
Abstract
The Central Plains Urban Agglomeration is an important growth pole of China’s economy, but the rapid economic growth is accompanied by serious air pollution problems. In this paper, the latest available PM2.5 monitoring data in 2015–2017 and exposure-response relationship model are used to quantitatively analyze the health effect damages due to PM2.5 pollution. The way of disease cost, adjusted human capital, and willingness to pay were adopted to estimate the economic loss of health effect damages. The results show that health effect damages of PM2.5 pollution in 2015–2017 were 11.9251 million, 11.4292 million, and 11.1012 million, respectively, accounting for 7.41%, 7.05%, and 6.94% of the total population of this area. The health effect economic loss was 97.398 billion RMB, 93.516 billion RMB, and 94.485 billion RMB, accounting for 1.73%, 1.53%, and 1.41% of the GDP. Chronic bronchitis and premature death due to PM2.5 are the main sources of health effect economic loss. Elderly people and infants are vulnerable groups of PM2.5 pollution. Affected by economic growth level, population density, and economic structure, Heze, Zhengzhou, Handan, and Liaocheng were greatly affected by PM2.5 pollution, and their health effect damages was larger. The health effect damages and health effect economic loss due to PM2.5 pollution in this area show a downward trend, indicating that air pollution reduction measures have played a positive role. However, the whole effect is still large. According to the results, this paper puts forward the policies.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In China, the rapid growth of economy has led to the deterioration of the atmospheric environment, and the harm caused by air pollution has also been increasingly severe, especially the pollution by PM2.5.
In 2013, out of the monitored 74 cities in China, there were only 3 cities that achieved air quality standards (Ministry of ecology and Environment of the People’s Republic of China 2014). In 2016, 338 prefecture-level cities and above had 2464 days of severe pollution, 784 days of heavy pollution. Among the heavy pollution days, 80.3% with PM2.5 as the primary pollutant (Ministry of ecology and Environment of the People’s Republic of China 2017). A total of 121 of the 338 cities achieved the air quality standards, with qualification rate of 35.8% in 2018 (Ministry of ecology and Environment of the People’s Republic of China 2019). It can be seen that although the quality of China’s atmospheric environment has been gradually improved since 2013, the situation is still not optimistic, especially the PM2.5 pollution (Fig. 1).

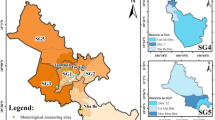
PM2.5 concentration in Central Plains Urban Agglomeration from 2015 to 2017
The Central Plains Urban Agglomeration (CPUA) is located in the central and eastern China, including 30 cities, namely all 18 cities in Henan province, Liaocheng and Heze in Shandong province; Changzhi, Jincheng, and Yuncheng in Shanxi province; Huaibei, Bengbu, Suzhou, Fuyang, and Bozhou in Anhui province; and Xingtai and Handan in Hebei province. According to the Environmental Assessment Report on the Development Strategy for the Central Region published by the Ministry of Ecological Environment in 2015, PM2.5 concentrations in two thirds of the area in this region were more than 70 μg/m3. The State Council pointed out the environmental protection again in the Development Program of CPUA in 2016 (National Development and Reform Commission of the People’s Republic of China 2016). In 2017, Handan, Xingtai, and Zhengzhou in this area ranked among the top ten cities with the worst air quality (Ministry of Ecology and Environment of the People’s Republic of China 2017). The air pollution of this region is still severe, which not only seriously threatens the health of residents but also brings about great economic loss.
World Health Organization statistics show that air pollution causes two million premature deaths every year, of which fine particulate matter has the greatest impact on human health. PM2.5 is a fine particle less than 2.5 μm in diameter, which can cause many respiratory diseases after inhalation. Compared with other pollutants, PM2.5 is the most serious hazard to human health (Zhou 2013).
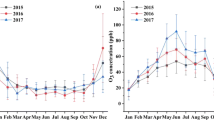
For Henan Province, the main province of CPUA, PM2.5 in the central and western regions was mainly from local, and 40–50% of PM2.5 in the eastern and northern regions were from the surrounding areas. Residential sources, industrial parks and motor vehicle emissions were the main sources of PM2.5 (Wang et al. 2016). The overall characteristics of PM2.5 pollution presented the winter > spring > autumn > summer (Cao et al. 2018).
Specifically, taking Zhengzhou, the capital of Henan Province, and Xingtai, Hebei Province as examples, the sources of PM2.5 in Zhengzhou were soil dust, coal combination, and the secondary aerosol secondary aerosol, and its main components were nitrate, sulfate, and carbon fragments (Geng et al. 2013). The sources of PM2.5 in Xingtai were coal combination, secondary nitrate, vehicle exhaust dust, and secondary sulfur, etc. The main components were sulfur, organic carbon, nitrate, elementary carbon, and ammonium (Hu et al. 2019).
Scholars have done a lot of research on the effect of fine particle concentration on the incidence of related health ends (Pope III et al. 2002; Miri et al. 2016; Khaniabadi et al. 2019; Phosri et al. 2019; Qu et al. 2019; Qiu et al. 2019; Wu et al. 2019a, b; Hashmi et al. 2019). Poisson regression and generalized additive model are common methods to study the relationships between pollutant concentrations and health incidence. Many previous studies using these methods have fully demonstrated the impact of fine particle concentration on the health incidence (De Leon et al. 1996; Burnett et al. 1997; Samet et al. 2000; Wong et al. 2002; Dai et al. 2004; Zhang et al. 2018; Hu et al. 2015; Li et al. 2019; He et al. 2016) and found that the incidence of each related health end would increase with the increase of pollutant concentration.
After the harm of air pollution to human health has been confirmed, how to analyze the health effect damages and health effect economic loss quantitatively is particularly important. Miraglia et al. (2005) evaluated the health effect damages and health effect economic loss in Sao Paulo area by using Daly model. Nam et al. (2010) quantified economic loss of air pollution by using European data and CGR model. Nagpure et al. (2014) found that there were more premature deaths from air pollution in big cities of developing countries than in developed countries. Brand and Hunt (2018) found that the health economic loss attribute to air pollution from car fuel combustion in the UK was between 22.6 billion pounds and 71.3 billion pounds. Lelieveld et al. (2019) found that there were 790,000 premature deaths from air pollution every year in Europe. Cromar et al. (2019) believed that if the American Thoracic Society air pollution standard was followed, the excessive death caused by air pollution in the United States would greatly reduce.
As for China, the study of Matus et al. (2012) shows that the economic loss of ozone pollution and fine particle pollution increased by 90 billion US dollars between 1975 and 1997. Miao et al. (2017) and Tian et al. (2018) found that the premature deaths of air pollution were 1.7–1.99 million in China in 2006, and in 2030, the economic loss of PM2.5 pollution will account for 0.68% of GDP. Chen et al. (2017) found that a total of 200 billion RMB was used to treat health hazards due to air pollution from 2006 to 2012. Huang et al. (2018), Sun et al. (2018), and Wu et al. (2019a, b) also found that due to the implementation of environmental protection policies, 47,240 to 60,213 people avoided premature death from 2013 to 2017, and if the emission reduction measures were continued from 2015 to 2025, Beijing Tianjin Hebei region would generate 366–810 billion economic benefits. Chen and Bloom (2019) calculated that the economic loss caused by air pollution in China from 1990 to 2030 was 1137 billion US dollars.
The exposure-response relationship model is usually adopted to assess the health effect damages due to air pollution, and health loss can be quantified by using the way of disease cost, adjusted human capital, and willingness to pay. Ghude et al. (2016) and Balakrishnan et al. (2019) used this model to evaluate the health loss and economic loss due to air pollution based on India data. Liu et al. (2016) and Maji et al. (2018) found that 1.37 million and 0.964 million people died prematurely due to PM2.5 in China in 2013 and 2016, respectively. Li et al. (2017) and Wu et al. (2017) took Beijing and Shanghai as research objects, evaluated the economic loss by PM2.5 pollution in Beijing, and then predicted the influence of pollution in Shanghai in 2030.
After analyzing the relevant research results, we find that most of previous studies mainly focused on the influences of PM2.5 pollution in Pearl River Delta, Jing-Jin-Ji Region and Yangtze River Delta. By contrast, there is rare research on CPUA, and even fewer quantitative assessments on the influences of PM2.5 pollution in this area. As the different indicators have different characteristics and each method has its limitations, using only one method for evaluation will lead to deviation between the evaluation results and the actual situation. Thus, this paper evaluated the health effect damages due to PM2.5 pollution from 2015 to 2017 in CPUA by using exposure-response relationship model. After that, the way of disease cost, adjusted human capital, and willingness to pay were adopted to estimate the health effect economic loss.
Methods and data
Evaluation of health effect damages
Selection of health effect ends
In terms of damage of population health, PM2.5 pollution mainly causes increase of mortality, the admission rate, the outpatient rate, and morbidity and weakens somatic function of individuals. On the premise of using Chinese research results to ensure a relevant accurate evaluation results, this paper took the availability of data and the coverage degree of health effect ends into full consideration and selected several health effect ends which were highly related to PM2.5 pollution.
Health effect ends selected include the death from cardiovascular disease, respiratory disease, and lung cancer. Cardiovascular disease hospitalization and respiratory disease hospitalization. Doctors’ office visiting from Pediatric clinic, internal medicine. And Acute upper respiratory infection and chronic bronchitis are also included.
Method for evaluating the health effect damages
The effect of pollutant concentration on human health is very significant. When the pollutant concentration exceeds the threshold, it will cause damage to human health. To evaluate the health effect damages due to PM2.5 pollution reasonably, the exposure-response relationship model was selected. In assessing the health effect damages, this model is very common and can calculate the health effect damages of pollutants at different concentrations. The incidence of health effect ends (death, hospitalization, outpatient) at the actual concentration was as follows. And the formulas (1)–(3) were all derived from Huang and Zhang (2013).
where R = the incidence at the actual concentration. R0 = the health risk at the reference concentration. β = the exposure-response coefficient. C = the actual concentration of PM2.5. C0 = the reference concentration of PM2.5.
It can be seen from the above formula that the change of the health effect ends incidence rate due to PM2.5 pollution is as follows:
Thus, the health effect damages E can be calculated by using the values of R, β, C, C0, and P:
Evaluation of health effect economic loss
When assessing the health effect economic loss, the way of disease cost, adjusted human capital, and willingness to pay are commonly used. The adjusted human capital method measures the economic loss due to premature death based on human economic output. The disease cost method includes the loss caused by medical expenses and loss of working time. The willingness to pay method generally refers to using the way of investigating exposure population to obtain the monetary expenses that the exposure population would pay to avoid illness or death, which can directly reflect the health effect economic loss.
Health effect economic loss by premature death
This paper using the way of adjusted human capital evaluated the economic loss by premature death. This method can reflect the different economic loss by premature death in different age groups, and the evaluation results are closer to the actual situation. The formulas (4)–(7) all came from Zhao et al. (2014).
The first step is the calculation of the number of premature deaths:
where Pδn = the number of premature deaths in the nth age group due to the δth disease. Pn = the population of the n age group. Rδn = the mortality rate in the nth age group due to the δth disease. βδ= the exposure-response coefficient of death due to the δth disease.
The second step is to calculate the residual life lost by premature death, i.e., the difference between life expectancy and age at the time of death:
where tδn = the number of years of the early death of an individual who dies in the nth age group due to the δth disease. en = the life expectancy of the nth age group. And dδn = the age at which an individual die at the nth age group due to the δth disease.
The third step is to calculate the future loss of an individual due to early death and discount it:
where GDPδn = the individual health effect economic loss due to the premature death who dies in the nth age group due to the δth disease. i = the year (ith year). GDP0 = the per capita GDP at the time of individual death. α = the GDP growth rate (the World Bank’s forecast of China’s average GDP growth rate in 2019–2021). γ = the discount rate (take the bank’s medium and long-term loan interest rate of 4.7%).
The fourth step is to sum up the health effect economic loss due to premature death of all individuals:
where CT = the health effect economic loss of premature death. Among the health effect ends, diseases causing premature death include cardiovascular disease, respiratory disease, and lung cancer, and the total exposure population was divided into 19 age groups.
Health effect economic loss of hospitalization and outpatient service
The health effect economic loss of hospitalization and outpatient is calculated by using the disease cost method and the eq. (8) is as follows (Huang and Zhang 2013):
where Ci = the health effect economic loss of health effect end i. Cpi = the unit expense of health effect end i. GDPp = daily per capita GDP. Di = the delay times. Ei = the health effect damages of health effect end i, which can be obtained by eq. 3.
Health effect economic loss of acute upper respiratory infection
As there is no statistical data in China, based on the ratio of unit economic loss of outpatient and acute bronchitis calculated in the research of Huang and Zhang (2013), this paper estimated the unit economic loss of acute bronchitis in cities of CPUA and takes it as the unit health effect economic loss of acute upper respiratory tract infection.
Health effect economic loss of chronic bronchitis
Chronic bronchitis is a chronic disease, its health effect economic loss is not short-term and cannot be directly assessed by disease cost method as other health effect ends. To make the evaluation more accurate, on the basis of the research results of value of a statistical life (VSL) obtained by Li et al. (2017), using the CPI index of Beijing and the per capita disposable income of CPUA, this paper calculated the VSL of the residents in CPUA in 2015 and 2016. Then, based on the research results of Magat and Huber (1991) and Chen (2008), this paper found out that the unit economic loss of chronic bronchitis accounted for 40% of VSL. Combined with the VSL of each city resident, the health effect economic loss of chronic bronchitis can be calculated.
Data processing
Data of PM2.5 concentration and exposure population
Previous studies show that PM2.5 can directly penetrate the alveoli for blood gas exchange, which is harmful to human body. In this paper, 0 is chosen as the threshold of PM2.5.
The data of PM2.5 concentration used in this paper are the daily data published by the city monitoring points from January 2015 to December 2017. Annual concentration is the average daily concentration. The exposure population is taken by the permanent population of CPUA in 2015–2017. The data is from the sixth census yearbook and the city statistical yearbooks.
Data of exposure-response coefficient and the incidence rate
The choice of exposure-response coefficient is critical. However, China’s PM2.5 concentration is relatively high, and most foreign scholars’ research is completed in low pollution concentration areas. Direct use of foreign scholars’ research results may lead to deviation in the evaluation results. Therefore, the exposure-response coefficients selected in this paper are taken from the research results of Chinese scholars (Table 1).
In terms of mortality, due to the lack of the mortality of specific age and specific disease in the health statistics of China’s provinces, this paper uses the national mortality of specific age and specific disease as the baseline incidence rate of premature death. The data come from the China Health and Family Planning Yearbook 2016, 2017, and 2018.
In terms of hospitalization rate, this paper firstly obtains the ratio of the national hospitalization rate of each disease to the national average hospitalization rate. It is assumed that all the researched provinces follow the same ratio, and then, the hospitalization rate of each disease equals to the average hospitalization rate of each province multiplied by the ratio in the province.
In terms of outpatient rate, the number of pediatric clinic and internal medicine in each province are from the China Health and Family Planning Yearbook 2016, 2017, and 2018. The outpatient rate of pediatric clinic in each province is obtained through dividing the number of pediatric outpatients by the number of people under the age of 14 in the province. The outpatient rate of internal medicine in each province is obtained through dividing the number of internal medicine outpatients by the number of permanent populations.
In terms of morbidity, since China has not made detailed statistics in the provinces, the data in Hebei and Shandong provinces are replaced by the data from eastern China’s cities. And the data of Henan, Shanxi, and Anhui Province are replaced by the data from the central cities. The data come from the China Health and Family Planning Yearbook 2016, 2017, and 2018.
The data of the per health effect economic loss from hospitalization and outpatient
Per health effect economic loss caused by hospitalization consists of hospitalization expenses and the loss of working time. For the hospitalization expenses, this paper firstly obtains the ratio of the provincial average hospitalization expenses to the national average hospitalization expenses, and then, the provincial hospitalization expenses of the diseases are obtained by multiplying the national hospitalization expenses by the ratio. For the time loss, this paper used patient’s hospital stay as the lost time. Firstly, this paper calculates the ratio of the national hospital stay of each disease to the national average hospital stay, and then, the provincial hospital stay for each disease is estimated by multiplying the provincial average hospital stay by the ratio.
Health effect economic loss caused by outpatient is also composed of outpatient expenses and the loss of working time. Since the provinces have not made detailed statistics on the outpatient expenses of different outpatients, this paper uses the provincial average outpatient expenses as the outpatient expenses of pediatric clinic and internal medicine. The time loss for internal medicine is calculated by 1 day, as the diseased children need to be accompanied by their parents. The time loss for pediatric clinics is also estimated by 1 day. The above data are all from the China Health and Family Planning Yearbook 2016, 2017, and 2018 (Tables 2 and 3).
Results
Health effect damage evaluation results
By substituting the incidence of each health effect end into the model, the health effect damages was calculated and the results are shown in Table 4.
According to the calculation results, from 2015 to 2017, PM2.5 pollution damaged the health of 11.9251 million people (5.3064–17.9269 million people), 11.4916 million people (5.0703–1.7076 million people), and 11.3012 million people (4.9886–16.9286 million people), accounting for 7.41% (3.30–11.14%), 7.05% (3.13–10.53%), and 6.94% (3.06–10.39%) of the total population in the CPUA, respectively. It could be seen that it was extensive for the health damage of the people affected by PM2.5 pollution. At the same time, we could also see that due to the improvement of environmental quality, the number of people whose health were damaged decreased by 495,900 and 128,000, respectively, from 2015 to 2016 and 2016 to 2017. The decline rate reached 4.16% and 1.12%, which could be seen that the measures taken by the government in recent years to solve environmental pollution problems had achieved remarkable benefits.
Due to PM2.5 pollution, there were 38,582 premature deaths in 2015 and the number were 34,112 and 32,786 from 2016 to 2017, respectively, with year-on-year decrease of 4470 and 1326, ranking the first among all health effect ends and reaching 11.59% and 3.89%, respectively. In addition, decrease rates of premature death caused by respiratory disease were 15.56% and 7.52%, respectively, in 2016 and 2017. It can be found that PM2.5 has the most direct and serious impact on the respiratory system. Thus, air pollution abatement can reduce respiratory damage effectively.
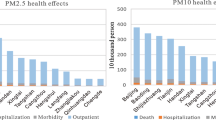
In terms of hospitalization, outpatient service, and illness, PM2.5 pollution caused 165.1 thousand, 165.4 thousand, and 167.8 thousand cardiovascular disease hospitalizations, 303.2 thousand, 303.2 thousand, and 311.0 thousand hospitalizations for respiratory diseases, 3.4 million, 3.2 million, and 3.4 million pediatric outpatient visits, 6.6 million, 6.2 million, and 6.2 million medical outpatient visits, 1.2 million, 1.1 million, and 1.1 million acute upper respiratory tract infections. And 179.9 thousand, 187.8 thousand, and 181.8 thousand people suffered from chronic bronchitis in 2015–2017.
In general, the health effect damages showed a declining trend from 2015 to 2017, which should be attributed to the strict implementation of pollution control policy by the government.
In terms of the structure of the health effect damages, it can be seen from the data in Table 4 that the number of outpatients was the largest, which were 9.98 million, 9.56 million, and 9.47 million in 2015–2017, accounting for 83.70%, 83.69%, and 83.81% of the total number of health effect damages. The number of people suffered from premature death was the lowest among the various health effect ends. Lung cancer was the leading cause in premature death, followed by respiratory disease and cardiovascular disease. For hospitalization, illness and outpatient visits, compared with hospitalization of cardiovascular disease, the number of hospitalization of respiratory diseases is more, and the number of acute upper respiratory infections is higher than that of chronic bronchitis. Besides, the increase in the number of internal medicine was also greater than that of pediatric clinic.
For each city, as shown in Fig. 2, the health effect damages due to PM2.5 pollution in Heze and Zhengzhou were obviously higher than those in other cities, and the damages of Nanyang, Zhoukou, and Handan were also larger, while those of Jincheng and Huaibei and Jiyuan were the smallest. In general, areas with dense population and high pollution concentration are more affected by air pollution.

The number of health effect damages in four types of health effect ends and 30 cities
For all age groups, the older the age, the more premature deaths, and the number of premature deaths began to increase rapidly after the age of 45 to 49 (see Fig. 3).

The number and the proportions of death and pathogenies in different ages and health effect ends
It should be noted that the main cause of premature death was respiratory disease which resulted from PM2.5 pollution before the age of 15. Among the infants between 0 and 4 years old, more than 90% of premature deaths were caused by respiratory disease. After the age of 10, the harm of lung cancer gradually emerged and lung cancer became the main cause of premature death after age of 25. At the 55 to 59 age group, the proportion of premature deaths due to lung cancer to the total deaths were 79.83%, 80.10%, and 79.76%, respectively, from 2015 to 2017. Then, proportions of deaths caused by respiratory disease and cardiovascular disease gradually increased with age. The main cause of death of people at the age above 85 was respiratory disease. It could be seen that due to poor immunity, infants at the age of 0 to 4 and old people at the age above 85 were the vulnerable groups in PM2.5 pollution and respiratory disease did the most harm to these two groups.
Health effect economic loss evaluation
According to the evaluation results of exposure-response relationship model, this paper used the way of disease cost, adjusted human capital, and willingness to pay to quantify the health effect economic loss. The results are shown in Fig. 4.

Health effect economic loss of different health ends from PM2.5 pollution
In 2015–2017, the health effect economic loss of PM2.5 pollution in this area was 97.4 billion RMB (73.03–123.78 billion RMB), 93.52 billion RMB (68.88–116.09 billion RMB), and 94.39 billion RMB (68.97–117.75billion RMB), respectively, accounting for 1.73% (1.30–2.19%), 1.53% (1.13–1.90%), and 1.41% (1.03–1.76%) of the GDP.
Compared with 2016, the health effect economic loss in 2017 increased slightly, but its share of GDP decreased for two consecutive years. That was because the rate of economic growth in 2016–2017 was faster than the decline rate in health effect damaged, which caused the absolute value of health effect economic loss to increase. But its proportion to GDP was declining (see Fig. 5).

Health effect economic loss of PM2.5 pollution and its percentage accounting for GDP
In terms of the structure of health effect economic loss, more than 90% of loss came from chronic bronchitis and premature death. The health effect economic loss of chronic bronchus in 2015–2017 accounted for 67.21%, 67.17%, and 65.99% of the total loss, and the health effect economic loss of premature death accounts for 24.61%, 24.51%, and 25.25% of the total loss, respectively.
For each city, the relative scale of health effect economic loss was basically the same as the relative scale of its health effect damages (see Fig. 6). Health effect economic loss in Heze and Zhengzhou was still significantly greater. Health effect economic loss in Handan, Liaocheng, and Nanyang was also high, while those in Huaibei, Hebi, and Jiyuan were the lowest. Though health effect damages of some cities were smaller than those of other cities, their health effect economic loss is large, which was caused by higher per capita GDP. In conclusion, the health effect economic loss was large in densely populated, economically developed, and highly polluted areas, which was consistent with the changing law of health effect damages.

Health effect economic loss from PM2.5 pollution in four types of health ends in 30 cities
As shown in Fig. 7, in terms of the health effect economic loss of specific age and specific disease, the results were similar to the change in the scale of health effect damaged. In the age from 0 to 40, the health effect economic loss was relatively small and then began to gradually increase. However, unlike the continuous upward trend of health effect damages, the health effect economic loss had not always increased with age increasing. At the age from 60 to 64, the health effect economic loss reached its peak and then began to decline. This is because premature deaths among young people cause more health effect economic loss than premature deaths among older people, because young people lose more life expectancy. Among the three diseases, the health effect economic loss due to lung cancer was the biggest economic loss, and it showed an upward trend. In 2015–2017, the economic loss caused by lung cancer accounted for 63.59%, 64.19%, and 64.86% of the total health effect economic loss of premature death, respectively.

Health effect economic loss of different ages and pathogenies from premature death
Discussion
This paper collected the daily monitoring data of PM2.5 and relevant data of mortality, hospitalization rate, outpatient rate, and morbidity in 30 cities in CPUA and carried out health effect damage analysis by using exposure-response relationship model. Then, the economic loss was evaluated by using the methods of disease cost, adjusted human capital, and willingness to pay. However, there are still some uncertainties in this paper.
(1) Method for assessing the health effect economic loss.
The economic loss assessment method used in this paper only quantifies the loss that directly related to social economy, and it does not take into account the subjective loss factors such as mental loss, which may make the assessment results smaller than the actual situation.
(2) Selection of the health effect ends.
After fully considering the coverage of health effect ends, nine health effect ends with high correlation with PM2.5 pollution have been selected in this paper. However, the research on exposure-response coefficients are not completely accessible; thus, this paper cannot cover all health effect ends, which may make the evaluation results lower than the actual situation.
(3) The exposure-response coefficients.
Due to the different characteristics of PM2.5 pollution from different regions or cities, the exposure-response coefficients are also different, which makes the assessment results different from the actual situation. But all of the exposure-response coefficients selected in this paper are taken from the research results of Chinese scholars, which can better adapt to the actual situation of China and reduce the evaluation error.
(4) The distribution of exposure population and PM2.5 concentration.
In order to facilitate calculation, this paper assumed that the exposed population and PM2.5 concentration is evenly distributed in different cities without considering the characteristics of population and concentration in different areas. To some extent, it may underestimate the loss of heavily polluted and densely populated areas and overestimate the loss of rural areas with low pollutant concentration and areas with small population density, which may make the evaluation results different from the actual situation.
Conclusions and policy implications
Conclusions
(1) Though the PM2.5 pollution in CPUA has caused a huge health effect and health effect economic loss, due to the improvement of environmental quality, there was a decline in the ratio of health effect economic loss accounting for GDP, which was from 1.73% (1.30–2.19%), 1.53% (1.13–1.90%) to 1.41% (1.03–1.76%) in 2015, 2016, and 2017. For health effect, it is the largest in increasing the number of outpatients. While for the health effect economic loss, they mainly come from the premature death and chronic bronchitis. For the health effect economic loss due to premature death, the lung cancer accounts for the largest proportion and the proportion is continuously increasing.
(2) Infants at the age from 0 to 4 and the older people at the age above 85 are the vulnerable groups in PM2.5 pollution. Because the respiratory system of the infants or young children is in the developmental stage, and the body of the older is gradually weakened. From the results, it can be seen for people under the age of 15 and above 85, the main cause of their premature death of PM2.5 pollution is respiratory disease.
(3) Health effect economic loss in cities, such as Heze, Zhengzhou, Handan, and Liaocheng, is higher than that in other cities, which indicates that the cities of dense population and developed economy suffer a severer health effect economic loss.
Policy implications
(1) Continue to strictly implement environmental protection policies and reduce PM2.5 emissions.
This paper shows that China’s environmental protection policy has achieved remarkable results in recent years. The government should continue to strictly implement environmental protection policies, reduce the use of traditional energy sources, especially coal, increase the proportion of clean energy use, remove excess capacity, improve the clean production audit of heavy industry-related enterprises, and carry out vehicle restrictions while developing public transportation to reduce PM2.5 emissions.
(2) Focus on vulnerable groups, namely children and the elderly, with a special focus on respiratory diseases due to PM2.5 pollution. Children and the elderly are vulnerable groups in PM2.5 pollution and are much more affected than other age groups. Therefore, health protection measures for these two groups should be formulated from both the government and residents’ perspectives.
(3) For cities with dense population, developed economy and large health effect economic loss, combined with urban pollution source structure to reduce air pollution. For example, the air pollution source structure of Zhengzhou belongs to the partial motor vehicle category, the Handan belongs to the comprehensive industrial pollution, and the Liaocheng belongs to the meta-coking iron. The emission reduction measures should be formulated according to the structural characteristics of different pollution sources in these cities to reduce the health effect damaged of PM2.5.
References
Balakrishnan K, Dey S, Gupta T, Dhaliwal RS, Brauer M, Cohen AJ et al (2019) The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: the Global Burden of Disease Study 2017. Lancet Pl Health 3(1):26–39
Brand C, Hunt A (2018) The health costs of air pollution from cars and vans. http://www.avere-france.org/Uploads/Documents/152879228236476690cc516267e8de491a2937d48b-The_health_costs_of_air_pollution_from_cars_and_vans_20180518.pdf
Burnett RT, Cakmak S, Brook JR, Krewski D (1997) The role of particulate size and chemistry in the association between summertime ambient air pollution and hospitalization for cardiorespiratory diseases. Environ Health Perspect 105(6):614–620
Cao J, Wang S, Han W, Gui C, Song D (2018) Spatial and temporal distribution of PM2.5 in Henan province. J Atmos Environ Opt 13(01):42–51
Chen S, Bloom DE (2019) The macroeconomic burden of noncommunicable diseases associated with air pollution in China. PLoS One 14(4)
Chen X, Shao S, Tian Z, Xie Z, Yin P (2017) Impacts of air pollution and its spatial spillover effect on public health based on China’s big data sample. J Clean Prod 142:915–925
Chen X (2008) Evaluating the health damage costs of atmospheric particulates. Xiamen University, Fujian
Cromar KR, Gladson LA, Ewart G (2019) Trends in excess morbidity and mortality associated with air pollution above American Thoracic Society–recommended standards, 2008–2017. Ann Am Thorac Soc 16(7):836–845
Dai H, Song W, Gao X, Chen L (2004) Study on relationship between ambient PM10, PM2.5 pollution and daily mortality in a district in Shanghai. J Hyg Res 33(3):293–297
De Leon AP, Anderson HR, Bland JM, Strachan DP, Bower J (1996) Effects of air pollution on daily hospital admissions for respiratory disease in London between 1987-88 and 1991-92. J Epidemiol Community Health 50(Suppl 1):63–70
Fang D (2014) Impact assessment of air pollution on the population health in major cities of China. Nanjing University, Jiangsu
Ghude SD, Chate DM, Jena C, Beig G, Kumar R, Barth MC, Pfister GG, Fadnavis S, Pithani P (2016) Premature mortality in India due to PM2.5 and ozone exposure. Geophys Res Lett 43(9):4650–4658
Geng N, Wang J, Xu Y, Zhang W, Chen C, Zhang R (2013) PM2.5 in an industrial district of Zhengzhou, China: chemical composition and source apportionment. Particuology 11(1):99–109
Hashmi DR, Shareef A, Qadri TR, Azam M (2019) Imperiling on urban environment by air pollution and its impact on human health. Pak J Sci Ind Res Ser A Phys Sci 62(2):104–112
He G, Fan M, Zhou M (2016) The effect of air pollution on mortality in China: evidence from the 2008 Beijing Olympic Games. J Environ Econ Manag 79:18–39
Hu B, Chen R, Xu J, Yang G, Xu D, Chen C, Zhao Y (2015) Health effects of ambient ultrafine (nano) particles in haze. Chin Sci Bull 60(30):2808–2823
Hu J, Wang H, Zhang J, Zhang M, Zhang H, Wang S, Chai F (2019) PM2.5 pollution in Xingtai, China: chemical characteristics, source apportionment, and emission control measures. Atmosphere 10(3):121
Hu W, Wei F, Jim Z, Wu G, Teng E, Chapman RS (2001) Study on relation between air pollution and children’s respiratory illness prevalence using two-step regression method. China Environ Sci 21(6):485–489
Huang D, Zhang S (2013) Health benefit evaluation for PM2.5 pollution control in Beijing-Tianjin-Hebei region of China. China Environ Sci 33(1):166–174
Huang J, Pan X, Guo X, Li G (2018) Health impact of China’s air pollution prevention and control action plan: an analysis of national air quality monitoring and mortality data. Lancet Pl Health 2(7):313–323
Jing L, Qin Y, Xu Z (2000) Relationship between air pollution and acute and chronic respiratory disease in Benxi. J Environ Health 17(5):268–270
Kan H, Chen B (1989) Analysis of exposure-response relationships of air particulate matter and adverse health outcomes in China. J Environ Health 06:422–424
Khaniabadi YO, Sicard P, Takdastan A, Hopke PK, Taiwo AM, Khaniabadi FO, de Marco A, Daryanoosh M (2019) Mortality and morbidity due to ambient air pollution in Iran. Clin Epidemiol Global Health 7(2):222–227
Lelieveld J, Klingmüller K, Pozzer A, Pöschl U, Fnais M, Daiber A, Münzel T (2019) Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur Heart J 40(20):1590–1596
Li L, Lei Y, Wu S, Chen J, Yan D (2017) The health economic loss of fine particulate matter (PM2. 5) in Beijing. J Clean Prod 161:1153–1161
Li W, Pei L, Li A, Luo K, Cao Y, Li R, Xu Q (2019) Spatial variation in the effects of air pollution on cardiovascular mortality in Beijing, China. Environ Sci Pollut R 26(3):2501–2511
Liu J, Han Y, Tang X, Zhu J, Zhu T (2016) Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci Total Environ 568:1253–1262
Liu X, Xie P, Liu Z, Li T, Zhong L, Xiang Y (2010) Economic assessment of acute health impact due to inhalable particulate air pollution in the Pearl River Delta. J Peking Univ Nat Sci Ed 46:829–834
Maji KJ, Ye W, Arora M, Nagendra SS (2018) PM2.5-related health and economic loss assessment for 338 Chinese cities. Environ Int 121:392–403
Matus K, Nam KM, Selin NE, Lamsal LN, Reilly JM, Paltsev S (2012) Health damages from air pollution in China. Glob Environ Chang 22(1):55–66
Miao W, Huang X, Song Y (2017) An economic assessment of the health effects and crop yield losses caused by air pollution in mainland China. Environ Health Perspect 56:102–113
Ministry of Ecology and Environment of the People's Republic of China. Chinese Environmental Situation Communique in 2013. http://www.mee.gov.cn/hjzl/zghjzkgb/lnzghjzkgb/201605/P020160526564151497131.pdf. Accessed 27 May 2014
Ministry of Ecology and Environment of the People's Republic of China. Chinese Environmental Situation Communique in 2016. http://www.mee.gov.cn/hjzl/zghjzkgb/lnzghjzkgb/201706/P020170605833655914077.pdf. Accessed 5 June 2017
Ministry of Ecology and Environment of the People's Republic of China. Chinese Environmental Situation Communique in 2018. http://www.mee.gov.cn/hjzl/zghjzkgb/lnzghjzkgb/201905/P020190619587632630618.pdf. Accessed 29 May 2019
Miraglia SGEK, Saldiva PHN, Böhm GM (2005) An evaluation of air pollution health impacts and costs in São Paulo, Brazil. Environ Manag 35(5):667–676
Miri M, Derakhshan Z, Allahabadi A, Ahmadi E, Conti GO, Ferrante M, Aval HE (2016) Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran. The AirQ model approach. Environ Res 151:451–457
Nam KM, Selin NE, Reilly JM, Paltsev S (2010) Measuring welfare loss caused by air pollution in Europe: a CGE analysis. Energ Policy 38(9):5059–5071
National Development and Reform Commission of the People’s Republic of China (2016) Circular of the National Development and Reform Commission on printing and distributing the development plan of the Central Plains Urban Agglomeration. http://www.ndrc.gov.cn/zcfb/zcfbghwb/201701/t20170105_834451.html
Phosri A, Ueda K, Phung VLH, Tawatsupa B, Honda A, Takano H (2019) Effects of ambient air pollution on daily hospital admissions for respiratory and cardiovascular diseases in Bangkok, Thailand. Sci Total Environ 651:1144–1153
Pope CA III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. Jama 287(9):1132–1141
Qiu H, Zhu X, Wang L, Pan J, Pu X, Zeng X, Zhang L, Peng Z, Zhou L (2019) Attributable risk of hospital admissions for overall and specific mental disorders due to particulate matter pollution: a time-series study in Chengdu, China. Environ Res 170:230–237
Qu F, Liu F, Zhang H, Chao L, Guan J, Li R, Yu F, Yan X (2019) The hospitalization attributable burden of acute exacerbations of chronic obstructive pulmonary disease due to ambient air pollution in Shijiazhuang, China. Environ Sci Pollut R 26(30):30866–30875
Samet JM, Dominici F, Curriero FC, Coursac I, Zeger SL (2000) Fine particulate air pollution and mortality in 20 US cities, 1987–1994. New Engl J Med 343(24):1742–1749
Sun D, Fang J, Sun J (2018) Health-related benefits of air quality improvement from coal control in China: evidence from the Jing-Jin-Ji region. Resour Conserv Recycl 129:416–423
Tian X, Dai H, Geng Y, Wilson J, Wu R, Xie Y, Hao H (2018) Economic impacts from PM2.5 pollution-related health effects in China’s road transport sector: a provincial-level analysis. Environ Int 115:220–229
Magat WA, Huber J (1991) Pricing environmental health risks: survey assessment of risk-risk and risk-dollar trade-offs for chronic bronchitis. J Environ Econ Manag 21:32–51
Nagpure AS, Gurjar BR, Martel JC (2014) Human health risks in national capital territory of Delhi due to air pollution. Atmos Pollut R 5(3):371–380
Wang Y, Li J, Li A, Xie P, Zheng H, Zhang Y, Wang Z (2016) Modeling study of surface PM2.5 and its source apportionment over Henan in 2013–2014. Acta Sci Circumst 36:3543–3553
Wong CM, Atkinson RW, Anderson HR, Hedley AJ, Ma S, Chau PYK, Lam TH (2002) A tale of two cities: effects of air pollution on hospital admissions in Hong Kong and London compared. Environ Health Perspect 110(1):67–77
Wu R, Dai H, Geng Y, Xie Y, Masui T, Liu Z, Qian Y (2017) Economic impacts from PM2. 5 pollution-related health effects: a case study in Shanghai. Environ Sci Technol 51(9):5035–5042
Wu W, Xue W, Wang Y, Lei Y, Feng T, Cai Z (2019a) Health benefit evaluation for air pollution prevention and control action plan in China. Environ Sci 40(07):2961–2966
Wu T, Ma Y, Wu X, Bai M, Peng Y, Cai W, Wang Y, Zhao J, Zhang Z (2019b) Association between particulate matter air pollution and cardiovascular disease mortality in Lanzhou, China. Environ Sci Pollut R 26(15):15262–15272
Xie P, Liu X, Liu Z, Li T, Bai Y (2009) Exposure-response functions for health effects of ambient participate matter pollution applicable for China. China Environ Sci 29(10):1034–1040
Zhang H, Niu Y, Yao Y, Chen R, Zhou X, Kan H (2018) The impact of ambient air pollution on daily hospital visits for various respiratory diseases and the relevant medical expenditures in Shanghai, China. Int J Environ Res Public Health 15(3):425
Zhao X, Fan C, Wang Y (2014) Evaluation of health losses by air pollution in Beijing: a study based on corrected human capital method. China Popul Resour Environ 24:169–176
Zhou J (2013) Health effects of air pollution. B Chinese Acad Sci 3:371–377
Funding
The support was from the National Natural Science Foundation of China under Grant No. 71803182 and 71773118, Beijing Social Science Foundation Project under Grant No.19YJC023, Open Fund of State Key Laboratory of Water Resource Protection and Utilization in Coal Mining under Grant No. SHJT-17-42.20.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Eyup Dogan
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fu, X., Li, L., Lei, Y. et al. The economic loss of health effect damages from PM2.5 pollution in the Central Plains Urban Agglomeration. Environ Sci Pollut Res 27, 25434–25449 (2020). https://doi.org/10.1007/s11356-020-08560-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-020-08560-3