
Abstract
Bisphenols (BPs) are potential thyroid disruptors that are widely used in many consumer products, leading to their widespread exposure in the general population. Current cross-sectional and case-control studies have found associations between exposure to BPs and serum thyroid function, but the results were contradictory. The objectives of this study are to describe demographic characteristics, BP exposure levels, and thyroid function measurements in potentially exposed and control districts and to investigate the association of urinary BPs with thyroid function. Data were collected from a general population aged 3–79 years (N = 281) recruited by the Zhejiang Human Biomonitoring Program (ZJHBP). The concentrations of 10 kinds of BPs in urine and serum free triiodothyronine (FT3), total triiodothyronine (TT3), free thyroxine (FT4), total thyroxine (TT4), thyroid-stimulating hormone (TSH), thyroglobulin (Tg), thyroglobulin antibodies (TgAb), thyroid peroxidase antibodies (TPOAb), and thyrotropin receptor antibody (TRAb) in serum were measured. Multiple linear regression and weighted quantile sum (WQS) regression were used to estimate the relationship between single and mixed exposure of BPs and thyroid function. Bisphenol A (BPA), bisphenol S (BPS), and bisphenol P (BPP) were detected, respectively, in 82.73%, 94.24%, and 55.40% of the population in the exposed area and 81.69%, 61.27%, and 43.66% of the population in the control area. Among adult females, serum TT3 was negatively associated with urinary BPA (β = −0.033, 95% CI = −0.071, −0.008, P = 0.021). Among minor females, FT4 and Tg levels were negatively associated with the urinary BPA (β = −0.026, 95% CI = −0.051, −0.002, P = 0.032 for FT4; β = −0.129, 95% CI = −0.248, −0.009, P = 0.035 for Tg), and TPOAb was positively associated with urinary BPA (β = 0.104, 95% CI = 0.006, 0.203, P = 0.039). In WQS models, BPs mixture was positively associated with FT3 (βWQS = 0.022, 95% CI = 0.002, 0.042) and TT3 (βWQS = 0.033, 95% CI = 0.004, 0.062), and negatively associated with FT4 (βWQS = −0.024, 95% CI = −0.044, 0.004). We found widespread exposure to BPA, BPS, and BPP in the general population of Zhejiang province and found an association between BPA and thyroid hormones. This association is gender- and age-dependent and needs to be confirmed in further studies.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Bisphenols (BPs) refer to a class of organic compounds that comprise two hydroxyphenyl structures. Bisphenol A (BPA; 2,2-bis (4-hydroxyphenyl) propane) is a major monomer used in the manufacture of polycarbonate and epoxy resins found in metal cans, food containers, medical equipment, thermal receipts, and adhesives (Mustieles et al. 2020). It is estimated that at least 8 million tons of BPA are produced throughout the world every year, and hundreds of tons are released into the natural environment (Schirmer et al. 2021). BPA with different concentrations has been detected in surface water, soil, and the atmosphere all over the world and is also commonly identified in human serum, urine, and breast milk (Chakraborty et al. 2019; Larsson et al. 2017; Yamazaki et al. 2015; Lee et al. 2018). Due to the adverse effects of BPA on humans, the European Union and China prohibited BPA-based baby bottles and infant formula packaging in 2010 and 2011 (Liang et al. 2020). In response to this, BPA has since then been increasingly replaced by analogues such as bisphenol S (BPS) and bisphenol F (BPF). However, the biological and environmental effects of these analogues are still ambiguous.
A large amount of research on BPA has revealed the mechanism of its damage to health. As an endocrine disruptor, BPA can disrupt the synthesis, secretion, release, and transport of hormones (Mhaouty-Kodja et al. 2018). It was found that mature adipocytes differentiated under BPA exposure showed insulin resistance and low glucose uptake, suggesting that BPA exposure may cause obesity (De Filippis et al. 2018). BPA exposure may also contribute to type 2 diabetes mellitus (T2DM) (Farrugia et al. 2021; Sowlat et al. 2016). The genotoxicity of BPA is shown by the chromosomal mutation during meiosis, which leads to an increase of sex chromosome diploid of male sterile sperm (Radwan et al. 2018). BPA analogues have a similar structure to BPA, and they may also have potential health impacts and show similar endocrine effects. Although recent studies have found potential effects of BPA analogues such as BPS on the reproductive system and mammary gland as well as on behavior and obesity, few studies have so far been conducted, and more research is needed to confirm the health effects of BPA substitutes (Ahn et al. 2020; John et al. 2019; Rezg et al. 2018; Wormsbaecher et al. 2020).
Thyroid hormone plays a vital role in many physiological processes, such as energy balance, metabolism, and the development of nervous, cardiovascular, and reproductive systems (Blanco 2020; Pagnin et al. 2021; Silva et al. 2018; Sinha et al. 2018; Vassalle et al. 2021). Researchers have demonstrated in vivo (zebrafish) and in vitro (rat thyroid follicular cells) that BPA exposure can change the expression of genes involved in the synthesis of thyroid hormones, leading to a decrease in thyroid hormone synthesis (Gentilcore et al. 2013; Wu et al. 2016). However, in existing epidemiological studies, the relationship between exposure to other BPs and thyroid function in the general population is confusing. Cross-sectional studies in the USA (BPs = 1.92 (1.17, 3.33) ng/mL) and Thailand (BPs = 0.35 (0.09, 0.84) ng/mL) found negative associations between BPs exposure and thyroid function, and another cross-sectional study in China (BPs = 48.06 (12.58, 164.52) ng/mL) found a positive association between BP exposure and thyroid function, while no association was observed in a case-control study in Cyprus (BPs = 2.3 (1.1, 4.6) ng/mL) (Andrianou et al. 2016; Meeker and Ferguson 2011; Sriphrapradang et al. 2013; Wang et al. 2012). These studies may have caused these inconsistent results due to reasons such as race, regions, sample size, and individual differences. Furthermore, epidemiological studies on the association of BPA analogues with thyroid function are rarely reported. Cohort studies in Puerto Rico and Korea reported a negative association of urinary BPS with Tsh and a negative association of urinary BPF with FT4, and a cross-sectional study in Poland found a negative association between BPC and TSH (Aker et al. 2019; Jang et al. 2021; Milczarek-Banach et al. 2020); further confirmation in population studies is needed.
Most of the current studies focus on the general population living in residential areas, and there are few on the exposure to BP compounds of people residing around industrial parks. Therefore, we selected those residing around an industrial park in Zhejiang province as survey participants to study the body burden levels of residents in areas with high and low exposure. The industrial park is a large joint chemical enterprise with multiple industries, including those producing fertilizers, refrigerants, industrial gases, pharmaceuticals, and resin materials. Established in the 1960s, the industrial park has a long history of possible long-term exposure to environmental pollutants of residents in the periphery. In summary, in this cross-sectional study, we aim to investigate the association of urinary concentrations of BPA and its nine analogues with thyroid function at an industrial park in Zhejiang province, China. And based on previous studies, we hypothesized that exposure to BPA and its analogues might be associated with altered thyroid function. These nine analogues consist of BPF, BPS, bisphenol AF (BPAF), bisphenol Z (BPZ), bisphenol P (BPP), bisphenol B (BPB), bisphenol C (BPC), bisphenol E (BPE), and bisphenol AP (BPAP).
Methods
Study population
This study is part of the Zhejiang Human Biomonitoring Program (ZJHBP), a population-based representative and prospective cross-sectional study that has been established to record the degree of human exposure to various environmental chemicals and understand the exposure profile, degree, and continuous trend of the general population in Zhejiang province, China. district A, where the industrial park was located, was selected as the exposed area, and district B was selected as the control area. Both district A and district B are located in the same city, and the living standards and dietary habits of residents in the two regions were similar. Participants recruited in the two districts of Zhejiang gave written consent for the collection of blood and urine samples and their participation in the ZJHBP study. This study was conducted from September to October 2021. The exclusion criteria were as follows: history of thyroid disease (including thyroid cancers), history of surgical thyroid interventions, family history of thyroid function, mental disease, cognitive impairment, history of occupational exposure to poisons, and living in the monitoring area for less than 6 months. The participants were also excluded if there were missing biological samples, a lack of information on critical variables, or if they were treated with medicines that affect thyroid function, such as amiodarone, phenytoin sodium, and carbamazepine.
A total of 144 residents were sampled from each of the two surveillance areas and divided into six strata according to age (i.e., aged 3–5 years, 6–11 years, 12–18 years, 19–39 years, 40–59 years, and 60–79 years). Each stratum was divided into two strata according to gender, producing a total of 12 strata. Four participants were selected at each stratum according to simple random sampling for the questionnaire survey and biological sample collection. Participants under age eighteen were defined as minors, and those above age eighteen were defined as adults. A total of 288 people were selected from the two districts, and respondents with incomplete information and a lack of biological samples were excluded. Finally, 281 subjects from the two districts (139 from A and 142 from B) were included in the analysis.
Questionnaires and physical examination
Site investigations were conducted simultaneously in both districts from 10 to 12 September 2021. Professionally trained investigators recorded information through detailed questionnaires on personal basic information (age, gender, ethnicity, education level, marital status, etc.), history of disease, family history of disease, occupational history, and lifestyle factors. All questionnaire information was collected on tablets and audio recorded in real time. Height (cm) and weight (kg) were measured without shoes, and body mass index (BMI) was calculated by dividing weight by the square of height (kg/m2).
Blood samples were collected after at least 8 h of fasting in the morning about 7 to 9 a.m. These were left to coagulate for 30 min and then centrifuged at 3000 rpm for 10 min at room temperature to obtain serum. Serum samples were frozen at −80 °C and stored at the Zhejiang Center for Disease Control and Prevention. The participants’ urine samples were collected in the morning, aliquoted into 4.5 mL polypropylene tubes, and then stored in refrigerators at −80 °C until analysis.
Serum thyroid hormone measures
Serum-free triiodothyronine (FT3), total triiodothyronine (TT3), free thyroxine (FT4), total thyroxine (TT4), thyroid-stimulating hormone (TSH), thyroglobulin (Tg), thyroglobulin antibodies (TgAb), thyroid peroxidase antibodies (TPOAb), and thyrotropin receptor antibody (TRAb) were measured by electrochemiluminescence immunoassay (Cobas® e601; Roche, Mannheim, Germany). The limit of quantitation (LOQ) of TT3, FT3, TT4, FT4, TSH, Tg, TgAb, TPOAb, and TRAb was 0.3 nmol/L, 0.4 pmol/L, 5.4 nmol/L, 0.5 pmol/L, 0.005 μIU/mL, 0.04 ng/mL, 10 IU/mL, 5 IU/mL, and 0.8 IU/L, respectively. TPOAb, TgAb, and TRAb positivity were defined as TPOAb > 34 IU/mL, TgAb > 115 IU/mL, and TRAb >1.75 IU/L.
Measurements of BP concentrations in urine
Urine samples were pretreated by the quick, easy, cheap, effective, rugged, and safe (QuEChERS) method combined with liquid–liquid extraction (LLE) (Zhang et al. 2019). A total of 1 mL of urine was spiked with 2 ng of the internal standards (BPA−13C12, BPF−13C6, BPS−13C12, BPP−13C4, BPB−D8, BPZ−D6, BPAF−13C12, BPAP−13C6, BPE−13C6) followed by the addition of 100 μL of 1 M ammonium acetate buffer (PH = 5, containing 4000 units of β-glucuronidase/arylsulfatase) and 50 μL 100 ng/mL 4-methylumbelliferyl-β-D-glucuronide in methanol. After enzymatic hydrolysis at 37 °C in a water bath for 3 h, 3 mL ethyl acetate was added and shaken for 40 min and then centrifuged at 4400 rpm for 15 min. The supernatant was extracted; then, 1 mL of deionized water (containing 150 mg MgSO4, 50 mg PSA, and 50 mg C18) was added; after being shaken and centrifuged, the supernatant was dried at 37 °C and then dissolved with 100 μL 70% methanol solution, shaken, and centrifuged (4400 rpm, 15 min). BPs were analyzed using ultra performance liquid chromatography (UPLC) coupled with a triple quadrupole mass spectrometer operating in electrospray ionization (ESI) mode (Waters ACQUITY UPLC I-Class, Xevo TQ-S, Milford, MA) (van der Meer et al. 2019). The LOQ of BPA, BPF, BPS, BPAF, BPZ, BPP, BPB, BPC, BPE, and BPAP was 0.08, 0.08, 0.05, 0.05, 0.05, 0.05, 0.5 ,0.5, 0.5, and 0.05 ng/mL. Urine creatinine was determined by the enzymatic method, which was used to standardize urinary dilution.
We also searched for studies on population BP exposure worldwide over the past 2 decades on PubMed, obtained their reported BP concentrations, and compared them with our study. We searched separately for studies in China (Cui et al. 2021; Guo et al. 2021; Jiang et al. 2020; Li et al. 2019; Liang et al. 2020; Liu et al. 2019b; Ouyang et al. 2020; Wang et al. 2019; wuHu et al. 2019; Zhang et al. 2016), Asia (Gys et al. 2020; Kang et al. 2020; Lee et al. 2020; Liu et al. 2019a; Machtinger et al. 2018; Park et al. 2017), Europe (Casas et al. 2015; Derakhshan et al. 2019; Frederiksen et al. 2013a; Milczarek-Banach et al. 2020; Myridakis et al. 2015; Peinado et al. 2020; Philips et al. 2018; Tkalec et al. 2021; Ye et al. 2009), North America (Kataria et al. 2017; Meeker and Ferguson 2011; Mendy et al. 2020; Quiros-Alcala et al. 2021; Tai and Chen 2016), and Australia (Heffernan et al. 2016).
Quality control procedure
The quality control of the questionnaire survey content includes the main technical materials such as questionnaires and work manuals required for the survey, which are uniformly compiled by China CDC and provided with electronic questionnaires. In order to ensure the progress of the work, communicate with the relevant local departments in advance to make arrangements for investigators and professional training. The quality control of blood sample collection includes standing still within 2 h and centrifuging to separate serum, and urine samples need to avoid contamination by semen or menstrual blood. All biological samples need to be packaged in clean and sterile collection tubes. Those that cannot be tested within 8 h need to be stored and transported at 4 °C, and samples that need to be stored for a long time should be stored at −80 °C.
Statistical analysis
In the statistical description, continuous variables were represented by mean ± standard deviation (SD), and categorical variables were represented by frequency (percentage). The differences in characteristics between the two districts were examined using one-way ANOVA tests for continuous variables and chi-square tests for categorical variables. BP and thyroid hormone concentrations below LOQ were replaced with a value equal to half LOQ. The data were not normally distributed (Shapiro-Wilk test, P > 0.05), the Mann–Whitney U test of continuous variables was used to compare the thyroid hormone level and BP concentration between the two districts, and the chi-square test of proportion was used to evaluate the difference in BP detection rate. Thyroid hormone and BP concentrations were distributed in a skewed manner, so the data were log-transformed prior to association and regression analysis.
In the questionnaire, data on age (continuous variable), gender (categorical variable), BMI (continuous variable), marital status (categorical variable), education level (categorical variable), smoking status(categorical variable), alcohol consumption (categorical variable), occupation (categorical variable), physical activity (categorical variable) and creatine concentration (continuous variable) were determined as covariates. The selection of these covariates was based on previous studies (Meeker and Ferguson 2011). Smoking was classified as current, former, or never. Alcohol consumption was defined as any alcohol consumed within a year.
Multiple linear regression was conducted to assess the association between urinary BP and thyroid hormone measurements, and the covariates mentioned above were included in the regression model. The collinearity between BPs was evaluated in the regression model by calculating the coefficient of variance inflation factor. In all models, urinary concentrations of BPs were converted to μg/g creatinine to adjust for dilution.
Weighted quantile sum (WQS) model was used to estimate the mixture effects of BP exposure on people’s thyroid function. A detailed description of WQS regression can be found elsewhere (Carrico et al. 2015). The WQS index was created using quartiles of BP concentrations, and the estimated empirical weight of each BPs in the index represents their relative contribution to the combined effect on thyroid function. This approach took all the measured BPs into consideration and constrained all the BPs into a single direction of effect on the health outcome. The sum of WQS weights is constrained to be equal to 1. In this study, bisphenols with estimated weights greater than 0.333 (1/3) were thought to have a significant effect on thyroid function (Nguyen 2023; Nguyen and Kim 2022). All analyses were conducted with SPSS statistical software (version 25.0; SPSS Inc., Chicago, IL) and R (version 4.2.3). For the statistical significance, the cut off P-value was set to 0.05.
Results
Study population
Table 1 shows that the study population included 281 participants, with 139 from district A and 142 from district B. The mean age and BMI in district A were 29.73 years (SD 23.04) and 20.07 kg/m2 (SD 5.67), respectively. Approximately half of the participants were male (52.52%). A high proportion did not smoke (81.29%) or consume alcohol (76.26%). The mean age and BMI in district B were 30.49 years (SD 23.52) and 21.40 kg/m2 (SD 5.32), respectively. The characteristics of the participants in the two districts were similar. There were no significant differences in age, BMI, gender, education level, marital status, smoking status, and alcohol drinking between districts A and B (P > 0.05). The same results were found both in adults and minors in the two districts, and the questionnaire for minors did not include marital status, smoking, and alcohol consumption. The detailed characteristics of adults and minors are presented in Tables S1 and S2.
Levels of bisphenols in urine
Distributions of urinary BP levels between the two districts are compared in Table S3. Due to the detection rate of other BPs being less than 40%, only BPA, BPS, and BPP were included in the analysis. Figure 1 shows the BP exposure levels among different ages in the two districts. For adults and minors, the exposure levels of BPA (0.47 vs. 0.27 ng/mL for adults; 1.46 vs. 0.35 ng/mL for minors) and BPS (0.32 vs. 0.06 ng/mL for adults; 0.37 vs. 0.08 ng/mL for minors) in the exposed area were higher than in the control area, and the exposure to BPA was much higher in minors than in adults in the exposed area (P < 0.05). We found that BPP urinary concentrations were higher among adults in the exposed area than among those in the control area (P < 0.01), and no significant differences were found between adults and minors (P > 0.05). The levels of BPs in adults and minors in both districts are also detailed in Tables S4 and S5. When stratified by gender, BPA and BPS levels were higher in district A than in district B in both males and females (P < 0.01), but no differences were found between men and women within the same area (P > 0.05) (Table S6). We further stratified by gender and age and found that in adult males, BPS (0.30 vs. 0.08 ng/mL) and BPP (0.08 vs. 0.03 ng/mL) concentrations were significantly higher in district A than in district B. However, in adult females, BPA and BPS levels were higher in the exposed area than in the control area (Table 2). Among minors, in both males and females, BPA and BPP levels were higher in district A than in district B (Table 3), and no gender differences in exposure levels were observed at different ages. Spearman’s association coefficients between the three BPs ranged from 0.185 to 0.379 (P < 0.01) (Table S7). In all participants, with the increase of age, the urinary BPA, BPS and BPP concentration decreased significantly (r = −0.323, P < 0.001 for BPA; r = −0.181, P = 0.002 for BPS; r = −0.141, P = 0.018 for BPP). Age was significantly associated with higher and lower levels of exposure.

Median concentrations of three major bisphenols in adults and minors’ urine in two districts. *Correlation coefficient is significant at 0.05 level. **Correlation coefficient is significant at 0.01 level
Thyroid function analysis
Levels of thyroid hormones in the serum of participants are shown in Table S8. With the exception of TRAb, which had a detection rate of less than 30%, all other thyroid hormones had a high percentage of LOQ, so TRAb was excluded from the analysis. The median levels of serum FT3, TT3, TSH, Tg, and TgAb were comparable between participants in the two districts, and there was no significant difference in the abnormal rate of thyroid function between the two districts (Table S9).
Stratifying adults and minors, we found that median TT4 (93.29 vs. 105.50 nmol/L) and TPOAb (9.05 vs. 10.20 IU/mL) concentrations were significantly lower in A than in B among adults (P < 0.05) (Table S10), while TT4 (17.41 vs. 17.88 nmol/L) and FT4 (94.48 vs. 103.40 pmol/L) levels were significantly lower in A than in B among minors (P < 0.05) (Table S11). We further stratified by gender, finding a more pronounced difference between males and females. In adult males, FT3 (5.09 vs. 5.50 pmol/L) levels in A were lower than those in B, and in adult females, TT3 (1.53 vs. 1.67 nmol/L), TT4 (93.21 vs. 101.50 nmol/L,) and TPOAb (8.46 vs. 11.19 IU/mL) levels in A were significantly lower than those in B (Table 4). In minor males, no differences were observed (P > 0.05), and in minor females, TT4 (88.88 vs. 99.27 nmol/L) levels were significantly lower in the exposed area than in the control area (P < 0.05) (Table 5).
Relationships between bisphenol exposure and levels of thyroid hormones
In all populations, we found a positive relationship between FT3 and BPS (β = 0.022, 95% CI = 0.009, 0.001, P = 0.043), TT4 and BPP (β = 0.012, 95% CI = 0.012, 0.035, P = 0.001), and TT3 and BPS (β = 0.021, 95% CI = 0.002, 0.040, P = 0.028) (Table S12). Our study found differences in outcomes between adults and minors, and differences between genders were also observed. Stratified according to adults and minors, no association was observed among adults (Table S13). In minors, we observed a negative association between urinary BPA and serum FT4 (β = −0.013, 95% CI = −0.026, −0.001, P = 0.037) and a positive association between BPP and TT4 (β = 0.035, 95% CI = 0.006, 0.064, P = 0.017) (Table S14).
Table S15 and Table S16 presented the relations between BP concentrations in urine and measures of thyroid function in males and females, adjusted for age, BMI, gender, education levels, marital status, smoking status, alcohol assumption, urinary creatinine, occupation, and physical activity. in linear regression. As shown in Fig. 2, in adult females, serum TT3 levels were negatively correlated with urinary BPA levels (β = −0.033, 95% CI = −0.071, −0.008, P = 0.021). In minor females, the levels of serum FT4 and Tg were negatively related to the levels of urinary BPA (β = −0.026, 95% CI = −0.051, −0.002, P = 0.032 for FT4; β = −0.129, 95% CI = −0.248, −0.009, P = 0.035 for Tg). Positive association between levels of urinary BPA and TPOAb was also observed (β = 0.104, 95% CI = −0.248, −0.009, P = 0.039).

Association between urinary BPA concentrations and thyroid function indicator levels serum samples from the adult females (a) and minor females (b)
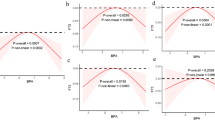
The WQS model was used to further analyze the association between mixed BPS and thyroid function in all populations. The WQS weights and regression index of BP mixture with thyroid function in the WQS model were shown in Fig. 3. BP mixture was positively associated with FT3 (βWQS = 0.022, 95% CI = 0.002, 0.042) and TT3 (βWQS = 0.033, 95% CI = 0.004, 0.062) and negatively associated with FT4 (βWQS = −0.024, 95% CI = −0.044, 0.004), with BPS (0.532), BPA (0.618), and BPA (0.547) as their corresponding highest weight chemicals. Detailed results of adjusted models are presented in Table S17.

The WQS model regression index weights for FT3 (a), TT3 (b), and FT4 (c). All models adjusted for ln-transformed urinary creatinine, age, BMI, education level, marital status, smoking status, alcohol drinking, occupation, and physical activity
Discussion
Wide exposure to BPA, BPS, and BPP was found among the general population in Zhejiang province, with all detection rates > 40%. The median urinary concentration of BPA was the highest among the 10 BPs. Urinary concentrations of BPA and BPS were higher in the exposed area than in the control area in both adults and minors, indicating that residents living around the industrial park have a higher body burden of BPs (Fig. 1). Figure 4 shows a comparison of the distributions of BP concentrations in urine around the world over the past 2 decades. Based on the results we listed, most studies reported higher proportions of BPA, BPF, and BPS. Compared with domestic levels, the urinary BP concentrations in the studies from Nanjing (0.39 ng/mL) (Liu et al. 2019b), Dalian (0.68 ng/mL) (Guo et al. 2021), and Hubei (0.82 ng/mL) (Cui et al. 2021) were similar to the control district (0.41 ng/mL) of our study but lower than the exposed district (1.42 ng/mL). The BP levels in the exposed area were similar to those in Xuzhou (1.25 ng/mL) (Li et al. 2019) and Shanghai (1.14 ng/mL) (Ouyang et al. 2020) but much lower than those in Guangxi (3.15 ng/mL) (Liang et al. 2020) and Qingyuan (3.73 ng/mL) (Zhang et al. 2016). The study area in Qingyuan was near an e-waste dismantling plant, which may be the reason for such high BP levels in the population in this area. Compared with other countries, BP levels in the exposure district in our study were similar to those in the study in Hokkaido, Japan (1.07 ng/mL) (Gys et al. 2020), but lower than other studies in Asian countries, such as south Korea (2.35 ng/mL) (Kang et al. 2020), Singapore (2.69 ng/mL) (Liu et al. 2019a), and Israel (2.10 ng/mL) (Machtinger et al. 2018), and in Europe, except for in Greece (1.20 ng/mL) (Myridakis et al. 2015), Poland (0.77 ng/mL) (Milczarek-Banach et al. 2020), and Denmark (1.37ng/mL) (Frederiksen et al. 2013a). Other studies have reported higher BP levels than our study, including in the Netherlands (2.59 ng/mL) (Philips et al. 2018), Slovenia (1.99 ng/mL) (Tkalec et al. 2021), Spain (3.80 ng/mL) (Casas et al. 2015), Sweden (1.74 ng/mL) (Derakhshan et al. 2019), and Norway (4.50 ng/mL) (Ye et al. 2009). In North America, the levels in the Canadian study were similar to those in our study (1.22 ng/mL) (Tai and Chen 2016), but in the USA, these were much higher than in ours (2.43, 1.89,4.80 ng/mL) (Kataria et al. 2017; Mendy et al. 2020; Quiros-Alcala et al. 2021). In the New York study, the concentration of BPS was much higher than that of BPA and BPF, which may be related to the widespread use of local BPA alternatives in the market (Kataria et al. 2017). Compared with that in our study, the BP concentration in Brisbane, Australia, was at a higher level (3.80 ng/mL) (Heffernan et al. 2016).

Median levels of bisphenols (ng/mL) in urine worldwide over the past 2 decades. The data are shown by region and sample collection years. The red and black lines indicate the levels in the exposed and control areas of the study, respectively. *Geometric mean levels
In this study, it was found that although the exposure level of BPs in district A was higher than that in district B, compared with the studies in other regions domestic and abroad, the exposure level in district A was lower, and that in district B was much lower than other regions. The possible reason is that the main products of this industrial park are refrigerants whose raw materials are fluorides, and the production of epoxy resin materials made of BPs as raw materials is less, resulting in a lower exposure concentration of BPs.
In addition, urinary BPA concentration in minors in the exposed area was significantly higher than that in local adults (Fig. 1). The results of this study also showed a negative association between age and BP exposure concentration. BPA exposure is usually through dietary intake (He et al. 2009), and minors are generally considered to be vulnerable to exposure to environmental pollutants. Minors are more exposed to BPA compared to adults. According to the U.S. Environmental Protection Agency (U.S. EPA), higher food consumption relative to body weight is higher in minors compared to adults, which justifies higher concentrations in minors (EPA 2011). Thus, the relatively higher urinary BPA concentrations in minors may be due to relatively higher oral exposure to BPA, although this cannot fully explain the higher urinary BPA concentrations in minors. Studies in other regions have reported similar findings (Bushnik et al. 2010; Frederiksen et al. 2013a; Larsson et al. 2014). A number of studies have collected urine samples from mothers of minors and found that the level of BPA in minors’ urine is much higher than that of mothers (Covaci et al. 2015; Frederiksen et al. 2013b; Larsson et al. 2014). However, in adults and minors in the same district, we did not find any difference in BPA concentration between different genders. This is consistent with reports from previous studies demonstrating that men and women do not differ significantly in BPA concentrations (Aekplakorn et al. 2015; Olsen et al. 2012).
In summary, we collected most of the population studies from around the world and found the BP levels in the exposed area of our study to be among the world’s medium levels, whereas our control area is among the world’s low levels. Although countries have gradually banned BPA in baby bottles and packaging, other routes of exposure continue, and BPA still dominates total BPs in most countries and regions. However, there are also areas where BPA has been replaced by its analogues, such as in the New York study, where BPS accounted for most of the BPs (Fig. 4). We did not measure the concentration of BPs in environmental samples, so the route of exposure was unclear. Follow-up studies are needed to explore the pathways of local population exposure to BPs.
The rates of thyroid function abnormalities in the two areas were all low, and there was no significant difference between them. This indicates that the general population was still at a relatively healthy level, even though BP exposure between the two places was quite different. In the total population, we reported positive associations between BPS and FT3, BPS and TT3, and BPP and TT4, but these results have not been reported in any previous literature. In the WQS model, we found a positive correlation of mixed BPs with FT3 and TT3 and a negative correlation with FT4, which was more consistent with the results of multiple linear regression. BPA was the greatest weighing chemical responsible for the association, and the weight of BPP was negligible. BPA has the most influential impact on the accumulated chemical mixture index and was the heaviest weighted chemical associated with thyroid function in our study.
Considering that factors such as age and gender may lead to bias in the results, we further stratified these confounding factors. The results of participants aged 3–17 years were inconsistent with those of adults. We did not find any association between thyroid hormones and BPs in adults (Table S13). We found evidence of a negative association between urine BPA levels and serum FT4 levels and a positive association between BPP and TT4 (Table S14). A study of minors aged 8–16 years reported a negative association between serum FT4 and BPA levels (r = −0.483, P < 0.05 (Sur et al. 2019). Another population-based birth cohort study in Rotterdam, the Netherlands, found that maternal exposure to higher BPA during the third trimester of pregnancy led to lower FT4 levels in children (β = −0.11, P < 0.05; (Derakhshan et al. 2021). Opposite results have been reported in minors. The latest study of 386 mother–singleton pairs in a small birth cohort in China found that maternal urinary BPA concentration was positively associated with a 1% (95% CI = 0.20%, 1.92%) increase in cord serum FT4 concentration (Guo et al. 2020). Thus, differences in study design, sample size, type of population, exposure, and covariates all have the potential to contribute to inconsistencies in the results.
Different associations by gender observed between BPA and thyroid hormones in adults and minors (Tables S15 and S16) warrant explanation. A study of children (aged 6 years, N = 574) in Korea reported an associated gender-dependent change, with a significant inverse association between urinary BPs and FT4 observed only among girls (Jang et al. 2021). There is also controversy among different studies regarding the effect of BPA on FT4 levels. In a study of 555 Chinese women in the third trimester of pregnancy, Wang et al. (2020) found that among mothers with higher BMI and higher BPA exposure, compared with those with lower BPA levels in the third trimester, cord serum FT4 was 2.96 (95% CI = 0.12, 5.80) pmol/L higher in male newborns and 2.22 (95% CI = 0.67, 3.78) pmol/L higher in females (Wang et al. 2020). A study in Thailand found a significant inverse association between serum BPA and FT4 levels in men, in contrast to no association observed in women (Sriphrapradang et al. 2013). A study on other environmental contaminants, such as phthalates, also reported sex-dependent associations with thyroid hormones (Park et al. 2017). No clear mechanism explains the sex-dependent association at present, but physiological differences between men and women, such as menstrual and sex hormone differences, may partly explain the differences in association (Hatch et al. 2010; Mahalingaiah et al. 2008). According to the latest research report, the genetic risk score (GRS) for FT4 was associated with increased testosterone and estradiol in women only, while GRS for TSH were found to be associated with increased free androgen in men (Kjaergaard et al. 2021). In addition, the relationship between thyroid hormone levels and TSH has been reported to be related to age, and the pattern of change varies by sex. In males, free hormone concentrations were negatively correlated with age, whereas TSH levels were independent of age; in females, free thyroid hormone concentrations were not affected by age, but TSH levels were positively correlated with age (Suzuki et al. 2012). In addition, a study of 162 mother–child pairs found that prenatal exposure to polybrominated diphenyl ethers (PBDEs) was associated with thyroid hormone alterations in children at 3 years of age, with a gender-dependent relationship. TSH was significantly reduced in females, and FT4 was decreased in males (Vuong et al. 2018).
Overall, some gender-dependent relationships have been found in studies of the effects of multiple pollutant exposure on thyroid hormones. Although the underlying mechanism was unclear, the gender-dependent effects of BPA may be caused by differences in the expression of genes related to lipid metabolism and differences in sex hormones (Babelova et al. 2015).
In our current study, we found evidence for associations between urinary BPA and serum TT3 in Zhejiang adult females. The association was negative, suggesting those with higher BPA concentrations had lower TT3 levels. An experimental study showed that BPA inhibited T3-mediated gene activation in a dose-dependent manner through thyroid receptors alpfa1 (TRalpfa1) and TRbeta. In addition, BPA also upregulated the expression of the T3 suppressor gene. In conclusion, BPA has an antagonistic effect on T3 (Moriyama et al. 2002). In minor females, BPA exposure was associated with lower FT4 and Tg levels. A previous large-scale population study in the USA reported an inverse association between urinary BPA concentrations and serum T4, which supports our results (Meeker and Ferguson 2011). Recent in vivo studies found that neonatal exposure to BPA decreases serum T4 in female rats (Fernandez et al. 2018), but in previous studies, no association between Tg and BPA was observed. Conversely, BPA levels were positively correlated with TPOAb levels, signifying that exposure to BPA increases the likelihood of being positive for TPOAb, and its elevation usually increases the occurrence of autoimmune thyroid disease. A large sample study in Thailand found that TPOAb-positive subjects tended to increase significantly as BPA quartiles increased; however, only the association between BPA and TPOAb positivity was consistent in both men and women (Chailurkit et al. 2016). However, in the current study, the causality leading to BPA exposure to TPOAb positivity and subsequent autoimmune thyroid disease could not be easily determined. We found no significant association between BPA with TSH, and the same results were reported in a study of minors (Meeker and Ferguson 2011). However, there are also studies that reached different conclusions in this regard. For example, one study found a negative association between BPA concentrations and TSH (Brucker-Davis et al. 2011), and a positive association was found for female newborns in another (Derakhshan et al. 2021). This may be because interindividual differences in TSH levels may camouflage true differences due to BPA exposure in small cross-sectional general population studies.
Some current studies have discovered the molecular mechanism of BPA on thyroid function. Previous studies have found that BPA can directly act on the pituitary-thyroid axis, altering the expression of genes involved in thyroid hormone synthesis and the expression of thyroid-specific transcription factors through TTFs, NF-kB, and RAR/RXR cellular pathways (Gentilcore et al. 2013). Studies on rat thyroid microsomes have shown that BPA is a non-competitive inhibitor of the sodium-iodide symporter (NIS), which confirmed that exposure to BPA has a negative effect on thyroid follicular cells (FRTL-5) through inhibition of NIS-mediated iodide uptake and expression of genes involved in thyroid hormone synthesis (Slc5a5, Tpo, Tg, Pax8, Foxe1, Nkx2-1) (Wu et al. 2016). A recent study found that DIO gene polymorphism is the possible mechanism of bisphenols targeting thyroid hormones. For the association between BPA and FT4, they found negative associations for the genotypes DIO1(rs2235544)-CC, DIO2(rs12885300)-CC, and DIO2 (rs12885300)-CT (Abumallouh et al. 2022).
The major strength of the study is its relatively comprehensive measurement of BP monomer types and thyroid function indicators. We evaluated the internal exposure level of residents near the industrial park and compared it with the control area. To the best of our knowledge, this is the first cross-sectional study of the association between BPs and thyroid function in the general population in Zhejiang province. And compared to the traditional analysis method, we also used the WQS model to estimate the association between mixed BPs and thyroid function.
There are also several limitations. First, the cross-sectional observational study design limited the causality that could be observed from the association between BP exposure and thyroid function. Second, lack of investigation of sources of BP exposure, such as BPs ingested through food. Third, we did not collect data of urinary iodine, serum cotinine, and comorbidities, which may have biased the association analysis. Fourth, we did not measure other chemicals in the participants’ urine, which may have affected the reliability of the results. Fifth, we selected a single first-morning spot urine sample for the determination of BP concentrations, which could not fully represent the average body burden of the participants due to BPs’ short half-life (Pollack et al. 2016). Finally, the small sample size may have biased the interpretation of the results due to the large variation between individuals. And due to wide age distribution of the selected population, small sample sizes in subgroups may lead to instability of results.
Conclusion
This study explored the information of 281 individuals aged 3–79 years with BPA and its analogues in Zhejiang, China. BPA, BPS, and BPP were the predominant BPs in urine samples from the general population, and the total BPs were higher in the exposed area than in the control area, albeit at a lower worldwide level. According to the current preliminary study, urinary BPA is negatively correlated with serum TT3 in adult women. In minor females, BPA is negatively correlated with FT4 and Tg but negatively correlated with TPOAb. Mixed BP exposure was positively associated with FT3 and TT3, but negatively associated with FT4. Although our country has reduced the use of BPs, humans still face the risk of exposure to BPs in the environment due to the widespread existence of products containing BPs. So the adverse effects of daily exposure to BPs remain a public health concern. Our findings will contribute to the evidence of potential thyrotoxic effects of BP exposure and their sex-specific effects, and provide scientific basis for population health risk assessment or policy public health measures. Further research is necessary, and the existing findings are controversial. Therefore, more long-term, prospective, large-sample studies considering the interaction of various pollutants are needed to establish a more complete relationship between BP concentration and thyroid function.
References
Aekplakorn W, Chailurkit LO, Ongphiphadhanakul B (2015) Relationship of serum bisphenol A with diabetes in the Thai population, National Health Examination Survey IV, 2009. J Diabetes 7:240–249
Ahn YA, Baek H, Choi M, Park J, Son SJ, Seo HJ, Jung J, Seong JK, Lee J, Kim S (2020) Adipogenic effects of prenatal exposure to bisphenol S (BPS) in adult F1 male mice. Sci Total Environ 728:138759
Aker AM, Ferguson KK, Rosario ZY, Mukherjee B, Alshawabkeh AN, Calafat AM, Cordero JF, Meeker JD (2019) A repeated measures study of phenol, paraben and triclocarban urinary biomarkers and circulating maternal hormones during gestation in the Puerto Rico PROTECT cohort. Environ Health 18:28
Andrianou XD, Gangler S, Piciu A, Charisiadis P, Zira C, Aristidou K, Piciu D, Hauser R, Makris KC (2016) Human exposures to bisphenol A, bisphenol F and chlorinated bisphenol A derivatives and thyroid function. PLoS One 11:e0155237
Babelova A, Burckhardt BC, Salinas-Riester G, Pommerenke C, Burckhardt G, Henjakovic M (2015) Next generation sequencing of sex-specific genes in the livers of obese ZSF1 rats. Genomics 106:204–213
Blanco AM (2020) Hypothalamic- and pituitary-derived growth and reproductive hormones and the control of energy balance in fish. Gen Comp Endocrinol 287:113322
Brucker-Davis F, Ferrari P, Boda-Buccino M, Wagner-Mahler K, Pacini P, Gal J, Azuar P, Fenichel P (2011) Cord blood thyroid tests in boys born with and without cryptorchidism: correlations with birth parameters and in utero xenobiotics exposure. Thyroid 21:1133–1141
Bushnik T, Haines D, Levallois P, Levesque J, Van Oostdam J, Viau C (2010) Lead and bisphenol A concentrations in the Canadian population. Health Rep 21:7–18
Carrico C, Gennings C, Wheeler DC, Factor-Litvak P (2015) Characterization of weighted quantile sum regression for highly correlated data in a risk analysis setting. J Agric Biol Environ Stat 20:100–120
Casas M, Forns J, Martinez D, Avella-Garcia C, Valvi D, Ballesteros-Gomez A, Luque N, Rubio S, Julvez J, Sunyer J, Vrijheid M (2015) Exposure to bisphenol A during pregnancy and child neuropsychological development in the INMA-Sabadell cohort. Environ Res 142:671–679
Chailurkit LO, Aekplakorn W, Ongphiphadhanakul B (2016) The association of serum bisphenol A with thyroid autoimmunity. Int J Environ Res Public Health 13
Chakraborty P, Sampath S, Mukhopadhyay M, Selvaraj S, Bharat GK, Nizzetto L (2019) Baseline investigation on plasticizers, bisphenol A, polycyclic aromatic hydrocarbons and heavy metals in the surface soil of the informal electronic waste recycling workshops and nearby open dumpsites in Indian metropolitan cities. Environ Pollut 248:1036–1045
Covaci A, Den Hond E, Geens T, Govarts E, Koppen G, Frederiksen H, Knudsen LE, Morck TA, Gutleb AC, Guignard C, Cocco E, Horvat M, Heath E, Kosjek T, Mazej D, Tratnik JS, Castano A, Esteban M, Cutanda F et al (2015) Urinary BPA measurements in children and mothers from six European member states: overall results and determinants of exposure. Environ Res 141:77–85
Cui FP, Yang P, Liu C, Chen PP, Deng YL, Miao Y, Luo Q, Zhang M, Lu WQ, Zeng Q (2021) Urinary bisphenol A and its alternatives among pregnant women: predictors and risk assessment. Sci Total Environ 784:147184
De Filippis E, Li T, Rosen ED (2018) Exposure of adipocytes to bisphenol-A in vitro interferes with insulin action without enhancing adipogenesis. PLoS One 13:e0201122
Derakhshan A, Philips EM, Ghassabian A, Santos S, Asimakopoulos AG, Kannan K, Kortenkamp A, Jaddoe VWV, Trasande L, Peeters RP, Korevaar TIM (2021) Association of urinary bisphenols during pregnancy with maternal, cord blood and childhood thyroid function. Environ Int 146:106160
Derakhshan A, Shu H, Peeters RP, Kortenkamp A, Lindh CH, Demeneix B, Bornehag CG, Korevaar TIM (2019) Association of urinary bisphenols and triclosan with thyroid function during early pregnancy. Environ Int 133:105123
EPA, US (2011) Exposure factors handbook: 2011 edition.E P A / 6 0 0 / R-09/052F. National Center for Environmental Assessment, Washington, DC
Farrugia F, Aquilina A, Vassallo J, Pace NP (2021) Bisphenol A and type 2 diabetes mellitus: a review of epidemiologic, functional, and early life factors. Int J Environ Res Public Health 18
Fernandez MO, Bourguignon NS, Arocena P, Rosa M, Libertun C, Lux-Lantos V (2018) Neonatal exposure to bisphenol A alters the hypothalamic-pituitary-thyroid axis in female rats. Toxicol Lett 285:81–86
Frederiksen H, Aksglaede L, Sorensen K, Nielsen O, Main KM, Skakkebaek NE, Juul A, Andersson AM (2013a) Bisphenol A and other phenols in urine from Danish children and adolescents analyzed by isotope diluted TurboFlow-LC-MS/MS. Int J Hyg Environ Health 216:710–720
Frederiksen H, Nielsen JK, Morck TA, Hansen PW, Jensen JF, Nielsen O, Andersson AM, Knudsen LE (2013b) Urinary excretion of phthalate metabolites, phenols and parabens in rural and urban Danish mother-child pairs. Int J Hyg Environ Health 216:772–783
Gentilcore D, Porreca I, Rizzo F, Ganbaatar E, Carchia E, Mallardo M, De Felice M, Ambrosino C (2013) Bisphenol A interferes with thyroid specific gene expression. Toxicology 304:21–31
Guo C, Ren F, Jin J, Zhang H, Wang L, Zhang H, Chen J (2021) Internal exposure of Chinese children from a typical coastal city to bisphenols and possible association with thyroid hormone levels. Environ Int 156:106759
Guo J, Wu C, Zhang J, Li W, Lv S, Lu D, Qi X, Feng C, Liang W, Chang X, Zhang Y, Xu H, Cao Y, Wang G, Zhou Z (2020) Maternal and childhood urinary phenol concentrations, neonatal thyroid function, and behavioral problems at 10 years of age: The SMBCS study. Sci Total Environ 743:140678
Gys C, Ait Bamai Y, Araki A, Bastiaensen M, Caballero-Casero N, Kishi R, Covaci A (2020) Biomonitoring and temporal trends of bisphenols exposure in Japanese school children. Environ Res 191:110172
Hatch EE, Nelson JW, Stahlhut RW, Webster TF (2010) Association of endocrine disruptors and obesity: perspectives from epidemiological studies. Int J Androl 33:324–332
He Y, Miao M, Herrinton LJ, Wu C, Yuan W, Zhou Z, Li DK (2009) Bisphenol A levels in blood and urine in a Chinese population and the personal factors affecting the levels. Environ Res 109:629–633
Heffernan AL, Thompson K, Eaglesham G, Vijayasarathy S, Mueller JF, Sly PD, Gomez MJ (2016) Rapid, automated online SPE-LC-QTRAP-MS/MS method for the simultaneous analysis of 14 phthalate metabolites and 5 bisphenol analogues in human urine. Talanta 151:224–233
Jang Y, Choi YJ, Lim YH, Lee KS, Kim BN, Shin CH, Lee YA, Kim JI, Hong YC (2021) Associations between thyroid hormone levels and urinary concentrations of bisphenol A, F, and S in 6-year-old children in Korea. J Prev Med Public Health 54:37–45
Jiang Y, Li J, Xu S, Zhou Y, Zhao H, Li Y, Xiong C, Sun X, Liu H, Liu W, Peng Y, Hu C, Cai Z, Xia W (2020) Prenatal exposure to bisphenol A and its alternatives and child neurodevelopment at 2 years. J Hazard Mater 388:121774
John N, Rehman H, Razak S, David M, Ullah W, Afsar T, Almajwal A, Alam I, Jahan S (2019) Comparative study of environmental pollutants bisphenol A and bisphenol S on sexual differentiation of anteroventral periventricular nucleus and spermatogenesis. Reprod Biol Endocrinol 17:53
Kang S, Shin BH, Kwon JA, Lee CW, Park EK, Park EY, Kim B (2020) Urinary bisphenol A and its analogues and haemato-biochemical alterations of pregnant women in Korea. Environ Res 182:109104
Kataria A, Levine D, Wertenteil S, Vento S, Xue J, Rajendiran K, Kannan K, Thurman JM, Morrison D, Brody R, Urbina E, Attina T, Trasande L, Trachtman H (2017) Exposure to bisphenols and phthalates and association with oxidant stress, insulin resistance, and endothelial dysfunction in children. Pediatr Res 81:857–864
Kjaergaard AD, Marouli E, Papadopoulou A, Deloukas P, Kus A, Sterenborg R, Teumer A, Burgess S, Asvold BO, Chasman DI, Medici M, Ellervik C (2021) Thyroid function, sex hormones and sexual function: a Mendelian randomization study. Eur J Epidemiol 36:335–344
Larsson K, Lindh CH, Jonsson BA, Giovanoulis G, Bibi M, Bottai M, Bergstrom A, Berglund M (2017) Phthalates, non-phthalate plasticizers and bisphenols in Swedish preschool dust in relation to children's exposure. Environ Int 102:114–124
Larsson K, Ljung Bjorklund K, Palm B, Wennberg M, Kaj L, Lindh CH, Jonsson BA, Berglund M (2014) Exposure determinants of phthalates, parabens, bisphenol A and triclosan in Swedish mothers and their children. Environ Int 73:323–333
Lee I, Park JY, Kim S, An JN, Lee J, Park H, Jung SK, Kim SY, Lee JP, Choi K (2020) Association of exposure to phthalates and environmental phenolics with markers of kidney function: Korean National Environmental Health Survey (KoNEHS) 2015-2017. Environ Int 143:105877
Lee J, Choi K, Park J, Moon HB, Choi G, Lee JJ, Suh E, Kim HJ, Eun SH, Kim GH, Cho GJ, Kim SK, Kim S, Kim SY, Kim S, Eom S, Choi S, Kim YD, Kim S (2018) Bisphenol A distribution in serum, urine, placenta, breast milk, and umbilical cord serum in a birth panel of mother-neonate pairs. Sci Total Environ 626:1494–1501
Li L, Ying Y, Zhang C, Wang W, Li Y, Feng Y, Liang J, Song H, Wang Y (2019) Bisphenol A exposure and risk of thyroid nodules in Chinese women: a case-control study. Environ Int 126:321–328
Liang J, Liu S, Liu T, Yang C, Wu Y, Jennifer Tan HJ, Wei B, Ma X, Feng B, Jiang Q, Huang D, Qiu X (2020) Association of prenatal exposure to bisphenols and birth size in Zhuang ethnic newborns. Chemosphere 252:126422
Liu M, Jia S, Dong T, Han Y, Xue J, Wanjaya ER, Fang M (2019a) The occurrence of bisphenol plasticizers in paired dust and urine samples and its association with oxidative stress. Chemosphere 216:472–478
Liu Y, Yan Z, Zhang Q, Song N, Cheng J, Torres OL, Chen J, Zhang S, Guo R (2019b) Urinary levels, composition profile and cumulative risk of bisphenols in preschool-aged children from Nanjing suburb, China. Ecotoxicol Environ Saf 172:444–450
Machtinger R, Berman T, Adir M, Mansur A, Baccarelli AA, Racowsky C, Calafat AM, Hauser R, Nahum R (2018) Urinary concentrations of phthalate metabolites, bisphenols and personal care product chemical biomarkers in pregnant women in Israel. Environ Int 116:319–325
Mahalingaiah S, Meeker JD, Pearson KR, Calafat AM, Ye X, Petrozza J, Hauser R (2008) Temporal variability and predictors of urinary bisphenol A concentrations in men and women. Environ Health Perspect 116:173–178
Meeker JD, Ferguson KK (2011) Relationship between urinary phthalate and bisphenol A concentrations and serum thyroid measures in U.S. adults and adolescents from the National Health and Nutrition Examination Survey (NHANES) 2007-2008. Environ Health Perspect 119:1396–1402
Mendy A, Salo PM, Wilkerson J, Feinstein L, Ferguson KK, Fessler MB, Thorne PS, Zeldin DC (2020) Association of urinary levels of bisphenols F and S used as bisphenol A substitutes with asthma and hay fever outcomes. Environ Res 183:108944
Mhaouty-Kodja S, Belzunces LP, Canivenc MC, Schroeder H, Chevrier C, Pasquier E (2018) Impairment of learning and memory performances induced by BPA: evidences from the literature of a MoA mediated through an ED. Mol Cell Endocrinol 475:54–73
Milczarek-Banach J, Rachon D, Bednarczuk T, Mysliwiec-Czajka K, Wasik A, Miskiewicz P (2020) Exposure to bisphenol A analogs and the thyroid function and volume in women of reproductive age-cross-sectional study. Front Endocrinol (Lausanne) 11:587252
Moriyama K, Tagami T, Akamizu T, Usui T, Saijo M, Kanamoto N, Hataya Y, Shimatsu A, Kuzuya H, Nakao K (2002) Thyroid hormone action is disrupted by bisphenol A as an antagonist. J Clin Endocrinol Metab 87:5185–5190
Mustieles V, D'Cruz SC, Couderq S, Rodriguez-Carrillo A, Fini JB, Hofer T, Steffensen IL, Dirven H, Barouki R, Olea N, Fernandez MF, David A (2020) Bisphenol A and its analogues: a comprehensive review to identify and prioritize effect biomarkers for human biomonitoring. Environ Int 144:105811
Myridakis A, Fthenou E, Balaska E, Vakinti M, Kogevinas M, Stephanou EG (2015) Phthalate esters, parabens and bisphenol-A exposure among mothers and their children in Greece (Rhea cohort). Environ Int 83:1–10
Nguyen HD (2023) An evaluation of the effects of mixed heavy metals on prediabetes and type 2 diabetes: epidemiological and toxicogenomic analysis. Environ Sci Pollut Res Int 30:82437–82457
Nguyen HD, Kim MS (2022) Cadmium, lead, and mercury mixtures interact with non-alcoholic fatty liver diseases. Environ Pollut 309:119780
Olsen L, Lampa E, Birkholz DA, Lind L, Lind PM (2012) Circulating levels of bisphenol A (BPA) and phthalates in an elderly population in Sweden, based on the prospective investigation of the vasculature in Uppsala Seniors (PIVUS). Ecotoxicol Environ Saf 75:242–248
Ouyang F, Zhang GH, Du K, Shen L, Ma R, Wang X, Wang X, Zhang J (2020) Maternal prenatal urinary bisphenol A level and child cardio-metabolic risk factors: a prospective cohort study. Environ Pollut 265:115008
Pagnin M, Kondos-Devcic D, Chincarini G, Cumberland A, Richardson SJ, Tolcos M (2021) Role of thyroid hormones in normal and abnormal central nervous system myelination in humans and rodents. Front Neuroendocrinol 61:100901
Park C, Choi W, Hwang M, Lee Y, Kim S, Yu S, Lee I, Paek D, Choi K (2017) Associations between urinary phthalate metabolites and bisphenol A levels, and serum thyroid hormones among the Korean adult population - Korean National Environmental Health Survey (KoNEHS) 2012-2014. Sci Total Environ 584-585:950–957
Peinado FM, Lendinez I, Sotelo R, Iribarne-Duran LM, Fernandez-Parra J, Vela-Soria F, Olea N, Fernandez MF, Freire C, Leon J, Perez-Cabrera B, Ocon-Hernandez O, Artacho-Cordon F (2020) Association of urinary levels of bisphenols A, F, and S with endometriosis risk: preliminary results of the EndEA study. Int J Environ Res Public Health 17(4):1194.
Philips EM, Jaddoe VWV, Asimakopoulos AG, Kannan K, Steegers EAP, Santos S, Trasande L (2018) Bisphenol and phthalate concentrations and its determinants among pregnant women in a population-based cohort in the Netherlands, 2004-5. Environ Res 161:562–572
Pollack AZ, Perkins NJ, Sjaarda L, Mumford SL, Kannan K, Philippat C, Wactawski-Wende J, Schisterman EF (2016) Variability and exposure classification of urinary phenol and paraben metabolite concentrations in reproductive-aged women. Environ Res 151:513–520
Quiros-Alcala L, Hansel NN, McCormack M, Calafat AM, Ye X, Peng RD, Matsui EC (2021) Exposure to bisphenols and asthma morbidity among low-income urban children with asthma. J Allergy Clin Immunol 147:577–586.e577
Radwan M, Wielgomas B, Dziewirska E, Radwan P, Kaluzny P, Klimowska A, Hanke W, Jurewicz J (2018) Urinary bisphenol A levels and male fertility. Am J Mens Health 12:2144–2151
Rezg R, Abot A, Mornagui B, Aydi S, Knauf C (2018) Effects of bisphenol S on hypothalamic neuropeptides regulating feeding behavior and apelin/APJ system in mice. Ecotoxicol Environ Saf 161:459–466
Sarzo B, Abumallouh R, Marin N, Llop S, Beneito A, Lopez-Flores I, Ferrero N, Sakhi AK, Ballester F, Lopez-Espinosa MJ (2022) Association between phenols and thyroid hormones: the role of iodothyronine deiodinase genes. Environ Pollut 311:119926
Schirmer E, Schuster S, Machnik P (2021) Bisphenols exert detrimental effects on neuronal signaling in mature vertebrate brains. Commun Biol 4:465
Silva JF, Ocarino NM, Serakides R (2018) Thyroid hormones and female reproduction. Biol Reprod 99:907–921
Sinha RA, Singh BK, Yen PM (2018) Direct effects of thyroid hormones on hepatic lipid metabolism. Nat Rev Endocrinol 14:259–269
Sowlat MH, Lotfi S, Yunesian M, Ahmadkhaniha R, Rastkari N (2016) The association between bisphenol A exposure and type-2 diabetes: a world systematic review. Environ Sci Pollut Res Int 23:21125–21140
Sriphrapradang C, Chailurkit LO, Aekplakorn W, Ongphiphadhanakul B (2013) Association between bisphenol A and abnormal free thyroxine level in men. Endocrine 44:441–447
Sur U, Erkekoglu P, Bulus AD, Andiran N, Kocer-Gumusel B (2019) Oxidative stress markers, trace elements, and endocrine disrupting chemicals in children with Hashimoto’s thyroiditis. Toxicol Mech Methods 29:633–643
Suzuki S, Nishio S, Takeda T, Komatsu M (2012) Gender-specific regulation of response to thyroid hormone in aging. Thyroid Res 5:1
Tai X, Chen Y (2016) Urinary bisphenol A concentrations positively associated with glycated hemoglobin and other indicators of diabetes in Canadian men. Environ Res 147:172–178
Tkalec Z, Kosjek T, Snoj Tratnik J, Stajnko A, Runkel AA, Sykiotou M, Mazej D, Horvat M (2021) Exposure of Slovenian children and adolescents to bisphenols, parabens and triclosan: urinary levels, exposure patterns, determinants of exposure and susceptibility. Environ Int 146:106172
van der Meer TP, van Faassen M, Frederiksen H, van Beek AP, Wolffenbuttel BHR, Kema IP, van Vliet-Ostaptchouk JV (2019) Development and interlaboratory validation of two fast UPLC-MS-MS methods determining urinary bisphenols, parabens and phthalates. J Anal Toxicol 43:452–464
Vassalle C, Parlanti A, Pingitore A, Berti S, Iervasi G, Sabatino L (2021) Vitamin D, thyroid hormones and cardiovascular risk: exploring the components of this novel disease triangle. Front Physiol 12:722912
Vuong AM, Braun JM, Webster GM, Thomas Zoeller R, Hoofnagle AN, Sjodin A, Yolton K, Lanphear BP, Chen A (2018) Polybrominated diphenyl ether (PBDE) exposures and thyroid hormones in children at age 3years. Environ Int 117:339–347
Wang B, Li M, Zhao Z, Lu J, Chen Y, Xu Y, Xu M, Wang W, Wang T, Bi Y, Ning G (2019) Urinary bisphenol A concentration and glucose homeostasis in non-diabetic adults: a repeated-measures, longitudinal study. Diabetologia 62:1591–1600
Wang F, Hua J, Chen M, Xia Y, Zhang Q, Zhao R, Zhou W, Zhang Z, Wang B (2012) High urinary bisphenol A concentrations in workers and possible laboratory abnormalities. Occup Environ Med 69:679–684
Wang X, Tang N, Nakayama SF, Fan P, Liu Z, Zhang J, Ouyang F (2020) Maternal urinary bisphenol A concentration and thyroid hormone levels of Chinese mothers and newborns by maternal body mass index. Environ Sci Pollut Res Int 27:10939–10949
Wormsbaecher C, Hindman AR, Avendano A, Cortes-Medina M, Jones CE, Bushman A, Onua L, Kovalchin CE, Murphy AR, Helber HL, Shapiro A, Voytovitch K, Kuang X, Aguilar-Valenzuela R, Leight JL, Song JW, Burd CJ (2020) In utero estrogenic endocrine disruption alters the stroma to increase extracellular matrix density and mammary gland stiffness. Breast Cancer Res 22:41
Wu Y, Beland FA, Fang JL (2016) Effect of triclosan, triclocarban, 2,2',4,4'-tetrabromodiphenyl ether, and bisphenol A on the iodide uptake, thyroid peroxidase activity, and expression of genes involved in thyroid hormone synthesis. Toxicol In Vitro 32:310–319
wuHu J, Zhao H, Braun JM, Zheng T, Zhang B, Xia W, Zhang W, Li J, Zhou Y, Li H, Li J, Zhou A, Zhang Y, Buka SL, Liu S, Peng Y, Wu C, Jiang M, Huo W et al (2019) Associations of trimester-specific exposure to bisphenols with size at birth: a Chinese prenatal cohort study. Environ Health Perspect 127:107001
Yamazaki E, Yamashita N, Taniyasu S, Lam J, Lam PK, Moon HB, Jeong Y, Kannan P, Achyuthan H, Munuswamy N, Kannan K (2015) Bisphenol A and other bisphenol analogues including BPS and BPF in surface water samples from Japan, China, Korea and India. Ecotoxicol Environ Saf 122:565–572
Ye X, Pierik FH, Angerer J, Meltzer HM, Jaddoe VW, Tiemeier H, Hoppin JA, Longnecker MP (2009) Levels of metabolites of organophosphate pesticides, phthalates, and bisphenol A in pooled urine specimens from pregnant women participating in the Norwegian Mother and Child Cohort Study (MoBa). Int J Hyg Environ Health 212:481–491
Zhang T, Xue J, Gao CZ, Qiu RL, Li YX, Li X, Huang MZ, Kannan K (2016) Urinary Concentrations of Bisphenols and their association with biomarkers of oxidative stress in people living near e-waste recycling facilities in China. Environ Sci Technol 50:4045–4053
Zhang Y, Ling Y, Zhang Y, Zhang F (2019) Research progress on pretreatment and detection of bisphenols in food and environmental samples. Se Pu 37:1268–1274
Acknowledgements
We are thankful to all participants in the ZJHBP study.
Funding
This study was a part of the Zhejiang Human Biomonitoring Program (ZJHBP) of the Zhejiang Center for Disease Control and Prevention, Republic of China, which was supported by the Central Guiding Local Science and Technology Development Fund Projects (No. 2023ZY1024).
Author information
Authors and Affiliations
Contributions
Yang Hu: conceptualization; data curation; formal analysis; investigation; writing—original draft.
Shiming Lai: methodology; formal analysis.
Ying Li: investigation.
Xiaodong Wu: investigation.
Mingluan Xing: formal analysis.
Xueqing Li: investigation.
Dandan Xu: investigation.
Yuan Chen: formal analysis.
Jie Xiang: formal analysis.
Ping Cheng: formal analysis.
Xiaofeng Wang: supervision; funding acquisition.
Zhijian Chen: methodology; conceptualization.
Hao Ding: investigation.
Peiwei Xu: investigation; writing—review and editing; supervision.
Xiaoming Lou: funding acquisition; supervision.
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the Human Ethics Committee of Zhejiang Provincial Center for Disease Control and Prevention.
Consent to participate
All authors and participants have agreed to participate in this study.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
The contents of this study have not been previously published and have not been submitted elsewhere.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 90 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hu, Y., Lai, S., Li, Y. et al. Association of urinary bisphenols with thyroid function in the general population: a cross-sectional study of an industrial park in China. Environ Sci Pollut Res 30, 107517–107532 (2023). https://doi.org/10.1007/s11356-023-29932-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-29932-5