study design, number of participants, mean/median age, male/female ratio, operation location, nature of anastomotic strictures, level of oesophageal anastomosis, follow-up period, time-to-stricture interval, stapler sizes, and stricture rates.
Statistical analysis was performed using Review Manager 5.3 (RevMan 5.3) software (Cochrane Collaboration). The primary outcome for the meta-analysis was the incidence of symptomatic GI stricture confirmed by endoscopic or radiological methods. Pooled odds ratios were calculated for different regions of the GI tract; oesophagus, gastric, and lower GI. If the oesophagus was included in any join, then it was classified as an oesophageal anastomosis. Pooled outcome measures were determined using random-effects models. A P value of <0.05 was considered statistically significant. Assessment of heterogeneity was also assessed through the I2 statistic as Cochran’s Q has shown to be poor at detecting true heterogeneity between studies [19]. Publication bias was also assessed by funnel plots in Review Manager 5.3.
Results
Twenty-one studies were included (Table 1), representing a total of 7226 patients [12, 13, 15, 20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]. Seven oesophageal, twelve gastric, and three lower GI studies were identified. One study assessed data from both gastric and oesophageal surgery [13]. Only one randomized controlled trial was identified [12], with the remainder being prospective or retrospective observational studies. Strictures were associated with both benign and malignant indications for surgery (see Table 1). The primary outcomes of stricture incidence for each study are reported in Table 2. The Newcastle–Ottawa Score of each study is shown in Supplementary Table 1, with a median score of 7 (range 4–9). Outcome reporting bias and publication bias were assessed via a funnel plot (Supplementary Fig. 1).
Oesophageal anastomosis
The seven oesophageal studies encompassed 1081 patients [13, 27, 28, 32, 35,36,37]. For the pooled oesophageal anastomosis studies, a clear increase in stricture rates was observed with the use of smaller circular stapler diameters. Stricture rates amongst oesophageal anastomosis ranged from 3 to 100% (Table 2) with a mean of 31%. The mean stricture rate for 21 mm diameter stapled anastomoses was 72% ± 24 (Standard deviation), 23% ± 16 for 25 mm diameter, and 16% ± 17 for 28/29 mm diameter. Comparing 21 to 25 mm showed a substantial increase in stricture rates (Fig. 2a; pooled odds ratio (OR) 4.39 ([95% CI: 2.12, 9.07]; P < 0.0001, I2 = 0%). Comparing 25 mm with 28/29 mm showed the same relationship with higher stricture rates being associated with smaller stapler sizes (Fig. 2b pooled OR 1.71 ([95% CI: 1.15, 2.53]; P = 0.008, I2 = 2%).

a Forest plot of oesophageal 21 versus 25 mm circular stapler stricture rates. b Forest plot of oesophageal 25 versus 28/29 mm circular stapler stricture rates
Gastric anastomosis
The twelve gastric studies encompassed 4331 patients [12, 13, 15, 20, 21, 24, 25, 29,30,31, 33, 34]. These papers similarly showed strong associations between increased stricture rates and smaller-diameter circular staplers. Stricture rates amongst gastric anastomosis ranged from 0 to 60% (Table 2) with a mean of 13%. The mean stricture rate for 21 mm diameter stapled anastomoses was 22% ± 15, 10% ± 11 for 25 mm diameter, and 1% ± 1 for 28/29 mm diameter. Comparing 21–25 mm demonstrated a substantial increase in stricture rates with the smaller stapler (Fig. 3a; pooled OR 3.12 ([95% CI: 2.23, 4.36]; P < 0.00001, I2 = 13%. A larger effect was observed when comparing the 25 mm stapler with 28/29 mm (Fig. 3b; pooled OR 7.67 ([95% CI: 1.86, 31.57]; P = 0.005, I2 = 0%).

a Forest plot of gastric 21 versus 25 mm circular stapler stricture rates. b Forest plot of gastric 25 versus 28/9 mm circular stapler stricture rates
Lower GI anastomosis
The three lower GI studies encompassed 188 patients, all from studies involving ileal pouch–anal anastomoses [22, 23, 26]. Stricture rates amongst lower GI anastomosis ranged from 9 to 60% (Table 2) with a mean of 39%. The mean stricture rate for 25 mm diameter stapled anastomoses was 51% ± 13, and 26% ± 15 for 28/29 mm diameter. The pooled comparison between 25 and 28/29 mm also showed a trend towards higher stricture rates with the smaller stapler size although this did not reach the significance threshold with the limited available data (Fig. 4; pooled OR 2.61 ([95% CI: 0.82,8.29]; P = 0.100, I2 = 50%). One paper was found that compared 28/29 with 31/33 mm (ileal pouch–anal anastomosis, 2120 patients), which showed no difference in stricture rates between the two groups (14).

Forest plot of lower GI 25 versus 28/29 mm circular stapler stricture rates
Sensitivity analysis and tests for bias
A sensitivity analysis was performed, evaluating for study quality. All results reported above for gastric and oesophageal stricture rates remained significant when studies of Newcastle–Ottawa grade 4–5 were excluded (all P < 0.01). Funnel plots were performed to assess publication bias, demonstrating no significant bias within the limited number of available studies (Supplementary Fig. 1).
Discussion
This systematic review and meta-analysis investigated the impact of circular stapler diameter on anastomotic stricture rates in the GI tract. A strong correlation was demonstrated between smaller stapler diameters and higher stricture rates, particularly in oesophageal and gastric anastomoses. A nonsignificant trend was found in lower GI anastomoses amongst the few studies identified from this region.
A previous meta-analysis of patients undergoing bariatric surgery also identified that smaller stapler diameters were associated with higher anastomotic stricture rates [11]. This study expands on those results by including seven additional gastric studies (2903 additional patients) as well as including data from all other regions of the GI tract. Only one randomized trial has compared circular stapler diameters in GI surgery [12]. In that study, Fischer et al. [12] identified anastomoses with a 21-mm stapler was associated with a doubled stricture rate compared with a 25-mm stapler in patients undergoing Roux-en-Y gastric bypass. More generally, our results also show that rates of anastomotic stricture remain clinically important [4, 5, 38,39,40,41].
Multiple other factors have been implicated in anastomotic stricture including complications (e.g. ischaemia, postoperative anastomotic leakage), anastomotic location, radiotherapy, and other patient factors. Unfortunately, we found that many of these issues are inconsistently reported in the literature, preventing a reliable estimation of their relative importance. In addition, the majority of studies investigating anastomotic stricture have been observational, and therefore the potential confounding effects of these variables could not be reliably accounted for in our meta-analysis. However, the significant association identified between stapler diameter and stricture rates in this review supports a robust direct causal relationship, which may help to guide stapler selection in surgical practice.
The findings of this meta-analysis show that although smaller stapler sizes may be chosen for ease of luminal insertion in GI surgery, the associated increased rate of anastomotic stricture risks higher overall morbidity. The occurrence of strictures is associated with impaired patient quality of life, nutritional impairment, further intervention and increased healthcare expenditure [3, 5, 6]. A judgement must be made by the surgeon as to whether a larger-diameter stapler can be safely passed through the gut lumen without trauma or tearing of tissues. Data on leak rates and stapler size were limited, and it was not possible to meta-analyse this information.
The main limitation of this review is reflected in the design of included studies. Almost all included studies were observational, and therefore the effects of potential confounding variables cannot be excluded. Most identified evidence was rated as poor to moderate according the Newcastle–Ottawa Scale, with only one randomized trial included in the analysis. Few studies from lower GI surgery were identified, with pooled data showing suggestive trends that did not reach statistical significance. Further colorectal studies are clearly required to provide firm guidance about optimal stapler sizes in this region. Furthermore, the clinical implications of this study may be limited in modern laparoscopic bariatric procedures, which frequently employ sutured anastomoses with larger anastomotic diameters than those provided by circular staplers [42]. A previous systematic review demonstrated higher stricture rates following stapled oesophageal anastomoses when compared with hand-sewn [43], and the optimal anastomotic technique for each region of the GI tract remains unclear.
In conclusion, this review has identified a strong association between circular stapler diameter and stricture rates following oesophageal and gastric anastomoses. A nonsignificant trend was found for lower GI anastomoses, though available evidence was limited. In order to reduce anastomotic stricture rates throughout the GI tract, surgeons should use the largest of the circular stapler sizes analysed in this study whenever possible, as balanced against the safety of inserting the device through the confined channel of the GI lumen. Surgeons should be encouraged to customize their circular stapler size choice to the anatomy of each patient, rather than always using a constant size in their practice. Finally, novel circular stapler designs with an elliptical angled interface warrant further investigation as such designs could theoretically increase the anastomotic surface area without making luminal stapler insertion more difficult, though would increase the technical complexity of stapler design [44, 45].
References
Briel JW, Tamhankar AP, Hagen JA, DeMeester SR, Johansson J, Choustoulakis E et al (2004) Prevalence and risk factors for ischemia, leak, and stricture of esophageal anastomosis: gastric pull-up versus colon interposition. J Am Coll Surg 198(4):536–541
Fazio VW, Ziv Y, Church JM, Oakley JR, Lavery IC, Milsom JW et al (1995) Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg 222(2):120–127
Arye B, Michael PF, Karen MP, Sayeed I, Philip RS (2002) Gastrointestinal complications of laparoscopic Roux-en-Y Gastric bypass surgery: clinical and imaging findings. Radiology 223(3):625–632
Haughn C, Calic S, Carrodeguas L, Szomstein S, Rosenthal R, Bergamaschi R (2006) Stricture rates after circular stapled versus linear stapled gastro-jejunostomy for laparoscopic gastric bypass. Eur Surg 38(6):405–410
Yimcharoen P, Heneghan H, Chand B, Talarico JA, Tariq N, Kroh M et al (2012) Successful management of gastrojejunal strictures after gastric bypass: is timing important? Surg Obes Relat Dis 8(2):151–157
Sawai RS (2012) Management of colonic obstruction: a review. Clin Colon Rectal Surg 25(4):200–203
Choy PYG, Bissett IP, Docherty JG, Parry BR, Merrie A (2011) Fitzgerald A (2003) Stapled versus handsewn methods for ileocolic anastomoses. Cochrane Database Syst Rev. 9:CD004320
Bendewald FP, Choi JN, Blythe LS, Selzer DJ, Ditslear JH, Mattar SG (2011) Comparison of hand-sewn, linear-stapled, and circular-stapled gastrojejunostomy in laparoscopic Roux-en-Y gastric bypass. Obes Surg 21(11):1671–1675
Honda M, Kuriyama A, Noma H, Nunobe S, Furukawa TA (2013) Hand-sewn versus mechanical esophagogastric anastomosis after esophagectomy: a systematic review and meta-analysis. Ann Surg 257(2):238–248
Law S, Fok M, Chu K, Wong J (1997) Comparison of hand-sewn and stapled esophagogastric anastomosis after esophageal resection for cancer: a prospective randomized controlled trial. Ann Surg 226(2):169–173
Markar S, Penna M, Venkat-Ramen V, Karthikesalingam A, Hashemi M (2012) Influence of circular stapler diameter on postoperative stenosis after laparoscopic gastrojejunal anastomosis in morbid obesity. Surg Obes Relat Dis 8(2):230–235
Fisher B, Atkinson J, Cottam D (2007) Incidence of gastroenterostomy stenosis in laparoscopic Roux-en-Y gastric bypass using 21- or 25-mm circular stapler: a randomized prospective blinded study. Surg Obes Relat Dis 3(2):176–179
Johansson J, Zilling T, von Holstein CS, Johnsson F, Oberg S, Walther B (2000) Anastomotic diameters and strictures following esophagectomy and total gastrectomy in 256 patients. World J Surg 24(1):78–84. https://doi.org/10.1007/s002689910015
Kirat HT, Kiran RP, Lian L, Remzi FH, Fazio VW (2010) Influence of stapler size used at ileal pouch-anal anastomosis on anastomotic leak, stricture, long-term functional outcomes, and quality of life. Am J Surg 200(1):68–72
Nguyen NT, Stevens CM, Wolfe BM (2003) Incidence and outcome of anastomotic stricture after laparoscopic gastric bypass. J Gastrointest Surg 7(8):997–1003
Moher D, Liberati A, Tetzlaff J, Altman DG, The PG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med 6(7):e1000097
Deeks JJ, D’Amico R, Sowden A, Sakarovitch C et al (2003) Evaluating non-randomised intervention studies. Health Technol Assess 7(27):iii–x
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ et al (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1):1–12
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560
Khoraki J, Funk LM, Greenberg JA, Leverson G, Campos GM (2016) The effect of route of anvil insertion on stricture rates with circular stapled gastrojejunostomy during laparoscopic gastric bypass. Obes Surg 26(3):517–524
Zuiki T, Hosoya Y, Kaneda Y, Kurashina K, Saito S, Ui T et al (2013) Stenosis after use of the double-stapling technique for reconstruction after laparoscopy-assisted total gastrectomy. Surg Endosc 27(10):3683–3689
Senapati A, Tibbs CJ, Ritchie JK, Nicholls RJ, Hawley PR (1996) Stenosis of the pouch anal anastomosis following restorative proctocolectomy. Int J Colorectal Dis 11(2):57–59
Kissin MW, Cox AG, Wilkins RA, Kark AE (1985) The fate of the EEA stapled anastomosis: a clinico-radiological study of 38 patients. Ann R Coll Surg Engl 67(1):20–22
Tokunaga Y, Ryo J, Kitaoka A, Yagi T, Tokuka A, Ohsumi K (1999) Jejunal pouch to avoid stricture after esophagojejunostomy with circular stapler. J Am Coll Surg 189(5):466–469
Sima E, Hedberg J, Sundbom M (2016) Gastrointestinal symptoms, weight loss and patient satisfaction 5 years after gastric bypass: a study of three techniques for the gastrojejunal anastomosis. Surg Endosc 30(4):1553–1558
Lewis WG, Kuzu A, Sagar PM, Holdsworth PJ, Johnston D (1994) Stricture at the pouch-anal anastomosis after restorative proctocolectomy. Dis Colon Rectum 37(2):120–125
Dresner SM, Lamb PJ, Wayman J, Hayes N, Griffin SM (2000) Benign anastomotic stricture following transthoracic subtotal oesophagectomy and stapled oesophago-gastrostomy: risk factors and management. Br J Surg 87(3):362–373
Cakabay B, Aksel B, Unal E, Bayar S, Kocaoglu H, Demirci S et al (2012) Influence of the stapler size used in esophagojejunostomy anastomosis: anastomotic leak and strictures after total gastrectomy. Turkiye Klinikleri J Med Sci 32(2):428–431
Smith C, Garren M, Gould J (2011) Impact of gastrojejunostomy diameter on long-term weight loss following laparoscopic gastric bypass: a follow-up study. Surg Endosc 25(7):2164–2167
Gould JC, Garren M, Boll V, Starling J (2006) The impact of circular stapler diameter on the incidence of gastrojejunostomy stenosis and weight loss following laparoscopic Roux-en-Y gastric bypass. Surg Endosc 20(7):1017–1020
Kim DH, Oh CA, Oh SJ, Choi MG, Noh JH, Sohn TS et al (2012) Circular stapler size and risk of anastomotic complications in gastroduodenostomy for gastric cancer. World J Surg 36(8):1796–1799. https://doi.org/10.1007/s00268-012-1584-2
Deldycke A, Van Daele E, Ceelen W, Van Nieuwenhove Y, Pattyn P (2016) Functional outcome after Ivor Lewis esophagectomy for cancer. J Surg Oncol 113(1):24–28
Takata MC, Ciovica R, Cello JP, Posselt AM, Rogers SJ, Campos GM (2007) Predictors, treatment, and outcomes of gastrojejunostomy stricture after gastric bypass for morbid obesity. Obes Surg 17(7):878–884
Suggs WJ, Kouli W, Lupovici M, Chau WY, Brolin RE (2007) Complications at gastrojejunostomy after laparoscopic Roux-en-Y gastric bypass: comparison between 21- and 25-mm circular staplers. Surg Obes Relat Dis. 3(5):508–514
Petrin G, Ruol A, Battaglia G, Buin F, Merigliano S, Constantini M et al (2000) Anastomotic stenoses occurring after circular stapling in esophageal cancer surgery. Surg Endosc 14(7):670–674
Berrisford RG, Page RD, Donnelly RJ (1996) Stapler design and strictures at the esophagogastric anastomosis. J Thorac Cardiovasc Surg 111(1):142–146
Yendamuri S, Gutierrez L, Oni A, Mashtare T, Khushalani N, Yang G et al (2011) Does circular stapled esophagogastric anastomotic size affect the incidence of postoperative strictures? J Surg Res 165(1):1–4
Leyba J, Llopis S, Isaac J, Aulestia S, Bravo C, Obregon F (2008) Laparoscopic gastric bypass for morbid obesity-a randomized controlled trial comparing two gastrojejunal anastomosis techniques. JSLS 12(4):385–388
Dewar L, Gelfand G, Finley RJ, Evans K, Inculet R, Nelems B (1992) Factors affecting cervical anastomotic leak and stricture formation following esophagogastrectomy and gastric tube interposition. Am J Surg 163(5):484–489
Jex RK, van Heerden JA, Wolff BG, Ready RL, Ilstrup DM (1987) Gastrointestinal anastomoses. Factors affecting early complications. Ann Surg 206(2):138–141
Pierie JPEN, De Graaf PW, Poen H, van der Tweel I, Obertop H (1993) Incidence and management of benign anastomotic stricture after cervical oesophagogastrostomy. Br J Surg 80(4):471–474
Lessing Y, Pencovich N, Khatib M, Meron-Eldar S, Koriansky J, Abu-Abeid S (2017) One-anastomosis gastric bypass: first 407 patients in 1 year. Obes Surg 27:1–7
Castro P, Ribeiro F, Rocha A, Mazzurana M, Alvarez G (2014) Hand-sewn versus stapler esophagogastric anastomosis after esophageal ressection: sistematic review and meta-analysis. ABCD Arquivos Brasileiros de Cirurgia Digestiva (São Paulo) 27(3):216–221
Viola F, Covidien LP, Mansfield, MA (2014) Assignee. Surgical instrument with curvilinear tissue-contacting surfaces. US Patent 20130056516. 2014
Bilotti F, Pomeroy GM, Omaits TP, Csiky L, Neurohr MA, Pastorelli A, Inventors (2008) Ethicon endo-surgery, Inc., Cincinnati, OH (US), assignee. Elliptical intraluminal surgical stapler for anastomosis. US patent 7422138. 2008
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Allen, W., Wells, C.I., Greenslade, M. et al. Association Between Circular Stapler Diameter and Stricture Rates Following Gastrointestinal Anastomosis: Systematic Review and Meta-analysis. World J Surg 42, 3097–3105 (2018). https://doi.org/10.1007/s00268-018-4606-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-018-4606-x