
Abstract
Some heavy metals are associated with periodontitis; whereas most of these associations have focused on individual metal, there are no specific studies on the effects of combined heavy metal exposure on periodontitis. We conducted an analysis on the association between urinary heavy metal exposure and periodontitis in participants aged 30 years and older using multiple logistic regression and Bayesian kernel machine regression (BKMR). This analysis was performed on data from the National Health and Nutrition Examination Survey from 2011 to 2014. The study found that using logistic regression, the 4th quartile of urinary lead and molybdenum and the 3rd quartile of urinary strontium were positively associated with periodontitis compared to the reference quartile after adjusting for covariates. Odds ratio (OR) with 95% confidence interval (CI) was 1.738 (1.069–2.826), 1.515 (1.025–2.239), and 1.498 (1.010–2.222), respectively. The 3rd and 4th quartiles of urinary cobalt were negatively associated with periodontitis, and their ORs and 95% CIs were 0.639 (0.438–0.934) and 0.571 (0.377–0.964), respectively. The BKMR model showed that urinary barium, lead, and molybdenum were positively associated with periodontitis in a range of concentrations and urinary cobalt, manganese, tin, and strontium were negatively correlated with periodontitis. Furthermore, the overall association between urinary heavy metals and periodontitis was positive. Our study provides evidence for an association between exposure to multiple urinary heavy metals and periodontitis. However, further longitudinal studies are needed to explore the specific mechanisms involved.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Periodontitis is the most common irreversible chronic inflammatory disease in the world, which disrupts the oral connective tissue and affects dental support, ultimately leading to tooth loss (Ebersole et al. 2017), in addition to increasing the burden of chronic diseases (Petersen and Ogawa 2012). Periodontitis is the sixth most common human disease, with an overall prevalence of approximately 45–50%. It was estimated that periodontitis would affect above 50% of the global population in the future (Kassebaum et al. 2014). An estimated 42% of Americans who are 30 years of age or older have periodontitis (Eke et al. 2018). In addition to its adverse effects on the oral cavity, periodontitis can also cause mild systemic inflammation that can eventually trigger or exacerbate known chronic inflammatory diseases, such as cardiovascular diseases, including hypertension (Munoz Aguilera et al. 2020), diabetes (Preshaw and Bissett 2019), and Alzheimer’s disease (Liccardo et al. 2020). The development and severity of periodontitis are influenced by a variety of factors, including oral plaque bacteria, lifestyle choices, and environmental factors (Ambili et al. 2014; Bartold 2018; Peres et al. 2019). The onset of periodontitis is strongly influenced by an unhealthy lifestyle, with smoking being one of the most important contributing factors (ALHarthi et al. 2019). Meanwhile, dietary factors are also associated with the degree of periodontitis, with a high intake of carbohydrates and a deficiency of vitamins C and D being risk factors for periodontitis (Chapple et al. 2017). In addition to these factors, previous research has suggested that heavy metal exposure may be related to the onset of periodontitis (Won et al. 2013). Copper and periodontitis have a linear connection, according to a research based on the National Health and Nutrition Examination Survey (NHANES) in the USA, with high copper intake increasing the risk of periodontitis (Li et al. 2022). In the Korean National Health and Nutrition Examination Survey, elevated levels of blood lead (Pb) and blood mercury were associated with the prevalence of periodontitis in men (Kim and Lee 2013). Prior research has focused on single metal exposures; however, we are often exposed to several heavy metals simultaneously, leading to complex interactions.
People live in an environment where heavy metals are widely distributed, including the atmosphere, soil, water, and various manufactured products (Liu et al. 2019; Uchimiya et al. 2020). Due to increased human activity and the excessive release of metals and their compounds into the environment, people are increasingly exposed to various heavy metals for long periods of time. Long-term exposure to heavy metal mixtures can lead to adverse health effects. Heavy metals such as Pb, cadmium (Cd), zinc, and metallothionein may cause oxidative stress and inflammatory responses in tissues and cells (Aziz et al. 2021; Han et al. 2013). Excessive Pb exposure can also significantly affect bone metabolism and the immune system, making individuals more susceptible to periodontitis attacks (Saraiva et al. 2007). The impact of heavy metal exposure on the onset and progression of periodontitis is complex, as it is often compounded by synergistic, antagonistic, or additive effects between heavy metals. Therefore, it is insufficient to attribute the onset of periodontitis to individual metals alone.
Most previous studies have focused on individual metal exposure without considering interactions between different metals, which may lead to biased results (Wang et al. 2018). The possible health implications of simultaneous exposure to several metals and their mixed effects on periodontitis are still incompletely understood. In order to identify environmental risk factors for periodontitis and create more effective public health interventions, it is necessary to quantify the effects of heavy metal exposure. Therefore, it is necessary to perform a risk assessment between metals and periodontitis using a suitable statistical model. For the purpose of analyzing the joint impact of multiple urinary heavy metal exposures on periodontitis, we selected two statistical methods, including multiple logistic regression model and Bayesian kernel machine regression model (BKMR). Among them, the BKMR model can address nonlinear and complex interactions between chemical exposures and provide more accurate results than multiple logistic regression (Bobb et al. 2018). The purpose of our research is to provide evidence from a population that demonstrates the relationship between heavy metal-combined exposure and periodontitis and identify the heavy metals that have the greatest impact on periodontitis onset.
Methods
Study population
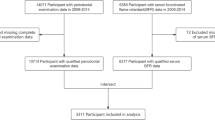
The NHANES, which uses a multi-stage sampling strategy to gather information on the health and nutritional status of adults and children in the USA, is carried out by the National Center for Health Statistics (NCHS), a division of the National Centers for Disease Control and Prevention. A total of approximately 5000 nationally representative samples are collected annually in each county in the USA. The sample of this study consists of two cycles in NHANES (2011–2012 and 2013–2014), since both cycles have complete surveys for periodontitis and heavy metal concentrations. The two cycles were combined, with a total of 19,931 participants. Participants under 30 years of age and lacking data on periodontitis and urine heavy metal measurements and related covariates were not included in this research. Participants are a population that is healthy and free from any comorbidities. The final analysis sample was 2269 participants with complete urine heavy metal examinations as well as periodontitis examinations and related covariate data (Fig. 1).

The flowchart of analytic sample selection
Heavy metal measurements
Thirteen urinary heavy metals (barium (Ba), Cd, cobalt (Co), cesium (Cs), manganese (Mn), molybdenum (Mo), Pb, antimony (Sb), tin (Sn), strontium (Sr), thallium (Tl), tungsten (W), and uranium (Ur)) were included in this study. In NHANES, urine was collected by staff in a subsample, which accounted for one-third of the study population. The urine samples were stored under appropriate freezing conditions and transported to the Laboratory Sciences Division at the National Center for Environmental Health in the USA. The analysis was conducted using an inductively coupled plasma dynamic reaction cell mass spectrometry (ICP-DRC-MS) with the PerkinElmer ELAN DRC II model, manufactured by PerkinElmer, a company based in the USA. No more than 80% of the urine metal concentrations observed in this study were below the limit of detection (LOD). NHANES converted metal concentrations below the detection limit using LOD divided by the square root of 2.
Periodontitis measurement
In the NHANES 2011–2014 “Oral Examinations-Periodontal Examinations” protocol, all periodontal examinations are performed by a dental hygienist at a Mobile Examination Center (MEC) and include measurement of six areas of each tooth (except third molar). Clinical attachment loss (AL) and probing depth (PD), two clinical periodontal measures, were included. Mild periodontitis was defined as ≥ 2 interproximal sites with AL ≥ 3 mm and < 4 mm and ≥ 2 interproximal sites with PD ≥ 4 mm not on the same tooth, or one site with PD ≥ 5 mm. Moderate periodontitis was defined as ≥ 2 interproximal sites with AL ≥ 4 mm and < 6 mm (not on the same tooth), or ≥ 2 interproximal sites with PD ≥ 5 mm (not on the same tooth). Severe periodontitis was defined as ≥ 2 interproximal sites with AL ≥ 6 mm not on the same tooth and ≥ one or more interproximal sites with PD ≥ 5 mm (Eke et al. 2012). Periodontitis was defined as the presence of these signs; otherwise, it was defined as no periodontitis.
Covariates
Based on previous studies (Wang et al. 2018), covariates in this study included sociodemographic characteristics, smoking status, drinking status, serum cotinine, and urinary creatinine. Additionally, considering the association between obesity and metal exposure, we include the body mass index (BMI) as a covariate in the analysis. The family poverty-to-income ratio was divided into three groups (Wu et al. 2020): ≤1.30, 1.31–3.50, and >3.50. Those who have smoked more than 100 cigarettes during their lifetime were considered smokers. Participants were classified as drinkers if they consumed 12 or more cups of alcoholic beverages in any single year. Serum cotinine indirectly responded to environmental tobacco exposure. Age, BMI, serum cotinine, and urinary creatinine were considered continuous variables. More details can be found in Table 1.
Statistical analysis
We used chi-square test and t-test to analyze categorical and continuous variables between the two groups, respectively. For urinary creatinine and serum cotinine, we took the Wilcoxon rank-sum test. The characterization of concentration levels and distribution of heavy metals in both groups were accomplished using geometric means and quartiles. Furthermore, non-parametric test (Kolmogorov-Smirnov test) was conducted to assess disparities in heavy metal levels between the two groups. We performed normality tests for urinary heavy metals, as their distribution was skewed, and we ln-transformed the concentrations of all heavy metals. To determine the correlation coefficients between urine heavy metals, we used the Pearson correlation. Normally distributed continuous variables were expressed as \(\overline{\upchi}\pm S\). The SPSS 23.0 software and R 4.1.0 software were used to process all statistical analyses, considered statistically significant at P<0.05. The SPSS 23.0 software was developed by the International Business Machines Corporation, a company based in the USA.
Multiple logistic regression
NHANES uses a stratified, multilevel probabilistic clustering procedure for sampling to ensure that the sample is representative; we thus weighted for subsamples. The relationship between the prevalence of periodontitis and urine heavy metal concentrations was examined using multiple logistic regression models. Based on previous related studies and theory, we included factors that might have an effect on the results (Wang et al. 2018). In the multiple logistic regression analysis, we fitted 2 models, model 1 without adjusting for any confounding factors and model 2 adjusting for relevant covariates. We log-transformed urinary creatinine so that it was used as an independent covariate rather than creatinine-adjusted concentration (Barr et al. 2005). Among the different urinary heavy metals (except Mn), we used the lowest quartile as a control and the second quartile, third quartile, and fourth quartile to calculate ORs and 95% CIs for the prevalence of the corresponding periodontitis. For urinary Mn, we calculated the corresponding OR and 95% CIs using the tertile. Because the number of urinary Mn below the detection limit is high, using quartile is not appropriate.
Bayesian kernel machine regression (BKMR)
The BKMR model is commonly used in environmental epidemiology to assess the health effects of mixtures of multiple pollutants due to its ability to estimate nonlinear and interacting exposure-response functions (Zhang et al. 2019). The model was performed for 10,000 iterations using a Markov chain Monte Carlo (MCMC) approach. The post-processing functions in this study were obtained from the fitted BKMR model (Bobb et al. 2015). The posterior inclusion probability (PIP) is used to measure the contribution of the components, which is derived from the selection process of the variables fitted to the BKMR. The overall effect of the heavy metals and 95% credible interval was defined as the difference of the estimated risk of periodontitis when all of the heavy metals were fitted at a specific percentile, compared with the median. We fixed all other heavy metals at their median levels and controlled for relevant covariates and then used individual exposure-response function to reflect the relationship between individual urinary heavy metal and periodontitis.
Result
Study population characteristics
The study included a total of 2269 participants, all of whom were 30 years of age or older (Table 1). The mean age of the participants was 53.9 ± 14.7 years. Females occupied 49.4%. The prevalence of periodontitis was estimated at 40.9%. Compared to non-periodontitis participants, periodontitis patients were significantly older, had lower educational attainment, and had lower household income. Statistically significant differences between periodontitis and non-periodontitis participants were found between age, gender, race, education, household PIR, smoking status, serum cotinine, and urinary creatinine, except for BMI (P=0.637) and drinking status (P=0.635). More detailed information is provided in Table 1. Table 2 presents the geometric means, means, and quartiles of urinary heavy metal concentrations in the two studied population groups. The highest geometric mean is observed for Sr (84.77 μg/L). Furthermore, Table 2 highlights notable disparities in heavy metal exposure levels between the two population groups, with the exception of Ba, Co, Mn, and Tl. Notably, individuals with periodontitis exhibit elevated levels of heavy metal concentration in their urine compared to the control group, with Pb and Mo concentrations being particularly pronounced.
Pearson’s correlations among the urinary heavy metal concentrations
Figure 2 shows the heat map of the correlation between the 13 urine heavy metals obtained using the Pearson correlation matrix. We found positive correlations among the 13 urine heavy metals. The correlations between urine heavy metals ranged from a weak correlation of 0.18 to a strong correlation of 0.77. We found the highest correlation between Tl and Cs (r=0.77, P<0.01) and a strong correlation between Pb and Cd (r=0.57, P<0.01).

Pearson’s correlations among the urinary concentrations of 13 heavy metals (N = 2269), NHANES, USA, 2011–2014. Note: **P<0.01
Association between individual urine heavy metal and periodontitis
As shown in Fig. 3A, in the results of the multivariate logistic regression without adjusting for confounders, when the 3rd and 4th quartiles were compared with the reference quartile, urine Co was negatively associated with periodontitis (OR (95% CI): 0.480 (0.311–0.740) and 0.434 (0.268–0.703), respectively), urine Pb was positively associated with periodontitis (OR (95% CI): 1.755 (1.162–2.649) and 2.237 (1.554–3.220), respectively). Urine Sr was positively associated with periodontitis only when the 3rd quartile was compared with the reference quartile (OR (95% CI): 1.680 (1.095–2.578)). After adjustment for relevant confounding factors, as shown in Fig. 3B, the 3rd quartile of urine Pb was no longer associated with periodontitis, while the 4th quartile remained positively associated with periodontitis (OR (95% CI): 1.738 (1.069–2.826)). Similarly, the 3rd and 4th quartiles of urine Co were still negatively correlated with periodontitis (OR (95% CI): 0.639 (0.438–0.934), 0.571 (0.377–0.964), respectively). Among other urinary heavy metals, the 3rd quartile of Sr was associated with periodontitis (OR (95% CI): 1.566 (1.059–2.315)). In addition, the 4th quartile of Mo was positively associated with periodontitis (OR (95% CI): 1.515 (1.025–2.239)).

OR (95% CI) of associations between metals and periodontitis. Quartile 1 was set as the reference. The model was unadjusted (A). The model was adjusted by age, BMI, gender, race, education, family PIR, smoking, drinking, serum cotinine, and log-transformed creatinine (B)
BKMR analysis
The PIPs derived from the BKMR fitting process are summarized as shown in Table 3. Among the 13 urinary heavy metals, Pb had the highest PIPs, indicating that it contributed the most to the effect of periodontitis. The overall association was mostly caused by Pb and Cs (PIPs: Pb=0.9986, Co=0.9648). The univariate exposure-response functions for each urinary heavy metals are shown in Fig. 4. When the other 12 urinary heavy metals were fixed at median levels, we found an S-shaped exposure-response function between Pb and periodontitis. Furthermore, Mo was found to be positively associated with periodontitis, while Co, Mn, Sr, and Sn were negatively associated with periodontitis. Figure 5 shows the mixed effects of the urinary heavy metals on periodontitis from BKMR, and we found a significant positive correlation between urinary heavy metals and periodontitis.

Association and 95% credible intervals for each metal with periodontitis while fixing other metals at their median level. The model was adjusted by age, BMI, gender, race, education, family PIR, smoking, drinking, serum cotinine, and log-transformed creatinine

The overall effect estimates and 95% confidence intervals of the thirteen urinary metal mixtures on periodontitis when metal mixtures were set at a particular percentile (ranging from the 25th to 75th percentiles) compared to the mixtures were held at their 50th percentile, resulting from the BKMR model. The model was adjusted by age, BMI, gender, race, education, family PIR, smoking, drinking, serum cotinine, and ln-transformed creatinine
Discussion
In this study, we analyzed the association between 13 urinary heavy metals and periodontitis. Two datasets (NHANES 2011–2012, NHANES 2013–2014) were selected in this study, which included 2269 Americans aged 30 years and older. Our research findings indicate that concentrations of Co, Mn, Sr, and Sn within specific ranges in urine are negatively associated with periodontitis, whereas concentrations of Pb, Mo, and Ba are positively associated with periodontitis. The results of the multiple logistic regression differ depending on whether the covariates are adjusted or not. This may be due to the inclusion of variables related to periodontitis, which leads to more reliable and accurate results in the regression model.
In addition, the results of the BKMR model were not consistent with the results of the multivariate logistic regression model. It is possible that the BKMR model has the advantage of flexibility in assessing nonlinear associations as well as interactions, thus showing different results. When exposed to total urinary heavy metals, the overall effect was positively correlated with the risk of periodontitis. This shows that heavy metal-combined exposure has a negative effect on periodontitis episodes and that more rigorous management of the corresponding heavy metal concentrations is necessary in the real life. The BKMR model seems to better reflect the actual effect when used to observe the mixed effect of urinary heavy metal exposure on periodontitis. Therefore, the results of this study are more reliable.
Heavy metal exposure to humans is a product of manufacturing and consumption. In nature, Co and its derivatives are abundantly dispersed. Co metal ions are widely distributed trace elements in nature, and their known biological function is as a metal component of vitamin B12 (Strachan 2010). Currently, there is no research elucidating the specific biological mechanism between Co and periodontitis. Previous studies have indicated that low levels of cobalt ions possess anti-inflammatory properties and can prevent IL-1β-induced cartilage degradation (Fu et al. 2020). Furthermore, similar research has demonstrated that cobalt-chromium particles can stimulate the generation of M2 macrophages, elevate the expression level of the anti-inflammatory cytokine IL-10, and, notably, reduce the expression of osteoclast-related transcriptional marker genes, aiding in the reduction of osteoclast numbers (Lu et al. 2023). This may help to explain why there was a negative connection between periodontitis and urine Co levels in this study.
A positive association between Pb exposure and periodontitis was demonstrated in Korean and American studies (Arora et al. 2009; Kim and Lee 2013). In this study, we also confirmed a positive association between urinary Pb exposure and periodontitis in certain concentration levels. And the PIPs of urinary Pb exposure were the largest, which could indicate that Pb has the largest impact on the occurrence and development of periodontitis. Long-term exposure to Pb in the human body can cause various pathological and physiological health disorders (Khalid and Abdollahi 2019). Although the mechanisms regarding the association between Pb exposure and periodontitis are not clear. Numerous studies have found higher levels of oxidative stress indicators in people with periodontitis, pointing to a possible link between the two conditions (Aziz et al. 2013; D'Aiuto et al. 2010). Prolonged exposure to Pb in humans predisposes to the production of reactive oxygen species (ROS), which leads to redox imbalance in the body and causes oxidative stress that severely affects the immune system, which may be a pathway for Pb exposure to affect periodontitis (Ahamed and Siddiqui 2007; Chakraborty et al. 2014). In addition, Pb exposure may affect bone metabolism and the immune system. Pb affects osteocyte and bone matrix synthesis by interfering with calcium metabolism, disrupting bone remodeling and leading to a decrease in bone mass, which damages gingival and periodontal membranes as well as alveolar bone tissue (Khalid and Abdollahi 2020; Tort et al. 2018). Finally, Pb-induced radicals can disrupt the transcription signaling pathway mediated by mitogen-activated protein kinases (MAPKs), resulting in the transcription of inflammatory cytokines such as IL-6 and TNF-α, thereby exacerbating the inflammatory response (Milnerowicz et al. 2015). The above-mentioned reasons explain to some extent the adverse effects of Pb exposure on periodontitis. However, further research is still required to determine the cause-and-effect link between periodontitis and Pb exposure.
In the present study, we found a positive correlation between urinary Mo and urinary Ba concentrations and periodontitis in the BKMR model, and no studies have shown a positive correlation between urinary Mo and urinary Ba and periodontitis, but some studies have found that Mo ions may activate monocytes/macrophages, which in turn contribute to elevated levels of pro-inflammatory cytokines such as IL-6 and TNF-α, which can break osteoclast activity which in turn disrupts bone remodeling and adversely affects periodontal tissues (Caicedo et al. 2009). This may be the reason why urinary Mo concentration is positively correlated with periodontitis. Similarly, it has been shown that metal Ba exposure is positively correlated with oxidative stress indicators (Domingo-Relloso et al. 2019). Oxidative stress is associated with the immune system, and when oxidative damage exceeds the scavenging effect of the body’s antioxidant system, reactive oxygen species are formed leading to redox imbalance. This may affect the onset and progression of periodontitis (Sczepanik et al. 2020). Furthermore, our study found that urinary Mn, Sr, and Sn were negatively associated with periodontitis in the BKMR model. Although Sr was a risk factor for periodontitis in the multiple logistic regression model, urinary Sr was negatively associated with periodontitis over a range of concentrations after fitting by the BKMR model, which is more suitable for environmental pollutant studies. It has been shown that Sr ranelate can reduce the number of osteoclasts and inhibit osteoclast activity, thus protecting the alveolar bone and treating periodontitis (Karakan et al. 2017). This may explain the result that Sr is negatively associated with periodontitis. Previous studies have demonstrated a direct and significant negative correlation between the metal Mn and Sn and periodontitis (Kim et al. 2018; Kim et al. 2014), which is consistent with our findings. Mn is a micronutrient and a cofactor of superoxide dismutase (SOD), and it may be that Mn concentration increases SOD activity and decreases oxidative stress levels, thus reducing the occurrence of periodontitis. Regarding Sn, people are widely exposed to Sn due to the consumption of canned foods (Shimbo et al. 2013), whereas the mechanism of the association between metal Sn exposure and periodontitis is still unclear and needs further study.
In addition, our research has found a positive correlation between co-exposure to heavy metals and periodontitis. Currently, the underlying mechanisms of this co-exposure have not been fully elucidated. Previous studies have suggested that combined exposure to Pb and Cd is associated with systemic immune inflammation. The key mechanism is the excessive production of ROS induced by the co-exposure to Pb and Cd, leading to oxidative stress and subsequent systemic immune inflammation (Zhang et al. 2022). Additionally, co-exposure to heavy metals is associated with arthritis and levels of inflammatory factors (Fang et al. 2023). Different heavy metals may exhibit interactive effects on TNF-α (Luo et al. 2022). These outcomes are similar to our research findings. Metals such as Pb, Ba, and Mo may induce periodontitis through similar biological pathways, such as promoting inflammation, oxidative damage, or increasing osteoclast activity, suggesting potential synergistic or enhanced effects among them. Conversely, Sr and Mn may reduce the number of osteoclasts and levels of oxidative stress, indicating potential antagonistic effects among Sr, Mn, Pb, Ba, and Mo. Therefore, further research is necessary to investigate their potential interactions and biological mechanisms.
The strengths of this study were as follows: First, we utilized a country-representative NHANES sample, which has excellent survey methodology and quality control. Second, we considered the interactions and nonlinear relationships between urinary heavy metals. This revealed, for the first time, the relationship between combined urinary heavy metal exposure and periodontitis. We also assessed the confounding effect between heavy metals and periodontitis using the BKMR model, making the results more reliable. Finally, we took into account possible confounding factors as carefully as possible in each model, thus greatly eliminating confounding bias. Nevertheless, our study has some limitations. First, the NHANES data is cross-sectional, which limits our ability to infer a causal relationship between urine heavy metal exposure and periodontitis. Therefore, a causal relationship cannot be demonstrated. In addition, the NHANES data does not have the regional information, which may be simultaneously associated to the concentrations in urine and the diseases. We were unable to explore this potential relationship in our study. Lastly, diet is one of the most critical factors that affect periodontitis, but NHANES data did not provide us with sufficient dietary information. Therefore, longitudinal studies are necessary to further validate this relationship.
Conclusion
We found that there is a positive trend between the combined exposure to urinary heavy metals and the risk of periodontitis among individuals aged 30 and above in the USA. Additionally, we discovered that the relationship between urinary heavy metals and periodontitis varies depending on the specific type of metal. Our findings need to be confirmed in other longitudinal cohort studies but are of public health importance given the widespread exposure to heavy metals and the high burden of periodontitis. To further understand the biological connections between heavy metals and periodontitis, more research is required.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
References
Ahamed M, Siddiqui MK (2007) Low level lead exposure and oxidative stress: current opinions. Clin Chim Acta 383(1-2):57–64. https://doi.org/10.1016/j.cca.2007.04.024
ALHarthi SS, Natto ZS, Midle JB, Gyurko R, O'Neill R, Steffensen B (2019) Association between time since quitting smoking and periodontitis in former smokers in the National Health and Nutrition Examination Surveys (NHANES) 2009 to 2012. J Periodontol 90(1):16–25. https://doi.org/10.1002/JPER.18-0183
Ambili R, Preeja C, Archana V, Nisha KJ, Seba A, Reejamol MK (2014) Viruses: are they really culprits for periodontal disease? A critical review. J Investig Clin Dent 5(3):179–187. https://doi.org/10.1111/jicd.12029
Arora M, Weuve J, Schwartz J, Wright RO (2009) Association of environmental cadmium exposure with periodontal disease in U.S. adults. Environ Health Perspect 117(5):739–744. https://doi.org/10.1289/ehp.0800312
Aziz AS, Kalekar MG, Suryakar AN, Benjamin T, Prakashan MJ, Ahmed BM, Sayyad M (2013) Assessment of some biochemical oxidative stress markers in male smokers with chronic periodontitis. Indian J Clin Biochem 28(4):374–380. https://doi.org/10.1007/s12291-012-0283-y
Aziz J, Rahman MT, Vaithilingam RD (2021) Dysregulation of metallothionein and zinc aggravates periodontal diseases. J Trace Elem Med Biol 66:126754. https://doi.org/10.1016/j.jtemb.2021.126754
Barr DB, Wilder LC, Caudill SP, Gonzalez AJ, Needham LL, Pirkle JL (2005) Urinary creatinine concentrations in the U.S. population: implications for urinary biologic monitoring measurements. Environ Health Perspect 113(2):192–200. https://doi.org/10.1289/ehp.7337
Bartold PM (2018) Lifestyle and periodontitis: the emergence of personalized periodontics. Periodontol 78(1):7–11. https://doi.org/10.1111/prd.12237
Bobb JF, Claus Henn B, Valeri L, Coull BA (2018) Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ Health 17(1):67. https://doi.org/10.1186/s12940-018-0413-y
Bobb JF, Valeri L, Claus Henn B, Christiani DC, Wright RO, Mazumdar M et al (2015) Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 16(3):493–508. https://doi.org/10.1093/biostatistics/kxu058
Caicedo MS, Pennekamp PH, McAllister K, Jacobs JJ, Hallab NJ (2009) Soluble ions more than particulate cobalt-alloy implant debris induce monocyte costimulatory molecule expression and release of proinflammatory cytokines critical to metal-induced lymphocyte reactivity. J Biomed Mater Res A 9999A:NA–NA. https://doi.org/10.1002/jbm.a.32627
Chakraborty S, Tewari S, Sharma RK, Narula SC, Ghalaut PS, Ghalaut V (2014) Impact of iron deficiency anemia on chronic periodontitis and superoxide dismutase activity: a cross-sectional study. J Periodontal Implant Sci 44(2):57–64. https://doi.org/10.5051/jpis.2014.44.2.57
Chapple IL, Bouchard P, Cagetti MG, Campus G, Carra MC, Cocco F et al (2017) Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol 44(Suppl 18):S39–s51. https://doi.org/10.1111/jcpe.12685
D'Aiuto F, Nibali L, Parkar M, Patel K, Suvan J, Donos N (2010) Oxidative stress, systemic inflammation, and severe periodontitis. J Dent Res 89(11):1241–1246. https://doi.org/10.1177/0022034510375830
Domingo-Relloso, A., Grau-Perez, M., Galan-Chilet, I., Garrido-Martinez, M. J., Tormos, C., Navas-Acien, A., . . . Tellez-Plaza, M. (2019). Urinary metals and metal mixtures and oxidative stress biomarkers in an adult population from Spain: the Hortega study. Environ Int, 123:171-180. https://doi.org/10.1016/j.envint.2018.11.055
Ebersole JL, Dawson D 3rd, Emecen-Huja P, Nagarajan R, Howard K, Grady ME et al (2017) The periodontal war: microbes and immunity. Periodontol 75(1):52–115. https://doi.org/10.1111/prd.12222
Eke PI, Page RC, Wei L, Thornton-Evans G, Genco RJ (2012) Update of the case definitions for population-based surveillance of periodontitis. J Periodontol 83(12):1449–1454. https://doi.org/10.1902/jop.2012.110664
Eke PI, Thornton-Evans GO, Wei L, Borgnakke WS, Dye BA, Genco RJ (2018) Periodontitis in US adults: National Health and Nutrition Examination Survey 2009-2014. J Am Dent Assoc 149(7):576–588 e576. https://doi.org/10.1016/j.adaj.2018.04.023
Fu S, Meng H, Freer F, Kwon J, Shelton JC, Knight MM (2020) Sub-toxic levels of Co(2+) are anti-inflammatory and protect cartilage from degradation caused by IL-1beta. Clin Biomech (Bristol, Avon) 79:104924. https://doi.org/10.1016/j.clinbiomech.2019.12.006
Fang L, Zhao H, Chen Y, Ma Y, Xu S, Xu S et al (2023) The combined effect of heavy metals and polycyclic aromatic hydrocarbons on arthritis, especially osteoarthritis, in the U.S. adult population. Chemosphere 316:137870. https://doi.org/10.1016/j.chemosphere.2023.137870
Han DH, Lee HJ, Lim S (2013) Smoking induced heavy metals and periodontitis: findings from the Korea National Health and Nutrition Examination Surveys 2008-2010. J Clin Periodontol 40(9):850–858. https://doi.org/10.1111/jcpe.12133
Karakan NC, Akpınar A, Göze F, Poyraz Ö (2017) Investigating the effects of systemically administered strontium ranelate on alveolar bone loss histomorphometrically and histopathologically on experimental periodontitis in rats. J Periodontol 88(2):e24–e31. https://doi.org/10.1902/jop.2016.160227
Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W (2014) Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res 93(11):1045–1053. https://doi.org/10.1177/0022034514552491
Khalid M, Abdollahi M (2019) Epigenetic modifications associated with pathophysiological effects of lead exposure. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev 37(4):235–287. https://doi.org/10.1080/10590501.2019.1640581
Khalid M, Abdollahi M (2020) Role of lead in dental diseases. J Environ Sci Health C Toxicol Carcinog 38(4):329–361. https://doi.org/10.1080/26896583.2020.1834313
Kim HS, Cho HJ, Bae SM, Kim YY, Baek SI, Bae KH (2018) Association of periodontitis with the concentration levels of germanium and tin in hair. Biol Trace Elem Res 186(1):68–73. https://doi.org/10.1007/s12011-018-1296-z
Kim HS, Park JA, Na JS, Lee KH, Bae KH (2014) Association between plasma levels of manganese and periodontal status: a study based on the fourth Korean National Health and Nutrition Examination Survey. J Periodontol 85(12):1748–1754. https://doi.org/10.1902/jop.2014.140250
Kim Y, Lee BK (2013) Association between blood lead and mercury levels and periodontitis in the Korean general population: analysis of the 2008-2009 Korean National Health and Nutrition Examination Survey data. Int Arch Occup Environ Health 86(5):607–613. https://doi.org/10.1007/s00420-012-0796-y
Li W, Shang Q, Yang D, Peng J, Zhao H, Xu H, Chen Q (2022) Abnormal micronutrient intake is associated with the risk of periodontitis: a dose-response association study based on NHANES 2009-2014. Nutrients 14(12). https://doi.org/10.3390/nu14122466
Liccardo D, Marzano F, Carraturo F, Guida M, Femminella GD, Bencivenga L et al (2020) Potential bidirectional relationship between periodontitis and Alzheimer’s disease. Front Physiol 11:683. https://doi.org/10.3389/fphys.2020.00683
Liu X, Liang Y, Guo J (2019) Heavy metal pollution in Nanchang City and its health implication on traffic policemen. Environ Sci Pollut Res Int 26(18):17885–17890. https://doi.org/10.1007/s11356-017-0289-3
Luo KH, Tu HP, Yang CH, Yang CC, Chen TH, Chuang HY (2022) Use of generalized weighted quantile sum regressions of tumor necrosis factor alpha and kidney function to explore joint effects of multiple metals in blood. Int J Environ Res Public Health 19(12). https://doi.org/10.3390/ijerph19127399
Lu Y, Xu X, Yang C, Hosseinkhani S, Zhang C, Luo K et al (2023) Copper modified cobalt-chromium particles for attenuating wear particle induced-inflammation and osteoclastogenesis. Biomater Adv 147:213315. https://doi.org/10.1016/j.bioadv.2023.213315
Milnerowicz H, Sciskalska M, Dul M (2015) Pro-inflammatory effects of metals in persons and animals exposed to tobacco smoke. J Trace Elem Med Biol 29:1–10. https://doi.org/10.1016/j.jtemb.2014.04.008
Munoz Aguilera E, Suvan J, Buti J, Czesnikiewicz-Guzik M, Barbosa Ribeiro A, Orlandi M et al (2020) Periodontitis is associated with hypertension: a systematic review and meta-analysis. Cardiovasc Res 116(1):28–39. https://doi.org/10.1093/cvr/cvz201
Peres MA, Macpherson LMD, Weyant RJ, Daly B, Venturelli R, Mathur MR et al (2019) Oral diseases: a global public health challenge. Lancet 394(10194):249–260. https://doi.org/10.1016/s0140-6736(19)31146-8
Petersen PE, Ogawa H (2012) The global burden of periodontal disease: towards integration with chronic disease prevention and control. Periodontol 60(1):15–39. https://doi.org/10.1111/j.1600-0757.2011.00425.x
Preshaw PM, Bissett SM (2019) Periodontitis and diabetes. Br Dent J 227(7):577–584. https://doi.org/10.1038/s41415-019-0794-5
Saraiva MC, Taichman RS, Braun T, Nriagu J, Eklund SA, Burt BA (2007) Lead exposure and periodontitis in US adults. J Periodontal Res 42(1):45–52. https://doi.org/10.1111/j.1600-0765.2006.00913.x
Sczepanik FSC, Grossi ML, Casati M, Goldberg M, Glogauer M, Fine N, Tenenbaum HC (2020) Periodontitis is an inflammatory disease of oxidative stress: we should treat it that way. Periodontol 2000 84(1):45–68. https://doi.org/10.1111/prd.12342
Shimbo S, Watanabe T, Nakatsuka H, Yaginuma-Sakurai K, Ikeda M (2013) Dietary tin intake and association with canned food consumption in Japanese preschool children. Environ Health Prev Med 18(3):230–236. https://doi.org/10.1007/s12199-012-0311-9
Strachan S (2010) Trace elements. Curr Anaesth Crit Care 21(1):44–48. https://doi.org/10.1016/j.cacc.2009.08.004
Tort B, Choi YH, Kim EK, Jung YS, Ha M, Song KB, Lee YE (2018) Lead exposure may affect gingival health in children. BMC Oral Health 18(1):79. https://doi.org/10.1186/s12903-018-0547-x
Uchimiya M, Bannon D, Nakanishi H, McBride MB, Williams MA, Yoshihara T (2020) Chemical speciation, plant uptake, and toxicity of heavy metals in agricultural soils. J Agric Food Chem 68(46):12856–12869. https://doi.org/10.1021/acs.jafc.0c00183
Wang X, Mukherjee B, Park SK (2018) Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003-2014. Environ Int 121(Pt 1):683–694. https://doi.org/10.1016/j.envint.2018.09.035
Won YS, Kim JH, Kim YS, Bae KH (2013) Association of internal exposure of cadmium and lead with periodontal disease: a study of the fourth Korean National Health and Nutrition Examination Survey. J Clin Periodontol 40(2):118–124. https://doi.org/10.1111/jcpe.12033
Wu B, Jiang Y, Jin X, He L (2020) Using three statistical methods to analyze the association between exposure to 9 compounds and obesity in children and adolescents: NHANES 2005-2010. Environ Health 19(1):94. https://doi.org/10.1186/s12940-020-00642-6
Zhang H, Yan J, Niu J, Wang H, Li X (2022) Association between lead and cadmium co-exposure and systemic immune inflammation in residents living near a mining and smelting area in NW China. Chemosphere 287(Pt 3):132190. https://doi.org/10.1016/j.chemosphere.2021.132190
Zhang, Y., Dong, T., Hu, W., Wang, X., Xu, B., Lin, Z., . . . Xia, Y. (2019). Association between exposure to a mixture of phenols, pesticides, and phthalates and obesity: comparison of three statistical models. Environ Int, 123, 325-336. https://doi.org/10.1016/j.envint.2018.11.076
Funding
This manuscript was supported by the Scientific Research Promotion Plan of Anhui Medical University (2021xkjT013), the Projects of Natural Science Research of Anhui Provincial Department of Education (KJ2020A0163), and the Key Project of Nature Science Research Project of Anhui Provincial Department of Education (2022AH050686).
Author information
Authors and Affiliations
Contributions
Zhen-Hua Li and Jiong Li conducted a literature review as well as writing and revising the article. Yi-Cheng Mao helped with data collection and analysis, as well as paper review. Jia-Wen Zhao contributed to the study design and quality assessment. Hui-Yu Hu assisted with the manuscript’s assessment and revision. Sun Zhang and Zhe-Ye Liu assisted in data collection and interpretation. Xue-Jie Liu and Kai Huang assisted with the manuscript revision and gave valuable input.
Xiu-Jun Zhang and Cheng-Yang Hu were in charge of the study’s idea and design, and they also helped to revise the article.
Corresponding author
Ethics declarations
Ethics approval
The application of every technique followed all applicable rules and regulations. The US National Center for Healthcare Statistics (NCHS) granted permission for the 2011–2014 NHANES to be conducted.
Consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, H., Li, J., Mao, YC. et al. Association of urinary heavy metal combined exposure with periodontitis among US adults from NHANES 2011–2014. Environ Sci Pollut Res 30, 107887–107898 (2023). https://doi.org/10.1007/s11356-023-29888-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-29888-6