
Abstract
Objectives
We present data from the Korean National Health and Nutrition Examination Survey 2008–2009 regarding the association between blood lead and mercury levels and periodontitis in a representative sample of the adult South Korean population.
Methods
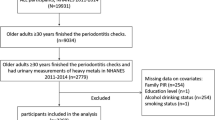
The analysis was restricted to participants ≥20 years of age who completed the health examination survey, including blood lead, cadmium, and mercury measurements (n = 3,966). Odds ratios (ORs) for periodontitis were calculated for log-transformed blood metal levels and quartiles thereof after covariate adjustment.
Results
In a logistic regression analysis using log-transformed blood lead and mercury levels as independent variables after covariate adjustment, including blood lead, mercury, and cadmium, the ORs and 95 % CI values in men for having periodontitis with doubling of blood lead and mercury were 1.699 (1.154–2.503) and 1.394 (1.057–1.838), respectively. Furthermore, in a logistic regression analysis using tertiles of blood lead and mercury as independent variables after covariate adjustment, the ORs and 95 % CIs of men for having periodontitis in the highest tertile were 1.756 (1.184–2.604) and 1.575 (1.507–2.347), respectively. ORs in the logistic regression analysis for men using log-transformed blood cadmium or the tertile of blood cadmium as independent variables after covariate adjustments were not statistically significant in either model. Unlike men, ORs in the logistic regression analyses for women using the same independent variables after covariate adjustment were not statistically significant in any blood metal analysis.
Conclusions
The association between blood lead and mercury levels and periodontitis was significant regardless of the type of variable (continuous or categorical) in the Korean male population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Periodontal disease is a chronic and long-lasting low-grade inflammatory disease (Li et al. 2009). Generally, the term describes diseases that affect the gingiva and cause damage to the supporting connective tissue and bone, which anchor the teeth to the jaws (Williams 1990). Periodontal disease is one of the most common chronic diseases in the world and occurs in at least 35 % of the American population (Albandar et al. 1999). In Korea, the prevalence of periodontal disease is 73.4 % among adults >19 years of age (Korean Center of Disease Control 2009). Several factors are related to an increased risk of periodontal disease, including smoking, diabetes mellitus, osteoporosis, stress, and age (Genco 1996).
Lead, cadmium, and mercury are widely dispersed in the environment. Adults are primarily exposed to these contaminants in the workplace or the general environment. Lead from environmental or occupational sources enters the body by inhalation or other sources of intake (Lockitch 1993). Chronic lead exposure may affect bone metabolism (Pounds et al. 1991; Silbergeld et al. 1993) and possibly the immune system (Pineda-Zavaleta et al. 2004; Pinkerton et al. 1998). This makes lead a potential risk factor for periodontitis, which is a complex multifactorial disease that affects bone and is initiated by an imbalance in the host defense system and the pathogenicity of microorganisms (Offenbacher 1996). Previous population-based studies showed a positive statistically significant association between blood lead and periodontitis after adjusting for major known risk factors using data from the Third National Health and Nutritional Examination Survey (NHANES III), 1988–1994 (Dye et al. 2002; Saraiva et al. 2007). However, there is no corresponding report for other countries.
Inorganic mercury exposure typically produces a syndrome of dermatitis, gingivitis, stomatitis, and tremor, together with central nervous system (CNS) dysfunction (Landrigan 1982). Han et al. (2009) recently showed that mercury exposure was associated with periodontitis in a Korean population living near an industrial complex. However, there is no other report on the subject.
In the present study, we examined the association of periodontitis with increased blood lead and mercury levels while controlling for various confounding variables using a nationally representative sample in Korea.
Methods
Design and data collection
This study was based on data obtained from the KNHANES 2008–2009, representing the second and third years of the KNHANES IV (2007–2009), which used a rolling sampling design involving a complex, stratified, multistage, probability-cluster survey of a representative sample of the non-institutionalized civilian population of South Korea. Detailed information on the design of the survey has been provided previously (Lee and Kim 2012). Briefly, the survey consisted of three components: a health interview survey, health examination survey, and nutrition survey.
The present cross-sectional analysis was restricted to participants ≥20 years of age who completed the health examination survey, including blood lead, cadmium, and mercury measurements (n = 3,996). Information on age, education, smoking history, and alcohol intake was collected during the health interview. Height and weight measurements were performed with the participants wearing light clothing and no shoes. Body mass index (BMI) was calculated as weight in kilograms divided by the square of the height in meters. Obesity was categorized into three groups: lean (BMI < 18.5), normal (18.5 ≤ BMI < 25), and obese (BMI ≥ 25). Age, as reported at the time of the health interview, was categorized into six groups. Education level was categorized into three groups: below high school, high school, and college or higher. Household income was categorized into four groups: < 25 %, 25–49 %, 50–75 %, and >75 % of total house income in the survey. Smoking status was divided into three categories: current smoker, past smoker, and never-smoker. Smoking status was defined based on self-reported cigarette use: never-smokers had smoked fewer than 100 cigarettes in their lifetime, and participants who smoked 100 or more cigarettes were classified as past or current smokers, based on current usage. Alcohol consumption was assessed by questioning the participants about their drinking behavior during the month prior to the interview. The participants were asked about their average frequency (days per month) of alcoholic beverage consumption and amount (in mL) of alcoholic beverages ingested on a single occasion. The responses were converted into the amount of pure alcohol (in g) consumed per day. Alcohol consumption status was categorized into four groups according to average daily alcohol consumption: non-drinker, light drinker (1–15 g), moderate drinker (16–30 g), and heavy drinker (>30 g).
Definition of periodontitis
Periodontitis was defined using the World Health Organization (WHO) community periodontal index (CPI) as a CPI greater than or equal to “code 3.” A CPI score of code 3 indicates that more than one site had a 3.5-mm pocket or larger in the index teeth. Index teeth numbers were 2, 3, 8, 14, 15, 18, 19, 24, and 31, respectively.
Determination of lead, cadmium, and mercury levels in whole blood
To assess the levels of heavy metals in whole blood, 3-mL blood samples were drawn into standard commercial evacuated tubes containing sodium heparin (Vacutainer). Blood lead and cadmium were measured by graphite furnace atomic absorption spectrometry with a Zeeman background correction (AAnalyst 600; Perkin Elmer, Turku, Finland). Blood mercury levels were measured using the gold-amalgam collection method with DMA-80 (Milestone, Bergamo, Italy).
All blood metal analyses were performed by the Neodin Medical Institute, a laboratory certified by the Korean Ministry of Health and Welfare. For internal quality assurance and control, commercial reference materials were used (Lyphochek, Whole Blood Metals Control; Bio-Rad, Hercules, CA, USA). The coefficients of variation were 0.95–4.82 %, 2.65–6.50 %, and 1.59–4.86 % in three reference samples for blood cadmium, lead, and mercury, respectively. As part of external quality assurance and control, the institute passed both the German external quality assessment scheme operated by Friedrich-Alexander University and the Quality Assurance Program operated by the Korea Occupational Safety and Health Agency. The institute was also certified by the Ministry of Employment and Labor as one of the designated laboratories for the analysis of specific chemicals, including heavy metals and certain organic chemicals. The detection limits for blood cadmium, lead, and mercury in the present study were 0.056 μg/L, 0.120 μg/dL, and 0.158 μg/L, respectively. No sample exhibited values below the detection limits of blood cadmium, lead, or mercury.
Statistical analysis
Statistical analyses were performed using the SAS software (ver. 9.22; SAS Institute, Cary, NC, USA) and SUDAAN (Release 10.0; Research Triangle Institute, Research Triangle Park, NC, USA), a software package that incorporates sample weights and adjusts analyses for the complex sample design of the survey. Survey sample weights were used in all analyses to produce estimates that were representative of the non-institutionalized civilian Korean population.
Descriptive statistics were obtained by determining frequency distributions of categorical variables, and their statistically significant differences were analyzed using a χ2 analysis. Blood lead, mercury, and cadmium levels were log-transformed because their distributions were positively skewed. The adjusted geometric mean (GM) with standard error and weighted arithmetic mean (AM) with standard error of laboratory tests and oral health status (the number of active caries and the number of decayed, missing, or filled permanent teeth, [DMFT]) were calculated by periodontitis status using the Proc Descript function in SUDAAN.
Odds ratios (ORs) and 95 % confidence interval (CI) values for periodontitis were calculated for log-transformed blood metal levels and the tertiles thereof after covariate adjustment. Covariates for model 1 were age, residence area, education level, smoking and drinking status, household income, menopause (women only), hemoglobin, glucose, the use of floss or an interproximal tooth brush, the number of DMFT, and number of active caries. Covariates for model 2 included other metals plus those in model 1. For women, menopausal status was added as an additional covariate in both models.
Results
Subject characteristics by classification variables according to the status of periodontitis are shown in Table 1. There were significant differences in the frequency distribution by age, drinking status, education level, and the use of floss or an interproximal tooth brush in both sexes, whereas significant differences were observed in the frequency distribution by smoking status in men and by obesity in women. On the other hand, no difference in the frequency distribution was found according to residence area.
The weighted GM of blood cadmium and lead levels and the weighted AM of age were significantly higher in participants with periodontitis as compared with participants not having periodontitis in both sexes; however, there was no difference in the weighted means of blood mercury and the number of active caries according to periodontal status in either sex. On the other hand, the weighted AM of the number of DMFT was significantly higher in women with periodontitis versus those without periodontitis and the weighted AM of hemoglobin was significantly higher only in men without periodontitis versus those with periodontitis. The weighted AM of blood fasting glucose levels were significantly higher in participants with periodontitis as compared with participants not having periodontitis in both sexes.
ORs and 95 % CI values for periodontitis were calculated for log-transformed blood lead, mercury, and cadmium levels, as well as for tertiles of the three blood metals after covariate adjustment (Table 2). Covariates for model 1 were age, residence area, education level, household income, smoking and drinking status, hemoglobin, glucose, the use of floss or an interproximal tooth brush, the number of DMFT, and number of active caries. Covariates for model 2 included the other two blood metals plus those in model 1. For women, menopausal status was added as an additional covariate in both models.
In a logistic regression analysis using log-transformed blood lead and mercury levels as independent variables after covariate adjustment, the ORs and 95 % CI values in men for having periodontitis with a doubling of blood lead and mercury were 1.854 (1.265–2.716) and 1.456 (1.110–1.910) in model 1 and 1.699 (1.154–2.503) and 1.394 (1.057–1.838) in model 2, respectively. Furthermore, in a logistic regression analysis using tertiles of blood lead and mercury as independent variables after covariate adjustment, the ORs and 95 % CIs in men for having periodontitis in the highest tertile were 1.909 (1.296–2.812) and 1.663 (1.124–2.460) in model 1 and 1.756 (1.184–2.604) and 1.575 (1.507–2.347) model 2, respectively.
On the other hand, ORs in a logistic regression analysis of men using log-transformed blood cadmium or tertiles of blood cadmium as independent variables after covariate adjustment were not statistically significant in either model. In contrast to men, ORs in a logistic regression analysis of women using the same independent variables after covariate adjustment were not statistically significant in any blood metal analysis in either model.
Discussion
The overall GM of blood lead level was 2.306 μg/dL in the Korean general adult population. Exposure to lead has decreased substantially in South Korea since phasing out leaded gasoline in 1986. However, the current blood lead levels in Koreans were higher than 1.43 μg/dL in the recent US NHANES data (CDC 2009). Food and other environmental conditions could contribute to the differences. The overall GM of blood mercury level was 4.480 μg/L in the Korean general adult population. The current blood mercury levels in Koreans were higher than 0.797 μg/L in the recent US NHANES data (CDC 2009). Total blood mercury levels are known to increase with fish consumption (Jarup 2003; Mozaffarian and Rimm 2006). Inorganic mercury exposure such as tooth amalgam treatment or other environmental exposure could contribute to the differences.
In the present study, increased blood lead and mercury levels were associated with the prevalence of periodontitis in men after adjusting for various covariates, including cadmium. Based on ORs, a doubling of blood lead and mercury resulted in a 69.9 and 39.4 % increase, respectively, in the risk of periodontitis in men only. Men in the highest quartile of blood lead and mercury levels were 75.6 and 57.5 % more likely to have periodontitis, respectively, versus those in the lowest quartile. The association between blood lead and mercury levels and periodontitis was significant regardless of the type of variable (continuous or categorical) among men. However, we detected no association between blood cadmium levels and periodontitis. This study also failed to show that blood lead or mercury levels were risk factors for periodontitis in women.
To our knowledge, this is the first reported study to show an association between blood lead levels and periodontitis in any Asian country. This study confirmed the association between blood lead levels and periodontitis reported in the US. Regarding the association between blood lead levels and periodontitis, the mechanism remains unclear. Dye et al. (2002) proposed that periodontal bone loss could contribute to the delivery of lead into the bloodstream, resulting in increased blood lead levels. It is possible that periodontal attachment and bone loss may contribute to increased lead blood levels; however, given the episodic nature of periodontitis, it hardly seems likely that the association found was solely the result of periodontal tissue breakdown. Saraiva et al. (2007) suggested another mechanism. Specifically, chronic lead exposure may affect bone metabolism (Pounds et al. 1991; Silbergeld et al. 1993) and possibly the immune system (Pineda-Zavaleta et al. 2004; Pinkerton et al. 1998). These changes could be potential risk factors for periodontitis, as it is a complex multifactorial disease that affects bone and is initiated by an imbalance in the host defense system and the pathogenicity of microorganisms (Offenbacher 1996). El-Said et al. (2008) also showed that chronic occupational exposure to moderate levels of lead significantly affected oral health conditions among exposed workers and strongly correlated with an increased level of blood lead among them. The most common adverse effects of lead on the dental health of exposed workers were significant increases in the prevalence of periodontal diseases (gingivitis and periodontitis) and decay (caries), missing and filled teeth (expressed as the DMFT index), and dental abrasions. The possible causal relationship between blood lead levels and periodontitis should be studied further.
Inorganic mercury typically produces a syndrome of dermatitis, gingivitis, stomatitis, and tremor, together with CNS dysfunction (Landrigan 1982). Han et al. (2009) recently showed that mercury exposure was associated with periodontitis in a Korean population living near an industrial complex. The findings of Han et al. (2009) were based on a convenience sample in two Korean cities. A convenience sample is based on voluntary participation and may not fully represent the general Korean population, with the potential for biases. The present study reconfirmed an association between blood mercury levels and periodontitis using a representative sample of the general South Korean population (KNHANES). Taken together, blood mercury levels were associated with periodontitis. The association between periodontitis and mercury levels was stronger in males than in females. The present results show that men had higher blood mercury levels than women (GM, 5.422 vs. 3.715 μg/L), and females had a better periodontal health status than males (the prevalence of periodontitis; 18.1 vs. 21.1 %). High body-burden mercury in males might be a contributory factor to stronger association in males. The association shown in males in the present study is consistent with the report of Han et al. (2009), who showed that males with high mercury levels were more likely to have periodontitis than females without high mercury levels. Further, the association between periodontitis and mercury levels was stronger in males than in females.
According to the results of an in vitro study, the cytotoxicity of mercury in human oral fibroblasts was related to its high affinity for intracellular protein thiols (Liu et al. 1992). Once bound to tissue proteins, mercury can cause oxidative stress with subsequent inflammation in biological systems (Shenker et al. 2002). The toxicity of mercury reported in an experimental study showed an association between dental materials and cell death (Reichl et al. 2006). Freden et al. (1974) reported that mercury from dental amalgam accumulated in the gingival tissue adjacent to amalgam fillings. Fibroblasts in the oral mucosa and periodontal tissues accumulate inorganic mercury deposits after exposure (Bolewska et al. 1990). With the accumulation of a high mercury burden in a living environment, a significant number of fibroblasts could be lost due to the cytotoxic effects of mercury, which may aggravate periodontal destruction via immunological pathways.
Considering the public health importance of periodontitis and lead or mercury exposure in the general population, the present study has important public health implications. In addition, this study has several important strengths. First, we used a representative sample of the general South Korean population. Second, rigorous quality controls were applied to the procedures used in the KNHANES. Third, most potential confounders/effect modifiers were considered and adjusted for. These included not only sex, age, residence area, education level, economic status, smoking and drinking status, menopausal status, hemoglobin, oral health status, and behavior, but also blood lead, cadmium, and mercury levels.
However, this study also has some limitations. First, our associations were obtained by cross-sectional analysis, as were those of many previous reports. Thus, we cannot determine any temporal relationship or causality in these associations. We cannot exclude the possibility of reverse causality. The epithelium is often inflamed in periodontitis which indeed might lead to a higher absorption of the metals. A prospective study, in which the metal levels are determined before the development of periodontitis, will be required to establish the causal nature of these associations. In addition, an unknown or unappreciated variable might be the common link that resulted in the observed association. Second, we assessed periodontal status by CPI. Although CPI is an easier way to evaluate periodontal treatment need in community settings, it can overestimate the prevalence of periodontitis because it includes pseudo pockets. In addition, the use of representative teeth may underestimate the prevalence (Saito et al. 2001). Third, KNHANES did not include any data on the number of amalgam fillings which are important source of absorbed mercury. Fourth, KNHANES did not include an occupation/job code to screen lead- or mercury-exposure jobs.
In conclusion, we showed an association between blood lead and mercury levels and periodontitis in the Korean male general population.
References
Albandar JM, Brunelle JA, Kingman A (1999) Destructive periodontal disease in adults 30 years of age and older in the United States, 1988–1994. J Periodontol 70:13–29
Bolewska J, Holmstrup P, Moller-Madsen B, Kenrad B, Danscher G (1990) Amalgam associated mercury accumulations in normal oral mucosa, oral mucosal lesions of lichen planus and contact lesions associated with amalgam. J Oral Pathol Med 19:39–42
Centers for Disease Control and Prevention (CDC) Fourth national report on human exposure to environmental chemicals. CDC, 2009 Available at: http://www.cdc.gov/exposurereport. Accessed May 24 2012
Dye BA, Hirsch R, Brody DJ (2002) The relationship between blood lead levels and periodontal bone loss in the United States. Environ Health Perspect 110:997–1002
El-Said KF, El-Ghamry AM, Mahdy NH, El-Bestawy NA (2008) Chronic occupational exposure to lead and its impact on oral health. J Egypt Public Health Assoc 83:451–466
Freden H, Hellden L, Milleding P (1974) Mercury content in gingival tissues adjacent to amalgam fillings. Odontol Revy 25:207–210
Genco RJ (1996) Current view of risk factors for periodontal diseases. J Periodontol 67:1041–1049
Han DH, Lim SY, Sun BC, Janket SJ, Kim JB, Paik DI, Paek D, Kim HD (2009) Mercury exposure and periodontitis among a Korean population: the Shiwha-Banwol environmental health study. J Periodontol 80:1928–1936
Jarup L (2003) Hazards of heavy metal contamination. Br Med Bull 68:167–182
Korean Center of Disease Center, Ministry of Health and Welfare (2009) Korean national health and examination surveys: the 4th surveys, 2007. Available at: http://knhanes.cdc.go.kr. Accessed December 9 2009
Landrigan PJ (1982) Occupational and community exposures to toxic metals: lead, cadmium, mercury and arsenic. West J Med 137:531–539
Lee BK, Kim Y (2012) Iron deficiency is associated with increased levels of blood cadmium in the Korean general population: analysis of the 2008–2009 Korean National Health and Nutrition Examination Survey data. Environ Res 112:155–163
Li P, He L, Sha YQ, Luan QX (2009) Relationship of metabolic syndrome to chronic periodontitis. J Periodontol 80:541–549
Liu Y, Cotgreave I, Atzori L, Grafstrom RC (1992) The mechanism of Hg2+ toxicity in cultured human oral fibroblasts: the involvement of cellular thiols. Chem Biol Interact 85:69–78
Lockitch G (1993) Perspectives on lead toxicity. Clin Biochem 26:371–381
Mozaffarian D, Rimm EB (2006) Fish intake, contaminants, and human health: evaluating the risks and the benefits. JAMA 296:1885–1899
Offenbacher S (1996) Periodontal diseases: pathogenesis. Ann Periodontol 1:821–878
Pineda-Zavaleta AP, Garcia-Vargas G, Borja-Aburto VH et al (2004) Nitric oxide and superoxide anion production in monocytes from children exposed to arsenic and lead in region Lagunera, Mexico. Toxicol Appl Pharmacol 198:283–290
Pinkerton LE, Biagini RE, Ward EM et al (1998) Immunologic findings among lead exposed workers. Am J Ind Med 33:400–408
Pounds JG, Long GJ, Rosen JF (1991) Cellular and molecular toxicity of lead in bone. Environ Health Perspect 91:17–32
Reichl FX, Esters M, Simon S et al (2006) Cell death effects of resin-based dental material compounds and mercurials in human gingival fibroblasts. Arch Toxicol 80:370–377
Saito T, Shimazaki Y, Koga T, Tsuzuki M, Ohshima A (2001) Relationship between upper body obesity and periodontitis. J Dent Res 80:1631–1636
Saraiva MC, Taichman RS, Braun T, Nriagu J, Eklund SA, Burt BA (2007) Lead exposure and periodontitis in US adults. Periodontal Res 42:45–52
Shenker BJ, Pankoski L, Zekavat A, Shapiro IM (2002) Mercury-induced apoptosis in human lymphocytes: caspase activation is linked to redox status. Antioxid Redox Signal 4:379–389
Silbergeld EK, Sauk J, Sommerman M et al (1993) Lead in bone: storage site, exposure source, target organ. Neurotoxicology 14:225–236
Williams RC (1990) Periodontal disease. N Engl J Med 322:373–382
Conflicts of interest
The authors declare they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, Y., Lee, BK. Association between blood lead and mercury levels and periodontitis in the Korean general population: analysis of the 2008–2009 Korean National Health and Nutrition Examination Survey data. Int Arch Occup Environ Health 86, 607–613 (2013). https://doi.org/10.1007/s00420-012-0796-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-012-0796-y