
Abstract
Ho Chi Minh City (HCMC) is changing and expanding quickly, leading to environmental consequences that seriously threaten human health. PM2.5 pollution is one of the main causes of premature death. In this context, studies have evaluated strategies to control and reduce air pollution; such pollution-control measures need to be economically justified. The objective of this study was to assess the socio-economic damage caused by exposure to the current pollution scenario, taking 2019 as the base year. A methodology for calculating and evaluating the economic and environmental benefits of air pollution reduction was implemented. This study aimed to simultaneously evaluate the impacts of both short-term (acute) and long-term (chronic) PM2.5 pollution exposure on human health, providing a comprehensive overview of economic losses attributable to such pollution. Spatial partitioning (inner-city and suburban) on health risks of PM2.5 and detailed construction of health impact maps by age group and sex on a spatial resolution grid (3.0 km × 3.0 km) was performed. The calculation results show that the economic loss from premature deaths due to short-term exposure (approximately 38.86 trillion VND) is higher than that from long-term exposure (approximately 14.89 trillion VND). As the government of HCMC has been developing control and mitigation solutions for the Air Quality Action Plan towards short- and medium-term goals in 2030, focusing mainly on PM2.5, the results of this study will help policymakers develop a roadmap to reduce the impact of PM2.5 during 2025–2030.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ho Chi Minh City (HCMC), a megapolis with great economic potential, is the economic locomotive of Vietnam (Gubry & Le 2014; Phung et al. 2020). Along with the capital Hanoi in the North, HCMC is a city of special urban type and is the country’s largest economic, political, cultural, and educational centre (Linh et al. 2019; Department of Statistics Ho Chi Minh City-a, 2019). Air quality in HCMC is affected by meteorological conditions along with emissions from local sources, of which local emissions have the most significant influence (Bui et al. 2021). Accelerating the process of industrialisation, urbanisation, and mechanisation in urban areas has increased emissions and energy consumption significantly, leading to the emission of many pollutants, and air pollution has become an increasingly serious environmental problem (Ho et al. 2019; Phung et al. 2020). The results of the 2017 emissions inventories of Ho et al. (2019) and Vu et al. (2020) show that there are approximately 4029 tons of PM2.5/year of emissions. Approximately 1813.1 tons/year, accounting for 45%, come from road sources (on-road and non-road). 926.7 tons/year (23%) come from regional waste sources (domestic activities), and 1289.3 tons/year (32%) come from point waste sources (public production activities).
PM2.5 concentration in the wet season is usually lower than that in the dry season (Phan et al. 2020) because rainfall and air humidity are often much lower (Pillai et al. 2002; Glavas et al. 2008). Different weather trends as well as meteorological conditions typically create seasonal fluctuations in PM2.5 concentrations. From August to October 2014 (wet season), the average PM2.5 concentration (measured) was 97.79 ± 63.07 µg/m3, whereas the average PM2.5 concentration from March to May 2015 (dry season) was 168.20 ± 104.85 µg/m3 (about 1.72 times higher) (Phan et al. 2020). For PM2.5 pollution, HCMC had a large variation between hours of the day but very little seasonal variation; it regularly had high levels of PM2.5, lasting for several hours with concentrations above 75 µg/m3, but there were no long-term pollution episodes (Thu et al. 2018). Based on the research results of Thu et al. (2018) and Hien et al. (2019), PM2.5 pollutants in HCMC are a combination of urban pollutants (from industrial, transport, energy, and residential sources) and pollutants from elsewhere carried through the circulation of air masses along the southern coast of the HCMC.
PM2.5 pollution is formed through complex chemical and physical processes (B. Zhao et al. 2019), which is considered an important parameter for assessing the level of air pollution (Huy et al. 2018; Toledo et al. 2018; Chen et al. 2020; Ha Chi & Kim Oanh 2021). PM2.5 concentrations are significantly influenced by anthropogenic emission sources, such as emissions from vehicles, biomass burning, and fossil fuel combustion, typically with sulphur dioxide (SO2), nitrogen oxides (NOx), ammonia (NH3), black carbon (BC), organic carbon (OC), and non-methane volatile organic compounds (NMVOCs) (Fiore et al. 2015; von Schneidemesser et al. 2015; Chen et al. 2020).
Low- and middle-income countries (LMICs) often suffer from the effects of air pollution on public health, with millions of deaths each year owing to fine particulate matter (PM2.5) (Kuylenstierna et al. 2020). Therefore, protecting public health is an important goal of air pollution control (B. Zhao et al. 2019), and the effectiveness of these control strategies has been demonstrated at the regional scale and global (Kuylenstierna et al. 2020). Quantitative research on costs-economic benefits when implementing measures to control and reduce air pollution has attracted attention from many different countries, typically in Korea, with research by Chae and Park (2011) and Kim et al. (2019); the USA has a study by Pan et al. (2019) and Sacks et al. (2018); South Africa has the study of Altieri and Keen (2019); Spain has the study of Boldo et al. (2014), especially China with a block; and a large number of studies have been published, typically the study of Voorhees et al. (2014), Ding et al. (2016), Chen et al. (2017a, b, c), Li et al. (2019), Song et al. (2019), and Xing et al. (2019). Particularly in some Southeast Asian countries, including Thailand, Ha Chi and Kim Oanh (2021) have also built basic technologies and frameworks for quantification about damage/benefit caused by PM2.5 fine dust problems. Furthermore, to quantify the damage/benefit caused by PM2.5 fine dust exposure, the analysis and evaluation of the spatial distribution of PM2.5 concentrations is extremely important.
Several tools have been developed to rapidly estimate economic losses and public health risks due to changes in air quality, based on concentration–response functions (CRFs) (Bayat et al. 2019). The Benefits Mapping and Analysis Program (BenMAP) software has proven to be one of the most comprehensive tools (Anenberg et al. 2016), and the AirQ + tool developed by the WHO has also been used (WHO 2018). Various methods have been studied and applied to determine the functions of CRFs in the relationship between surface changes in air quality and human health impacts, including linear, logarithmic, and hybrid methods (R. Burnett et al. 2018). Along with the above tools, a group of scientists from universities and research institutes in China and the USA have built a separate platform called ABaCAS (Air Benefit and Cost and Attainment Assessment System) to analyse, quantify, and evaluate the benefits achieved by reducing air pollution, especially PM2.5 and ground-level O3, to achieve the goals of socio-economic development and a sustainable environment (Voorhees et al. 2014; Ding et al. 2016; Chen et al. 2017a, b, c; Li et al. 2019; Song et al. 2019; Xing et al. 2019). These studies have focused on analysing and clarifying how the current state of air quality (mainly PM2.5) will benefit when applying a series of mitigation solutions and measures. Investment costs and cost optimisation when implementing measures to control and minimise air pollution were also evaluated. Finally, the benefits of air pollution control on public health and the local economy are quantified.
To improve the current state of residents’ health in the HCMC facing environmental challenges, it is necessary to have solutions to overcome, minimise impacts of, and calculate economic benefits/costs due to short-term exposure to PM2.5 pollution. Assessment of acute and long-term (chronic) impacts is an important step towards developing a sustainable solution. This study has the overall objective of shaping computational technology; assessing the environmental, economic, and social benefits based on integrated technology; and applying mathematical models, databases, and geographic information systems (GIS). The objective of this study was to quantify the damage caused by PM2.5 pollution, taking 2019 as the base year. The results of this study will help clarify the limitations of enforcement policies and provide timely support for managers to adjust strategies and policies to effectively reduce air pollution.
Materials and methods
Description of study area
HCMC has 268,000 businesses, accounting for 31% of the country. A number of projects with foreign investment capital (FDI) in Ho Chi Minh City alone in 2019 had 1320 newly licenced projects (HCMC People’s Committee 2019) reflecting the growth of this mega-urban economy. Strong economic development has brought many important achievements; typically, gross regional domestic product (GRDP) reached more than 1.34 million billion VND (up to 8.32% compared to 2018), and attracted foreign investment reached 8.3 billion USD (up 39.00% compared to 2018) (HCMC Statistical Office 2020). Provincial competitiveness index (PCI) of Ho Chi Minh City for 5 consecutive years (2015–2019) has been at a good level, of which the composite PCI score (PCI score) in 2019 reached 67.16 (1028 times higher than 2018) and had a similar trend with 10 component PCI indices (PCI subindices) (Loc et al. 2019; Vietnam 2021; Table S1).
Economic development also gives rise to environmental pollution problems, especially ambient air pollution and PM2.5 problem (HCMC DNRE 2018). For sustainable development for the period of 2020–2025 and orientation to 2030, the city government HCMC has continued to implement solutions to depollute the environment to achieve the goals of sustainable development. Specifically, the “Program to reduce environmental pollution in the period 2020–2030” focuses on the goals of promoting high-tech investment, encouraging the use of advanced technology and equipment in production and business, and minimising quality waste and control and thoroughly treat pollution, combine waste treatment to create energy, protect and improve the quality of the ecological environment, and focus on construction solutions to serve the work of pollution reduction environment (MPC 2020).
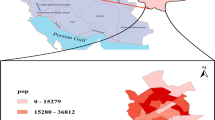
To facilitate further analysis and evaluation, in this study, HCMC was divided into five suburban areas (sub-divisions) as follows: (1) the central urban area (SG1) includes districts 1, 3, 4, 5, 6, and 6. 8, District 10, District 11, Phu Nhuan District, Binh Thanh District, Tan Phu District, Tan Binh District, and Go Vap District; (2) the Eastern Urban Area ( SG2) includes District 9, District 2, and Thu Duc; (3) Western urban areas ( SG3) include Binh Tan District and Binh Chanh District; (4) Southern urban area ( SG4) includes District 7, Nha Be District, and Can Gio District; and (5) Northern Urban Area (SG5) includes District 12, Hoc Mon District, and Cu Chi District. The study area and the characteristics of its PCI index in Fig. 1.

Study area (HCMC): five urban sub-divisions, the population in 2019, and PCI changes during 2015–2019
Analysis of PM2.5 concentration distribution
Meteorological factors can significantly affect the spatial and temporal distribution of PM2.5. Therefore, meteorological conditions were considered during the simulation process of PM2.5 concentration in HCMC by the coupled WRF/CMAQ models, which has been demonstrated in various studies worldwide, typically in the USA (DeGaetano & Doherty 2004; Tai et al. 2010), China (Tu et al. 2007; Chen et al. 2017c; Ding et al. 2019; Hu et al. 2021), and Vietnam (Tran et al. 2020; Bui & Nguyen 2023). Meteorological factors can help reduce PM2.5 pollution levels and consequently lower human health risks. However, seasonal fluctuations in meteorological conditions have caused unexpected effects on air pollution. In HCMC, under a combination of meteorological factors and emission sources (mainly transportation and industrial processes), PM2.5 air pollution levels vary greatly during the day and have small seasonal fluctuations. The peak levels of PM2.5 often last for several hours with a few long-term episodes of pollution (Thu et al. 2018).
The offline WRF model ver.3.8 (Skamarock et al. 2008) is used to simulate meteorological conditions. The NCEP (the National Center for Environmental Prediction) Final (FNL) Operational Global Analysis data every 6 h that has a spatial resolution of 1.0° × 1.0° from the US National Center for Atmospheric Research (NCAR) (https://rda.ucar.edu/datasets/ds083.2/) was used as the initial and boundary conditions and the heuristic analysis for the WRF model. The NCEP FNL data is generated from the Global Data Assimilation System (GDAS) (NCEP 2000) based on continuously collected data sources. These are meteorological parameters such as surface pressure, sea level pressure, geologic temperature, sea surface temperature, soil temperature, ice cover, relative humidity, wind vector U, and wind vector V. FNL data have been used in many studies to simulate meteorological conditions and air quality in various regions of the world (Wang et al. 2021a, b). The global topographical surface data package used as input for the WRF model was acquired from the United States Geological Survey (USGS) provided by the University Corporation for Atmospheric Research (UCAR) (NCAR 2020). This dataset consists of seven main groups of data, namely, terrain elevation, topographic features, land use, soil type, soil temperature, vegetation cover ratio, and the Albedo index, with a detailed data resolution of approximately 2 min (~ 3.7 km).
These study simulations started on 15 December 2018 and continued for all 12 months of 2019 (from 00:00 local standard time (LST) of 1 January 2019 to 23:00 LST on 31 December 2019). The first 5 days of the simulation were used to establish the depth of soil temperature and humidity because soil effects are often used to optimise surface moisture and temperature parameters (Pleim & Xiu 2003; Pleim & Gilliam 2009; Qin et al. 2019). The CMAQ model ver.5.2.1 (http://cmascenter.org/cmaq/) was updated and published in June 2017 by the US Environmental Protection Agency (U.S. EPA) (Borge et al. 2014; Hu et al. 2015; Lang et al. 2017) and was applied to simulate the concentration distribution of PM2.5 concentration in this study area between 1 January 2019 and 31 December 2019.
The meteorological factor characteristic data, which comprise the WRF model output and the CMAQ model input data, were processed by the Meteorology-Chemistry Interface Processor (MCIP) tool (version 4.5.3) to generate input formats that satisfy the CMAQ model requirements. To ensure the accuracy of boundary conditions of meteorological fields, the horizontal domains of the conventional WRF model are slightly larger than that of the CMAQ model (Li et al. 2022). The CMAQ model in this study is configured with the same nested domains as the WRF model, but three grid cells in each direction of the computed domains are removed from the domains D01, D02, and D03 of the WRF model. For the CMAQ model, there are a total of 29 classes in the sigma coordinate system; specifically, the sigma values (σ) for the CMAQ calculation domains at the class boundaries are 1000, 0.997, 0.990, 0.983, 0.976, 0.970, 0.962, 0.954, 0.944, 0.932, 0.917, 0.898, 0.874, 0.844, 0.806, 0.760, 0.707, 0.647, 0.582, 0.513, 0.444, 0.375, 0.308, 0.243, 0.183, 0.126, 0.073, 0.023, and 0.000. At the same time, the Carbon Bond 6 (CB6r3) (Yarwood et al. 2010; Emery et al. 2015; Luecken et al. 2019) for chemical substances has also been built in the CMAQ model. Man-made emissions of NOx, CO, CH4, NH3, SO2, and VOCs (in the year 2018) are obtained from the global anthropogenic emission inventory including CAMS-GLOB-ANT ver.4.1 and CAMS-GLOB-AIR ver.1.1 (Granier et al. 2019) with a spatial resolution of 0.1° × 0.1° grids and 0.5° × 0.5° grids, respectively. For biogenic emissions obtained from the global biogenic emissions inventory such as CAMS-GLOB-BIO ver.2.1 (Granier et al. 2019) of NOx and VOCs (in 2018), they are grids with a spatial resolution of 0.25º × 0.25º. All these emissions are interpolated linearly (Jiang et al. 2010; Liu et al. 2013; Wang et al. 2016) into the internal domain of resolution space of 3.0 km × 3.0 km and used to simulate PM2.5 concentration on the domain D03 (HCMC). The detailed technical description of the nested domains in the coupled WRF/CMAQ models used in this study is shown in Table S2.
Health impact assessment
Health impact functions (HIFs) have been widely used in many previous studies to assess the burden of disease associated with short- and long-term PM2.5 exposure such as Lelieveld et al. (2013), Song et al. (2017), Zhao et al. (2019), Dedoussi et al. (2020), and Wang et al. (2021ab). Thus, we estimated the health effects for HCMC’s residents due to acute PM2.5 exposure using the log-normal model (Sacks et al. 2018, 2020) and chronic exposure by applying the integrated expose-response function (IER) (Burnett et al. 2014).
In this study, a Monte Carlo numerical simulation procedure was applied to estimate the 95% confidence intervals (CI) (Chen et al. 2017a; Sacks et al. 2018; Altieri & Keen 2019) for the average number of premature deaths and hospitalisations of each type of health endpoint. Each calculation was simulated in the short- and long-term health impact models. For each health endpoint type, we randomly selected values from the probability distribution of each CRF coefficient and combined them with the baseline incidence rate values to calculate the corresponding health impact level based on the selected values. All numerical simulation computations were run continuously (~ 5000 times) to determine the 95% CI results for the distribution of health-affected cases (premature mortality and hospitalisation) due to exposure to PM2.5.
Estimating long-term (chronic) health effects
The IER model (Burnett et al. 2014) was applied to estimate long-term health effects. This model is based on cohort studies of ambient PM2.5 in the USA and Europe, consisting of cigarette smoke and household solid fuel burning included in the exposure calculation. PM2.5 could be up to approximately 30,000 μg/m3 (Burnett et al. 2014; Cohen et al. 2017). This model also provides a concentration–response relationship for a range of PM2.5 concentrations in the atmosphere (Wang et al. 2020). The IER model has been used in the Global Burden of Disease (GBD) studies by Lim et al. (2012) and Cohen et al. (2017). Furthermore, the IER model has also been used to assess premature mortality from PM2.5 exposure in China, especially from 2013 to 2017 (Song et al. 2017; Gao et al. 2018; Maji et al. 2018; Wang et al. 2018; Liu et al. 2020; Wu et al. 2021). The IER function is expressed in Eqs. (1) and (2), the evaluation function that has been reviewed and proven to be the most suitable for calculating health risks among many different valuation functions (Burnett et al. 2014; Cohen et al. 2017).
where HIlong-term or ΔYi is the value of the public health impact related to the premature mortality of diseases caused by PM2.5 pollution attributed to health endpoint i mentioned above; BIRi is the baseline mortality incidence of health endpoint type i exposed at the 2019 annual average PM2.5 concentration in the current state (C); EP is the population size exposed to PM2.5 in the form of a grid with a resolution of ~ 3.0 km × 3.0 km consistent with the current PM2.5 concentration data (C); C0 is the level of PM2.5 concentration below the threshold that is not expected to affect public health; C0 is referenced between 5.8 and 8.0 µg/m3 (Hao et al. 2021); RRi is the relative risk value for each type of calculated loss; and αi, γi, and δi are the regression parameters studied for health endpoint type i.
In this study, the health endpoints and IER parameters, including αi, γi, and δi as studied by Burnett et al. (2014) and Song et al. (2017), were applied and used. The parameters and selection of HIFs for the different types of health endpoints were classified according to the ICD-10 report (10th version of the International Classification of Diseases). Within this classification, circumstances that may overlap with other health effects (ICD-10, 2016) are shown in Table 1. The types of damage assessed include chronic obstructive pulmonary disease (COPD), ischaemic heart disease (IHD), lung cancer (LC), and stroke in adults and elderly groups, while acute lower respiratory infection (ALRI) occurs in children. The map showing the relative risk distributions of premature deaths from IHD, stroke, COPD, and LC in a ~ 3.0 × 3.0 km2 grid is reported in Fig. S1.
Estimating short-term (acute) health effects
To assess the health effects of short-term PM2.5 exposure (premature mortality and hospitalisation), concentration–response functions (CRFs) were developed by epidemiological studies, based on time series analysis of interactions between PM2.5 concentrations and health (Zhao et al. 2019). Notably, in most of the studies by Dominici et al. (2002), Kan et al. (2007), Huang et al. (2012ab), Shang et al. (2013), Wang et al. (2015), and Sui et al. (2021), the baseline mortality and morbidity incidence rates caused by PM2.5 pollution were considered to have a Poisson distribution. Subsequently, the relationship between the number of deaths and diseases and PM2.5 concentration could be determined by Poisson or Log-linear regression or several similar methods (Dominici et al. 2002; Kan & Chen 2004; Kan et al. 2008; Shang et al. 2013). In this study, the model had a log-normal form, as described by Eq. (3) (Chen et al. 2017b; Sacks et al. 2018, 2020), which are used to estimate the daily short-term effects of PM2.5 on human health. The coefficients of the CRFs (β) were determined using Eq. (4), based on the RR values (Andreão et al. 2020).
where ΔYi is the number of hospitalisations in this study due to short-term exposure to the type of health endpoint i; BIRi is the baseline incidence rate of health endpoint type i (the mortality/morbidity rate before the change in PM2.5 concentration); EP is the exposed population with short-term exposure to PM2.5; C’0 is the level of PM2.5 concentration below the threshold that is not expected to affect public health (24-h average); C – C’0 or ΔPM2.5 is the change in PM2.5 concentration level in the current state compared with the recommended threshold; βi is the regression coefficient of CRFs determined from epidemiological studies that describe the corresponding RRi of health endpoint type i with 95% confidence interval (CI); and ΔQ is the change in PM2.5 concentration that epidemiological studies have used to estimate RR, typically ΔQ = 10 μg/m3 or 1 μg/m3. The details of all coefficients βi and RRi used in this study were obtained from our previous detailed study of HCMC in 2018 (Bui & Nguyen 2022).
Economic valuation estimates
In the absence of a market for human lives, the monetary quantification of deaths is based primarily on non-market valuation approaches (OECD 2012). A standard method for estimating the monetary cost of a positive welfare effect, such as a reduction in mortality risk, is to create a hypothetical market for death risk to be considered and analysed based on the value of statistical life (VSL) (Braathen et al. 2010; Xie 2011; Maji et al. 2018). The VSL value is calculated in survey studies assessing individuals’ Willingness to Pay” (∂WTP) to partially reduce the risk of death ∂R (Maji et al. 2018). Thus, for a relatively small value of ∂R, the VSL value is defined as VSL = ∂WTP/∂R (Persson et al. 2001; Huang et al. 2012a, b). When no studies assessed the economic value of life lost, the “Conversion of Benefits’ approach was used. This approach converts unit health costs from international studies to local contexts’ (Johnson et al. 2015; Narain & Sall 2016; Kim et al. 2019), with the main idea being to account for income differences to expand VSL (Yin et al. 2017). The economic cost of illness-related loss is estimated using WTP as well as the Cost of Illness (COI) approach (Maji et al. 2018). The COI method calculates the cost of a disease in terms of medical treatment costs, hospital stay, and reduced productivity (Hoffmann et al. 2012).
In this study, the method of determining VSL and COI values was applied, similar to that described in our previous studies (Bui et al. 2020), (Bui et al. 2021; Bui & Nguyen 2022). Therefore, the total economic valuation cost (EC) or economic health burden due to the decline in public health was evaluated according to Eq. (5) as follows:
where HIi or is the impact level of health endpoint i associated with short- and long-term PM2.5 exposure; HCi,2019 or is the corresponding unit economic value of health endpoint type i (units of VND or USD), and EC (or Economic Burden) is the total value of economic losses due to various types of health damage estimated cause (in VND or USD). The EC value considered in this study corresponds to the total economic value of damage due to both acute and chronic health impacts caused by exposure to PM2.5 pollution in the ambient air in HCMC. Detailed statistics of unit economic values for each specific type of health endpoint caused by PM2.5 pollution are shown in Table S3.
Assessing PM2.5 exposure risks
Regional PM2.5 exposure risk (C. Zhao et al. 2021) was used to quantify differences in exposure to PM2.5 exposure risk across urban and suburban areas, calculated according to Eq. (6) (Zhang et al. 2022) as follows:
where i is the position of the ith grid in the study area, Ri is the risk value of PM2.5 exposure in the population at grid i, EPi is the population size exposed to PM2.5 in grid i, Ci is the PM2.5 concentration level (monthly 24-h average and 2019 annual mean) in the ith grid cell, and n is the total number of grid cells covering the entire study area.
Threshold of PM2.5 concentration (C′0) and baseline incidence rate (BIR)
With the assessment of acute health impacts, the selection of the daily average PM2.5 threshold concentration (C′0) affects the magnitude of the results of the calculation of the number of affected cases (Chinh Nguyen 2013). A wide range of available studies (Vu et al. 2020; Vien et al. 2021; Dang et al. 2021; Bui & Nguyen 2022) have evaluated the HCMC. These studies used the Vietnamese National Ambient Air Quality (NAAQS), such as QCVN 05:2013/BTNMT, and the WHO global air quality guidelines (WHO AQG). The assessment based on these two systems of technical standards can allow detailed quantification of the extent of damage or costs incurred by society as a basis for applying mitigation solutions of PM2.5 concentration to the allowable threshold (Chinh Nguyen 2013). Therefore, the reference C′0 value in this study could be used to include C′0 = 50 µg/m3 according to the NAAQS or C′0 = 15 µg/m3 according to the WHO AQG (WHO 2021).
National baseline values for premature mortality-specific deaths were obtained from the GBD study 2019 (https://ghdx.healthdata.org/gbd-2019) of the Institute for Health Metrics and Evaluation (IHME) (Health Effects Institute, 2020). Values of baseline mortality incidence due to stroke, IHD, COPD, LC, and ALRI for long-term impacts were determined for all regions of Vietnam from the GBD study 2019, being 141.12 (95% CI: 114.81; 166.30), 77.45 (95% CI: 63.76; 92.27), 29.52 (95% CI: 11.07; 36.96), 26.11 (95% CI: 20.23; 32.90), and 22.15 (95% CI: 18.43; 26.68) cases per 105 population, respectively. Meanwhile, the baseline mortality incidence due to all-cause respiratory and cardiovascular diseases for the short-term effects were 79.16 (95% CI: 49.65; 95.68) and 249.20 (95% CI: 209.90; 289.45) cases per 105 population, respectively. The baseline morbidity incidence of all-cause respiratory diseases is approximately 13.79%, and all-cause cardiovascular disease is approximately 8.44%, as captured in the Health Statistical Yearbook (https://moh.gov.vn/thong-ke-y-te) of the Ministry of Health of Vietnam for the provinces of the southeast region in 2019. Moreover, the details of baseline rate values (BIRi) for the types of health endpoints for both mortality and morbidity for each district of HCMC, including stroke, IHD, COPD, and LC, are applied to the short- and long-term impact assessments associated with statistical exposure to PM2.5, as shown in Table S4.
PM2.5-exposed population size (EP)
The population data in this study were collected from the City’s Statistical Yearbook of HCMC in 2019 (HCMC Statistical Office 2020) and the General Statistics Office of Vietnam based on the Report of Results of the 2019 Population and Housing Census (GSO 2020). The national population and housing data of the (GSO 2020) were surveyed as of 1 April 2019 with the resolution of the census data for each province carried out to county levels, divided by sex group, age group, and urban and rural areas of each county.
From the data source as shown in Fig. 1 and Table 2, it can be seen that the total population of HCMC in 2019 is 9038 million people with the total number of men being 4403 million people (accounting for 48.7%) and the total number of women being 4635 million people (contributed 51.3%). In terms of age group distribution, the children (≤ 14 years old) had 1708 million people (18.9%), while the adult (15–64 years old) and elderly (≥ 65 years old) groups had 6824 (75.5%) and 0.506 million people (5.6%). The lowest population is in Can Gio district (71,526 people), with a density of 0.102 thousand people/km2, and the highest population is in Binh Tan district (790,420 people), with a density of 15,195 thousand people/km2.
According to the sub-divisions (Fig. 1), SG1 has the highest exposed population of 4088 million people (45.23%), followed by SG5, SG3, and SG2 with 1630 million people (18.03%), 1506 million people (16.66%), and 1174 million people (12.99%), respectively, and the lowest is in SG4 with only 0.641 million people (7.09%). Detailed statistics on population (total and sex distribution) and population density distribution by district, as well as by the sub-divisions, are shown in Table 2. The gridded spatial distribution data of the total exposed population, the age-specific population, and gender-specific population of HCMC in 2019 with a resolution of ~ 3.0 km × 3.0 km was similarly constructed from a previous study (Bui & Nguyen 2022) which was shown in Fig. 2. The gridded spatial distribution of EP corresponds to the average annual and monthly 24-h average PM2.5 concentration values obtained from the coupled WRF/CMAQ simulation results. These results were incorporated into HIFs to assess the health effects of long-term and short-term PM2.5 exposure in the study area.

The gridded spatial distribution of population by age and gender groups in HCMC in 2019
Conceptual model
The conceptual model and implementation steps are illustrated in Fig. 3. The steps include (1) setting up related databases (database) and (2) selecting the health-economic impact calculation models (computing models) and using the data from steps (1) and (3) performing analysis and evaluation based on the estimated results achieved outcomes. To perform step (1), there are three main groups of data that need to be prepared: data on changes in PM2.5, health datasets, and population size datasets. Statistical exposure, datasets on health (health damage function, mortality rate, and underlying disease) as well as population size exposure (by age group and sex group) were collected from national statistical sources, from the Global Burden of Disease database 2019 as well as from previously available scientific studies. The dataset on the change in PM2.5 concentration according to the daily and annual average was obtained from the simulation results using the combined WRF/CMAQ models (this result has been evaluated and tested in a single and detailed way). In step (2), the values (BIRi, EPi, Ci, C0) and the set of coefficients (RRi, αi, γi, δi, C0′) were identified specifically from the company databases. These values are used for (i) acute health impact models (log-normal type model) and (ii) chronic health impact assessment models (IER) to estimate short- and long-term health effects in a population. The respective economic values of each type of loss were combined to calculate the corresponding economic valuation (economic valuation). Finally, in step (3), the results are analysed, evaluated, and visualised using maps of the distribution of health effects from short- and long-term PM2.5, as well as zoning maps of health risk effects from PM2.5, between inner-city and suburban areas of the HCMC.

Conceptual model and sequence of steps
Results and discussion
Evaluation of PM2.5 concentrations
The spatial distribution of monthly PM2.5 concentrations (early month: from 1 to 10; mid-month: from 11 to 20; and late-month: from 21 to 28/30/31 depending on the specific month) and variation in 24-h mean PM2.5 pollution distribution (ΔPM2.5 = C – C0) compared to NAAQS (50 µg/m3) and WHO-AQG (15 µg/m3) are shown in Fig. 4 and Fig. S2. Within HCMC, December 2019 had the lowest concentration of 0.077 µg/m3, and September 2019 had the highest concentration of 218.24 µg/m3, more than 4.36 times higher than that of NAAQS (50 µg/m3) and 14. 55 times higher than that of WHO-AQG (15 µg/m3). In each region as follows, in SG1 area, December 2019 had the lowest concentration of 0.88 µg/m3 and with the highest concentration of 190.57 µg/m3 in October 2019, being 3.81 times higher than NAAQS (50 µg/m3) and 12.7 times that of WHO-AQG (15 µg/m3). In SG2 area, December had the lowest concentration with 0.47 µg/m3 and with the highest concentration of 174.43 µg/m3 in December 2019, being 3.49 times higher than NAAQS (50 µg/m3) and 11.63 times higher than WHO- AQG (15 µg/m3). In SG4 area, May 2019 had the lowest concentration with 0.78 µg/m3 and with the highest concentration of 216.7 µg/m3 in September, being 4.33 times higher than NAAQS (50 µg/m3) and 14.45 times higher than WHO-AQG (15 µg/m3). In SG5 area, December 2019 had the lowest concentration with 0.08 µg/m3 and with the highest concentration of 192.6 µg/m3 in October 2019, being 3.85 times higher than NAAQS (50 µg/m3) and 12.84 times higher than WHO-AQG (15 µg/m3).

Changes in monthly 24-h mean PM2.5 concentration (early, mid, and late) compared to the threshold of NAAQS (ΔPM2.5) in HCMC in 2019
The spatial distribution of average PM2.5 concentration in 2019 across the entire HCMC ranges from 0.0077 to 218.24 µg/m3 (as shown in Fig. 5). Specifically in each area as follows, PM2.5 concentration in SG1 area ranged from 0.88 to 190.57 µg/m3 with the maximum concentration occurring at X = 677,122.895 and Y = 1,185,252.996. SG2 area ranges from 0.47 to 174.43 µg/m3 with the maximum concentration occurring at X = 689,169.4797 and Y = 1,203,449.403. SG3 area ranges from 0.17 to 218.24 µg/m3 with the maximum concentration occurring at X = 661,907.2451 and Y = 1,188,175.847. SG4 area ranges from 0.78 to 217.46 µg/m3 with the maximum concentration occurring at X = 701,667.0029 and Y = 1,146,152.322. SG5 area ranges from 0.08 to 202.21 µg/m3 with the maximum concentration occurring at X = 652,608.1011 and Y = 1,215,297.183. Compared with the allowable annual average threshold of PM2.5 according to NAAQS (QCVN 05:2013/BTNMT, annual average 25 µg/m3), all five sub-divisions above exceeded the threshold from 1.001 to 7.62 times in the SG1 area, from 1.12 to 6.98 times in the SG2 area, from 1.09 to 8.73 times in the SG3 area, from 1.09 to 8.7 times in the SG4 area, and from 1.3 to 8.09 times in the SG5 area. The simulation results showed that the pollution level was highest in SG4, followed by SG3, SG1, and SG2. In particular, SG1 has the lowest pollution level among the five areas in HCMC. In each area, the PM2.5 concentration tends to climb gradually from east to west and from northwest to southeast. Figure 5 shows the distribution of mean PM2.5 concentrations in 2019 as a grid with a resolution of ~ 3.0 km × 3.0 km.

Spatial distribution of annual mean PM2.5 concentration in HCMC in 2019
Premature mortality attributable to long-term (chronic) exposure to PM2.5 pollution
For the case of premature deaths due to 4 diseases (IHD, stroke, COPD, and LC), the average was in 2019 across the whole HCMC totalled 3,108.714 (95% CI: 1,024.707; 5,322.132) cases (as shown in Fig. 6). Premature mortality for men was 1,513.944 (95% CI: 499.032–2,591.879) and 1,594.770 (95% CI: 525.674–2,730.254). Meanwhile, considering the age group, the groups of children, adults, and the elderly had an early death of 587.547 (95% CI: 193.670; 1,005.883) cases, 2,347.079 (95% CI: 773.653; 4,018.210) cases, and 174.088 (95% CI: 57.384; 298.039) cases, respectively. Stroke had the highest number of deaths, followed by IHD, COPD, and LC, with the fewest deaths. Summarize the results described above for cases of premature death from IHD (HIIHD, mort), stroke (HIstroke, mort), COPD (HICOPD, mort), and LC (HILC, mort) due to long-term exposure to average PM2.5 concentrations in 2019 across the study area is shown in Fig. 6.

Summary of premature mortality due to IHD, stroke, COPD, and LC attributed to long-term PM2.5 exposure in HCMC in 2019
The study results showed that the number of premature IHD deaths (HIIHD, mort) across the whole HCMC totalled 752.898 (95% CI: 427.8; 1,320.26) cases (as shown in Fig. S3). In terms of sex, the premature mortality was 366.662 (95% CI: 208.338; 634.330) for men and 386.237 (95% CI: 219.461; 668.196) for women. According to age group, children, adults, and the elderly had early deaths of 142.298 (95% CI: 80.854; 246.177), 568.438 (95% CI: 322.989; 983.407), and 42.162 (95% CI: 23.957; 72.941), respectively. Specifically, in each region, the average early deaths in SG1, SG2, SG3, SG4, and SG5 were 579.955, 43.577, 60.654, 36,756, and 31,956, respectively.
For early stroke deaths (HIstroke, mort), throughout HCMC totalled 2,083.026 (95% CI: 549.779–3,288.486) cases (as shown in Fig. S4). By sex, the premature mortality was 1,014.434 (95% CI: 267.742; 1,601.493) cases and 1,068.592 (95% CI: 282.036; 1,686.993) cases for women. Considering age, the groups of children, adults, and the elderly had health risks of 393.692 (95% CI: 103.908; 621.524) cases, 1,572.685 (95% CI: 415.083; 2,482.807) cases, and 116.649 (95% CI: 30.788; 184.155) cases, respectively. In each region as follows, the average early death rate in SG1 was 1,604.618 cases, in SG2 area is 120.189 cases, in SG3 area is 168.226 cases, in SG4 area is 101.776 cases, and in the SG5 area is 88.216 cases.
In the case of premature deaths from COPD (HICOPD, mort), across HCMC, there were 188.226 (95% CI: 32.385; 344.247) cases (as shown in Fig. S5). By sex, the number of early deaths for men was 91.666 (95% CI: 15.820; 167.648) cases, and for women, it was 96.560 (95% CI: 16.665; 176.599) cases. Considering age, the groups of children, adults, and the elderly had health risks of 35.575 (95% CI: 6.140; 65.063) cases, 142.111 (95% CI: 24.526; 259.907) cases, and 10.541 (95% CI: 1.819; 19.278) cases, respectively. In each region as follows, the average early mortality rate in SG1 is 144.998 cases, in SG2 area is 10.822 cases, in SG3 area is 15.250 cases, in SG4 area is 9.206 cases, and in SG5 region, there are 7.951 cases.
For the case of LC premature deaths (HILC, mort), there are a total of 84.563 (95% CI: 14.643; 386.873) cases (as shown in Fig. S6). By sex, the number of early deaths was 41.182 (95% CI: 7.131; 188.407) for men and 43.381 (95% CI: 7.512; 198.466) for women. Considering age, the groups of children, adults, and the elderly had health risks of 15.982 (95% CI: 2.767; 73.119), 63.845 (95% CI: 11.055; 292.089), and 4.736 (95% CI: 0.820; 21.665) cases, respectively. In each region as follows, the average early mortality rate in SG1 is 65.146 cases, in SG2 area is 4.816 cases, in SG3 area is 6.907 cases, in SG4 area is 4.146 cases, and in the SG5 area is 3.548 cases.
For the case of ALRI premature deaths (HIALRI, mort), there are a total of 99.937 (95% CI: 44.965–132.131) cases (as shown in Fig. S7). By sex, the early death rate for men was 91.666 (95% CI: 15.820; 167.648) cases, and for women, it was 96.560 (95% CI: 16.665; 176.599) cases. In each region as follows, the average early death rate in SG1 is 101.784 cases, in SG2 area is 7.626 cases, in SG3 area is 10.668 cases, in SG4 area is 6.455 cases, and in the SG5 area is 5.597 cases. The SG1 region had the highest number of deaths, followed by SG3, SG2, SG4, and SG5, with the lowest number of deaths among the five sub-divisions.
Premature mortality attributable to short-term (acute) exposure to PM2.5 pollution
For the case of premature deaths from RDs from short-term exposure to PM2.5 pollution (HIARD, mort, QCVN) 2019 average across HCMC according to QCVN, there are a total of 6,107.627 (95% CI: 2,109.655; 9,935.407) cases. By gender, the early mortality was 3,450.628 (95% CI: 890.600; 5,960.590) cases and 383.965 (95% CI: 653.302; 6,902.560) cases for women. Considering age, the age groups of children, adults, and the elderly had an early mortality of 1,339.155 (95% CI: 299.000–2,313.248), 4,349.949 (95% CI: 1,739.340–6,886.664), and 418.523 (95% CI: 71.316–753.496) cases, respectively. In each region as follows, the rate of early deaths in the SG1 region was 4,706.114 (95% CI: 1,410.166; 7,655.537) with the maximum premature death occurring at X = 683164.3839 and Y = 1191330.519; in the SG2 area, there were 339.122 (95% CI: 132.511; 551.791) cases with the maximum premature death occurring at X = 689206.7516 and Y = 1197408.37; in the SG3 region, there were 509.222 (95% CI: 196.994; 828.189) cases with the maximum premature death occurring at X = 677104.1165 and Y = 1188272.616; in the SG4 region, there were 301.476 (95% CI: 207.381; 490.385) cases with the maximum premature death occurring at X = 686222.6482 and Y = 1188329.305; and in the SG5 region, there were 251.693 (95% CI: 162.604; 409.505) cases with the maximum premature death occurring at X = 677046.9887 and Y = 1197332.802. Early deaths from RDs due to short-term exposure to PM2.5 pollution according to WHO (HIARD,mort, WHO) totalled 12,204.218 (95% CI: 4,330.308; 19,752.847) cases. By gender, premature deaths were 6,887.044 (95% CI: 5,887.044; 11,819.136) cases and 7,648.385 (95% CI: 1,313.493; 13,665.780) cases. Considering age, the age groups of children, adults, and the elderly had an early death from RDs of 2,672.795 (95% CI: 694.427; 4,586.893), 8,696.511 (95% CI: 3,492.498; 13,674.173), and 834.911 (95% CI: 143.383; 1,491.781), respectively. In each region, the early death rate from RD in SG1 was 9,401.911 (95% CI: 3,333.995; 15,217.226) cases, in SG2, 695.074 (95% CI: 246.567; 1,125.268) cases, in SG3, 996.754 (95% CI: 353.742; 1,612.935) cases, in the SG4 region, 598.411 (95% CI: 212.342; 968.479) cases, and in the SG5 area, 512.068 (95% CI: 181.661; 828.939) cases with the maximum impact at coordinates such as HIARD, mort, QCVN.
The early deaths from CVDs due to short-term exposure to PM2.5 pollution (HIACVD, mort, TCVN) according to QCVN totalled 2,006.210 (95% CI: − 2,528.565; 7,133.484) cases. By sex, there were 1,194.888 (95% CI: − 129.713; 2,606.679) premature deaths in men and 667.152 (95% CI: − 410.159; 1,964.226) cases in women. Based on age, the age groups of children, adults, and the elderly had early deaths from RDs of 354.823 (95% CI: − 504.756; 1,327.404), 1,417.416 (95% CI: − 2,016.353; 5,302.592), and 233.971 (95% CI: − 7.457; 503.488), respectively. In each region, premature mortality from RDs in SG1 was 1,545.847 (95% CI: − 1,948.337; 5,496.568) cases; in SG2, it was 111.360 (95% CI: − 140.331; 396.023); in SG3, it was 167.311 (95% CI: − 210.904; 594.829) cases; in SG4, it was 99.036 (95% CI: − 124.827; 352.127) cases; and in SG5, it was 82.657 (95% CI: − 104.166; 293.937) cases with the maximum impact level at positions such as HIARD, mort, QCVN. Early deaths from CVDs due to short-term exposure to PM2.5 pollution (HIACVD,mort, WHO) according to the WHO totalled 4,034.032 (95% CI: − 5,102.099; 14,298.205) cases. By gender, premature deaths were 2,402.135 (95% CI: − 261.263; 5,230.949) and 1,342.276 (95% CI: − 826.457; 3,945.627) cases. Considering by age, the age groups of children, adults, and the elderly had early deaths from RDs of 713.601 (95% CI: − 1,018.494; 2,660.862), 2,850.630 (95% CI: − 4,068.588; 10,629.368), and 469.801 (95% CI: − 15.018; 1,007.975) cases. In each region, as follows, the early mortality due to RDs in SG1 was 3,107.750 (95% CI: − 3,930.573; 11,015.088) cases, in the SG2 region, 229.683 (95% CI: − 290.447; 814.213) cases, in SG3, 329.557 (95% CI: − 416.872; 1,167.925) cases; in the SG4 region, 197.817 (95% CI: − 250.204; 701.114) cases; and in the SG5 area, 169.225 (95% CI: − 214.004; 599.865) with the maximum impact level at positions such as HIARD, mort, QCVN.
Morbidity cases attributable to short-term exposure to PM2.5 pollution
The study results revealed that for (HIIHD, morb), there were a total of 2,175.979 (95% CI: 1,105.159; 2,757.440) cases (as shown in Fig. 7). By sex, the morbidity of IHD in men was 1,059.702 (95% CI: 538.213; 1,342.873) and in women was 1,116.277 (95% CI: 566.947; 1,414,567) cases. Considering age, the groups of children, adults, and the elderly had IHD rates of 411.260 (95% CI: 208.875; 521.156) cases, 1,642.864 (95% CI: 834.395; 2,081.867) cases, and 121.855 (95% CI: 61.889; 154.417) cases, respectively. In each region, the rate of IHD in the SG1 area was 2,124.024 cases, in SG2 area is 160.072 cases, in SG3 area is 221.553 cases, in the SG4 area is 134.507 cases, and in the SG5 area is 117.285 cases, respectively. Summarize the results described above for cases of IHD (HIIHD, morb), stroke (HIstroke, morb), COPD (HICOPD, morb), and LC (HILC, morb) over the entire HCMC is shown in Fig. 7.

Summary of morbidity cases due to IHD, stroke, COPD, and LC attributed to PM2.5 exposure in HCMC in 2019
The 2019 mean cases (HIstroke, morb) across HCMC totalled 2,412.826 (95% CI: 2,258.405; 4,204.063) cases (as shown in Fig. S8). By sex, the morbidity of stroke in men was 1,175.046 (95% CI: 1,099.843; 2,047.379), and in women, it was 1,237.779 (95% CI: 1,158.562; 2,156.684). Considering age, the groups of children, adults, and the elderly have health risk levels of 456.024 (95% CI: 426.838; 794.568) cases, 1,821.683 (95% CI: 1,705.096; 3,174.067) cases, and 135.118 (95% CI: 126.471; 235.428) cases, respectively. The average number of stroke cases in the SG1 region is 1,858.777 cases; in SG2 area, it is 138.030 cases; in SG3 area, it is 196.295 cases; in SG4 area, it is 118.164 cases; and in SG5 area, it is 101.56 cases.
For the COPD case (HICOPD, morb), there are a total of 38.672 (95% CI: 11.249–23.065) cases (as shown in Fig. S9). By sex, the morbidity of COPD was 18.833 (95% CI: 5.478; 11.233) cases and 19.839 (95% CI: 5.771; 11.833) cases. Considering age, the groups of children, adults, and the elderly had health risks of 7.309 (95% CI: 2.126; 4.359), 29.198 (95% CI: 8.493; 17.414), and 2.166 (95% CI: 0.630; 1.292) cases, respectively. Specifically, in each region, the average morbidity of COPD in SG1 was 29.793 cases, in SG2 was 2.200 cases, in SG3 was 3.162 cases, in SG4 was 1.897 cases, and in SG5 was 1.621 cases.
For the LC case (HILC, morb), there are a total of 4.425 (95% CI: 2.450–77.341) cases (as shown in Fig. S10). By sex, the morbidity of LC was 2.155 (95% CI: 1.193; 37.665) cases and 2.27 (95% CI: 1.257; 39.676) in women. Considering age, the groups of children, adults, and the elderly had health risks of 0.836 (95% CI: 0.463; 14,617) cases, 3.341 (95% CI: 1.850; 58.393) cases, and 0.248 (95% CI: 0.137; 4.331) cases, respectively. In each region as follows, the average morbidity of LC in SG1 is 3.409 cases, in SG2 area is 0.252 cases, in SG3 area is 0.362 cases, in SG4 area is 0.217 cases, and in the SG5 area is 0.185 cases.
Thus, for the cases due to four diseases (IHD, stroke, COPD, and LC), there are a total of 5,213.363 (95% CI: 4,448.083; 5,409.629) cases (as shown in Fig. S11). When considering sex, the morbidity in males was 2,538.908 (95% CI: 2,166.21; 2,634.489) cases, and in females, it was 2,674.455 (95% CI: 2,281.866; 2,775.139) cases. Considering age, the groups of children, adults, and the elderly had morbidity cases of 985.326 (95% CI: 840.688; 1,022.420), 3,936.089 (95% CI: 3,358.302; 4,084.270), and 291.948 (95% CI: 249.093; 302.939) cases, respectively. There, IHD has the most cases of IHD, followed by stroke, COPD, and LC in the fewest cases.
Assessment of economic valuation impacts
Estimation of economic value is lost because of the short- and long-term impacts of PM2.5 exposure in HCMC in 2019 that is calculated on the basis of VSL value and COI cost assumptions according to Chinh Nguyen (2013), Bui et al. (2020), Bui et al. (2021), and Bui and Nguyen (2022). The total economic value of the damage caused by PM2.5 pollution to public health due to long-term exposure is as high as 14,887.48 (95% CI: 4,907.271; 25,487.42) billion VND, equivalent to about 1,995.794 (95% CI: 657.862; 3,416.809) billion USD, accounting for approximately 1.105% of the HCMC GRDP in 2019 (about 1,347,369 billion VND). Specifically, the number of premature deaths from long-term exposure to IHD was 3,605.591 (95% CI: 2,048.713; 6,323.933) billion VND; stroke was 9,975.507 (95% CI: 2,632.864; 15,748.400) billion VND; COPD was 901.405 (95% CI: 155.090; 1,648.582) billion VND; LC was 404.968 (95% CI: 70.125; 1,852.715) billion VND; and ALRI was 478.593 (95% CI: 215.335; 632.769) billion VND. Meanwhile, the total economic value of the damage caused by PM2.5 pollution to public health due to short-term exposure is up to 38,856.760 (95% CI: − 2,006.140; 81,742.070) billion VND, equivalent to approximately 5,209.083 (95% CI: − 268.940; 10,958.230) billion USD, accounting for about 2.884% of the GRDP of HCMC in 2019. Thus, the short-term health impact is relatively more pronounced than the long-term effects of exposure to PM2.5 pollution in HCMC.
PM2.5 exposure and risk zoning
The highest average PM2.5 exposure risk in 2019 (Fig. 8) occurred in the SG1 area, while the lowest risk (5.33) occurred in the SG4 area. Overall, the risk of PM2.5 exposure in the central area was 1.24–2.18 times higher than that in the surrounding area. Among the five sub-division areas, the PM2.5 exposure risk of SG1 was the highest, followed by SG4, SG3, and SG5, and the lowest in SG2. Specifically in each area as follows, the risk of PM2.5 exposure in the SG1 area ranges from 1.274581 to 11.630498 with the maximum risk occurring at X = 683164.3839 and Y = 1191330.519; in the SG2 region ranges from 0.004646 to 6.495985 with the maximum risk occurring at X = 686204.0094 and Y = 1191349.219; in the SG3 region ranges from 0.00001 to 9.402697 with the maximum risk occurring at X = 680143.703 and Y = 1188291.725; in the SG4 region ranges from 0.000049 to 5.336322 with the maximum risk occurring at X = 686222.6482 and Y = 1188329.305; and in the SG5 region ranges from 0.000293 to 9.252161 with the maximum risk occurring at position X = 683126.69 and Y = 1197370.864. In the SG1 region, October has the highest risk of PM2.5 exposure of the year (11.73), while the lowest risk (11.5) occurs in August. In the SG2 region, April has a risk of exposure to the highest PM2.5 of the year (6.58), while the lowest risk (6.37) occurred in June. In the SG3 region, September has the highest risk of PM2.5 exposure in the year (9.68), while when the lowest risk (9.2) occurs in August. In the SG4 region, May 2019 has the highest risk of PM2.5 exposure of the year (5.39), while the lowest risk (5.2) occurs in June 2019. In the SG5 region, April 2019 has the highest risk of PM2.5 exposure in the year (9.38), while the lowest risk (9.25) also occurs in April 2019. Figs. S12—S16 represent PM2.5 exposure risk by age group and by sex group based on the 2019 mean PM2.5 concentration exposure.

Risks associated with PM2.5 exposure in HCMC population in 2019
This study was conducted at the provincial level within a country, although the health impact estimates presented in grid form differ. Several studies comprise results in an administrative unit form, but all have shown a similar interest in the intracity and neighbouring spatial distribution of health effects due to PM2.5. Innovations in the study methodology have resulted in outcomes that may explain the short- and long-term effects of PM2.5 on the health of HCMC residents. A combination of different models, including the precursor emission model, meteorological model (WRF), and air quality model (CMAQ), was used to achieve this goal to explain the spatiotemporal distribution of PM2.5 and health impact models to focus on analysing the relationship between PM2.5 concentrations, populations, and specific types of health damage caused by PM2.5. Simulation development revealed that PM2.5 emissions and precursors and meteorological factors influence the hourly formation of PM2.5 across the entire HCMC area. This aid overcomes the significant limitations of the monitoring station data sources, particularly in situations where guaranteeing spatial coverage over the entire city is not feasible.
HIFs, one of the classical health risk assessment approaches, have been applied and recommended by the US Environmental Protection Agency (US EPA) and have been used throughout China and several other countries worldwide (Lelieveld et al. 2013; Lelieveld et al. 2015; J. Wang et al. 2015; Xue et al. 2019; Guan et al. 2021). HIFs have demonstrated the impact of PM2.5 pollution on the HCMC residents. Specifically, the short-term health effect estimation model evaluates the daily effects of PM2.5, to demonstrate the monthly and seasonal variations in human health risks. Models that estimate long-term health effects have shown cumulative health risks over 1 year.
This study has certain limitations that must be addressed. First, the population data of HCMC used for the calculations are based on a fixed-year basis (2019); thus, this population data source cannot fully support the health impact calculations for a day, month, or season. Second, the mortality reports are incomplete, with significant variation between different districts in HCMC, particularly regarding the number of child deaths (mainly under 5 years old). Data on nonfatal health outcomes are based on surveys of a different quality. Third, shortcomings were observed in determining the cause of death, as these findings were based solely on verbal autopsy interviews. This method is considered an acceptable alternative to the absence of a valid civil status registration system, as is the case in Vietnam (Ngo et al. 2010; Nhung et al. 2013). Finally, comprehensive hospital records are unavailable for ALRI in children and IHD, stroke, COPD, and LC in adults and the elderly. These limitations are a consequence of the largely paper-based patient record system, which lacks patient details, such as age, gender, and cause of death. Furthermore, data on daily hospital admissions for RDs and CVDs were collected from the four largest provincial and central hospitals in HCMC: the Children’s Hospital No. 2, Gia Dinh People’s Hospital, 115 People’s Hospital, and Thong Nhat Hospital.
Conclusions
This study modelled the spatiotemporal changes in PM2.5 concentrations in urban, suburban, and rural areas across HCMC. The annual average concentration of PM2.5 in 2019 ranged from 42.6 to 50.9 μg/m3, and most of them exceeded the allowable thresholds of NAAQS and WHO AQG. The results showed different levels of human health impacts in HCMC due to PM2.5 exposure. Both the short- and long-term public health burdens (mortality and morbidity) were analysed in detail. Additionally, the burdens of the related economic losses were clarified. The typical outcomes were as follows:
-
First, the total number of premature deaths were 3109, which were due to circulatory system diseases (IHD and stroke) and RDs (COPD and LC) resulting from long-term exposure to PM2.5. The highest number of cases was due to strokes, accounting for up to 67% of the total cases. Females and adults had the highest number of deaths, with 1595 and 2347 premature deaths, respectively.
-
Second, the total number of premature mortality cases was 6,08 (caused by RDs and CVDs) due to short-term exposure to PM2.5. This finding shows a trend similar to that of the long-term exposure results. The number of premature deaths in females (63%) and adults (71%) still accounted for most cases. The total number of hospitalisations due to IHD, stroke, COPD, and LC was 5213.
-
Finally, economic losses caused by PM2.5 pollution averaged 53.7 trillion VND (equivalent to 7.2 trillion USD) and contributed to 3.9% of the total GRDP value of HCMC in 2019. The level of economic loss caused by short-term health effects (39 trillion VND) was 2.6 times higher than that caused by long-term impacts (15 trillion VND).
The research framework was selected to evaluate the short- and long-term effects of PM2.5 pollution, focusing on the health endpoints attributed to RDs and CVDs and documenting the specific diseases along with the associated individuals’ age and sex. The outcomes of the study are an important scientific basis for assessing the socio-economic impacts of PM2.5. Calculating the economic loss value is essential for encouraging investment into the implementation of future structural and non-structural measures to control PM2.5, which may benefit local communities and city authorities.
Data availability
We declare that all data relating to this manuscript are truthful, and we will gladly share it with any interested readers or at the request of the editor board.
References
Altieri KE, Keen SL (2019) Public health benefits of reducing exposure to ambient fine particulate matter in South Africa. Sci Total Environ 684:610–620. https://doi.org/10.1016/j.scitotenv.2019.05.355
Andreão WL, Pinto JA, Pedruzzi R, Kumar P, Albuquerque TTA de (2020) Quantifying the impact of particle matter on mortality and hospitalizations in four Brazilian metropolitan areas. J Environ Manage 270. https://doi.org/10.1016/j.jenvman.2020.110840
Anenberg SC, Belova A, Brandt J, Fann N, Greco S, Guttikunda S, Heroux ME, Hurley F, Krzyzanowski M, Medina S, Miller B, Pandey K, Roos J, Van Dingenen R (2016) Survey of ambient air pollution health risk assessment tools. Risk Anal 36(9):1718–1736. https://doi.org/10.1111/risa.12540
Bayat R, Ashrafi K, Shafiepour Motlagh M, Hassanvand MS, Daroudi R, Fink G, Künzli N (2019) Health impact and related cost of ambient air pollution in Tehran. Environ Res 176. https://doi.org/10.1016/j.envres.2019.108547
Boldo E, Linares C, Aragonés N, Lumbreras J, Borge R, de la Paz D, Pérez-Gómez B, Fernández-Navarro P, García-Pérez J, Pollán M, Ramis R, Moreno T, Karanasiou A, López-Abente G (2014) Air quality modeling and mortality impact of fine particles reduction policies in Spain. Environ Res 128:15–26. https://doi.org/10.1016/j.envres.2013.10.009
Borge R, Lumbreras J, Pérez J, de la Paz D, Vedrenne M, de Andrés JM, Rodríguez ME (2014) Emission inventories and modeling requirements for the development of air quality plans. Application to Madrid (Spain). Sci Total Environ 466–467:809–819. https://doi.org/10.1016/j.scitotenv.2013.07.093
Braathen NA, Lindhjem H, Navrud S (2010) Valuing lives saved through environmental, transport and health policies: a meta-analysis of stated preference studies. 33(2008), 1–60. https://www.kent.ac.uk/scarr/events/beijingpapers/BraathenLindhjemNavrudPpr.pdf
Bui LT, Nguyen PH (2022) Evaluation of the annual economic costs associated with PM25-based health damage a case study in Ho Chi Minh City Vietnam. Air Quality, Atmosphere Health. https://doi.org/10.1007/s11869-022-01282-0
Bui LT, Nguyen PH (2023) Ground-level ozone in the Mekong Delta region: precursors, meteorological factors, and regional transport. Environ Sci Pollut Res 30(9):23691–23713. https://doi.org/10.1007/s11356-022-23819-7
Bui LT, Nguyen PH, Nguyen DCM (2020) Model for assessing health damage from air pollution in quarrying area – case study at Tan Uyen quarry, Ho Chi Minh megapolis Vietnam. Heliyon 6(9):e05045. https://doi.org/10.1016/j.heliyon.2020.e05045
Bui LT, Nguyen PH, My Nguyen DC (2021) Linking air quality, health, and economic effect models for use in air pollution epidemiology studies with uncertain factors. Atmos Pollut Res 12(7):101118. https://doi.org/10.1016/j.apr.2021.101118
Burnett RT, Arden PC, Majid E, Casey OSLS, Sumi MHSH, Gitanjali S, Bryan H, Michael B, Ross AHRSKRBJGBN, Haidong K, Francine L, Annette PUCTMMGS., … Aaron C (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspectives, 122(4), 397–403. https://doi.org/10.1289/ehp.1307049
Burnett R, Chen H, Szyszkowicz M, Fann N, Hubbell B, Pope CA, Apte JS, Brauer M, Cohen A, Weichenthal S, Coggins J, Di Q, Brunekreef B, Frostad J, Lim SS, Kan H, Walker KD, Thurston GD, Hayes RB, … Spadaro JV (2018) Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proceed Natl Acad Sci U S Am, 115(38), 9592–9597. https://doi.org/10.1073/pnas.1803222115
Chae Y, Park J (2011) Quantifying costs and benefits of integrated environmental strategies of air quality management and greenhouse gas reduction in the Seoul Metropolitan Area. Energy Policy 39(9):5296–5308. https://doi.org/10.1016/j.enpol.2011.05.034
Chen Li, Shi M, Gao S, Li S, Mao J, Zhang H, Sun Y, Bai Z, Wang Z (2017a) Assessment of population exposure to PM2.5 for mortality in China and its public health benefit based on BenMAP. Environ Pollut 221:311–317. https://doi.org/10.1016/j.envpol.2016.11.080
Chen Li, Shi M, Li S, Bai Z, Wang Z (2017b) Combined use of land use regression and BenMAP for estimating public health benefits of reducing PM2.5 in Tianjin. China Atmos Environ 152:16–23. https://doi.org/10.1016/j.atmosenv.2016.12.023
Chen Z, Cai J, Gao B, Xu B, Dai S, He B, Xie X (2017) Detecting the causality influence of individual meteorological factors on local PM(25) concentration in the Jing-Jin-Ji region. Scientific Reports 7:40735. https://doi.org/10.1038/srep40735
Chen Lei, Zhu J, Liao H, Yang Y, Yue X (2020) Meteorological influences on PM2.5 and O3 trends and associated health burden since China’s clean air actions. Sci Total Environ 744(219):140837. https://doi.org/10.1016/j.scitotenv.2020.140837
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, Balakrishnan K, Brunekreef B, Dandona L, Dandona R, Feigin V, Freedman G, Hubbell B, Jobling A, Kan H, Knibbs L, Liu Y, Martin R, Morawska L, … Forouzanfar MH (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet, 389(10082), 1907–1918. https://doi.org/10.1016/S0140-6736(17)30505-6
Dang TN, Thanh NNN, Vien NT, Dung PHT, An NDT, Dung TTT, Giang DT (2021) Mortality and economic burden of PM25 on cardiovascular disease in Ho Chi Minh City in 2018. Vietnam J Prevent Med 31(6):9–18. https://doi.org/10.51403/0868-2836/2021/369
Dedoussi IC, Eastham SD, Monier E, Barrett SRH (2020) Premature mortality related to United States cross-state air pollution. Nature 578(7794):261–265. https://doi.org/10.1038/s41586-020-1983-8
DeGaetano AT, Doherty OM (2004) Temporal, spatial and meteorological variations in hourly PM2.5 concentration extremes in New York City. Atmos Environ 38(11):1547–1558. https://doi.org/10.1016/j.atmosenv.2003.12.020
Department of Statistics Ho Chi Minh City-a (2019) Part I: Brief introduction of the formation of Key Economic Region of South Vietnam. In General Statistics Office (Vol. 1, Issue 1)
Ding D, Zhu Y, Jang C, Lin CJ, Wang S, Fu J, Gao J, Deng S, Xie J, Qiu X (2016) Evaluation of health benefit using BenMAP-CE with an integrated scheme of model and monitor data during Guangzhou Asian Games. J Environ Sci (china) 42:9–18. https://doi.org/10.1016/j.jes.2015.06.003
Ding D, Xing J, Wang S, Liu K, Hao J (2019) Estimated contributions of emissions controls, meteorological factors, population growth, and changes in baseline mortality to reductions in ambient pm2:5 and pm2:5-related mortality in china, 2013–2017. Environ Health Perspect 127(6):1–12. https://doi.org/10.1289/EHP4157
HCMC DNRE (2018) Current status of air quality in Ho Chi Minh City
Dominici F, McDermott A, Zeger SL, Samet JM (2002) On the use of generalized additive models in time-series studies of air pollution and health. Am J Epidemiol 156(3):193–203. https://doi.org/10.1093/aje/kwf062
Emery C, Jung J, Koo B, Yarwood G (2015) Final report: Improvements to CAMx snow cover treatments and carbon bond chemical mechanism for winter ozone. http://www.camx.com/files/udaq_snowchem_final_6aug15.pdf
Fiore AM, Naik V, Leibensperger EM (2015) Air quality and climate connections. J Air Waste Manag Assoc 65(6):645–685. https://doi.org/10.1080/10962247.2015.1040526
Gao M, Beig G, Song S, Zhang H, Hu J, Ying Q, Liang F, Liu Y, Wang H, Lu X, Zhu T, Carmichael GR, Nielsen CP, McElroy MB (2018) The impact of power generation emissions on ambient PM2.5 pollution and human health in China and India. Environ Int 121:250–259. https://doi.org/10.1016/j.envint.2018.09.015
Glavas SD, Nikolakis P, Ambatzoglou D, Mihalopoulos N (2008) Factors affecting the seasonal variation of mass and ionic composition of PM2.5 at a central Mediterranean coastal site. Atmos Environ 42(21):5365–5373. https://doi.org/10.1016/j.atmosenv.2008.02.055
Granier C, Darras S, Denier Van Der Gon H, Jana D, Elguindi N, Bo G, Michael G, Marc G, Jalkanen JP, & Kuenen J (2019) The Copernicus Atmosphere Monitoring Service global and regional emissions (April 2019 version). Data from ECCAD. April
GSO (2020) Completed results of the 2019 Vietnam population and housing census
Guan Y, Xiao Y, Wang F, Qiu X, Zhang N (2021) Health impacts attributable to ambient PM25 and ozone pollution in major Chinese cities at seasonal-level. J Clean Prod 311(May):127510. https://doi.org/10.1016/j.jclepro.2021.127510
Gubry P, Le HT (2014) People moving in Ho Chi Minh City. In V. T. Hong, P. Gubry, & L. Van Thanh (Eds.), Roads to the city - Migration to Ho Chi Minh City from a Mekong Delta region (1st ed., Issue May, p. 21). Ho Chi Minh City Publishing House
Ha Chi NN, Kim Oanh NT (2021) Photochemical smog modeling of PM25 for assessment of associated health impacts in crowded urban area of Southeast Asia. Environ Technol Innovat 21:101241. https://doi.org/10.1016/j.eti.2020.101241
Hao X, Li J, Wang H, Liao H, Yin Z, Hu J, Wei Y, Dang R (2021) Long-term health impact of PM2.5 under whole-year COVID-19 lockdown in China. Environ Pollut 290(September):118118. https://doi.org/10.1016/j.envpol.2021.118118
HCMC People’s Committee (2019) HCMC’s socio-economic situation report in 2019, tasks, and solutions for 2020
HCMC Statistical Office (2020) Statistical yearbook of Ho Chi Minh City 2019
Hien TT, Chi NDT, Nguyen NT, Vinh LX, Takenaka N, Huy DH (2019) Current status of fine particulate matter (PM2.5) in Vietnam’s most populous city, Ho Chi Minh City. Aerosol Air Qual Res 19(10):2239–2251. https://doi.org/10.4209/aaqr.2018.12.0471
Ho QB, Vu HNK, Nguyen TT, Nguyen TTH, Nguyen TTT (2019) A combination of bottom-up and top-down approaches for calculating of air emission for developing countries: a case of Ho Chi Minh City. Vietnam Air Quality, Atmos Health 12(9):1059–1072. https://doi.org/10.1007/s11869-019-00722-8
Hoffmann S, Batz MB, Morris JG Jr (2012) Annual cost of illness and quality-adjusted life year losses in the United States Due to 14 foodborne pathogens†. J Food Prot 75(7):1292–1302. https://doi.org/10.4315/0362-028X.JFP-11-417
Hu J, Wu L, Zheng B, Zhang Q, He K, Chang Q, Li X, Yang F, Ying Q, Zhang H (2015) Source contributions and regional transport of primary particulate matter in China. Environ Pollut 207:31–42. https://doi.org/10.1016/j.envpol.2015.08.037
Hu M, Wang Y, Wang S, Jiao M, Huang G, Xia B (2021) Spatial-temporal heterogeneity of air pollution and its relationship with meteorological factors in the Pearl River Delta. China. Atmos Environ 254(January):118415. https://doi.org/10.1016/j.atmosenv.2021.118415
Huang D, Xu J, Zhang S (2012a) Valuing the health risks of particulate air pollution in the Pearl River Delta. China Environ Sci Policy 15(1):38–47. https://doi.org/10.1016/j.envsci.2011.09.007
Huang W, Cao J, Tao Y, Dai L, Lu SE, Hou B, Wang Z, Zhu T (2012b) Seasonal variation of chemical species associated with short-term mortality effects of PM 2.5 in Xi’an, a central city in China. Am J Epidemiol 175(6):556–566. https://doi.org/10.1093/aje/kwr342
Huy DH, Chi NDT, Phu NLS, Hien TT (2018) Fine particulate matter (PM2.5) in Ho Chi Minh City: analysis of the status and the temporal variation based on the continuous data from 2013–2017. Sci Technol Develop J: Nat Sci 2(5):130–137
ICD-10 (2016) International statistical classification of diseases and related health problems 10th Revision. http://apps.who.int/classifications/icd10/browse/%0A2016/en
Jiang F, Guo H, Wang TJ, Cheng HR, Wang XM, Simpson IJ, Ding AJ, Saunders SM, Lam SHM, & Blake DR (2010) An ozone episode in the Pearl River Delta: field observation and model simulation. J Geophys Res: Atmos, 115(D22). https://doi.org/10.1029/2009JD013583
Johnson RJ, Rolfe J, Windle J, Benner J (2015) The economics of non-market goods and resources benefit transfer of environmental and resource values. In Benefit Transfer of Environ Res Values. https://doi.org/10.1007/978-94-017-9930-0
Kan H, Chen B (2004) Particulate air pollution in urban areas of Shanghai, China: health-based economic assessment. Sci Total Environ 322(1–3):71–79. https://doi.org/10.1016/j.scitotenv.2003.09.010
Kan H, London SJ, Chen G, Zhang Y, Song G, Zhao N, Jiang L, Chen B (2007) Differentiating the effects of fine and coarse particles on daily mortality in Shanghai. China Environ Int 33(3):376–384. https://doi.org/10.1016/j.envint.2006.12.001
Kan H, London SJ, Chen G, Zhang Y, Song G, Zhao N, Jiang L, Chen B (2008) Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: the Public Health and Air Pollution in Asia (PAPA) study. Environ Health Perspect 116(9):1183–1188. https://doi.org/10.1289/ehp.10851
Kim D, Kim J, Jeong J, Choi M (2019) Estimation of health benefits from air quality improvement using the MODIS AOD dataset in Seoul. Korea Environ Res 173(March):452–461. https://doi.org/10.1016/j.envres.2019.03.042
Kuylenstierna JCI, Heaps CG, Ahmed T, Vallack HW, Hicks WK, Ashmore MR, Malley CS, Wang G, Lefèvre EN, Anenberg SC, Lacey F, Shindell DT, Bhattacharjee U, Henze DK (2020) Development of the Low Emissions Analysis Platform – Integrated Benefits Calculator (LEAP-IBC) tool to assess air quality and climate co-benefits: application for Bangladesh. Environ Int, 145(October). https://doi.org/10.1016/j.envint.2020.106155
Lang J, Zhou Y, Chen D, Xing X, Wei L, Wang X, Zhao N, Zhang Y, Guo X, Han L, Cheng S (2017) Investigating the contribution of shipping emissions to atmospheric PM2.5 using a combined source apportionment approach. Environ Pollut 229:557–566. https://doi.org/10.1016/j.envpol.2017.06.087
Lelieveld J, Barlas C, Giannadaki D, Pozzer A (2013) Model calculated global, regional and megacity premature mortality due to air pollution. Atmos Chem Phys 13(14):7023–7037. https://doi.org/10.5194/acp-13-7023-2013
Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A (2015) The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525(7569):367–371. https://doi.org/10.1038/nature15371
Li J, Zhu Y, Kelly JT, Jang CJ, Wang S, Hanna A, Xing J, Lin C-J, Long S, Yu L (2019) Health benefit assessment of PM2.5 reduction in Pearl River Delta region of China using a model-monitor data fusion approach. J Environ Manage 233:489–498. https://doi.org/10.1016/j.jenvman.2018.12.060
Li J, Yu S, Chen X, Zhang Y, Li M, Li Z, Song Z, Liu W, Li P, Xie M, Xing J (2022) Evaluation of the WRF-CMAQ model performances on air quality in China with the impacts of the observation nudging on meteorology. Aerosol Air Qual Res 22(4):220023. https://doi.org/10.4209/aaqr.220023
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee M, Atkinson C, Bacchus LJ, Bahalim AN, Balakrishnan K, Balmes J, Barker-Collo S, Baxter A, Bell ML, Blore JD., … Ezzati M (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet, 380(9859), 2224–2260. https://doi.org/10.1016/S0140-6736(12)61766-8
Linh VT, Liem ND, Dung HM, Loi NK (2019) Research on application of models for trending evaluation of flood and salinization in climate change context Pilot research in Ho Chi Minh City. Vietnam J Hydrometeorol 2019(EME2):98–110. https://doi.org/10.36335/VNJHM.2019(EME2).98-110
Liu H, Wang X, Zhang J, He K, Wu Y, Xu J (2013) Emission controls and changes in air quality in Guangzhou during the Asian Games. Atmos Environ 76(x):81–93. https://doi.org/10.1016/j.atmosenv.2012.08.004
Liu S, Xing J, Wang S, Ding D, Chen L, Hao J (2020) Revealing the impacts of transboundary pollution on PM25-related deaths in China. Environ Int 134:105323. https://doi.org/10.1016/j.envint.2019.105323
Loc VT, Tuan DA, Greene M, Leon G, Binh NTC, Malesky E, Thach PN, Ha LT, Thu TM, Mosley L, Kwon R (2019) The Vietnam Provincial Competitiveness Index Measuring, PCI 2019 - assess the quality of economic management to promote business development (Profile of 63 Provinces and Cities in Vietnam). www.pcivietnam.vn
Luecken DJ, Yarwood G, Hutzell WT (2019) Multipollutant modeling of ozone, reactive nitrogen and HAPs across the continental US with CMAQ-CB6. Atmos Environ 201:62–72. https://doi.org/10.1016/j.atmosenv.2018.11.060
Maji KJ, Ye WF, Arora M, Shiva Nagendra SM (2018) PM2.5-related health and economic loss assessment for 338 Chinese cities. Environ Int 121(September):392–403. https://doi.org/10.1016/j.envint.2018.09.024
HCMC MPC (2020) Summary of content 51 Programs and Projects on components to implement the Resolution of the 11th Congress of the Party Committee of Ho Chi Minh City, term 2020–2025 on 4 City Development Programs 2020–2025/2030 (p. 83). Central Propaganda and Training Commission, Ho Chi Minh City Municipal Party Committee
Narain U, Sall C (2016) Methodology for valuing the health impacts of air pollution
NCAR. (2020) Weather-research-and-forecasting-model. WRF- The Weather Research and Forecasting Model
NCEP (2000) CISL RDA: NCEP FNL Operational Model Global Tropospheric Analyses, continuing from July 1999. National Centers for Environmental Prediction/National Weather Service/NOAA/U.S. Department of Commerce, 2000t
Ngo AD, Rao C, Hoa NP, Adair T, Chuc NTK (2010) Mortality patterns in Vietnam, 2006: findings from a national verbal autopsy survey. BMC Res Notes 3:0–7. https://doi.org/10.1186/1756-0500-3-78
Chinh Nguyen (2013) Assessment of economic losses due to pollution and environmental degradation. National Political Publishing House
Nhung NTT, Long TK, Linh BN, Vos T, Huong NT, Anh ND (2013) Estimation of Vietnam National Burden of Disease 2008. Asia Pacific J Public Health 26(5):527–535. https://doi.org/10.1177/1010539513510556
OECD (2012) Mortality risk valuation in environment, health and transport policies. https://doi.org/10.1787/9789264130807-en
Pan S, Roy A, Choi Y, Eslami E, Thomas S, Jiang X, Gao HO (2019) Potential impacts of electric vehicles on air quality and health endpoints in the Greater Houston Area in 2040. Atmos Environ 207:38–51. https://doi.org/10.1016/j.atmosenv.2019.03.022
Persson U, Norinder A, Hjalte K, Gralén K (2001) The value of a statistical life in transport: findings from a new contingent valuation study in Sweden. J Risk Uncertain 23(2):121–134. https://doi.org/10.1023/A:1011180018244
Phan CC, Nguyen TQH, Nguyen MK, Park KH, Bae GN, Seung-bok L, Bach QV (2020) Aerosol mass and major composition characterization of ambient air in Ho Chi Minh City. Vietnam Int J Environ Sci Technol 17(6):3189–3198. https://doi.org/10.1007/s13762-020-02640-0
Phung NK, Long NQ, Van Tin N, Le DTT (2020) Development of a pm2.5 forecasting system integrating low-cost sensors for Ho Chi Minh City. Vietnam. Aerosol Air Qual Res 20(6):1454–1468. https://doi.org/10.4209/aaqr.2019.10.0490
Pillai PS, Suresh Babu S, Krishna Moorthy K (2002) A study of PM, PM10 and PM25 concentration at a tropical coastal station. Atmos Res 61(2):149–167. https://doi.org/10.1016/S0169-8095(01)00136-3
Pleim JE, Gilliam R (2009) An indirect data assimilation scheme for deep soil temperature in the Pleim–Xiu land surface model. Journal of Applied Meteorology and Climatology, 48(7), 1362–1376. http://www.jstor.org/stable/26172895
Pleim,JE, Xiu A (2003) Development of a land surface model. Part II: Data Assimilation. J Appl Meteorol, 42(12), 1811–1822. https://doi.org/10.1175/1520-0450(2003)042<1811:DOALSM>2.0.CO;2
Qin M, Yu H, Hu Y, Russell AG, Odman MT, Doty K, Pour-Biazar A, McNider RT, Knipping E (2019) Improving ozone simulations in the Great Lakes Region: the role of emissions, chemistry, and dry deposition. Atmos Environ 202:167–179. https://doi.org/10.1016/j.atmosenv.2019.01.025
Sacks JD, Lloyd JM, Zhu Y, Anderton J, Jang CJ, Hubbell B, Fann N (2018) The Environmental Benefits Mapping and Analysis Program Community Edition BenMAP CE a tool to estimate the health and economic benefits of reducing air pollution. Environ Model Software 104(2):118–129. https://doi.org/10.1016/j.envsoft.2018.02.009
Sacks JD, Fann N, Gumy S, Kim I, Ruggeri G, Mudu P (2020) Quantifying the public health benefits of reducing air pollution: critically assessing the features and capabilities of WHO’s AirQ+ and US EPA’s Environmental Benefits Mapping and Analysis Program Community Edition (BenMAP CE). Atmosphere, 11(5), 1–15. https://doi.org/10.3390/atmos11050516
Shang Y, Sun Z, Cao J, Wang X, Zhong L, Bi X, Li H, Liu W, Zhu T, Huang W (2013) Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ Int 54:100–111. https://doi.org/10.1016/j.envint.2013.01.010
Skamarock WC, Klemp JB, Dudhi J, Gill DO, Barker DM, Duda MG, Huang XY, Wang W, Powers JG (2008) A description of the advanced research WRF Version 3. Tech Rep, June, 113. https://doi.org/10.5065/D6DZ069T
Song C, He J, Wu L, Jin T, Chen X, Li R, Ren P, Zhang L, Mao H (2017) Health burden attributable to ambient PM2.5 in China. Environ Pollut 223:575–586. https://doi.org/10.1016/j.envpol.2017.01.060
Song S-K, Shon Z-H, Kang Y-H, Kim K-H, Han S-B, Kang M, Bang J-H, Oh I (2019) Source apportionment of VOCs and their impact on air quality and health in the megacity of Seoul. Environ Pollut 247:763–774. https://doi.org/10.1016/j.envpol.2019.01.102
Health Effects Institute (2020) State of global air. Data Source: Global Burden of Disease Study 2019. IHME
Sui X, Zhang J, Zhang Q, Sun S, Lei R, Zhang C, Cheng H, Ding L, Ding R, Xiao C, Li X, Cao J (2021) The short-term effect of PM25/O3 on daily mortality from 2013 to 2018 in Hefei. China. Environ Geochem Health 43(1):153–169. https://doi.org/10.1007/s10653-020-00689-x
Tai APK, Mickley LJ, Jacob DJ (2010) Correlations between fine particulate matter (PM25) and meteorological variables in the United States: implications for the sensitivity of PM25 to climate change. Atmos Environ 44(32):3976–3984. https://doi.org/10.1016/j.atmosenv.2010.06.060
Thu NTA, Blume L, Addison E, Franielczyk K (2018) Air quality in Vietnam in 2017. In Air Quality Report - GreenID (Issue 2)
Toledo T, Albuquerque DA, Andrade MDF, Ynoue RY, Moreira DM, Andreão WL, Soares F (2018) WRF-SMOKE-CMAQ modeling system for air quality evaluation in São Paulo megacity with a 2008 experimental campaign data. Environ Sci Pollut Res 25:36555–36569
Tran CC, Ta TD, Duong AT, Phan OTK, Nguyen DA (2020) Analysis on Temporal Pattern of Fine Particulate Matter (PM2.5) in Hanoi, Vietnam and the Impact of Meteorological Conditions. J Environ Protect 11(03):246–256. https://doi.org/10.4236/jep.2020.113014
Tu J, Xia ZG, Wang H, Li W (2007) Temporal variations in surface ozone and its precursors and meteorological effects at an urban site in China. Atmos Res 85(3–4):310–337. https://doi.org/10.1016/j.atmosres.2007.02.003
Vien NT, Thanh NNN, Dung PHT, An NDT, Dung TTT, Giang DT, Dang TN (2021) PM25 increased respiratory mortality in Ho Chi Minh City: a multi-source data study. J Med Res Hanoi Med Univ 142(6):108–118. https://doi.org/10.52852/tcncyh.v142i6.197
Vietnam VCCI (2021) The provincial competitiveness index. The Provincial Competitiveness Index Portal of Vietnam. https://pcivietnam.vn/en
von Schneidemesser E, Monks PS, Allan JD, Bruhwiler L, Forster P, Fowler D, Lauer A, Morgan WT, Paasonen P, Righi M, Sindelarova K, Sutton MA (2015) Chemistry and the linkages between air quality and climate change. Chem Rev 115(10):3856–3897. https://doi.org/10.1021/acs.chemrev.5b00089
Voorhees AS, Wang J, Wang C, Zhao B, Wang S, Kan H (2014) Public health benefits of reducing air pollution in Shanghai: a proof-of-concept methodology with application to BenMAP. Sci Total Environ 485–486:396–405. https://doi.org/10.1016/j.scitotenv.2014.03.113
Vu HNK, Ha QP, Nguyen DH, Nguyen TTT, Nguyen TT, Nguyen TTH, Tran ND, Ho BQ (2020) Poor air quality and its association with mortality in Ho Chi Minh City: case study. Atmosphere 11(7):1–20. https://doi.org/10.3390/atmos11070750
Wang J, Wang S, Voorhees AS, Zhao B, Jang C, Jiang J, Fu JS, Ding D, Zhu Y, Hao J (2015) Assessment of short-term PM2.5-related mortality due to different emission sources in the Yangtze River Delta. China Atmos Environ 123:440–448. https://doi.org/10.1016/j.atmosenv.2015.05.060
Wang N, Lyu XP, Deng XJ, Guo H, Deng T, Li Y, Yin CQ, Li F, Wang SQ (2016) Assessment of regional air quality resulting from emission control in the Pearl River Delta region, southern China. Sci Total Environ 573:1554–1565. https://doi.org/10.1016/j.scitotenv.2016.09.013
Wang Q, Wang J, He MZ, Kinney PL, Li T (2018) A county-level estimate of PM2.5 related chronic mortality risk in China based on multi-model exposure data. Environ Int 110:105–112. https://doi.org/10.1016/j.envint.2017.10.015
Wang F, Qiu X, Cao J, Peng L, Zhang N, Yan Y, Li R (2021) Policy-driven changes in the health risk of PM2.5 and O3 exposure in China during 2013–2018. Sci Total Environ 757:143775. https://doi.org/10.1016/j.scitotenv.2020.143775
Wang X, Li L, Gong K, Mao J, Hu J, Li J, Liu Z, Liao H, Qiu W, Yu Y, Dong H, Guo S, Hu M, Zeng L, Zhang Y (2021) Modelling air quality during the EXPLORE-YRD campaign – Part I. Model performance evaluation and impacts of meteorological inputs and grid resolutions. Atmos Environ 246:118131. https://doi.org/10.1016/j.atmosenv.2020.118131
Wang Y, Wild O, Chen H, Gao M, Wu Q, Qi Y, Chen X, Wang Z (2020) Acute and chronic health impacts of PM2.5 in China and the influence of interannual meteorological variability. Atmos Environ, 229(February). https://doi.org/10.1016/j.atmosenv.2020.117397
WHO (2018) AirQ+: software tool for health risk assessment of air pollution
WHO (2021) WHO global air quality guidelines. Particulate matter (PM2.5 and PM10), Ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. In World Health Organization
Wu W, Yao M, Yang X, Hopke PK, Choi H, Qiao X, Zhao X, Zhang J (2021) Mortality burden attributable to long-term ambient PM25 exposure in China: using novel exposure-response functions with multiple exposure windows. Atmos Environ 246:118098. https://doi.org/10.1016/j.atmosenv.2020.118098
Xie Y (2011) Values and limitations of statistical models. Res Social Strat Mobility 29(3):343–349. https://doi.org/10.1016/j.rssm.2011.04.001
Xing J, Zhang F, Zhou Y, Wang S, Ding D, Jang C, Zhu Y, Hao J (2019) Least-cost control strategy optimization for air quality attainment of Beijing–Tianjin–Hebei region in China. J Environ Manage 245(May):95–104. https://doi.org/10.1016/j.jenvman.2019.05.022
Xue T, Liu J, Zhang Q, Geng G, Zheng Y, Tong D, Liu Z, Guan D, Bo Y, Zhu T, He K, Hao J (2019) Rapid improvement of PM25 pollution and associated health benefits in China during 2013–2017. Sci China Earth Sci 62(12):1847–1856. https://doi.org/10.1007/s11430-018-9348-2
Yarwood G, Jung J, Whitten GZ, Heo G, Mellberg J, Estes M (2010) Updates to the Carbon Bond Mechanism for Version 6 (CB6). Presented at the 9th Annual CMAS Conference, Chapel Hill, NC, October 11–13, 6(415), 1–4
Yin H, Pizzol M, Xu L (2017) External costs of PM2.5 pollution in Beijing, China: uncertainty analysis of multiple health impacts and costs. Environ Pollut 226:356–369. https://doi.org/10.1016/j.envpol.2017.02.029
Zhang L, Zhao N, Zhang W, Wilson JP (2022) Changes in long-term PM2.5 pollution in the urban and suburban areas of China’s three largest urban agglomerations from 2000 to 2020. Remote Sens, 14(7). https://doi.org/10.3390/rs14071716
Zhao B, Wang S, Ding D, Wu W, Chang X, Wang J, Xing J, Jang C, Fu JS, Zhu Y, Zheng M, Gu Y (2019) Nonlinear relationships between air pollutant emissions and PM 2.5 -related health impacts in the Beijing-Tianjin-Hebei region. Sci Total Environ 661:375–385. https://doi.org/10.1016/j.scitotenv.2019.01.169
Zhao C, Pan J, Zhang L (2021) Spatio-temporal patterns of global population exposure risk of pm2.5 from 2000–2016. Sustainability (Switzerland), 13(13). https://doi.org/10.3390/su13137427
Acknowledgements
The authors would like to thank the Ho Chi Minh City University of Technology for the support of time and facilities from the Ho Chi Minh City University of Technology (HCMUT), VNU-HCM for this study.
Funding
This research was funded by the Viet Nam National University Ho Chi Minh City (VNU-HCM), grant No: B2023-20–23.
Author information
Authors and Affiliations
Contributions
Long Ta Bui: Conceptualisation, funding acquisition, investigation, project administration, resources, supervision, methodology, models, writing—original draft, writing—review and editing.
Nhi Hoang Tuyet Nguyen: Data analysis, models, GIS.
Phong Hoang Nguyen: Data curation, data analysis, formal analysis, validation, GIS.
Corresponding author
Ethics declarations
Ethical approval
The authors declare the following:
The manuscript is not submitted to more than one journal for simultaneous consideration.
The manuscript is original and not have been published elsewhere in any form or language (partially or in full), unless the new work concerns an expansion of previous work.
The manuscript is not split up into several parts to increase the quantity of submissions and submitted to various journals or to one journal over time (i.e. “salami-slicing/publishing”).
Results are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. We adhere to discipline-specific rules for acquiring, selecting, and processing data.
We have provided all data and proper mentions of other works.
Consent to participate
I consent to participate to publish my manuscript entitled “Chronic and acute health effects of PM2.5 exposure and the basis of pollution control targets” to the Environmental Science and Pollution Research (ESPR).
Consent to publish
I consent to publish my manuscript entitled “Chronic and acute health effects of PM2.5 exposure and the basis of pollution control targets” to the Environmental Science and Pollution Research (ESPR).
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bui, L.T., Nguyen, N.H.T. & Nguyen, P.H. Chronic and acute health effects of PM2.5 exposure and the basis of pollution control targets. Environ Sci Pollut Res 30, 79937–79959 (2023). https://doi.org/10.1007/s11356-023-27936-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-27936-9