
Abstract
Background and purpose
Although there has been risen investigations and clinical attention to the impacts that physical activity has on the quality of life (QoL) of the elderly, there is a lack of evidence regarding applying aquatic exercise training in this population. This study aimed to determine whether an aquatic training intervention improves QoL among healthy elderly men.
Methods
A total of 40 elderly men aged 66–86 years were recruited from the Department of Education Retirees. Participants were randomly assigned in a 1:1 ratio to a 12-week aquatic training regimen (exercise group) or a non-exercise control group. The exercise group performed three 45-min sessions per week. Data were collected using a Survey short form-36 (SF-36) questionnaire before and after the intervention.
Results
The aquatic training intervention induced significant improvements in physical (84.6% vs − 1.4%; P < 0.001) and mental (57.1% vs − 11.3%; P < 0.001) health component score in comparison with the control condition.
Conclusion
The findings showed that the aquatic training intervention could be an efficient strategy that helps to ameliorate the physical and mental aspects linked to aging and may be an important preventive approach for the future risks in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aging is a process that happens over time and results in unfavorable structural and functional deviations in the body. In this context, because of the fact that physical and cognitive impairments can cause physical dependence and social isolation, they are being considered as two of the most acute variations among the elderly [1]. Nowadays, investigators have defined life expectancy as expecting to live healthy, which does not imply any diseases whatsoever, rather life without functional limitation [2]. In fact, quality of life (QoL) comprises objective and subjective dimensions that interact with one another. On the other hand, it must be noted that QoL is a dynamic concept since individual and social values, needs and attitudes alter with time and reaction to life events and experiences. Moreover, any QoL's dimension can significantly affect other dimensions [3]. Health-related QoL indicates the functional impacts of ill health and its consequences on an individual’s perception of physical, psychological and social aspects of their life [4].
The increasing number of older people on one hand and the onset of diseases and disabilities with age on the other hand have made old age an important issue in most societies. Thus, protection and improvement of health condition and QoL in old age gains importance, so that they can avoid being inflicted with chronic diseases and can improve elderly people’s independence and their participation in familial and social activities [5]. Therefore, paying attention to the QoL, the effect of various psychological considerations, and revision of lifestyle can, to a large extent, increment efficiency and independence of elderly people and assist them in controlling various difficulties of old age and different treatments and can as well be helpful in comprehensive and proper policy-makings for this social group.
Because of the association among QoL and physical activity, morbidity and mortality, measures of it are an essential indicator for assessing health programs in the elderly [6]. Investigations evaluating the relationship between physical exercise and QoL in aged population demonstrated that higher levels of physical activity are linked to a better QoL [6,7,8,9,10]. Recently, a systematic review of reviews and meta-analyses demonstrated that physically active older individuals experience better QoL and improved cognitive functioning [11]. Moreover, other evidence also reveals that older people who engaged in regular exercise training reported an improvement in their QoL [10, 12].
Considering these advantages, performing conventional training and physical activities has some limitations due to psychological and physical issues related to the aging process, especially in those patients who suffer from joint pain and motor disabilities, therefore, regular physical exercise should be conducted with a low health risks. In this regard, an appropriate and alternative method for aged population with the aforesaid difficulties is aquatic training that has a long and noteworthy history for curing diseases, in which water is used as a medium for mental tranquility and alleviation of pain. In addition, buoyancy quality of water not only leads to weight loss and it can provide easy movement in water for those who have difficulty walking on the ground but also the resistance quality of water can create the condition of resistance training, which has psychological benefits as well as physical advantages [13]. Due to other physical properties of water like tenacity and hydrostatic pressure, water can actualize most of the given objectives of rehabilitation programs and allows old individuals to carry out physical training or activities in a painless environment [14]. These reasons have made water exercises and its therapeutic values favored by the elderly and a specific topic for researchers’ studies.
A previous study [15] on aquatic training efficacy in elderly was conducted by Barbosa et al. (2019); however, not only it was a non-randomized controlled trials, but also it included both males and females aged 60 years and older. Therefore, the main objective of this study was to determine the effects of a 12-week aquatic training intervention performed by older health men aged 65 years and older to improve QoL.
Materials and methods
Design
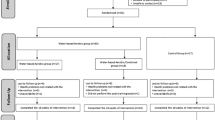
This study was a 12-week randomized controlled trial, conducting from October 1, 2019, to February 30, 2020, at the pars hotel indoor swimming pool (Mashhad, Iran). The study followed the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Sport Sciences Research Institute of Iran (IR.SSRI.REC.1400.016). Informed written consent was retrieved from all participants. The study flow diagram is represented in Fig. 1.

Study flow diagram
Participants and randomization
Forty healthy sedentary elderly men (age: 74.73 ± 5.51 years) who had not performed any type of physical exercise regularly for at least three months were recruited via advertisements. Inclusion criteria were broad: the participants had to be 65 years or older, had to have the ability to walk independently and did not use any walking aids, had to have the ability to perform their activities of daily living, and had to have the ability to understand basic motor commands. The exclusion criteria were also as following: urinary or fecal incontinence, renal insufficiency, open wounds, contagious skin diseases, infectious diseases, catheters, vascular thrombi, cardiac insufficiency, uncontrolled arterial pressure, dyspnea upon minimal effort, use of psychotropic drugs (benzodiazepines) or participation in any other physical activity or physical therapy program.
After the initial evaluation, subjects were randomly allocated to aquatic training (n = 20) and non-exercise control (n = 20) groups following a 1:1 ratio. The assessment staff were blinded to the main study design and group allocation. Subjects were informed and reminded not to discuss their randomization assignment with the assessment staff.
Interventions
The aquatic training program was 45 min, three sessions per week for 12 weeks at the indoor pool (rectangular-shaped, 10 by 12 m) of a day service facility in Mashhad city. The water temperature was 30–32 °C, and ambient temperature of 29 °C. Aquatic training was led by a trained fitness instructor and supervised by researcher. Each session consisted of a 10-min warm-up, 30-min aquatic exercise, and a 5-min cool-down and relaxation exercises. The intensity was low to moderate (11–13 on a rating of perceived exertion (RPE) scale) [16], with constant intensity, frequency and speed, for 12 weeks. Each series was performed continuously and between each one there was a one-min rest. The training program was based on the protocol described elsewhere [17].
In the control group, the subjects were instructed not to undertake any formal exercise or change their physical activity level during the study period.
Measurement
Health-related QoL was evaluated by the Short Form 36-Item Health Survey version 2 (SF-36v2) questionnaire [18,19,20]. The SF-36 is a well-documented questionnaire for evaluation of general health-related QoL. This instrument assesses eight health-related subscales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. Among these, the former four domains contribute to the physical component, and the latter four subscales relate to the mental component. The questionnaire scores have been valued for each scale varies from 0 to 100, and the higher value indicates more positive QoL [21, 22]. The internal consistency of SF-36 is good, with Cronbach’s alpha of 0.76–0.90 for all domains of the questionnaire [23].
Statistical analysis
Data normality was examined using the Shapiro–Wilk test. Changes of variables were determined using a 2 (group: aquatic training and control) × 2 (time: pre-test and post-test) repeated measures analysis of variance. If the main effect (time) was significant, Student’s paired t test was used for the analysis of differences between time points in the same group. All data were analyzed by SPSS software (version 26, IBM, Armonk, NY), and variables are presented as mean ± standard deviation (SD). The significance level was established at P < 0.05.
Results
Of the 43 healthy older men who began the study, three participants (one in the control group and two in the aquatic training group) dropped due to personal issues. At baseline, no significant differences were observed between groups for demographic characteristics (Table 1).
Physical health QoL component score and subscales
Change from pre- to post-intervention for the SF-36 physical health QoL component score and subscales are demonstrated in Fig. 2a and Table 2, respectively. The aquatic training condition group had greater improvements than the control group on the physical health component score and all subscales (P < 0.001 for all subscales).

Effect of aquatic training on SF-36 physical health component score (a) and mental health component score (b). Data are presented as mean ± SD. *Significant difference (P < 0.05) between pre- and post-intervention values. #significant difference (P < 0.05) between aquatic training and control groups (time × group interaction)
Mental health QoL component score and subscales
Change from pre- to post-intervention for the SF-36 mental health QoL component score and subscales are depicted in Fig. 2b and Table 2, respectively. The aquatic training condition group had greater improvements than the control group on the mental health component score and all subscales (P < 0.001 for all subscales).
Discussion
The current study examined the effects of aquatic training on the QoL of healthy older men. Improvements were found in all QoL subscales following a 12-week aquatic training regimen, with 3 times/week. The results show that this intervention period was sufficient to produce significant alterations in both physical and mental component scores of QoL in this population.
The American College of Sports Medicine has endorsed participation in physical exercise is able to decrement the natural negative impacts of aging, inhibiting the development of chronic illnesses, and therefore provide an increment in life expectancy [24]. As far as exercise safety is concerned, in the water buoyancy and viscosity lower the forces apply to body mass-bearing joints, such as the knee, and as a result the aquatic exercise does not damage muscles and joints. In this context, many research has been demonstrated that physical activity conducted in an aquatic environment is associated with a safer situation for the elderly people, because it enhances both physical and social advantages from decreasing the impact of the joints, neuromuscular wear, and increasing the activity in a collective environment, therefore encouraging an interpersonal relationship between participants [25,26,27,28,29].
The improvements in QoL perception in elderly male in our study were comparable to those reported by Bocalini et al., who evaluated the effects of short-term exercise detraining on the functional fitness of older women after a 12-week water-based exercise program. They confirmed that 12 weeks of water exercise improves the functional fitness parameters and QoL of older women. Nevertheless, they stated that the neuromuscular parameters and the QoL score returns to baseline levels after a short detraining period of 4–6 weeks [26]. Moreover, our results are consistent with findings of Barbosa et al. (2019) and Moreira et al. (2020) [15, 30]. Barbosa and colleagues investigated the self-reported QoL in 28 elderly men and women who took part in a 12-week aquatic training program [15]. Their findings demonstrated that none of the aspects that assess the QoL showed improvement following the intervention, except for the aspects related to “past, present and future activities”, “death and dying”, and “social participation”, which revealed a tendency to improve after 12 weeks of an aquatic training program. Moreira and colleagues also examined the impacts of an aquatic training regimen on functional capacity, perceptual aspects, and QoL performed by older adults with musculoskeletal disorders and moderate/high risk of falls. They concluded that the water-based intervention might be applied as a preventive strategy for the older adults with musculoskeletal disorders and at risk of falling to improve physical and usual perceptual aspects (QoL and pain) and fall risk awareness [30].
The positive impact of aquatic exercise on QoL may be linked to the fact that this type of intervention provides an enabling environment for the elderly to exercise at higher intensities than would be possible on land [30]. The overall muscle relaxation produced by water causes a feeling of pleasure and self-efficacy and diminishes the unpleasant sensation induced by aging. Hence, it improves psychological aspects emerging from the physical and mental well-being feeling [31]. Furthermore, the water-based exercises might have also reduced oxidative stress, ameliorated motor unit synchronization and augmented motor neurons excitability and helped to better physical and functional autonomy [32]. Taken together, the combination of these elements may have also affected self-esteem, self-concept, body image, communication and socialization, which are related to overall and specific QoL [31]. In addition, regarding the effect of physical activities performed in water on physical factors, it can be stated that these types of workouts improve cardiovascular functioning, prevent muscle atrophy and decline of muscle strength caused by aging, as well as improve balance and increase flexibility [33].
The current research had some limitations that must be addressed. First, the sample size was relatively small, which limits our power of analysis. Second, only men were investigated, which restricts us from expanding the results to both sexes; possible differences for gender were not controlled and other research comprising men and women are needed to determine if sex may have a role. Finally, additional investigations designed to compare the impacts of water- and land-based training on the QoL aspects of the elderly are needed.
Conclusion
In conclusion, a 12-week aquatic training regimen improved not only physical health QoL component score, but also mental health QoL component score. Physical and mental changes might have also increased safety and self-confidence aspects, which might cause improved social QoL. The present investigation revealed that aquatic training intervention could be an efficient method that helps to ameliorate the physical and mental aspects linked to aging and can be an important preventive approach for the future risks in these populations.
References
Lee EE, Martin AS, Kaufmann CN, Liu J, Kangas J, Daly RE, Tu XM, Depp CA, Jeste DV (2019) Comparison of schizophrenia outpatients in residential care facilities with those living with someone: study of mental and physical health, cognitive functioning, and biomarkers of aging. Psychiatry Res 275:162–168
Annear MJ, Cushman G, Gidlow B (2009) Leisure time physical activity differences among older adults from diverse socioeconomic neighborhoods. Health Place 15(2):482–490
Resnick B, Ory MG, Hora K, Rogers ME, Page P, Bolin JN, Lyle RM, Sipe C, Chodzko-Zajko W, Bazzarre TL (2008) A proposal for a new screening paradigm and tool called exercise assessment and screening for you (EASY). J Aging Phys Act 16(2):215–233. https://doi.org/10.1123/japa.16.2.215
de Siqueira Rodrigues BG, Cader SA, Torres NVOB, de Oliveira EM, Dantas EHM (2010) Pilates method in personal autonomy, static balance and quality of life of elderly females. J Bodyw Mov Ther 14(2):195–202
Schmitz N, Kruse J, Kugler J (2004) The association between physical exercises and health-related quality of life in subjects with mental disorders: results from a cross-sectional survey. Prev Med 39(6):1200–1207
Ramalho JR, Mambrini JV, César CC, de Oliveira CM, Firmo JO, Lima-Costa MF, Peixoto SV (2015) Physical activity and all-cause mortality among older Brazilian adults: 11-year follow-up of the Bambuí Health and Aging Study. Clin Interv Aging 10:751
Puciato D, Borysiuk Z, Rozpara M (2017) Quality of life and physical activity in an older working-age population. Clin Interv Aging 12:1627
Marquez DX, Aguiñaga S, Vásquez PM, Conroy DE, Erickson KI, Hillman C, Stillman CM, Ballard RM, Sheppard BB, Petruzzello SJ (2020) A systematic review of physical activity and quality of life and well-being. Transl Behav Med 10(5):1098–1109
Northey JM, Cherbuin N, Pumpa KL, Smee DJ, Rattray B (2018) Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis. Br J Sports Med 52(3):154–160
Rugbeer N, Ramklass S, Mckune A, Van Heerden J (2017) The effect of group exercise frequency on health related quality of life in institutionalized elderly. Pan Afr Med J 26
Cunningham C, O’Sullivan R, Caserotti P, Tully MA (2020) Consequences of physical inactivity in older adults: a systematic review of reviews and meta-analyses. Scand J Med Sci Sports 30(5):816–827
Pucci GCMF, Neves EB, Santana FSd, Neves DdA, Saavedra FJF (2021) Effect of resistance training and pilates on the quality of life of elderly women: a randomized clinical trial. Revista Brasileira de Geriatria e Gerontologia 23
Lord S, Mitchell D, Williams P (1993) Effect of water exercise on balance and related factors in older people. Aust J Physiother 39(3):217–222
De Leo D, Diekstra RF, Lonnqvist J, Lonnqvist J, Cleiren MH, Frisoni GB, Buono MD, Haltunen A, Zucchetto M, Rozzini R (1998) LEIPAD, an internationally applicable instrument to assess quality of life in the elderly. Behav Med 24(1):17–27
Barbosa BT, Silva RLSd, Meneses ABCd, Brindeiro-Neto W, Bacurau TP, Rocha AISdS, Souza LISd, Brasileiro-Santos MdS (2019) Self-related quality of life of elderly submitted to a 12-week aquatic training program. J Hum Sport Exer 14(2):281–291
Borg G (1970) Perceived exertion as an indicator of somatic stress. Scand J Rehabilit Med
Alikhajeh Y, Barabadi E, Mohammad Rahimi GR (2020) A comparison of 6 weeks of aquatic exercise and kinesio taping in patients with chronic nonspecific low back pain. J Sport Rehabil 30(1):37–42
Ware Jr JE, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Medical Care:473–483
Angst F, Verra ML, Lehmann S, Aeschlimann A (2008) Responsiveness of five condition-specific and generic outcome assessment instruments for chronic pain. BMC Med Res Methodol 8(1):1–8
Campolina AG, Ciconelli RM (2008) SF-36 and the development of new assessment tools for quality of life. Acta Reumatologica Portuguesa 33(2):127–133
Ware JE Jr (2000) SF-36 health survey update. Spine 25(24):3130–3139
Contopoulos-Ioannidis DG, Karvouni A, Kouri I, Ioannidis JP (2009) Reporting and interpretation of SF-36 outcomes in randomised trials: systematic review. BMJ 338
Sato D, Kaneda K, Wakabayashi H, Nomura T (2007) The water exercise improves health-related quality of life of frail elderly people at day service facility. Qual Life Res 16(10):1577–1585
Chodzko-Zajko WJ, Proctor DN, Singh MAF, Minson CT, Nigg CR, Salem GJ, Skinner JS (2009) Exercise and physical activity for older adults. Med Sci Sports Exerc 41(7):1510–1530
Barker AL, Talevski J, Morello RT, Nolan GA, De Silva RD, Briggs AM (2016) Jumping into the deep-end: results from a pilot impact evaluation of a community-based aquatic exercise program. Clin Rheumatol 35(6):1593–1601
Bocalini DS, Serra AJ, Rica RL, Santos Ld (2010) Repercussions of training and detraining by water-based exercise on functional fitness and quality of life: a short-term follow-up in healthy older women. Clinics 65:1305–1309
Devereux K, Robertson D, Briffa NK (2005) Effects of a water-based program on women 65 years and over: a randomised controlled trial. Aust J Physiother 51(2):102–108
Oh S, Lim J-M, Kim Y, Kim M, Song W, Yoon B (2015) Comparison of the effects of water-and land-based exercises on the physical function and quality of life in community-dwelling elderly people with history of falling: a single-blind, randomized controlled trial. Arch Gerontol Geriatr 60(2):288–293
Sato D, Kaneda K, Wakabayashi H, Nomura T (2009) Comparison two-year effects of once-weekly and twice-weekly water exercise on health-related quality of life of community-dwelling frail elderly people at a day-service facility. Disabil Rehabil 31(2):84–93
Moreira NB, da Silva LP, Rodacki ALF (2020) Aquatic exercise improves functional capacity, perceptual aspects, and quality of life in older adults with musculoskeletal disorders and risk of falling: a randomized controlled trial. Exp Gerontol 142:111135
Dundar U, Solak O, Yigit I, Evcik D, Kavuncu V (2009) Clinical effectiveness of aquatic exercise to treat chronic low back pain: a randomized controlled trial. Spine 34(14):1436–1440
Silva LAd, Tortelli L, Motta J, Menguer L, Mariano S, Tasca G, Silveira GdB, Pinho RA, Silveira PCL (2019) Effects of aquatic exercise on mental health, functional autonomy and oxidative stress in depressed elderly individuals: a randomized clinical trial. Clinics 74
Colado J (2003) Effects of an experimental strength training in the aquatic way on the increase of the transverse section of the muscle and the dynamical strength [dissertation]. University of Valencia, Valencia
Acknowledgements
The authors thank all the subjects for their contributions in the study.
Funding
This research has no fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors have no conflict of interest.
Ethical approval
The study followed the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Sport Sciences Research Institute of Iran (IR.SSRI.REC.1400.016). Informed consent Informed written consent was retrieved from all participants.
Informed consent
Informed written consent was retrieved from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Alikhajeh, Y., Afroundeh, R., Mohammad Rahimi, G. et al. The effects of a 12-week aquatic training intervention on the quality of life of healthy elderly men: a randomized controlled trial. Sport Sci Health 19, 665–670 (2023). https://doi.org/10.1007/s11332-022-00938-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-00938-9