
Abstract
Objectives
The reasons why the maxillary posterior region is challenging for dentists are its structure and anatomical variations. For this reason, it is necessary to have complete knowledge about the anatomy of this region. In dentistry, necessary information for the desired evaluation in this region can be provided by CBCT. The fact that it provides a three-dimensional evaluation and has measurement reliability emphasizes its importance in surgical applications. The septa, haller cell, and accessory ostium are variations of the maxillary sinus. There are few studies in the literature examining the relationship between maxillary sinus diameters and its variations. The aims of this study are to determine the prevalence of maxillary sinus variations and the average of maxillary sinus diameters, to examine their relationships according to age and gender, and to evaluate the effects of maxillary sinus diameters on variations.
Methods
In this retrospective study, CBCT images of 212 patients were examined. The examined CBCT images were analysed and recorded in more than one section. Descriptive statistics, chi-square tests, independent t test, one-way Anova tests were used to evaluate the data.
Results
As a result, a statistically significant difference was observed between the variations, gender and age groups in terms of morphometric characteristics of the maxillary sinus. The most common variation was observed to be accessory ostium.
Conclusions
The rate of patients with at least one anatomical variation was 77.8%. For this reason, a detailed analysis should be performed to avoid complications before surgical procedures are performed in the area.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The maxillary sinuses, the largest of the paranasal sinuses, are a pair of bony chambers located within each maxillary bone. Knowledge of maxillary sinus anatomy is important in forensic medicine and various dental and maxillofacial procedures [1].
In today's dentistry, dental implant applications are increasing day by day. The inadequacy of the posterior maxilla crest height, pathologies and variations in the maxillary sinus have been challenging factors for dentists, especially in elderly patients [2]. The maxillary sinus is a critical anatomical structure for dental implant procedures in the maxilla. Depression of the sinus floor is a common finding that prevents dental implant placement. In such cases, a sinus elevation procedure may be required [3, 4]. Having knowledge about the anatomy of the region before such a surgical operation will reduce the risk of possible complications [5, 6].
While some of the anatomical variations of the paranasal sinuses are known to increase susceptibility to infection, others cause surgical complications. Maxillary sinus septa are one of the variations of the maxillary sinus and originate from the lower and lateral walls of the sinus. The maxillary sinus septa jeopardizes the integrity of the membrane while the sinus floor is being lifted [2, 6,7,8,9,10,11,12]. It has been reported that maxillary sinus variations such as accessory maxillary ostium (AMO) and Haller cell (HC) may cause sinusitis [2, 13, 14].
Implant planning is often complicated due to alveolar ridge atrophy in the posterior maxilla. With the resorption of the crest after tooth loss, the vertical dimension of the crest decreases and maxillary sinus floor elevation is required. The presence of septa in the maxillary sinus affects the sinus elevation processes, as it increases the adhesion force of the Schneiderian membrane [15, 16]. While spiculer process larger than 2.5 mm in the maxillary sinus is considered as septa [17], spiculer process of 2–4 mm is considered as septa in the British literature [18].
The maxillary sinus septa divide the maxillary sinus into two or more parts [19]. Maxillary sinus septa are divided into two according to their development: primary septa caused by congenital differences and secondary septa formed by irregular pneumatisation of the maxillary sinus after tooth loss at the base of the maxillary sinus [8, 16, 20]. Sinus septa can occur anywhere in the maxillary sinus walls. Depending on their localization, they are divided into three as anterior, medial and posterior regions. They have been described as follows: anterior region is anterior to the mesial aspect of the first molar; medial region is between the mesial aspect of the first molar and the mesial aspect of the third molar; posterior region is the area distal to the mesial aspect of the third molar tooth. [8, 16, 18].
When the sinus septa are considered as orientation, it is evaluated in three groups as coronal, sagittal and axial, and each group is divided into three in terms of morphology, as an incomplete, completed and completed septa that has formed a separate chamber [17, 21]. Figure 1 shows the septa orientations of the maxillary sinus in three planes (Fig. 1).

Schematic drawing of septa orientation types
The maxillary sinus opens into the posterior part of the infundibulum through its ostium and drains its mucus into the middle meatus on the lateral wall of the nose. Sometimes there is an AMO that opens into the anterior and posterior parts of the inferior turbinate. AMO is considered any extra opening other than the natural ostium of the maxillary sinus. It is usually found in the nasal fontanelle or hiatus semilunaris area [22, 23]. Most authors state that the mucus circulation between the accessory and natural ostium disrupts the drainage of the maxillary sinus, leading to sinusitis [24, 25].
An AMO arises from a membranous region in the medial maxillary wall, located between the uncinate process and the inferior turbinate covered only by the mucoperiosteum. This area is known as the “fontanelle” and has been reported to be potentially perforated by the pressure of pus and edema derived from the recurrence of sinusitis [26].
Accessory maxillary ostium opens to the nasal wall 5 to 10 mm above and laterally from the connection point of the inferior turbinate. AMO is a predisposing factor for chronic maxillary sinusitis. Before the sinus floor lift procedure, surgeons should define the presence and position of the AMO and pay attention to these areas during the operation [27].
Haller cells were first described by Albrecht von Haller. In literature, HC are called infraorbital ethmoid cells or orbito-maxillary cells [29, 30]. Often originated from anterior ethmoid cells, they are defined as ethmoid air cells that extend along the medial part of the orbital floor, near the maxillary ostium [28, 30]. They are formed by the development of anterior ethmoid cells along the roof of the maxillary sinus and the lamina orbita of the ethmoid bone [14, 23, 30,31,32]. HC, located proximal to the maxillary sinus infundibulum, may cause obstruction of this drainage pathway and sinusitis [2, 14, 28]. This may be manifested by the size of the HCs, the degree of proximity to the infundibulum, or its infection [23, 28, 29, 31]. HCs are thought to be associated with pathologies such as orofacial pain, sinusitis, nasal obstruction, headache, cough, and mucocele [30].
Haller cells are one of the most frequently observed anatomical variations in the osteomeatal complex [33]. Since HC remain lateral to the infindibulum, they are not seen in nasal endoscopy. However, a bulge on the lateral wall below the level of the ethmoidal bulla and narrowness in the infindibulum may suggest the presence of HC [34].
Haller cells have been evaluated with different radiographic techniques such as panoramic radiography, CT, multi-sectional computed tomography, CBCT in the literature. CBCT is an imaging technique that enables the evaluation of paranasal anatomy with a low radiation dose and is suitable for imaging specific to hard tissues [29].
The pneumatization of the maxillary sinus is a physiological process. Its occurrence has been linked to factors such as heredity, bone density, previous sinus surgery, air pressure within the sinus, and extraction of posterior teeth. Pneumatization is remarkable in patients with the extraction of second molars and extraction of two or more adjacent teeth in the posterior maxilla. [35]. In posterior maxilla, a phenomenon, which is a combination of alveolar crest resorption and maxillary sinus pneumatization, is seen after tooth extraction [36]. While maxillary sinus pneumatization causes 30% of alveolar height loss, socket remodeling causes 70% [37].
Direct radiographs (Water’s, Cadwell, lateral, basal, oblique and submentovertex), CT, magnetic resonance imaging (MRI), ultrasound and CBCT can be used for the radiological diagnosis of the paranasal sinuses [38].
The development of two-dimensional panoramic imaging techniques began in the first half of the twentieth century. Since then, this radiographic technique has continuously improved and become the standard for clinicians in daily practice. In parallel with this, in 1982 CBCT was introduced as a tool for dental and maxillofacial diagnoses. Current literature shows that panoramic and intraoral radiographs are the most practical imaging techniques in dentistry [39].
With the introduction of CBCT, a relatively low-dose and high-resolution alternative has been provided for imaging the maxillofacial region. With its low cost, low radiation dose and high spatial resolution, CBCT has become the method of choice for evaluating potential implant sites, especially in complex situations that require three-dimensional views of the area of interest [40,41,42,43]. CT and CBCT are considered the gold standard for imaging the sinuses [43]. As well as some advantages over two-dimensional images such as real-size image rendering, CBCT also has advantages over CT such as vertical scanning of the patient in the natural sitting position, isotropic voxel size and less metal artifact. It provides high resolution and accurate size images in a short time. It has lower radiation dose, lower cost and energy efficiency compared to CT. It can be used not only for preoperative evaluations but also for intraoperative evaluations [44]. Because CBCT has isotropic voxels, more accurate and sensitive measurements can be made. Motion artifacts are reduced with fast scanning time. Thanks to artifact-reducing software that works in conjunction with CBCT programs, metal artifacts have decreased significantly and it has become possible to create higher-quality images [45].
The aims of this study are to determine the prevalence of maxillary sinus variations and the average of maxillary sinus diameters, to examine their relationships according to age and gender, and to evaluate the effects of maxillary sinus diameters on variations.
Materials and methods
Ethics committee approval for the study was obtained from the meeting of Selcuk University Faculty of Dentistry, Non-Interventional Clinical Research Evaluation Commission, dated 09.05.2019 and numbered 2019/03. CBCT images in the image archive of Selcuk University Faculty of Dentistry, Department of Oral, Dental and Maxillofacial Radiology were used. CBCT images taken between 01.12.2017 and 19.06.2019 for dental implant planning, determination of impacted tooth position and evaluation of pathological lesions, trauma and cephalometric analysis in orthodontics were included in the study.
Inclusion criteria: CBCT images of patients over 18 years of age, images with all margins of the maxillary sinus present, and images where resolution permits viewing the region. Exclusion criteria: images in which the entire area to be examined did not enter the image, images of patients who had developmental or neoplastic lesions that would affect the maxillary sinus dimensions and boundaries, trauma and low-quality images. The study included a total of 212 patients (120 male and 92 female) between the ages of 18–90 (mean 50.2 ± 15.6 years), and evaluated 424 maxillary sinus images. Before examining the relationship of variations of the maxillary sinus with age, the ages of the patients were divided into groups (… < 35, 35 ≤ … < 50, 50 ≤ … < 65, 65 ≤ …). Patients who lost all their premolar and molar teeth were classified as the posterior edentulous group. Since the number of patients with all posterior teeth was scarce in our sample group, patients who lost only one of their premolar or molar teeth were classified as the dentate group. Of the 424 quadrants, 200 were edentulous, while 224 were dentate.
All cone-beam computed tomography data used in the study were obtained using CBCT (Instrumentarium Dental, Palo DEx Group Oy Nahkelantie 160 FI-04300 TUUSULA, Finland) at the Oral, Dental and Maxillofacial Radiology clinic using 89 kvp, 4–12 mA values. The measurements were made by the same observer on a BenQ GL2460 (24 inch, 1920X1080 resolution) model screen, repeated three weeks apart. The parameters examined using 0.5 mm section thickness were vertical, sagittal and horizontal diameters of the maxillary sinus, maxillary sinus septa, AMO and HC.
A technique used by Akhlaghi et al. were applied for maxillary sinus diameters (Fig. 2) [46, 47].

Measurement of the vertical (VD). Horizontal (HD) and sagittal diameters (SD) of the maxillary sinus
Maxillary sinus diameters and measurements
Maximum horizontal (transversal) diameter, also called the width of the maxillary sinus, is measured by the distance between tangents passing through the deepest points of the lateral and medial walls of the maxillary sinus.
Maximum vertical (cranio-caudal) diameter, also called the height of the maxillary sinus, is measured by the distance between the tangent lines passing through the deepest point of the inferior wall and the highest point of the superior wall of the maxillary sinus.
Maximum sagittal (antero-posterior) diameter, also called the length of the maxillary sinus, is measured by the distance between the tangents passing through the deepest points of the anterior and posterior walls of the maxillary sinus [47,48,49].
The vertical diameter of the maxillary sinus was greatest in the region of the first molar. The horizontal, vertical and sagittal diameters of the maxillary sinus in adults were around 25–35, 36–45, and 38–45 mm, respectively [37, 50].
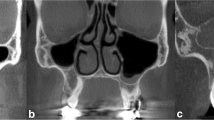
While examples of HC and AMO encountered in the study are shown in (Fig. 3), examples of septa and septa orientations are shown in (Fig. 4).

Hall cells (H). Accessory ostium (white arrows). uncinate process (U). Inferior concha (IC). Medial concha (MK) seen in coronal planes

Septa types and orientations. A, B, C axial septa images in axial. Coronal and sagittal planes. D, E, F coronal septa images in axial. Coronal and sagittal planes. G, H, I sagittal septa images in axial. Coronal and sagittal planes, respectively
In our study, the position, number, orientation and morphology type of septa were noted and statistical analysis was performed. It is necessary to examine CBCT images in at least two planes to determine the orientation of the septa and the type of orientation. Coronal and sagittal planes were examined for axial septa, axial and sagittal planes were examined for coronal septa, and axial and coronal planes were examined for sagittal septa.
The data obtained from the images were saved in the Microsoft Excel program. Statistical analysis was performed with IBM SPSS version 26 (Mac Os). Maximum, minimum, mean and standard deviation values of continuous data and frequency and percentage values of categorical data were obtained by descriptive statistics. The relationship of maxillary sinus diameters with gender and variations was analysed by independent t test, and the relationship with age groups was analysed by a one-way ANOVA test. The relationship between maxillary sinus variations and dental status was analysed by the chi-square test. p < 0.05 was considered statistically significant.
Results
Our study was performed using CBCT images of 424 maxillary sinuses in 212 patients. While 165 (77.8%) variations were observed in 212 patients, the most common variation was the AMO (122 patients, 57,5%) and the least observed variation was the HC (51 patients, 24.1%). In our study, the septa were seen in 89 (42%) patients and in 128 maxillary sinuses (30.2%) (Table 1).
The frequency distributions for the axial, coronal and sagittal septa orientations and their 3 types (incomplete/completed/completed and formed a separate chamber) were as in (Table 2). The most common septa orientation was coronal type (132 maxillary sinuses, 88%). The most common morphology type (valid for all septa orientation types) was the completed septa type. In our study, complete septa type that was completed and formed a separate chamber in sagittal and axial plane were not observed (Table 2).
In our study, the septa position was most frequently observed in the middle part while least commonly observed in the posterior region (Table 2).
The minimum, maximum and mean values of the maxillary sinus diameters are shown in (Table 3). The mean vertical, horizontal and sagittal diameters of the maxillary sinus are 36.36, 23.30 and 37.12 mm, respectively (Table 3).
Table 4 shows the relationships between the vertical, horizontal and sagittal diameters of the maxillary sinus and the AMO, septa, HC, gender and dental status. There is a statistically significant difference between the diameters of the maxillary sinus in three dimensions and gender (p < 0.05). Accordingly, the maxillary sinus diameters of men are larger than the sinus diameters of women. In the statistical tests, a statistically significant result was found between the diameters of the maxillary sinus and the septa, AMO and HC (p < 0.05). Maxillary sinus diameters are larger in the presence of AMO, HC and septa, but smaller in the absence of them. A statistical relationship was found only between the sagittal diameter of the maxillary sinus and the posterior dental status. It was observed that the mean maxillary sinus sagittal diameters of patients with posterior teeth were larger than those of posterior edentulous patients (Table 4).
Anova test was applied to examine the relationship between maxillary sinus diameters and age groups. After the result was found statistically significant, post-hoc analyses were performed. Accordingly, no statistical significance was found between the vertical diameter of the maxillary sinus and the age groups. Statistically significant difference was found between the horizontal and sagittal diameters and age groups. It was observed that the mean horizontal diameter of the 18–35 age group was greater than the mean horizontal diameter of the 50–65 age group. No statistical difference was found between other age groups in this diameter. It was observed that the mean sagittal diameter of the 65 + age group was larger than that of the 50–65 age group, and there was no statistical difference in this dimension between the other age groups (Table5).
As seen in Table 6, which shows the relationship between maxillary sinus variations and age group and gender, no statistical relationship was observed between the variations and gender and age groups (Table 6). Table 7 shows the relationship between maxillary sinus variations and dental status. Among the parameters shown in Table 7, septa and HC seem to be associated with dental status.
Discussion
The maxillary sinus is an important anatomical structure for maxillofacial surgery. Examination of this area before the surgical procedure gives the surgeon valuable information to prevent complications that may occur during the operation [28]. The success of sinus floor elevation operation is a procedure dependent on fragile anatomical structures and variations [10]. Even though sinus floor elevation procedure has complications such as perforation of the Schneiderian membrane, it has become a very reliable technique. The presence of maxillary sinus septa can cause accidental perforation of the Schneiderian membrane during the procedure and then the development of acute or chronic sinusitis and eventually graft resorption. In addition, the septa can be an obstacle to the elevation of the bone plate and sinus membrane during surgery. It is thought that maxillary sinus variations may predispose to infection. Hall cells can narrow the drainage pathway in the osteomeatal complex. AMO may disturb the mucociliary clearance of the maxillary sinus. The person who has HC or AMO is vulnerable to inflammatory sinus diseases [14, 27].
CT and panoramic radiographs are the most commonly used radiological methods for dental implants. It has been shown that CT is a more reliable radiological method than panoramic radiographs in previous studies. With the recent introduction of CBCT, the use of CBCT in maxillofacial imaging has increased. CBCT has become more popular in maxillofacial imaging because the radiation dose is less, it is cheaper and it produces less metal artifact than CT [6]. Paranasal sinus variations and anatomy should be well known for minimally invasive surgical techniques. Anatomical variations should be well known and visualized before the operation to avoid complications that may occur during surgical procedures and to perform the operation safely. Compared with two-dimensional imaging techniques, CT has been reported to be a more reliable technique for mucosal changes in the sinuses. CT and CBCT are generally accepted as the gold standard for radiographic imaging of the sinuses [40, 43]. For these reasons, CBCT images were used in our study.
Sinus membrane perforation is the most common complication in surgical procedures of patients with sinus septa. Since surgical applications involving the maxillary sinus segment have become more frequent, radiological evaluations that determine the size and localization of the septa have gained importance [8]. In this study, the septa were evaluated retrospectively with CBCT images. The prevalence of septa in this study was 42%. A wide range of septa prevalence such as 6.4–66.5% has been reported in the literature [5, 7,8,9,10,11,12, 14,15,16,17,18, 20, 23, 27, 50]. It has been reported that the incidence of septa varies in studies conducted in different societies. The frequency of septa observed in our study is consistent with the literature. The wide range of its incidence is explained by racial factors [19].
Sinus septa is an anatomical variation of the sinus cavity for which surgical intervention is usually not required. In recent years, data on the clinical importance of the orientation and location of the septa have drawn attention in the literature. With these data, it is thought that the sinus floor elevation procedure may reduce complications due to increased use [51]. In our study, the septa orientation type was most common in the coronal direction. In studies on the characteristics of the septa in the literature, the sinus septa were mostly observed in the coronal plane, in line with our study [10, 11, 16, 17, 21, 27]. Although they used a different classification when Kocak et al. and Lozano-Carrascal et al. classified the septa orientation, they reached a similar conclusion to us [10, 21]. The sinus septa can extend along the wall where it is formed, or it can form in incomplete, and it can also extend to all walls in three dimensions. In our study, the most common type was the completed type of septa and it was mostly seen in the middle part of the sinus floor. This result was also observed to be compatible with the literature [11, 17, 21].
While Zinreich and Kennedy defined the HC as the air cell located lateral to the infindibulum, adhering to the roof of the maxillary sinus and inferior to the ethmoid bulla, Bolger et al. defined it as the air cells located in the lower part of the lamina papyracea, including the air cell in the ethmoid infundibulum, under the ethmoid bulla and in the roof of the maxillary sinus [32]. In this study conducted with CBCT, the prevalence of HC was found to be 24.1%. Literature review showed that the prevalence of HC is between 8 and 39% [13, 14, 23, 28, 30, 31, 33, 34, 52]. It was observed that the result of this study was consistent with the range in the literature. However, when these studies were examined, it was noticed that there were differences even in the same race, which is thought to be due to regional and ethnic factors, as well as differences in the interpretation of HCs.
It is recommended to elevate the membrane towards the medial wall of the sinus, during sinus floor elevation. There are several reasons for this. The first is the blood supply provided by the posterior lateral nasal artery on the medial wall. The second is the fact that the membrane on the medial wall reduces the tension of the elevated membrane. However, although it is recommended to elevate the membrane towards the medial wall, attention should be paid to the AMO on the medial wall [27]. In our study, the prevalence of AMO was found 57,5%. In studies conducted in the literature, a prevalence was found in the range of 1.9–45.5%. The study conducted by Young et al. found the closest result to this study with a prevalence of 45.5% [13, 14, 24,25,26,27]. In the information gathered from the literature, nasal septum deviation is among the factors affecting the formation of the AMO. This study was conducted without considering nasal septum deviation. In the literature, it has been thought that there may be other variables that may affect the formation of the AMO, such as infections, minor nasal traumas in childhood and genetic factors [24]. Not examining these factors is one of the limitations of this study. Therefore, we suggest that these factors should also be examined in future studies about AMO.
In this study, the relationship between maxillary sinus variations and dental status was examined. While there is a statistically significant relationship between dental status with septa and HC, there is no statistically significant relationship with AMO. Dedeoglu and Altun found a higher frequency of AMO in posterior edentulous patients. It is thought that the reason for this difference may be due to other factors such as inflammatory pathologies of the maxillary sinus. Although there is no statistically significant relationship in some of the studies examining the relationship between septa and posterior dental status in the literature [2, 49], there are also studies that found statistically significantly higher frequency of septa in edentulous patients [16]. In this study, septa and HC were found with a higher frequency in patients with posterior teeth. It is thought that the reason for these differences may be due to methodological differences in the studies and genetic factors. It is thought that the methodological difference can be eliminated by increasing the number of patients. Dedeoglu and Altun did not find a statistically significant relationship between HC and posterior dental status. In this study, the frequency of HC in posterior edentulous patients was statistically higher in posterior edentulous patients. It is thought that genetic factors may play a role in this difference.
The vertical, horizontal and sagittal lengths of the maxillary sinus were measured and the relationship between them and the maxillary sinus variations was examined. Accordingly, a statistically significant relationship was found between these lengths and septa, HC and AMO. The mean maxillary sinus diameters of images with maxillary sinus variation were statistically significantly larger in all three planes. In this study, the relationship between maxillary sinus diameters and posterior dental status is also examined. There was only one statistically significant result and that was between sagittal diameter and posterior dental status. According to this result, sagittal diameter decreases statistically significantly after tooth extraction. To provide more support for the prosthesis to be made after tooth extraction and to preserve the dimensions of the maxillary sinus, we recommend that the prosthesis construction should not be postponed for a long time. The literature was reviewed in terms of the relationship between maxillary sinus diameters and maxillary sinus variations. Only one article was found that was conducted by Cakur et al., who examined the relationship between sinus height and the presence of septa and it is observed that there was no statistically significant relationship between them [50]. However, when the material and method part of the study was examined, it was observed that the maxillary sinus measurement technique was different. Creating a standard for the measurement of maxillary sinus diameters will eliminate the method differences in future studies. No article was found in which other diameters were associated with variations. Our study is thought to be the first in this regard. It is thought that this study can be a guide for future articles on this subject.
Maxillary sinus diameters were compared with gender and age groups, and a statistically significant relationship was found between them. It was observed that men have larger sinus diameters than women. The literature has associated the gender difference in maxillary sinus sizes with men's body height and weight, which are generally larger than women’s [49].
When the age groups were examined, it was observed that there was no statistically significant difference in the vertical diameter, but there were statistically significant differences in the other diameters. It was observed that the mean maxillary sinus diameter of the patients aged 18–35 years in the horizontal diameter was larger than those aged 50–65 years. It was also observed that the mean maxillary sinus diameter of patients over 65 years of age in sagittal diameter was greater than those between 50 and 65 years of age.
Conclusion
A limited Turkish population was evaluated in our study which examined the variations and diameters of the maxillary sinus. At least one variation was observed in 165 (77.8%) of 212 patients (at least one variation in 278 of 424 maxillary sinuses). AMO (57,5%) and septa (42%) were observed in a substantial amount. The most common type of orientation observed within the septa of the maxillary sinus was the completed coronal type. Septa was most frequently observed in the middle part. When the dimensional diameters of the maxillary sinus were examined, it was statistically determined that the values of male patients were higher than females.
In this current study, the relationship between maxillary sinus diameters and maxillary sinus variations are examined. In this regard, the number of studies are lacking in the literature. According to the results of this study, patients with maxillary sinus variation had higher maxillary sinus diameters. Therefore, it should be considered that there may be a variation if the maxillary sinus diameter is higher than its average values. Additionally, the fact that maxillary sinus diameters are higher in males is thought to be useful information for forensic science.
Considering that maxillary sinus variations with such a high incidence may cause complications in sinus surgeries, preoperative CBCT imaging is essential. Dentists should not ignore the variations in surgical interventions to be applied to the posterior maxilla, especially the maxillary sinus, to prevent complications, and should benefit from radiography methods that allow the evaluation of all three dimensions (where indicated).
References
Maspero C, Farronato M, Bellincioni F, Annibale A, Machetti J, Abate A, Davide C. Three-dimensional evaluation of maxillary sinus changes in growing subjects: a retrospective cross-sectional study. Materials (Basel). 2020. https://doi.org/10.3390/ma13041007.
Dedeoglu N, Altun O. Evaluation of maxillary sinus anatomical variations and pathologies in elderly, young, posterior dentate and edentulous patient groups with cone-beam computed tomography. Folia Morphol (Warsz). 2019. https://doi.org/10.5603/FM.a2019.0013.
Padhye NM, Bhatavadekar NB. Quantitative assessment of the edentulous posterior maxilla for implant therapy: a retrospective cone beam computed tomographic study. J Maxillofac Oral Surg. 2020. https://doi.org/10.5051/jpis.2019.49.4.237.
Yu SJ, Lee YH, Lin CP, Wu AYJ. Computed tomographic analysis of maxillary sinus anatomy relevant to sinus lift procedures in edentulous ridges in Taiwanese patients. J Periodontal Implant Sci. 2019. https://doi.org/10.5051/jpis.2019.49.4.237.
Krennmair G, Ulm C, Lugmayr H. Maxillary sinus septa: incidence, morphology and clinical implications. J Craniomaxillofac Surg. 1997. https://doi.org/10.1016/s1010-5182(97)80063-7.
Orhan K, KusakciSeker B, Aksoy S, Bayindir H, Berberoglu A, Seker E. Cone beam CT evaluation of maxillary sinus septa prevalence, height, location and morphology in children and an adult population. Med Princ Pract. 2013. https://doi.org/10.1159/000339849.
Kim MJ, Jung UW, Kim CS, Kim KD, Choi SH, Kim CK, Cho KS. Maxillary sinus septa: prevalence, height, location, and morphology. A reformatted computed tomography scan analysis. J Periodontol. 2006. https://doi.org/10.1902/jop.2006.050247.
Koymen R, Gocmen-Mas N, Karacayli U, Ortakoglu K, Ozen T, Yazici AC. Anatomic evaluation of maxillary sinus septa: surgery and radiology. Clin Anat. 2009. https://doi.org/10.1002/ca.20813.
Lana JP, Carneiro PMR, de Carvalho MV, de Souza PEA, Manzi FR, Horta MCR. Anatomic variations and lesions of the maxillary sinus detected in cone beam computed tomography for dental implants. Clin Oral Implants Res. 2012. https://doi.org/10.1111/j.1600-0501.2011.02321.x.
Lozano-Carrascal N, Salomo-Coll O, Gehrke SA, Calvo-Guirado JL, Hernandez-Alfaro F, Gargallo-Albiol J. Radiological evaluation of maxillary sinus anatomy: a cross-sectional study of 300 patients. Ann Anat. 2017. https://doi.org/10.1016/j.aanat.2017.06.002.
Park YB, Jeon HS, Shim JS, Lee KW, Moon HS. Analysis of the anatomy of the maxillary sinus septum using 3-dimensional computed tomography. J Oral Maxillofac Surg. 2011. https://doi.org/10.1016/j.joms.2010.07.020.
Shibli JA, Faveri M, Ferrari DS, Melo L, Garcia RV, d’Avila S, Figueiredo LC, Feres M. Prevalence of maxillary sinus septa in 1024 subjects with edentulous upper jaws: a retrospective study. J Oral Implantol. 2007. https://doi.org/10.1563/1548-1336(2007)33[293:POMSSI]2.0.CO;2.
Ali IK, Sansare K, Karjodkar FR, Vanga K, Salve P, Pawar AM. Cone-beam computed tomography analysis of accessory maxillary ostium and Haller cells: prevalence and clinical significance. Imaging Sci Dent. 2017. https://doi.org/10.5624/isd.2017.47.1.33.
Zirek A, Beklen H, Okyay Budak R, Güler OK, Yardimci AC, Bozkus F. Paranazal sinüslerde anatomik varyasyonların sıklığı ve enflamatuar sinüs hastalıklarına etkisi. Harran Üniversitesi Tıp Fakültesi Dergisi. 2016;13(3):215–22.
Amine K, Slaoui S, Kanice FZ, Kissa J. Evaluation of maxillary sinus anatomical variations and lesions: a retrospective analysis using cone beam computed tomography. J Stomatol Oral Maxillofac Surg. 2020. https://doi.org/10.1016/j.jormas.2019.12.021.
Hungerbuhler A, Rostetter C, Lubbers HT, Rucker M, Stadlinger B. Anatomical characteristics of maxillary sinus septa visualized by cone beam computed tomography. Int J Oral Maxillofac Surg. 2019. https://doi.org/10.1016/j.ijom.2018.09.009.
Bornstein MM, Seiffert C, Maestre-Ferrin L, Fodich I, Jacobs R, Buser D, von Arx T. An analysis of frequency, morphology, and locations of maxillary sinus septa using cone beam computed tomography. Int J Oral Maxillofac Implants. 2016. https://doi.org/10.1016/j.ijom.2018.09.009.
Shahidi S, Zamiri B, MomeniDanaei S, Salehi S, Hamedani S. Evaluation of anatomic variations in maxillary sinus with the aid of Cone beam computed tomography (CBCT) in a population in South of Iran. J Dent (Shiraz). 2016;17(1):7–15.
BirikenSipahi D, Beycan K, Ercalik YS. Maksiller sinus hacminin ve septum morfolojisinin Angle Sınıf I, II ve III iskeletsel iliskiye sahip bireylerde uc boyutlu olarak degerlendirilmesi. Selcuk Dent J. 2019;6(4):216–21.
Selcuk A, Ozcan KM, Akdogan O, Bilal N, Dere H. Variations of maxillary sinus and accompanying anatomical and pathological structures. J Craniofac Surg. 2008. https://doi.org/10.1097/scs.0b013e3181577b01.
Kocak N, Alpoz E, Boyacioglu H. Morphological assessment of maxillary sinus septa variations with cone-beam computed tomography in a turkish population. Eur J Dent. 2019. https://doi.org/10.1055/s-0039-1688541.
Hung K, Montalvao C, Yeung AWK, Li G, Bornstein MM. Frequency, location, and morphology of accessory maxillary sinus ostia: a retrospective study using cone beam computed tomography (CBCT). Surg Radiol Anat. 2020. https://doi.org/10.1007/s00276-019-02308-6.
Onwuchekwa RC, Alazigha N. Computed tomography anatomy of the paranasal sinuses and anatomical variants of clinical relevants in Nigerian adults. Egypt J Ear, Nose, Throat and Allied Sci. 2017. https://doi.org/10.1016/j.ejenta.2016.11.001.
Ozel HE, Ozdogan F, Esen E, Genc MG, Genc S, Selcuk A. The association between septal deviation and the presence of a maxillary accessory ostium. Int Forum Allergy Rhinol. 2015. https://doi.org/10.1002/alr.21610.
Yenigun A, Fazliogullari Z, Gun C, Uysal II, Nayman A, Karabulut AK. The effect of the presence of the accessory maxillary ostium on the maxillary sinus. Eur Arch Otorhinolaryngol. 2016. https://doi.org/10.1007/s00405-016-4129-8.
Yeung AWK, Consoul N, Montalvao C, Hung K, Jacobs R, Bornstein MM. Visibility, location, and morphology of the primary maxillary sinus ostium and presence of accessory ostia: a retrospective analysis using cone beam computed tomography (CBCT). Clin Oral Investig. 2019. https://doi.org/10.1007/s00784-019-02829-9.
Simsek Kaya G, Dalbatan O, Kaya M, Kocabalkan B, Sindel A, Akdag M. The potential clinical relevance of anatomical structures and variations of the maxillary sinus for planned sinus floor elevation procedures: a retrospective cone beam computed tomography study. Clin Implant Dent Relat Res. 2019. https://doi.org/10.1111/cid.12703.
Akay G, Yaman D, Karadag O, Gungor K. Evaluation of the relationship of dimensions of maxillary sinus drainage system with anatomical variations and sinusopathy: cone-beam computed tomography findings. Med Princ Pract. 2020. https://doi.org/10.1159/000504963.
Mathew R, Omami G, Hand A, Fellows D, Lurie A. Cone beam CT analysis of Haller cells: prevalence and clinical significance. Dentomaxillofac Radiol. 2013. https://doi.org/10.1259/dmfr.20130055.
Prem Kumar KS, Sudarshan R, Vijayabala GS, Srinivasan SR, Kini PV. A study on the assessment of Haller Cells in panoramic radiograph. Niger Med J. 2018. https://doi.org/10.4103/nmj.NMJ_166_18.
Yilmazsoy Y, Arslan S. Haller hucresi varyasyon sikliği ve maksiller sinuzit ile iliskisinin bilgisayarli tomografi ile degerlendirilmesi. J Health Sci Med. 2018. https://doi.org/10.32322/jhsm.442889.
Yucel A, Derekoy FS, Yilmaz MD, Altuntas A. Sinonazal anatomik varyasyonlarin paranazal sinüs enfeksiyonlarina etkisi. Kocatepe Tıp Dergisi. 2004;5(1):43–7.
Dursun E, Korkmaz H, Bayiz U, Gocmen H, Samim E, Eryilmaz A, Ozeri C. Maksiller Mukozal Retansiyon Kistlerinde Cerrahi Yaklasımlar ve Ostiomeatal Kompleks Anatomik Varyasyonları. T Klin KBB. 2001;1:154–61.
Misirlioglu M, Nalcaci R, Adisen MZ, Yilmaz YS. Paranasal sinus anatomik yapilari ve varyasyonlarinin dental volumetrik tomografi ile incelenmesi. A Ü Diş Hek Fak Derg. 2011;38(3):143–52.
Cha JK, Song YW, Park SH, Jung RE, Jung UW, Thoma DS. Alveolar ridge preservation in the posterior maxilla reduces vertical dimentional change: a randomized controlled clinical trial. Clin Oral Implants Res. 2019. https://doi.org/10.1111/clr.13436.
Lombardi T, Bernardello F, Berton F, Porrelli D, Rapani A, Piloni AC, Forillo L, Di Lenarda R, Stacchi C. Efficacy of alveolar ridge preservation after maxillary molar extraction in reducing crestal bone resorption and sinus pneumatization: a multicenter prospective case-control study. BioMed Res Int. 2018. https://doi.org/10.1155/2018/9352130.
Whyte A, Boeddinghaus R. The maxillary sinus: physiology, development and imaging anatomy. Dentomaxillofac Radiol. 2019. https://doi.org/10.1259/dmfr.20190205.
Kocak N. Maksiller sinusun radyolojik tani yontemlerinin ve anatomik limitasyonlarinin tedavi planlanmasinda rolu. Atatürk Üniv Diş Hek Fak Derg. 2019. https://doi.org/10.17567/ataunidfd.296422.
Wolff C, Mucke T, Wagenpfeil S, Kanatas A, Bissinger O, Deppe H. Do CBCT scans alter surgical treatment plans? Comparison of preoperative surgical diagnosis using panoramic versus cone-beam CT images. J Craniomaxillofac Surg. 2016. https://doi.org/10.1016/j.jcms.2016.07.025.
Donizeth-Rodrigues C, Fonseca-De Silveira M, Goncalves-De Alencar AH, Garcia Santos Silva MA, Francisco-Dde Mendonca E, Estrela C. Three-dimensional images contribute to the diagnosis of mucous retention cyst in maxillary sinus. Med Oral Patol Oral Cir Bucal. 2013. https://doi.org/10.4317/medoral.18141.
Tadinada A, Fung K, Thacker S, Mahdian M, Jadhav A, Schincaglia GP. Radiographic evaluation of the maxillary sinus prior to dental implant therapy: a comparison between two-dimensional and three-dimensional radiographic imaging. Imaging Sci Dent. 2015. https://doi.org/10.5624/isd.2015.45.3.169.
Vogiatzi T, Kloukos D, Scarfe WC, Bornstein MM. Incidence of anatomical variations and disease of the maxillary sinuses as identified by cone beam computed tomography: a systematic review. Int J Oral Maxillofac Implants. 2014. https://doi.org/10.11607/jomi.3644.
Constantine S, Clark B, Kiermeier A, Anderson PP. Panoramic radiography is of limited value in the evaluation of maxillary sinus disease. Oral Surg Oral Med Oral Pathol Oral Radiol. 2019. https://doi.org/10.1016/j.oooo.2018.10.005.
Ozalp O, Tezerisener HA, Kocabalkan B, Buyukkaplan US, Özarslan MM, Simsek Kaya G, Altay MA, Sindel A. Comparing the precision of panoramic radiography and cone-beam computed tomography in avoiding anatomical structures critical to dental implant surgery: a retrospective study. Imaging Sci Dent. 2018. https://doi.org/10.5624/isd.2018.48.4.269.
Tarim E, Kalabalik F. Bir turk orneklem grubunda dental volumetrik tomogafi endikasyonlari. Atatürk Üniv Diş Hek Fak Derg. 2014. https://doi.org/10.17567/dfd.80367.
Akhlaghi M, Bakhtavar K, Kamali A, Maarefdoost J, Sheikhazadi A, Mousavi F, SaberyAnary SH, Sheikhazadi E. The diagnostic value of anthropometric indices of maxillary sinuses for sex determination using CT-scan images in Iranian adults: a cross-sectional study. J Forensic Leg Med. 2017. https://doi.org/10.1016/j.jflm.2017.05.017.
Dangore-Khasbage S, Bhowate R. Utility of the morphometry of the maxillary sinuses for gender determination by using computed tomography. Dent Med Probl. 2018. https://doi.org/10.17219/dmp/99622.
Lorkiewicz-Muszynska D, Kociemba W, Rewekant A, Sroka A, Jonczyk-Potoczna K, PatelskaBanaszewska M, Przystanska A. Development of the maxillary sinus from birth to age 18. Postnatal growth pattern. Int J Pediatr Otorhinolaryngol. 2015. https://doi.org/10.1016/j.ijporl.2015.05.032.
Paknahad M, Shahidi S, Zarei Z. Sexual dimorphism of maxillary sinus dimensions using cone-beam computed tomography. J Forensic Sci. 2017. https://doi.org/10.1111/1556-4029.13272.
Cakur B, Sumbullu MA, Durna D, Yilmaz AB. Antral septa varlıgı ile maksiller sinus yukseklıgı arasindaki iliski. Atatürk Üniv Diş Hek Fak Derg. 2011;1:1–4.
Demirkol M, Demirkol N. The effects of posterior alveolar bone height on the height of maxillary sinus septa. Surg Radiol Anat. 2019. https://doi.org/10.1007/s00276-019-02271-2.
Devaraja K, Doreswamy SM, Pujary K, Ramaswamy B, Pillai S. Anatomical variations of the nose and paranasal sinuses: a computed tomographic study. Indian J Otolaryngol Head Neck Surg. 2019. https://doi.org/10.1007/s12070-019-01716-9.
Acknowledgements
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. ‘This article does not contain any studies with human or animal subjects performed by any of the authors.’
Funding
This work has been supported by Selcuk University Scientific Research Projects Coordination Unit under grant number 19102056.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declare no competing interests.
Ethical approval
All procedures followed were in accordance with the Ethical Standards of the Responsible Committee on Human Experimentation (İnstitutional and National) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed consent
Informed consent form was not obtained as it was a retrospective study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ayyildiz, H., Akgunlu, F. Are maxillary sinus variations related to maxillary sinus diameters?. Oral Radiol 39, 425–436 (2023). https://doi.org/10.1007/s11282-022-00655-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-022-00655-6