
Abstract
Safe drinking water is directly linked to good human health. An excessive amount of manganese (Mn) in drinking water supplies causes people show symptoms of neurotoxicity. In this study, the level of Mn in potable water sourced from tube wells located in 9 (nine) districts of Bangladesh was monitored. In total, 170 (one hundred and seventy) water samples were collected and Mn was quantified by atomic absorption spectroscopy (AAS). The levels of Mn found in the tube well water samples of Sirajganj, Meherpur, Chuadanga, Jhenaidah, Magura, Faridpur, Jashore, Satkhira, and Khulna were 0.37–1.86, 0.10–4.11, 0.30–0.76, 0.26–0.94, 0.01–0.18, 0.21–1.78, 0.08–1.23, 0.05–0.27, and 0.01–2.11 mg/L, respectively. Results revealed that Mn level was beyond the highest contaminated levels of 0.1 mg/L and 0.4 mg/L, which are recommended by Bangladesh Drinking Standard (BDS) and World Health Organization (WHO), respectively. The maximum Mn contaminated level reached up to 4.11 mg/L (mean, 0.53 mg/L). The Mn level in tube well water exceeded 51.1% and 75.9% set by the recommended value of WHO and BDS, respectively. Furthermore, the calculated hazard quotient (HQ) value for Mn was observed to be greater than unity, indicating both children and adults risked potential non-carcinogenic health issues. The water supply authorities should take steps to provide Mn-free drinking water for communities.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Drinking water is essential for people to maintain good health. In safe drinking water, a trace level of essential minerals is necessary for proper bodily functioning. Too little or too much in the way of mineral levels will badly affect human health. In Bangladesh, groundwater is the main source of drinking water. A few parts of the coastal area such as the Bagherhat and Satkhira districts use harvested rainwater for drinking purposes (Islam et al. 2019). Impurities of trace elements in potable water are one of the major health concerns particularly for children because they might pose toxic metals. A specific matter of concern is that the higher amount of manganese (Mn) in the drinking water can induce to develop many disease and impairment of the body function (Avila et al. 2013; Grandjean and Landrigan, 2006; Guilarte and Chen, 2007), which reflect the importance of measuring Mn in potable water and health risk assessment through consumption.
Manganese is widely disseminated in the biosphere in a combined state. It is the 12th most abundant element and forms almost 0.1% of the Earth’s surface (Bouchard et al. 2007; Keen et al. 2013). It is an indispensable element for the human body (Aschner et al. 2007) so that various physiological processes function properly (Erikson et al. 2005). For the immune system’s good functioning, Mn plays an essential role (Erikson and Aschner, 2003). It acts as a constituent of metalloenzymes (Keen et al. 2013). However, exposure to high amounts of Mn can be neurotoxic. Many studies of Mn exposures in children and associated adverse neurodevelopmental outcomes is well documented (Grandjean and Landrigan 2014, Lucchini et al. 2017, Rodriguez-Barranco et al. 2013; Keen et al. 2013; Wasserman et al. 2006). High Mn exposure can cause cognitive (Roels et al. 2012), Parkinson, psychiatric, and memory impairment (Grandjean and Landrigan, 2006; Guilarte and Chen, 2007). Manganese can also cause Alzheumer’s disease, Huntington’s disease, amyotrophic lateral sclerosis, mitochondrial dysfunction, astrocytosis, genotoxicity, etc. (Ghosh et al. 2020; Avila et al. 2013). Manganese is a well-known occupational toxicant, causing a depletion of brain dopamine and a syndrome of motor dysfunction and memory loss resembling Parkinson disease (McMillan, 1999). The concentration of Mn at 0.14 mg/kg/day as an oral reference doses (RfDo) can develop critical neurotoxicity (ATSDR, 2012), although this value sometimes considered to 0.047 mg/kg/day for association with Mn toxicity through consumption of drinking water (Brown et al. 2009). When peoples are exposed at elevated level of Mn through intake of drinking water, they might be of greater health risk due to the rapid absorption of Mn in the intestine and enter into blood cells (Chen et al. 2018). Potential neurological effects and/or behavior problems are reported in children following oral exposure to elevated levels (0.4 mg/L) on Mn consumption (Woolf et al. 2002; Sahni et al. 2007).
Usually, Mn in the groundwater ranges from 1 to 100 μg/L (Keen et al. 2013). However, the value may varies due to nature of the environments, such as Mn concentrations reported up to 1300 g/L in neutral groundwater and 9600 g/L in acidic groundwater (ATSDR, 2012). Many countries, for example, those in the European Union, UK, Canada, USA, and Japan recommended that Mn in potable water should be no more than 50 μg/L (Iyare, 2019); yet, in Bangladesh, it is 100 μg /L (ECR 1997). Bowler et al. (2006) reported that anthropogenic activities are responsible for Mn exposure, which might be the source of damage done to the central peripheral nervous systems. The Mn level in groundwater is increasing gradually which is an issue of concern globally (Bouchard et al. 2018; Groschen et al. 2009). Some recent studies investigated many factors (urbanization and industrialization, mining activities and landfill leaching, rock and soil weathering, industrial discharges, leakage of wastewater sewages, corrosion of pipes, temperature, pH, decomposition of organic matter, and reduction of iron (Fe) as well as many other hydrological and geological factors) that influence the release of Mn in drinking water (WHO 2020; Hou et al. 2020; Zhang et al. 2020, Kohl and Medlar, 2006; Ljung and Vahter, 2007). Of these, the main sources of Mn are from industrial activities including Fe and steel-alloys production, as an ingredient in various products such as fertilizers and pottery glazes, dry-cell batteries, glass and fireworks, burning of organo-manganese compounds–containing petrol, power plants, coke ovens, handloom industry, dyeing printing, and painting industry, textile industry, and from mining operations (William-Johnson and World Health Organization, 1999; USEPA, 2004; Stokes et al. 1988). Manganese can also be used as an impurity in coagulant production (such as ferric-based coagulants) for drinking water treatment. Hasan and Ali (2010) reported that the occurrence of Mn in groundwater of Bangladesh has consequences for as benign water supply. It is stated that environmental exposure to Mn causes human health risks (O’Neal and Zheng, 2015) and Mn in potable water increases the rate of all cancers (Spangler and Reid, 2010).
Various factors, for example, the concentration of Mn and competition of other metals, are responsible for Mn absorption by the gastrointestinal tract (Aschner and Aschner, 2005). Typically, Mn in food products ranges from 0.4–20 μg/g (Keen et al. 2013). Drinking water contaminated by Mn poses can endanger children’s health and especially the nervous system (Frisbie et al. 2012). Children who are exposed to Mn higher than 400 μg/L achieved poorer education outcomes compared to those with less Mn in their body (Khan et al. 2012). Bouchard et al. (2007) reported the positive correlation to hyperactive classroom behavior of 46 children (24 boys and 22 girls) between ages of 6 and 15 years (mean 11 years) association with Mn in drinking water in one study from Quebec (Canada). Thus, Mn in drinking water is a potential threat for children. Wasserman et al. (2006) discovered that the consumption of larger amounts of Mn in water (mean, 800 μg/L) by children at the age of 10 years resulted in them showing notably lower intelligence quotient (IQ). Many researchers stated that Mn is a poisonous substance that causes shortfalls in learning and IQ in children (Ericson et al. 2007; Henn et al. 2011; Yousef et al. 2011; Riojas-Rodriguez et al., 2010; Menezes-Filho et al. 2011; Kim et al. 2009; Wright et al. 2006). Kullar et al. (2019) reported a 1% and 2% of decreasing IQ with intake of Mn concentration of 133 μg/L and 266 μg/L, respectively. Moreover, during pregnancy, a higher Mn level causes low fetal weight and risk of increase infant mortality (Zota et al. 2009; Hafeman et al. 2007; Spangler and Spangler, 2009). Rahman et al. (2015) reported that the presence of high Mn (56–1496 μg/L) via consumption of drinking water decrease hemoglobin concentration and impaired fetal growth during pregnancy. Newborn babies are extremely vulnerable to exposed high level of Mn in drinking water by disrupting intellectual development during pregnancy. Hafeman et al. (2007) reported that amongst the 3824 new born infant, 335 was died before reaching 1 year of age due to the consumption of Mn in drinking water at concentrations ≥0.4 mg/L. In a study report in North Carolina (USA), Spangler and Spangler (2009) showed that for every log increase of Mn in drinking water, 2.1 increase of infant death per 1000 lives birth after with low birth weight.
Therefore, this study aims to examine the Mn level in potable water of the Sirajganj, Meherpur, Chuadanga, Jhenaidah, Magura, Faridpur, Jashore, Satkhira, and Khulna districts of Bangladesh, in order to ensure safe drinking water. These regions are currently experiencing increasing Mn contamination in drinking water due to its geology, hydrogeology, enormous industrialization, and many other anthropogenic activities. The children is considered as the most vulnerable and can be affected (especially neurodevelopment and behavior problems) by Mn-rich water even below the provisional guideline value of World Health Organization (WHO). Therefore, the obtained data were compared with the allowable limit (0.4 mg/L) of WHO (WHO, 2017; Cotruvo, 2017)) as well as national drinking water standard (0.1 mg/L) of Bangladesh (BDS). This monitoring study is very crucial to improve public awareness of Mn contamination in the drinking water around the world.
Materials and methods
Reagents
In all experiments, the stock solution was prepared from the analytical reagent (AR). The standard Mn solution was purchased from Fluka-Analytical, Switzerland.
Description of the study area
The study area was randomly selected based on previously reported and recognized as a contaminated area by different types of heavy metals (Chakraborti et al. 2010; Mohana et al. 2020; Ghosh et al. 2020; Rahman et al. 2016). The tube well water is the major sources for drinking and other domestic uses in the study area (Mohana et al. 2020). Industrialization and urbanization significantly developing at the site, which could impact background level of Mn. The randomly selected area is rural which is located at southwestern part of Bangladesh except Sirajgonj (north central and situated on the bank of Jamuna river; one of the main three rivers in Bangladesh) and is experiencing the most natural disaster prone areas in Bangladesh (Didar-Ul Islam et al., 2015; Akter et el. 2010; BBS 2015). Sirajgonj is also known as a flood prone and river erosion zone (BBS 2015); and Khulna (is known as western coastal zones (crossing the Rupsha and Bhairab river), which is connected to the Bay of Bengal and covered by the Sundarbans mangrove forest (BBS 2015; Hossain et al. 2014). The population density in Sirajganj, Chuadanga Sadar, Meherpur Sadar, Magura (Mohammadpur), Jhenaidah (Shailkupa), Faridpur (Alfadanga and Bhanga), Jashore Sadar, Khulna (City Corporation), and Satkhira Sadar are 1290/km2, 1052/km2, 929/km2, 890/km2, 968/km2, 1025/km2, 1707/km2, 16,268/km2, and 1156/km2, respectively (BBS 2013 and 2015). The total population of study area is reported to be 6,559,124, where number of males and females are 3,296,869 and 3,262,255, respectively (BBS 2013). The children below 10 years age are estimated to 1,371,572 and the total males and females above 10 years age are 5,187,552 in the studied areas (BBS 2013). Generally, in rural areas in Bangladesh, a tube well is utilized for 50–100 families in which on average each family consists of 7 (seven) members. However, this value may increase due to the scarcity of potable water. Detail information on population distribution can be found in supplementary Table S1. During each sample collection, the survey personnel met with a local administrative officer to gather information on the village demography and then randomly selected households’ tube well where samples were collected.
Water sample collection and analysis
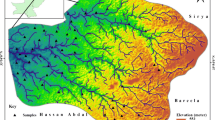
Tube well (TW) water samples were collected from 9 (nine) randomly selected districts in Bangladesh, specifically Sirajganj, Meherpur, Chuadanga, Jhenaidah, Magura, Faridpur, Jashore, Satkhira, and Khulna. A total 170 (one hundred and seventy) water samples were selected by randomized trial for this preliminary Mn-induced health-based study. Considering the facts that of the natural calamity, flood prone, unstable hydrology, unplanned industrialization as well as population density makes the Sirajgonj and Khulna most vulnerable, and therefore, a relatively higher volume of samples was collected from these two sites compared to other areas (Didar-Ul Islam et al., 2015; Akter et el. 2010; BBS, 2015). However, population density in Jashore sadar is higher than Sirajgonj, a higher size of samples were selected from Sirajgong due to considering the more vulnerability aspects. From each district, a different number of TW water samples were put into plastic 500-mL high-density polyethylene (HDPE) bottles acidified with 1% nitric acid (Merck KGaA, Germany) from the tube well. Before collecting the water samples from the TW, for the first 10–15 min (depending on the depth), water was allowed to run so that a steady stream flow of water from the aquifer water layer was possible. Water samples were collected and identified as follows: Sirajganj (40): SJ01 to SJ40, Meherpur (10): MHR01 to MHR10, Chuaganga (10): CA01 to CA10, Jheniadah (10): JH01 to JH10, Magura (10): MR01 to MR10, Satkhira (12): SA01 to SA12, Faridpur (10): FR01 to FR10 (10), Jashore (26): JE01 to JE26, and Khulna (42): KN01 to KN42. The sample identification (ID) of these 9 (nine) districts is depicted in Table 1, Table 2, Table 3, Table 4, Table 5, and Table 6, and the sampling location is shown in Fig. 1. The water samples were preserved at 4 °C until required for analysis. The Mn was quantified employing atomic absorption spectroscopy (SpectrAA220, Varian, Australia) with direct flame (air-acetylene) at the wavelength of 279.5 nm (Rahman et al. 2016; Rahman et al. 2019).

Study area in Bangladesh (A), and Sampling locations in nine districts (B)
Health risk calculation
The recommended USEPA (2011) method was applied to assess the chronic daily intake (CDI) of Mn and HQ for both children and adults. Equation (1) served for calculating the CDI:
Here, C indicates the true Mn concentration in groundwater (mg L−1), IRwater represents the water ingestion rate which was considered to be 2.1 L day−1 for children and 3.5 L day−1 for adults (Hossain et al. 2013), EF indicates the exposure frequency (365 days year−1), ED represents exposure duration (10 and 70 years for children and adults, respectively), BW means body weight of children (<15 years) and adults (≥15 years) which are approximately 31.97 kg and 50 kg, respectively (NCHS 2000; Ghosh et al. 2020); AT is the average time (365 × 10 = 3650 days for children and 365 × 70 = 25,550 days for adults).
The HQ was assessed using the following equation (USEPA, 2004):
RfDo refers to the oral reference dose (mg kg−1 day−1) and the RfDo for Mn was 0.14 mg kg−1 day−1 (USEPA, 2020). HQ < 1 means that the population is safe from certain harmful effects over a lifetime of Mn exposure, but HQ >1 stands for adverse non-carcinogenic health effects felt by the population exposed to Mn.
Quality control and data analysis
The limit of detection (LOD) of the atomic absorption spectroscopy (AAS) for Mn was determined to be 9.0 μg/L, which was obtained from 3 (three) times the standard deviation (SD) of the blank responses. Certified reference material (CRM), blanks, duplicates, and continuing calibration verification (CCV) were conducted after every 10 samples throughout the Mn analysis. The mean recovery (n = 10) from CRMs (TraceCERT, Sigma-Aldrich) was within the 85–104% range, thus confirming the accuracy of the Mn analysis. For plotting of the graph, figures, and statistical data analysis, we used Excel 2016, Adobe Photoshop elements 12, and Origin8 Software.
Results and discussion
The mean Mn level was 0.53 mg/L (range 0.01–4.11 mg/L) which exceeded 1.3 and 5.3 times the recommended levels of WHO (0.4 mg/L) and BDS (0.1 mg/L), respectively (Table 1).
Mn in TWs water of Sirajganj district
Table 2 shows the Mn in TWs water of Sirajganj district in the TW. It seems that all (40) of the tested samples’ Mn level exceeded the BDS level, which represents human health concern. The largest and smallest amount of Mn in TWs water was found in samples SJ33 (1.86 mg/L) and SJ31 (0.37 mg/L), respectively. In the meantime, 95% (38 out of 40) of TWs water Mn level was beyond the WHO (2008) guideline (0.4 mg/L). It implies that the Mn level was 1.03–4.65 times higher than the WHO guideline and 3.7–18.6 times higher than the BSD (0.1 mg/L) value (ECR, 1997). In contrast to BIS (2012), there was no acceptable (0.1 mg/L) and permissible (0.3 mg/L) Mn level of the tested TW water samples. The worst groundwater and TWs in Sirajganj district have been consistently reported over a long period of time, due to it being a severe flood-affected area and the many industries do not dispose of their waste in a planned way (Ali et al. 2019; Akter et al. 2010). Uddin et al. (2019) reported that a Mn concentration (1.58 mg/L) was considered hazardous for both drinking and irrigation in the Sirajganj district, whereas Akter et al. (2010) reported high Mn concentration (3.58 mg/L) in the industrial effluents (from handloom cottage, textile, dyeing, and printing) in the Belkuchi, Sirajganj that could impact TWs and subsequent human health. Hou et al. (2020) reported many factors for the elevated level of Mn in groundwater. Therefore, both natural and anthropogenic sources contribute to the concentration of Mn in TWs in the investigated area.
Mn in TWs water of Meherpur and Chuadanga district
Table 3 represents the Mn level that exists in Meherpur district. It appears that this Mn level ranged from 0.10 to 4.11 mg/L. The maximum and minimum Mn in TWs water were found in the samples MHR04 and MHR06, respectively. Referring to the Mn in TWs water samples from MHR06, MHR07, MR08, and MHR10, these exceeded the WHO guideline. In fact, it is indicated that 40% (4 out of 10) TWs water sample exceeded the WHO guideline. It also clear that Mn in TW water sample from MHR06 was 10.3 times higher than the WHO permissible level, which can negative impact on human health. On the other hand, except for MHR02 and MHR04, the remaining TWs had a Mn level greater than the BDS. However, 80% (8 out of 10) and 40% (4 out of 10) TWs water samples’ Mn concentration in the Meherpur district found above the BDS and WHO level, respectively. Hasan and Ali (2010) reported the Mn concentration (0.806–1.336 mg/L) for the 17 most contaminated districts including Meherpur, 1.34 mg/L (maximum). However, the sources of Mn in TWs of the investigated area could be due to the ground flow of the Padma River (close to the sampling area), irrigation, industrialization, etc. Hou et al. (2020) reported river network areas do influence the amount of Mn released in groundwater.
Two TWs water samples in Chuadanga district (CA04 and CA10) had a Mn level below the WHO guideline value (Table 3). The other 8 (eight) TWs water samples showed Mn level above the WHO guideline value. Conversely, all the TWs water samples’ Mn level exceeded the BDS limit several times. It is noted that 90% (except CA10) of the TWs water samples had Mn levels beyond what was permissible. The Mn in all TWs water samples crossed the acceptable limit (BIS, 2012).
Mn in TWs water of Jhenaidah and Magura district
The maximum and minimum concentration of Mn were 0.94 and 0.26 mg/L found in TWs water samples of JH08 and JH05, respectively (Table 4). Ninety percent (9 out of 10) of TWs water samples exceeded the WHO guideline value and all the water samples Mn level was above the BDS level (ECR, 1997). It appears that the Mn level was 26 to 94 times higher than the BDS level, which causes obvious detrimental to human health.
The Mn in TWs water samples from the Magura district are summarized in Table 4. The Mn level was ranged between 0.01 to 0.18 mg/L. Here, all the TWs water samples indicated a Mn level below the WHO recommendation level. Two TWs water samples (MR08 and MR10) were greater than the allowable limit of Mn level recommended by BDS and the rest of the TWs water samples Mn was below the BDS value.
Geologically, there are many oxbow lakes (baors) in Jhenaidah and Magura districts and the decomposition of different biomass could influence the Mn released to the groundwater. Rahman et al. (2016) reported Mn concentrations of 10–370 μg/L in TWs of different primary schools in Magura districts. Our findings are within that range. Hasan and Ali (2010) reported relatively more Mn (~0.971 mg/L) in the groundwater of Magura district.
Mn in TWs water of Satkhira and Faridpur districts
Table 5 depicts the Mn in TWs water of Satkhira district and the Mn content spanned from 0.05 to 0.27 mg/L. The Mn level in all the tested TWs water samples was below the WHO guideline value and 66.7% (8 out of 12) of TWs water surpassed the BDS stipulation in Satkhira district. In contrast to BIS (2012), 8 (SA01, SA02, SA04, SA05, SA07, SA08, SA10, and SA12) TWs water samples, the Mn level was below the permissible level, while the remaining 4 (SA03, SA06, SA09, and SA11) TWs water samples had acceptable Mn levels.
Satkhira is situated in the coastal belt region and recognized as one of the most vulnerable areas in Bangladesh in terms of safe drinking water (Didar-Ul Islam et al., 2015, Hasan et al. 2018). Hasan et al. (2018) reported a Mn concentration 0.6 mg/L in the groundwater of the Khulna-Satkhira coastal belt region. Aktaruzzaman et al. (2013) reported Mn (0.129–0.195 mg/L) in water and sediments (13.6–24.0 mg/L) in the shrimp farms operating in Satkhira district. Hydrological and hydrogeological factors mainly contribute to the release of Mn in TWs in this region.
Similarly, Mn in TWs water of the Faridpur district is summarized in Table 5. Results describes that the maximum and minimum Mn concentration were determined to be 1.78 and 0.21 mg/L, in sample FR02 and FR01, respectively. Only two TWs water samples (FR02 and FR08) were the Mn within the WHO permissible level and 80% TWs water samples contained Mn greater than the WHO guideline value. Results revealed that the Mn content in TWs water samples were above the permissible level of Bangladesh drinking water quality standard in Faridpur district. The chronic exposure by consumption of high Mn exposure could affect human health in this area. It is clear that the concentration of Mn in TWs water was 21 to 114 times higher than the BDS values. Except for the TW water sample FR01, the remaining TWs water samples contained Mn beyond the permissible level of BIS (2012). Hasan and Ali (2010) reported a maximum Mn concentration in the Faridpur district’s groundwater of 0.806 mg/L and this is similar to our findings.
Mn in TWs water of Jashore district
Table 6 shows the Mn level at the district of Jashore. The highest and lowest level of Mn was found at 0.08 (JE01) and 1.23 mg/L (JE18), respectively. Except for two (JE15 and JE18), 92.3% (24 out of 26) water samples Mn concentration crossed the BDS level. Ghosh et al. (2020) reported that 87% of TW samples in the Jashore district exceeded the BDS value. On the other hand, the amount of analyzed Mn was closer to the WHO guideline in 4 (JE02, JE03, JE09, and JE14) TWs water samples, while Mn concentration was below the WHO guideline for 12 (twelve) TWs water samples. The rest of the samples, for example, 38.5% (10 out of 26) TWs contained Mn levels beyond the WHO guideline and the value was 1.13 to 3.08 times higher. In terms of BIS (2012) and BDS, Mn in 7.7% (2 out of 26) of TWs water samples was within the acceptable limit. However, 92.3% (24 out of 26) of TWs water samples contained Mn beyond the BDS, and sometimes was actually several times higher than the BDS guideline recommendation. A recent study reported a Mn concentration of 0.05–0.93 mg/L in different TWs of Jashore, Bangladesh (Ghosh et al. 2020) which is similar to our findings. They also evaluated the hazardous effects of Mn on children and adults. The sources of Mn that contribute to the TWs are most likely domestic sewage, industrialization, poor management and indiscriminate disposal of industrial wastewater, river networks, etc.
Mn in TWs water of Khulna district
Correspondingly, Mn in TWs water of the Khulna district is illustrated in Table 7. It appears that the highest and lowest Mn levels in the water sample were 2.11 mg/L and 0.01 mg/L, respectively. Of the samples, 40.5% (17 out of 42) exceeded the BDS level for Mn and 26.2% (11 out of 42) was beyond the WHO guideline value. The Mn in TWs water of KN19, KN23, KN24, KN25, KN30, KN31, KN33, KN34, KN38, KN39, KN40, and KN41 was above the permissible level of BIS (2012). Islam et al. (2020) reported Mn, 0.01–22.4 (mean 0.47) mg/L in TWs from various households situated in the coastal region of Khulna. They detected a non-carcinogenic hazardous effect. Khulna is situated in the Rupsa River network and Islam et al. (2018) reported that the amount of Mn in Rupsa River water ranged from 0.2–2.19 (mean 0.70) mg/L, which is similar to our findings in different TWs in that region. An important outcome of this data is that the background concentrations of Mn in a particular region significantly correlated with the Mn concentration in TWs. However, the main sources of Mn in TWs in these regions are industrialization, coastal region, river network areas, etc. The extensive corrosion of pipelines which is evident in the presence of saline water can dictate the solubility of Fe and Mn in TWs. Hou et al. (2020) reported that on the inner wall of such pipes, hydrous Mn-oxides are deposited which can potentially be leached in drinking water.
Descriptive data of Mn in TWs water of 9 (nine) districts
Table 8 lists the Mn in TWs water of 9 (nine) districts and of these, Sirajganj recorded the worst quality water in terms of Mn contamination. The Mn level in all the tested TWs water was beyond the BDS level and 95% surpassed the WHO guideline values. Likewise, Chuadanga, Jheniadah, and Faridpur districts’ Mn level (above 0.1 mg/L) was such that their TWs water were not fit to drink. The Mn in TWs of Meherpur, Magura, Jashore, Satkhira, and Khulna districts was beyond the drinking water quality standard of Bangladesh permissible limit of 80%, 20%, 92.3%, 66.7%, and 40.5%, respectively. Except for Magura and Satkhira Mn in TWs, water was within the WHO guideline value. Conversely, Mn in TWs of Meherpur, Chuadanga, Jhenaidah, Faridpur, Jashore, and Khulna districts crossed the WHO guideline (on some occasions several times higher) at the levels of 40%, 70%, 90%, 80%, 38.5%, and 26.2%, respectively. Overall, the Mn levels in TWs water were 48.9% and 77.7% outside the WHO and BDS levels, respectively.
The mean Mn in TWs water from Sirajganj, Meherpur, Chuadanga, Jhenaidah, Faridpur, Jashore, Satkhira, and Khulna districts was 9.0, 7.0, 4.6, 6.1, 8.1, 4.5, 1.4 and 3.3 times higher than the BDS guideline values, respectively. Only the mean Mn level in TWs water of Magura district was closer to BDS level. It was shown that the mean Mn in TWs water from Magura, Satkhira, and Khulna was below the WHO guideline value. Conversely, it was higher than the WHO permissible level in districts like Sirajganj, Meherpur, Chuadanga, Jhenaidah, Faridpur, and Jashore, at 2.3, 1.8, 1.2, 1.5, 2.0, and 1.1 times, respectively. The mean Mn value in TWs water collected in this study at Magura district was greater than the mean value reported by Rahman et al. (2016). In this work, the mean Mn value in TWs of Faridpur district was higher than that documented by Bhuiyan et al. (2016). The mean value of Mn in TWs of other districts, i.e., Rangpur, Narayanganj (Araihazar), and Noakhali was reported to be 0.685, 0.793, and 0.140 mg/L, respectively (Wasserman et al. 2006; Islam et al. 2017; Rahman et al. 2015).
One study reported that consumption of a Mn concentration higher than 0.4 mg/L reduced intellectual functions of children (age 10 years) in Bangladesh (Wasserman et al. 2006), while in Canada it was reported for children in the 5.9–13.7 age range (Kullar et al., 2019). Another analysis suggested that infants had increased risk of mortality during the first year of life if they were exposed to drinking water with a Mn concentration > 0.4 mg/L when compared to infants not exposed to this danger (Hafeman et al. 2007).
Data comparison with recent studies
Table 9 depicts the Mn data comparison with recent studies in Bangladesh. Recently, Ghosh et al. (2020) reported 2.11 mg/L Mn in tube well water in Jashore district, which is 1.71 times higher than the same area in this study. Islam et al. (2017) found Mn in TWs water at Rangpur district ranging from 0.085–4.96 mg/L. It is noticeable that the lower level of Mn in TWs was below BDS level but the upper level of Mn in TWs water was 49.6 times greater than the BDS. When comparing the Mn in Magura district with a previous study, the lower level was the same (0.01 mg/L) but the upper level was higher (0.3699 mg/L) (Rahman et al. 2016). Rahman and Rahaman (2018) reported the high Mn concentration in drinking water at the range of 0.01 to 6.32 mg/L (mean 0.99 mg/L) in Kushtia district, Bangladesh, which is higher than this study. In comparison to the Noakhali district, Mn in TWs water varied between 0.0189 and 0.4995 mg/L (Rahman et al. 2015), in which the upper limit was lower than this study except for Magura and Satkhira districts. However, it is clear from Table 8 that the maximum Mn in TWs water of this study, as well as the previous study, was beyond the BDS. The maximum Mn in the TWs level of the previous study done on Noakhali and Rangpur (Rahman et al. 2015; Islam et al. 2017) as well as the Sirajganj, Meherpur, Chuadanga, Jhenaidah, Faridpur, Jashore, and Khulna districts in the present study exceeded the WHO guideline. The maximum Mn concentration was detected at 4.11 mg/L in the current study, which is 41.1 and 10.3 times greater than the WHO and BDS safe limits, respectively (Table 9). Therefore, children are extremely susceptible to reduced intellectual functions, i.e., motor dysfunctions, memory loss, Parkinson disease, and increased infant mortality via consumption of Mn-rich drinking water in the studied areas.
Health risk assessment
The mean CDI and HQ of Mn for both children and adults in each district are tabulated in Fig. 2. The increasing pattern of mean CDI values of Mn for both children and adults follows this sequence: Magura < Satkhira < Khulna < Jashore < Chuadanga < Jhenaidah < Meherpur < Faridpur < Sirajgonj (Fig. 2A). The estimated mean CDIs of Mn for both children and adults in most cases are very low (Fig. 2A). The decreasing pattern of HQs (mean value) for Mn are as follows: Sirajganj (children 0.42 and adults 0.45) > Faridpur (children 0.38 and adults 0.41) > Meherpur (children 0.33 and adults 0.35) > Jhenaidah (children 0.29 and adults 0.31) > Chuadanga (children 0.22 and adults 0.23) < Jashore (children 0.21 and adults 0.22) > Khulna (children 0.15 and adults 0.16) > Satkhira (children 0.06 adults 0.07) > Magura (children 0.028 and adults 0.03). The mean HQs for Mn in the study area for children and adults are less than unity (Fig. 2B), confirming there are no potential non-carcinogenic health risks posed by Mn through drinking water. However, the maximum HQ for Mn in Meherpur (MHR06) (1.93 for children and 2.05 for adults) and Khulna (KN39) (1.05 for adults) was determined greater than unity (Fig. S1 in supplementary information). The HQ of Mn for children was more than unity at only one sample, whereas that for adults was greater than unity at two water samples, which indicated a significantly high risk to the exposed population. A recent study noted that the HQ of Mn for children in the Jashore district was higher than unity at one sample but for adults was at sixteen samples (Ghosh et al. 2020).

Chronic daily intake (CDI) (A), and hazard quotient (B) of Mn through water ingestion for the nine districts of Bangladesh
Study limitation
This preliminary study conducted in only 9 districts for the monitoring of Mn contamination level from drinking water sources, especially tube well water in the rural area, Bangladesh. Therefore, the other districts or larger site is warranted to integrate in future research for investigation the level of Mn concentration as a large-scale monitoring work. Other sources of Mn exposure, such as dietary and supplementary foods, and particulate substance were not considered for estimation of health risk in this study.
Conclusion
Manganese-free potable water is essential for good health. The study results should help the relevant authorities identify the districts/areas that need to be safeguarded. Most of the tube well water Mn level did follow the WHO or Bangladesh drinking standard (BDS). The Mn level in tube well water exceeded the recommend value of the WHO and Bangladesh drinking standard by 51% and 76%, respectively. The maximum HQ value for children and adults was observed to be greater than unity in one and two samples, respectively, which suggests potential non-carcinogenic health risks are evident in the study area. It is very important to identify the tube wells which are safe or not safe for drinking purposes. The authorities should take the initiative to provide safe drinking water to the people so that they remain in good health. Before installing any water supply device, the water quality should be checked and subjected to treatment strategies if necessary. The data emanating from this will be helpful in the long term. Increased awareness, low-cost water supply, development of cost-effective household water treatment systems, and effective water safety planning at the household level will all help to reduce the risks associated with Mn in drinking water. These findings are important for future research to evaluate the exact sources of Mn contamination in drinking water in the investigated area and how they should be managed properly. This study recommends long-term monitoring of Mn in drinking water to prevent risks to health and ensure that good resource management policies are implemented.
Data availability
The datasets generated and analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Aktaruzzaman M, Hossain MS, Fakhruddin ANM, Uddin MJ, Rahman SH, Chowdhury MAZ, Alam MK, Fardous Z, Hossain MA (2013) Water and bottom sediments quality of brackish water shrimp farms in Kaliganj Upazila, Satkhira, Bangladesh. Soil Environ 32:29–35
Akter MS, Islam MN, Fardous Z, Khan MH, Rahman MA (2010) Assessment of heavy metals in handloom cottage, dyeing and printing industrial effluents in Belkuchi, Sirajganj. J Appl Sci Technol 7:85–90
Ali MH, Bhattacharya B, Islam AKMS, Islam GMT, Hossain MS, Khan AS (2019) Challenges for flood risk management in flood-prone Sirajganj region of Bangladesh. J Flood Risk Manag 12. https://doi.org/10.1111/jfr3.12450
Aschner JL, Aschner M (2005) Nutritional aspects of manganese homeostasis. Mol Asp Med 26:353–362. https://doi.org/10.1016/j.mam.2005.07.003
Aschner M, Guilarte TR, Schneider JS, Zheng W (2007) Manganese: recent advances in understanding its transport and neurotoxicity. Toxicol Appl Pharmacol 221:131–147. https://doi.org/10.1016/j.taap.2007.03.001
ATSDR (2012) Toxicological Profile for Formaldehyde. US Department of Health and Human Services. Public Health Service, and the Agency for Toxic Substances and Disease Registry, Atlanta, GA
Avila DS, Puntel RL, Aschner M (2013) Manganese in health and disease.Met Ions Life Sci 13:199–227
Bangladesh Bureau of Statistics, BBS (2013) Statistics and Informatics Division (SID) Ministry of Planning Government of the People’s Republic of Bangladesh. District Statistics 2011
Bangladesh Bureau of Statistics, BBS (2015) Population density and vulnerability: a challenge for sustainable development of Bangladesh. Statistics and Informatics Division (SID), Ministry of Planning
Bhuiyan MAH, Bodrud-Doza M, Islam ARMT, Rakib MA, Rahman MS, Ramanathan A (2016) Assessment of groundwater quality of Lakshimpur district of Bangladesh using water quality indices, geostatistical methods, and multivariate analysis. Environ Earth Sci 75:1020. https://doi.org/10.1007/s12665-016-5823-y
Bouchard M, Laforest F, Vandelac L, Bellinger D, Mergler D (2007) Hair manganese and hyperactive behaviors: Pilot study of school-age children exposed through tap water. Environ Health Perspect 115(1):122–127. https://doi.org/10.1289/ehp.9504
Bouchard MF, Surette C, Cormier P, Foucher D (2018) Low level exposure to manganese from drinking water and cognition in school-age children. Neurotoxicol 64:110–117. https://doi.org/10.1016/j.neuro.2017.07.024
Bowler RM, Gysens S, Diamond E, Nakagawa S, Drezgic M, Roels HA (2006) Manganese exposure: neuropsychological and neurological symptoms and effects in welders. Neurotoxicol 27:315–326. https://doi.org/10.1016/j.neuro.2005.10.007
Brown MT, Foos B (2009) Assessing children’s exposures and risks to drinking water contaminants: a manganese case study. Hum Ecol Risk Assess 15(5):923–947
Bureau of Indian Standard, BIS (2012) Drinking water-specification (1st Rev.) IS-10500. New Delhi, India
Chakraborti D, Rahman MM, Das B, Murrill M, Dey S, Mukherjee SC, Dhar RK, Biswas BK, Chowdhury UK, Roy S, Sorif S (2010) Status of groundwater arsenic contamination in Bangladesh: a 14-year study report. Water Res 44(19):5789–5802
Chen P, Bornhorst J, Aschner MA (2018) Manganese metabolism in humans. Front Biosci 23:1655–1679
Cotruvo JA (2017) 2017 WHO guidelines for drinking water quality: first addendum to the fourth edition. J Am Water Works Assoc 109(7):44–51
Didar-Ul Islam SM, Bhuiyan MA, Ramanathan AL (2015) Climate change impacts and vulnerability assessment in coastal region of Bangladesh: a case study on Shyamnagar upazila of Satkhira district. J Clim Chang 1:37–45
Environment Conservation Rules (ECR), Ministry of Environment & Forests (MoEF), Government of the People’s Republic of Bangladesh, 1997
Ericson JE, Crinella FM, Clarke-Stewart KA, Allhusen VD, Chan T, Robertson RT (2007) Prenatal manganese levels linked to childhood behavioral disinhibition. Neurotoxicol Teratol 29:181–187. https://doi.org/10.1016/j.ntt.2006.09.020
Erikson KM, Aschner M (2003) Manganese neurotoxicity and glutamate-GABA interaction. Neurochem Int 43:475–480. https://doi.org/10.1016/S0197-0186(03)00037-8
Erikson KM, Dorman DC, Lash LH, Aschner M (2005) Persistent alterations in biomarkers of oxidative stress resulting from combined in utero and neonatal manganese inhalation. Biol Trace Elem Res 104:151–163. https://doi.org/10.1385/BTER:104:2:151
Frisbie SH, Mitchell EJ, Dustin H, Maynard DM, Sarkar B (2012) World Health Organization discontinues its drinking-water guideline for manganese. Environ Health Perspect 120:775–778. https://doi.org/10.1289/ehp.1104693
Ghosh GC, Khan MJH, Chakraborty TK, Zaman S, Kabir AE, Tanaka H (2020) Human health risk assessment of elevated and variable iron and manganese intake with arsenic-safe groundwater in Jashore, Bangladesh. Sci Rep 10:1–9
Grandjean P, Landrigan PJ (2006) Developmental neurotoxicity of industrial chemicals. Lancet 368:2167–2178. https://doi.org/10.1016/S0140-6736(06)69665-7
Grandjean P, Landrigan PJ (2014) Neurobehavioural effects of developmental toxicity. Lancet Neurol 13(3):330–338
Groschen GE, Arnold TL, Morrow WS, Warner KL (2009) Occurrence and distribution of iron, manganese, and selected trace elements in ground water in the glacial aquifer system of the Northern United States. US Geological Survey Scientific Investigations Report 2009-5006. Available: http://pubs.usgs.gov/sir/2009/5006/
Guilarte TR, Chen MK (2007) Manganese inhibits NMDA receptor channel function: implications to psychiatric and cognitive effects. Neurotoxicol 28:1147–1152. https://doi.org/10.1016/j.neuro.2007.06.005
Hafeman D, Factor-Litvak P, Cheng Z, van Geen A, Ahsan H (2007) Association between manganese exposure through drinking water and infant mortality in Bangladesh. Environ Health Perspect 115:1107–1112. https://doi.org/10.1289/ehp.10051
Hasan S, Ali MA (2010) Occurrence of manganese in groundwater of Bangladesh and its implications on safe water supply. J Civ Eng (IEB) 38:121–128
Hasan MM, Ahmed KM, Sultana S, Rahman MS, Ghosh SK, Ravenscroft P (2018) Investigations on groundwater buffering in Khulna-Satkhira Coastal Belt using managed aquifer recharge. In: Groundwater of South Asia. Springer, Singapore, pp 453–462
Henn BC, Schnaas L, Ettinger AS, Schwartz J, Lamadrid-Figueroa H, Hernàndez-Avila M, Amarasiriwardena C, Hu H, Bellinger DC, Wright RO, Téllez-Rojo MM (2011) Associations of early childhood manganese and lead coexposure with neurodevelopment. Environ Health Perspect 120:126–131. https://doi.org/10.1289/ehp.1003300
Hossain MA, Rahman MM, Murrill M, Das B, Roy B, Dey S, Maity D, Chakraborti D (2013) Water consumption patterns and factors contributing to water consumption in arsenic affected population of rural West Bengal, India. Sci Total Environ 463:1217–1224
Hossain ML, Hossain MK, Das SR (2014) Vulnerability of Bangladesh to natural and anthropogenic disasters. Pothi.com publisher, India
Hou Q, Zhang Q, Huang G, Liu C, Zhang Y (2020) Elevated manganese concentrations in shallow groundwater of various aquifers in a rapidly urbanized delta, south China. Sci Total Environ 701:134777. https://doi.org/10.1016/j.scitotenv.2019.134777
Islam AT, Shen S, Bodrud-Doza M, Rahman MA, Das S (2017) Assessment of trace elements of groundwater and their spatial distribution in Rangpur district, Bangladesh. Arab J Geosci 10. https://doi.org/10.1007/s12517-017-2886-3
Islam MS, Mohanta SC, Siddique MAB, Al-Mamun MA, Hossain N, Bithi UH (2018) Physico-chemical assessment of water quality parameters in Rupsha river of Khulna region, Bangladesh. Int J Eng Sci (IJES) 7:73–78
Islam MA, Akber MA, Rahman MA, Islam MA, Kabir MP (2019) Evaluation of harvested rainwater quality at primary schools of southwest coastal Bangladesh. Environ Monit Assess 191:80. https://doi.org/10.1007/s10661-019-7217-6
Islam ARMT, Siddiqua MT, Zahid A, Tasnim SS, Rahman MM (2020) Drinking appraisal of coastal groundwater in Bangladesh: an approach of multi-hazards towards water security and health safety. Chemosphere 255:126933. https://doi.org/10.1016/j.chemosphere.2020.126933
Iyare PU (2019) The effects of manganese exposure from drinking water on school-age children: a systematic review. Neurotoxicol 73:1–7. https://doi.org/10.1016/j.neuro.2019.02.013
Keen CL, Ensunsa JL, Lonnerdal B, Zidenberg-Cherr S (2013) Manganese. Encyclopedia of human nutrition (3rd ed.) Academic Press, Amsterdam, pp. 148
Khan K, Wasserman GA, Liu X, Ahmed E, Parvez F, Slavkovich V, Levy D, Mey J, van Geen A, Graziano JH, Litvak PF (2012) Manganese exposure from drinking water and children’s academic achievement. Neurotoxicol 33:91–97. https://doi.org/10.1016/j.neuro.2011.12.002
Kim Y, Kim BN, Hong YC, Shin MS, Yoo HJ, Kim JW, Bhang SY, Cho SC (2009) Co-exposure to environmental lead and manganese affects the intelligence of school-aged children. Neurotoxicol 30:564–571. https://doi.org/10.1016/j.neuro.2009.03.012
Kohl PM, Medlar S J (2006) Occurrence of manganese in drinking water and manganese control. American Water Research Foundation, American Water Works Association and IWA Publishing, Denver
Kullar SS, Shao K, Surette C, Foucher D, Mergler D, Cormier P, Bellinger DC, Barbeau B, Sauvé S, Bouchard MF (2019) A benchmark concentration analysis for manganese in drinking water and IQ deficits in children. Environ Int 130:104889. https://doi.org/10.1016/j.envint.2019.05.083
Ljung K, Vahter M (2007) Time to re-evaluate the guideline value for manganese in drinking water? Environ Health Perspect 115(11):1533–1538
Lucchini R, Placidi D, Cagna G, Fedrighi C, Oppini M, Peli M, Zoni S (2017) Manganese and developmental neurotoxicity. Adv Neurobiol 18:13–34
McMillan DE (1999) A brief history of the neurobehavioral toxicity of manganese: some unanswered questions. Neurotoxicol 20(2-3):499–507
Menezes-Filho JA, Novaes Cde O, Moreira JC, Sarcinelli PN, Mergler D (2011) Elevated manganese and cognitive performance in school-aged children and their mothers. Environ Res 111:156–163. https://doi.org/10.1016/j.envres.2010.09.006
Mohana AA, Rahman MA, Islam MR (2020) Deep and shallow tubewell water from an arsenic-contaminated area in rural Bangladesh: risk-based status. Int J Energy Water Res 4(2):163–179
National Center for Health Statistics, NCHS (2000) In collaboration with the National Center for Chronic Disease Prevention and Health Promotion http://www.cdc.gov/growthcharts; accessed at: https://www.cdc.gov/growthcharts/data/set1clinical/cj41l021.pdf
O’Neal SL, Zheng W (2015) Manganese toxicity upon overexposure: a decade in review. Curr Environ Health Rep 2:315–328. https://doi.org/10.1007/s40572-015-0056-x
Rahman A, Rahaman H (2018) Contamination of arsenic, manganese and coliform bacteria in groundwater at Kushtia District, Bangladesh: human health vulnerabilities. J Water Health 16(5):782–795
Rahman MM, Dong Z, Naidu R (2015) Concentrations of arsenic and other elements in groundwater of Bangladesh and West Bengal, India: potential cancer risk. Chemosphere 139:54–64. https://doi.org/10.1016/j.chemosphere.2015.05.05
Rahman MA, Hashem MA, Nur-A-Tomal MS (2016) Potable water quality monitoring of primary schools in Magura district, Bangladesh: children’s health risk assessment. Environ Monit Assess 188:680. https://doi.org/10.1007/s10661-016-5692-6
Rahman MA, Kumar S, Mohana AA, Islam R, Hashem MA, Chuanxiu L (2019) Coliform bacteria and trace metals in drinking water, southwest Bangladesh: multivariate and human health risk assessment. Int J Environ Res 13:395–408
Riojas-Rodriguez H, Solis-Vivanco R, Schilmann A, Montes S, Rodriguez S, Rios C, Rodríguez-Agudelo Y (2010) Intellectual function in Mexican children living in a mining area and environmentally exposed to manganese. Environ Health Perspect 118:1465–1470. https://doi.org/10.1289/ehp.0901229
Rodríguez-Barranco M, Lacasaña M, Aguilar-Garduño C, Alguacil J, Gil F, González-Alzaga B, Rojas-García A (2013) Association of arsenic, cadmium and manganese exposure with neurodevelopment and behavioural disorders in children: a systematic review and meta-analysis. Sci Total Environ 454:562–577
Roels HA, Bowler RM, Kim Y, Henn BC, Mergler D, Hoet P, Téllez-Rojo MM (2012) Manganese exposure and cognitive deficits: a growing concern for manganese neurotoxicity. Neurotoxicol 33(4):872–880
Sahni V, Léger Y, Panaro L, Allen M, Giffin S, Fury D, Hamm N (2007) Case report: a metabolic disorder presenting as pediatric manganism. Environ Health Perspect 115(12):1776–1779
Spangler JG, Reid JC (2010) Environmental manganese and cancer mortality rates by county in North Carolina: an ecological study. Biol Trace Elem Res 133:128–135. https://doi.org/10.1007/s12011-009-8415-9
Spangler AH, Spangler JG (2009) Groundwater manganese and infant mortality rate by county in North Carolina: an ecological analysis. Ecohealth 6:596–600. https://doi.org/10.1007/s10393-010-0291-4
Stokes P, Campbell P, Schroeder W, Trick C, France R, Puckett K, Donaldson J (1988) Manganese in the Canadian environment. NRCC No. 26193. Natl. Res. Council of Canada, Assoc. Committee on Scientific Criteria for Environ. Quality, Ottawa, ON
Uddin MZ, Rahman MA, Ahmed I, Mohiuddin KM (2019) Groundwater quality for drinking and irrigation usages in Kazipur upazila under Sirajganj district of Bangladesh. J Bangladesh Agric Univ 17:309–318
USEPA (2004) Drinking water health advisory for manganese. US Environmental Protection Agency (accessed at: https://www.epa.gov/sites/production/files/2014-09/documents/support_cc1_magnese_dwreport_0.pdf)
USEPA (2011) Exposure factors handbook. United States Environmental Protection Agency, Washington DC (EPA/600/R-09/052F).
USEPA (2017) Safe Drinking Water Act (SDWA) and federal facilities: enforcement. https://www.epa.gov/enforcement/safe-drinking-water-act-sdwa-and-federal-facilities. Accessed 25 July 2017
USEPA (2020) Regional Screening Level (RSL) Resident Tapwater Table (TR = 1E-06, HQ = 1) May 2020 (corrected) [WWW Document]. URL 9Accessed at: https://semspub.epa.gov/work/HQ/200055.pdf)
Wasserman GA, Liu X, Parvez F, Ahsan H, Levy D, Litvak PF, Kline J, van Geen A, Slavkovich V, LoIacono NJ, Cheng Z, Zheng Y, Graziano JH (2006) Water manganese exposure and children’s intellectual function in Araihazar, Bangladesh. Environ Health Perspect 114:124–129. https://doi.org/10.1289/ehp.8030
WHO (2008) Guidelines for drinking-water quality, 3rd ed. Geneva, Switzerland
WHO (2017) Guidelines for drinking-water quality: incorporating the1st addendum. World Health Organization, Geneva
WHO (2011) Guidelines for drinking water quality (4th ed.). WHO Press, Geneva
William-Johnson M, World Health Organization (1999) Manganese and its compounds. Concise International Chemical Assessment Document 12. World health organization. (accessed at: https://apps.who.int/iris/bitstream/handle/10665/42184/924153012X.pdf)
Woolf A, Wright R, Amarasiriwardena C, Bellinger D (2002) A child with chronic manganese exposure from drinking water. Environ Health Perspect 110(6):613–616
World Health Organization (2020) Manganese in drinking-water: background document for development of WHO Guidelines for drinking-water quality. World Health Organization (accessed at: https://www.who.int/docs/default-source/wash-documents/wash-chemicals/gdwq-manganese-background-document-for-public-review.pdf?sfvrsn=9296741f_5)
Wright RO, Amarasiriwardena C, Woolf AD, Jim R, Bellinger DC (2006) Neuropsychological correlates of hair arsenic, manganese, and cadmium levels in school-age children residing near a hazardous waste site. Neurotoxicol 27:210–216. https://doi.org/10.1016/j.neuro.2005.10.001
Yousef S, Adem A, Zoubeidi T, Kosanovic M, Mabrouk AA, Eapen V (2011) Attention deficit hyperactivity disorder and environmental toxic metal exposure in the United Arab Emirates. J Trop Pediatr 57:457–460. https://doi.org/10.1093/tropej/fmq121
Zhang S, Tian Y, Guo Y, Shan J, Liu R (2020) Manganese release from corrosion products of cast iron pipes in drinking water distribution systems: effect of water temperature, pH, alkalinity, SO42- concentration and disinfectants. Chemosphere 262:127904. https://doi.org/10.1016/j.chemosphere.2020.127904
Zota AR, Ettinger AS, Bouchard M, Amarasiriwardena C, Schwartz J, Hu H, Wrighta RO (2009) Maternal blood manganese levels and infant birth weight. Epidemiology 20:367–373. https://doi.org/10.1097/EDE.0b013e31819b93c
Acknowledgements
The authors greatly acknowledge the Department of Public Health Engineering (DPHE), Zonal Laboratory Khulna, Jhenaidah, and Bogura for providing the laboratory facilities. We are also thankful to the field workers for their assistance in the sampling process.
Author information
Authors and Affiliations
Contributions
Aminur Rahman: visualization/conceptualization, investigation, methodology, and writing-review, and editing. Abul Hashem: investigation, methodology, supervision, data managing-organizing, writing-original draft, writing-review, and editing. Sohel Rana: sampling and data collection. Rashidul Islam: review and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The authors declare that the submitted manuscript is original. Authors also acknowledge that the current research has been conducted ethically and the final shape of the research has been agreed by all authors. Authors declared that this manuscript does not involve researching about humans or animals.
Consent to participate
The authors consent to participate in this research study.
Consent to publish
The authors consent to publish the current research in ESPR journal.
Conflict of interest
The authors declare no conflict of interest.
Additional information
Responsible Editor: Lotfi Aleya
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
• Seventy-six percent of tube well water manganese level exceeds Bangladesh drinking water standard.
• Compared to WHO guideline 51% tube well water manganese exceeds permissible level.
• Hazard quotient of Mn was greater than unity, potentially non-carcinogenic health risks.
Supplementary Information
ESM 1
(DOCX 30 kb)
Rights and permissions
About this article

Cite this article
Rahman, M.A., Hashem, M.A., Rana, M.S. et al. Manganese in potable water of nine districts, Bangladesh: human health risk. Environ Sci Pollut Res 28, 45663–45675 (2021). https://doi.org/10.1007/s11356-021-14016-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-021-14016-z