
Abstract
Summary
In this cross-sectional study, peripheral bone traits were examined relative to total daily steps measured with pedometer. Higher number of steps was associated with greater bone values at the calcaneus and tibia in women, but not in men. In women, dose-dependent associations at the radius were congruent with the weight-bearing bones.
Introduction
Habitual physical activity measured as daily steps may contribute to bone density and strength at the calcaneus and other weight-bearing bones.
Methods
Subgroups of 705–837 women and 480–615 men aged 31–46 years from the Cardiovascular Risk in Young Finns Study participated in the present study. Participants were instructed to use pedometer for 1 week, and the total daily steps, divided into tertiles, were evaluated relative to quantitative ultrasound-measured bone traits at the calcaneus and peripheral quantitative computed tomography-measured bone traits at the tibia and radius. Analysis of covariance was used to examine the between-group differences.
Results
In women, significant dose-dependent between-group differences were found in the weight-bearing bones and in non-weight-bearing radius. The differences in broadband ultrasound attenuation and speed of sound at the calcaneus were 3.8 and 0.5% greater in women within the highest tertile of daily steps compared to the lowest tertile (p values for trend ≤ 0.04). In tibia, women in the highest tertile (> 8765 steps/day) had on average 1–5.4% greater bone cross-sectional area, bone mineral content (BMC), trabecular density, and bone strength index at the distal site and 1.6–2.7% greater bone areas, BMC and strength strain index (SSI) at the shaft compared to women with less daily steps (p values for trend ≤ 0.02). Similarly, in radius, BMC and BSI at the distal site, and bone cross-sectional areas, BMC and SSI at the shaft were 1.7–3.4% greater in women within the highest tertile of daily steps compared to their peers (p values for trend ≤ 0.04). In men, the differences in calcaneal, tibial, and radial bone traits were mainly non-significant between the tertiles of daily steps.
Conclusion
Observed significant positive associations between daily steps and various bone traits at the calcaneus, tibia, and radius in women suggest that habitual physical activity may benefit skeletal health in adulthood.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Bone structure adapts to regular exercise that includes greater loading than induced by habitual daily activities. This is particularly well-documented in the lower and upper extremities of athletes participating in moderate–high impact sports that include, e.g., vertical jumps, rapid turns and stops, or repetitive impact loading [1,2,3,4]. Among general population, adults are recommended to exercise 3–5 times per week and indulge to endurance sports like running and brisk walking to load their skeletal structure [5, 6]. Also, a combination of strength training for a few times a week and a sufficient number of jumps daily are recommended as a part of bone-enhancing exercise.
Walking is the most common type of physical activity in humans. Indeed, daily steps have been suggested to increase bone mass and strength. In two studies on elderly Japanese women, daily walking steps were positively associated with the ultrasound parameters of calcaneus and negatively with bone resorption [7, 8]. In another study, on 50–80-year-old women and men, pedometer-determined steps were positively associated with areal bone mineral density (aBMD) at the hip especially in those over 65 years of age [9]. Also, in a Finnish exercise intervention trial on perimenopausal women, weekly endurance training including mainly brisk walking resulted in better maintenance of femoral neck aBMD [10]. Additionally, in a study comparing four different physical activity methods and two bone strength indices in young girls aged 8–13 years, pedometer steps were significantly associated with bone strength index (BSI) at the distal sites of femur and tibia [11]. In another study of young boys and girls aged 7–9 years, estimates of cortical bone and strength strain index (SSI) at the tibial mid-shaft were modestly higher in children who were in the active group according to daily steps and fitness tests compared to children classified to the inactive group [12]. So far, the longest follow-up of daily steps was collected in a study of Japanese women and men aged 65–84 years during a period of 5 years [13]. These researchers concluded that it would be beneficial to take at least 7000–8000 steps per day and noted also that habitual physical activity performed at higher intensity than three metabolic equivalents (MET) was associated with calcaneal bone health.
In the present study, we examined if daily steps measured with pedometer were associated with various bone traits determined at calcaneus, tibia, and radius. To the best of our knowledge, there are no previous studies that have investigated this association in a large sample of adults aged 31–46 years old.
Methods
Participants
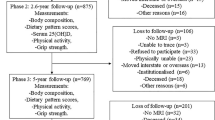
Participants in the present study, aged 31–46 years old, were participants of the Cardiovascular Risk in Young Finns Study which is an ongoing follow-up study of six age cohorts born in 1962, 1965, 1968, 1971, 1974, and 1977 (Table 1). At baseline in 1980, the study subjects were randomly chosen from the Finnish national register in the areas of five university cities Helsinki, Kuopio, Oulu, Tampere, and Turku (n = 3596 participated, 83% of those invited). Later, follow-up studies have been performed in 1983, 1986, 1989, 2001, 2007, and 2012 with the participation rates of 60–80% of the baseline cohort. Those who were lost in the follow-up have been described elsewhere [14, 15]. The study participants gave written informed consent, and the study protocol was reviewed and approved by the ethics committees of the participating universities.
Assessment of steps
In 2007, the pedometer study was conducted among 1876 individuals. Daily steps were gathered with the pedometer (Walking style One, HJ-152R-E, Omron Healthcare Co., LTD., Kyoto, Japan). Pedometers were instructed to be attached on the waistband or belt in the same position for 7 consecutive days and to be removed only while bathing or swimming [16]. Participants were asked to continue their habitual physical activity during the 1-week monitoring period. At the end of the day, the number of total steps was recorded in pedometer logs. Participants who had at least 4 monitoring days with at least 8-h pedometer wear time were included in all the analyses (n = 1853, 98.8% of those who completed the pedometer study). Sickness or injury status, exceptional step count recorded as an atypical day, or problems with pedometer use were imputed by the mean of other days. Pedometer accuracy for measuring total steps over 1000 m varied between 0.1–1.3% in different walking situations [16], and the Spearman’s rank correlation coefficient with steps measured by the accelometer (GT1M, ActiGraph, Pensacola, FL, USA) was 0.966 (p < 0.001) [17].
Bone measurements
In 2008, all those who had participated the Cardiovascular Risk in Young Finns baseline study, excluding those who had died (n = 77), moved abroad or forbid any further invitations, were invited to the peripheral quantitative computed tomography (pQCT) and quantitative ultrasound (QUS) bone measurements (n = 3386, 94.2% of the baseline cohort). Altogether, 1884 individuals (55.6% of those who were invited) from Turku, Helsinki, Tampere, Kuopio, and Oulu attended the pQCT measurements between February and December 2008 [18]. The corresponding number of the QUS measurements was 1953 (57.7% of the invited).
Both distal and diaphyseal sites of two functionally different bones, non-weight-bearing radius and weight-bearing tibia, were measured with pQCT (XCT 2000R, Stratec Medizintechnik GmbH, Pforzheim, Germany). Pregnant women were excluded from the measurements. Radius was measured on the non-writing hand and tibia on the left leg if no contraindication emerged, e.g., previous fracture of the given site. Distal sites were 4% for radius and 5% for tibia relative to the distal cortical endplate. The diaphyseal sites were 30% for both bones. Approximately 98% of the pQCT measurements were successfully scanned and analyzed. The main reasons for the failed pQCT investigation were missing scan images, inability to fit leg into the pQCT gantry, inaccurate positioning of the forearm or leg, or movement artifacts during scanning. For the distal sites, the contour and peel modes 2 were used according to the previously described procedures [19]. For the shafts, a density threshold of 710 mg/cm3 was applied to separate the cortical bone from other tissues. The pQCT measurements yielded the following bone traits: bone mineral content (BMC, mg), trabecular and cortical bone mineral densities (mg/cm3), and total and cortical bone cross-sectional areas (mm2). Additionally, three bone strength indices were calculated: SSI (mm3), BSI (g2/cm4), and cortical strength index (CSI). The conventional SSI was calculated as a density-weighted polar section modulus. It predicts the torsional bone strength and was determined for the diaphysis only. For the distal sites, BSI reflecting the compressive bone strength was calculated as a product of squared total bone mineral density and total cross-sectional area (total density2 × total area) [1]. The value of CSI corresponded to the ratio of cortical bone area and total bone area (cortical area/total area).
Additionally, the QUS technique (Sahara Clinical Bone Sonometer, Hologic Inc., Waltham, MA, USA) was used to measure the speed of sound (SOS, m/s) and broadband ultrasound attenuation (BUA, dB/MHz) at the calcaneus mainly from the left heel. Totally, ~ 23% of the QUS measurements were unsuccessful since there were problems in the propagation of ultrasound. The precision of the pQCT and QUS methods were evaluated in a subgroup (n = 39) with in vivo coefficients of variation (%), which varied between 0.3 and 4.8% [18].
Clinical measurements and lifestyle
In 2007, body weight, height, and body mass index (kg/m2) were determined with standard methods [20]. On the same year, energy and nutrient intakes were assessed with a 131-item food frequency questionnaire developed by the Finnish National Institute for Health and Welfare [21]. The quantities of nutrients were based on the Finnish Food Composition database, Fineli® [22]. Serum 25-hydroxy vitamin D (later calcidiol) levels (in nmol/l) of the study subjects were determined using radioimmunoassay (DiaSorin, Stillwater, Minnesota). Information on alcohol consumption (drinks during the previous week), smoking habits (daily or less frequently), and oral corticosteroid medication for at least 1 month (yes/no) were collected with self-administered questionnaires in 2007–2008. Maximal oxygen consumption (VO2max) and work rate (WRmax) were obtained from the exercise tests performed on electronically braked cycle ergometers during the years 2007–2009 in Tampere and Turku (Lode Corival 906900, Lode BV, Groningen, Netherlands). During the tests, 12-lead electrocardiography was recorded (Corina ECG amplifier and CardioSoft acquisition software ver. 4.2, GE Medical Systems, Freiburg, Germany) and breath-by-breath measurements performed with ventilator gas analyzers (V-max 29C, SensorMedics, Yorba Linda, CA, USA, and Jaeger Oxycon Pro, VIASYS Healthcare GmbH, Hoechberg, Germany). VO2max was determined as the highest oxygen uptake during the last 30-s averaged interval, and WRmax was calculated by adding the work during the last full minute interval to the fraction of the work performed over the final, interrupted interval. These tests and measurements have been described earlier in more detail [23]. Physical activity index in 2007 was calculated based on a self-report questionnaire which included items on intensity of physical activity, frequency of vigorous physical activity, hours spent on vigorous physical activity, average duration of a physical activity session, and participation in organized exercise.
Statistical analyses
For the statistical dose-dependence association analyses, participants were divided into tertiles by their mean daily steps. The following values were used as the cut-off values: < 6317 and > 8765 in women (min 1145; max 22,879) and < 5514 and > 7962 in men (min 1548; max 19,351). After the group classifications, associations with the characteristic variables were analyzed with the analysis of variance (ANOVA) or Brown-Forsythe test for continuous and chi-square test for categorical variables. In the main analyses, pQCT and QUS bone parameters were compared between the daily step tertiles with the analysis of covariance using age, height, weight, serum calcidiol level, and physical activity index as covariates. We also tested the linear trends with polynomial contrast because of an assumption of the dose-responsive effect of daily steps on bone traits. Analyses were done separately for women and men because of different endocrine profiles. Statistical analyses were carried out with IBM SPSS Statistics 24. p values ≤ 0.05 were considered statistically significant.
Results
The background characteristics of the study groups divided into tertiles by mean daily steps are shown in Table 1. In women, differences were seen in body height, weight, and body mass index (BMI) (p values ≤ 0.02). Body weight and BMI were the lowest among those women who had taken more than 8765 daily steps. Women in the highest tertile of steps had also higher mean serum calcidiol level, physical activity score, and maximal work rate value compared to less active women (p values ≤ 0.002). On the contrary, they smoked less than the other women (p value 0.02). In men, similar differences as in women were seen in body weight, BMI, physical activity score, and maximal work rate value (Table 1, p values ≤ 0.01). Mean serum calcidiol level was, instead, the highest among men in the middle tertile of daily steps (p value < 0.001). In addition, the VO2max value reflecting physical endurance capacity was the highest among men in the third tertile of daily steps (p value 0.001). On average, women had taken more daily steps than men during the monitoring week (7827 vs. 7063 steps/day, p value < 0.001).
In women, the differences in calcaneal BUA and SOS values were 3.8 and 0.5% greater in women in the highest tertile of daily steps compared to the lowest tertile (Table 2, p values for trend ≤ 0.04). Similarly in distal tibia, women with over 8765 daily steps had 1.1% larger total cross-sectional area, 3.2% higher BMC, 3.7% higher trabecular density, and 5.4% greater BSI than women in the lowest tertile of steps (Table 3, p values for trend ≤ 0.02). In tibial shaft, bone area was 1.7%, cortical bone area 1.6%, BMC 1.7%, and SSI 2.7% greater among women in the highest tertile of daily steps compared to the other women (Table 3, p values for trend ≤ 0.02). In radius, women in the highest tertile of daily steps had 2.2% higher BMC and 3.4% greater BSI at the distal site compared to women in the lowest tertile (Table 4, p values for trend ≤ 0.04). In radial shaft, total cross-sectional area was 2.3%, cortical area 1.7%, BMC 1.7%, and SSI 2.4% greater among women in the highest tertile of daily steps than in the lowest or middle tertile of steps (Table 4, p values for trend ≤ 0.03).
In men, the differences in calcaneal and radial bone traits were non-significant between the tertiles of daily steps (Tables 2 and 4). In distal tibia, total cross-sectional area and BMC were the highest in men within the middle tertile of steps (Table 3, p values for trend ≤ 0.03). In tibial shaft, bone area and SSI were, however, the greatest in men with least daily steps (Table 3, p values for trend ≤ 0.04). The differences between the highest and the lowest values ranged from 0.8 to 2%.
Discussion
In the present study, women aged 31–46 years whose mean daily steps exceeded 8765 had larger total and cortical bone cross-sectional areas, higher bone mineral mass and density, and greater proximal BSI and diaphyseal SSI at the weight-bearing tibia compared to their peers. Also, the calcaneal ultrasound parameters were higher among these more walking women. Similarly, in the non-weight-bearing radius, greater number of steps was associated with larger bone areas, higher bone mineral mass, and greater strength indices in women. In men, on the contrary, the results were non-significant at the calcaneus and radius. In tibia, some statistically significant but conflicting associations of daily steps with bone areas, BMC and SSI, were found in men. These results may reflect different physical activity habits between women and men in the present population. On an average, women had taken more daily steps than men during the monitoring week (difference 764 steps/day). Thus, women may have also exercised more frequently the so-called Nordic walking which was a popular leisure time activity at that time in Finland. In Nordic walking, sticks are used along with walking which makes it a good exercise for the arms and upper body too. This may explain the higher values in women’s radii with the highest number of daily steps compared to the other less walking women. In men, the associations between daily steps and studied bone traits were mainly non-significant why they should be interpreted cautiously. It may be, for instance, that men in the lowest tertile of daily steps took their steps at higher intensity which then contributed to slightly higher total area and SSI at the tibial shaft compared to the other men with more steps. This explanation cannot be, however, verified with pedometer which was used here to assess usual ambulatory activity.
Although, the loading effect of habitual daily steps on calcaneal, tibial, and radial bone traits seemed to be relatively small in women, it may have some clinical relevance. In a study where walking was the primary activity, 4 hours per week of walking was associated with 41% lower hip fracture risk in postmenopausal women compared to peers with less than 1 hour of walking per week [24]. Also, the walking pace seemed to influence the risk of hip fractures among these women, so that those who walked briskly were in the lowest fracture risk. However, in the meta-analysis of eight randomized controlled trials including postmenopausal women, no effect of walking interventions on lumbar spine BMD was found while the effect on femoral neck was modest [25]. The researchers concluded that the effect of walking on bone density as a sole exercise may be too small that it would reduce the fracture risk in these older women.
Previously, the positive association between daily steps and bone traits has been found in older women and men [7,8,9, 13] and in children [11, 12]. However, in a study of young students, no correlation was found between daily steps and ultrasound bone parameters [26]. Scheffler and others discussed that the reason behind this was a too homogenous population and that students may have been more health-conscious than the average population. It is also possible that the associations between different bone traits and habitual physical activity measured as total steps may vary with age as the total amount of physical activity may decrease or increase in different phases of life. The mean number of steps in the aforementioned studies varied from 6896 to 15,495 steps per day which is almost the same range as recommended for relatively healthy, younger adults [27].
We also found that daily steps were inversely associated with body weight in both genders and positively with serum calcidiol levels in women. Participants in the highest tertile of daily steps had on average 6.8–7.4% lower body weight and also 4.6–5.7% lower BMI than their study peers in the lowest tertile. In women, mean serum calcidiol level was on average 9.3% higher within the highest tertile of daily steps compared to the lowest tertile. In addition, the proportion of participants who smoked daily was the lowest in the highest tertile of daily steps in both genders. Participants with more daily steps had also higher physical activity score in general and better maximal work output in the cycle ergometer exercise test than their less walking counterparts. These health-related differences between the daily step groups may have also influenced the studied bone traits. For instance, vitamin D has many known effects on the physiological pathways relevant to bone mineral homeostasis, and it is also a common supplement along with calcium in patients with osteoporosis [28]. Also the differences in mean body weight and general physical activity may have confounded the results to some extent. In the earlier study from the Young Finns study cohort, overweight in childhood was associated with greater bone size later in adulthood [29]. Also, obesity in adulthood seemed to decrease the risk of low trabecular bone density at the distal sites of radius and tibia in the Young Finns cohort [18].
When considering the strengths of the present study, the observations were drawn from a large cohort including both women and men aged 31–46 years. To our knowledge, no similar studies in this age group have been done previously. In addition, three different peripheral bones, calcaneus, tibia, and radius were studied relative to objectively measured step counts which make our congruent results more reliable. Additionally, many health-related factors known to affect bone mass were examined in the present population and considered when interpreting the results.
There are some limitations in relation to the studied associations of step counts and peripheral bone parameters. The present study was a cross-sectional in design, and therefore, we do not know the outcomes between accumulated lifetime steps and different bone traits. However, prospective data on physical activity estimated with a self-report questionnaire from the present population was earlier shown to predict the level of physical activity in adulthood since childhood [30]. This same physical activity index was also used in our previous pQCT study where frequent habitual physical activity at the age of 9–18 years was associated with higher tibial bone size and strength indices in adulthood [31]. One limitation is also that steps were collected for a quite short period of time and can therefore be confounded by varying weather or participants’ health conditions. As earlier reported, the main reasons for non-participation and interruption of pedometer use were lost or broken pedometer (n = 75), illness (n = 30), and other reasons like untypical day (n = 22) [16]. In addition, subjects who participated the pedometer sub-study were more likely to have a higher socioeconomic position than all those who participated in the examinations of follow-up 2007. This may have resulted in higher number of reported steps compared to the general Finnish population. Pedometer itself has also some shortcomings since it cannot measure accurately the intensity of training or other types of exercises than locomotion, e.g., cycling, swimming, weight training, yoga, skiing, and similar exercises. These exercises can, however, be useful in promoting both general and bone health through developing the muscle strength. Despite these limitations, the objectively measured step data provided a relevant estimate of habitual physical activity in this population.
Conclusion
In conclusion, women aged 31–46 years who had taken more than 8765 daily steps had on average 1–5.4% greater bone cross-sectional areas, bone mineral content, trabecular density, and strength indices at the weight-bearing tibia compared to their study peers. Also, the calcaneal ultrasound parameters were 0.5–3.8% greater among more walking women. In non-weight-bearing radius, the results were similar as in the weight-bearing bones. In men, the associations of daily steps and peripheral bone traits were mainly non-significant. These results suggest that habitual daily steps may preserve bone mass and strength in women, but not in men. Obviously, more studies are needed to confirm these results.
References
Kontulainen S, Sievänen H, Kannus P, Pasanen M, Vuori I (2003) Effect of long-term impact-loading on mass, size, and estimated strength of humerus and radius of female racquet-sports players: a peripheral quantitative computed tomography study between young and old starters and controls. J Bone Miner Res 18:352–359
Nikander R, Sievänen H, Uusi-Rasi K, Heinonen A, Kannus P (2006) Loading modalities and bone structures at nonweight-bearing upper extremity and weight-bearing lower extremity: a pQCT study of adult female athletes. Bone 39:886–894
Nikander R, Kannus P, Dastidar P, Hannula M, Harrison L, Cervinka T, Narra NG, Aktour R, Arola T, Eskola H, Soimakallio S, Heinonen A, Hyttinen J, Sievänen H (2009) Targeted exercises against hip fragility. Osteoporos Int 20:1321–1328
Nikander R, Kannus P, Rantalainen T, Uusi-Rasi K, Heinonen A, Sievänen H (2010) Cross-sectional geometry of weight-bearing tibia in female athletes subjected to different exercise loadings. Osteoporos Int 21:1687–1694
Kohrt WM, Bloomfield SA, Little KD, Nelson ME, Yingling VR, American College of Sports Medicine (2004) American College of Sports Medicine position stand: physical activity and bone health. Med Sci Sports Exerc 36:1985–1996
Nikander R, Lepola V, Karinkanta S, Sievänen H. Muutama tunti reipasta liikuntaa viikossa - vähentyvätkö lonkkamurtumat kolmanneksella? Suomen Lääkärilehti 22/2008 vsk 63: 2033–2040 (only summary in English)
Kitagawa J, Omasu F, Nakahara Y (2003) Effect of daily walking steps on ultrasound parameters of the calcaneus in elderly Japanese women. Osteoporos Int 14:219–224
Kitagawa J, Nakahara Y (2008) Associations of daily walking steps with calcaneal ultrasound parameters and a bone resorption marker in elderly Japanese women. J Physiol Anthropol 27:295–300
Foley S, Quinn S, Jones G (2010) Pedometer determined ambulatory activity and bone mass: a population-based longitudinal study in older adults. Osteoporos Int 21:1809–1816
Heinonen A, Oja P, Sievänen H, Pasanen M, Vuori I (1998) Effect of two training regimens on bone mineral density in healthy perimenopausal women: a randomized controlled trial. J Bone Miner Res 13:483–490
Farr JN, Lee VR, Blew RM, Lohman TG, Going SB (2011) Quantifying bone-relevant activity and its relation to bone strength in girls. Med Sci Sports Exerc 43:476–483
Duckham RL, Rantalainen T, Ducher G, Hill B, Telford RD, Telford RM, Daly RM (2016) Effects of habitual physical activity and fitness on tibial cortical bone mass, structure and mass distribution in pre-pubertal boys and girls: the look study. Calcif Tissue Int 99:56–65
Shephard RJ, Park H, Park S, Aoyagi Y (2017) Objective longitudinal measures of physical activity and bone health in older Japanese: the Nakanojo Study. J Am Geriatr Soc 65:800–807
Juonala M, Viikari JS, Hutri-Kähönen N, Pietikäinen M, Jokinen E, Taittonen L, Marniemi J, Rönnemaa T, Raitakari OT (2004) The 21-year follow-up of the cardiovascular risk in Young Finns Study: risk factor levels, secular trends and east-west difference. J Intern Med 255:457–468
Raitakari OT, Juonala M, Rönnemaa T, Keltikangas-Järvinen L, Räsänen L, Pietikäinen M, Hutri-Kähönen N, Taittonen L, Jokinen E, Marniemi J, Jula A, Telama R, Kähönen M, Lehtimäki T, Åkerblom HK, Viikari JS (2008) Cohort profile: the cardiovascular risk in Young Finns Study. Int J Epidemiol 37:1220–1226
Hirvensalo M, Telama R, Schmidt MD, Tammelin TH, Xiaolin Y, Magnussen CG, Viikari JS, Raitakari OT (2011) Daily steps among Finnish adults: variation by age, sex, and socioeconomic position. Scand J Public Health 39:669–677
Mansikkaniemi K, Juonala M, Taimela S, Hirvensalo M, Telama R, Huupponen R, Saarikoski L, Hurme M, Mallat Z, Benessiano J, Jula A, Taittonen L, Marniemi J, Kähönen M, Lehtimäki T, Rönnemaa T, Viikari J, Raitakari OT (2012) Cross-sectional associations between physical activity and selected coronary heart disease risk factors in young adults. The cardiovascular risk in Young Finns Study. Ann Med 44:733–744
Laaksonen MML, Sievänen H, Tolonen S, Mikkilä V, Räsänen L, Viikari J, Lehtimäki T, Kähönen M, Raitakari OT (2010) The cardiovascular risk in Young Finns Study group. Determinants of bone strength and fracture incidence in adult Finns: cardiovascular risk in Young Finns Study (the GENDI pQCT study). Arch Osteoporos 5:119–130
Sievänen H, Koskue V, Rauhio A, Kannus P, Heinonen A, Vuori I (1998) Peripheral quantitative computed tomography in human long bones: evaluation of in vitro and in vivo precision. J Bone Miner Res 13:871–882
Raiko JR, Viikari JS, Ilmanen A, Hutri-Kähönen N, Taittonen L, Jokinen E, Pietikäinen M, Jula A, Loo BM, Marniemi J, Lehtimäki T, Kähönen M, Rönnemaa T, Raitakari OT, Juonala M (2010) Follow-ups of the cardiovascular risk in Young Finns Study in 2001 and 2007: levels and 6-year changes in risk factors. J Intern Med 267:370–384
Paalanen L, Männistö S, Virtanen MJ, Knekt P, Räsänen L, Montonen J, Pietinen P (2006) Validity of a food frequency questionnaire varied by age and body mass index. J Clin Epidemiol 59:994–1001
National Institute for Health and Welfare, Nutrition Unit. Fineli. Finnish food composition database. Release, 10; 2009. http://www.fineli.fi. Helsinki
Hulkkonen J, Aatola H, Pälve K, Lehtimäki T, Hutri-Kähönen N, Viikari JS, Raitakari OT, Kähönen M (2014) Determinants of exercise peak arterial blood pressure, circulatory power, and exercise cardiac power in a population based sample of Finnish male and female aged 30 to 47 years: the cardiovascular risk in Young Finns Study. BMC Cardiovasc Disord 14:35
Feskanich D, Willett W, Colditz G (2002) Walking and leisure-time activity and risk of hip fracture in postmenopausal women. JAMA 288:2300–2306
Martyn-St James M, Carroll S (2008) Meta-analysis of walking for preservation of bone mineral density in postmenopausal women. Bone 43:521–531
Scheffler C, Gniosdorz B, Staub K, Rühli F (2014) Skeletal robustness and bone strength as measured by anthropometry and ultrasonography as a function of physical activity in young adults. Am J Hum Biol 26:215–220
Tudor-Locke CE, Myers AM (2001) Methodological considerations for researhers and practitioners using pedometers to measure physical (ambulatory) activity. Res Q Exerc Sport 72:1–12
Bhattoa HP, Konstantynowicz J, Laszcz N, Wojcik M, Pludowski P (2016) Vitamin D: musculoskeletal health. Rev Endocr Metab Disord 18:363–371. https://doi.org/10.1007/s11154-016-9404-x
Uusi-Rasi K, Laaksonen M, Mikkilä V, Tolonen S, Raitakari OT, Viikari J, Lehtimäki T, Kähönen M, Sievänen H (2012) Overweight in childhood and bone density and size in adulthood. Osteoporos Int 23:1453–1461
Telama R, Yang X, Viikari J, Välimäki I, Wanne O, Raitakari O (2005) Physical activity from childhood to adulthood: a 21-year tracking study. Am J Prev Med 28:267–273
Tolonen S, Sievänen H, Mikkilä V, Telama R, Oikonen M, Laaksonen M, Viikari J, Kähönen M, Raitakari OT (2015) Adolescence physical activity is associated with higher tibial pQCT bone values in adulthood after 28-years of follow-up—he cardiovascular risk in Young Finns sudy. Bone 75:77–83
Funding
The Young Finns Study has been financially supported by the Academy of Finland: grants 286284, 134309 (Eye), 126925, 121584, 124282, 129378 (Salve), 117787 (Gendi) (ST), and 41071 (Skidi); the Social Insurance Institution of Finland; Competitive State Research Financing of the Expert Responsibility area of Kuopio, Tampere and Turku University Hospitals (grant X51001); Juho Vainio Foundation (ST); Paavo Nurmi Foundation; Finnish Foundation for Cardiovascular Research; Finnish Cultural Foundation (ST); Tampere Tuberculosis Foundation; Emil Aaltonen Foundation; Yrjö Jahnsson Foundation; Signe and Ane Gyllenberg Foundation, and Diabetes Research Foundation of Finnish Diabetes Association.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Tolonen, S., Sievänen, H., Hirvensalo, M. et al. Higher step count is associated with greater bone mass and strength in women but not in men. Arch Osteoporos 13, 20 (2018). https://doi.org/10.1007/s11657-018-0425-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-018-0425-9