
Abstract
Physiologically-based pharmacokinetic (PBPK) models explicitly incorporate tissue-specific blood flows, partition coefficients, and metabolic processes. Since PBPK models are derived using physiologic parameters and interactions of the compound with tissue components, these models are considered to be “bottom up” as opposed to “top down”. Modeling approaches can be characterized as either a posteriori (observational) or a priori (based solely on theory). Furthermore, approaches can be mechanistic (structure and components based on mechanisms) or empirical (based on observations alone). Both “bottom up” and “top down” approaches can incorporate either empirical or mechanistic components. In this perspective, we discuss some of the methods and assumptions of current PBPK modeling approaches. Specifically, we discuss drug partitioning into phospholipids and neutral lipids, use of blood-plasma ratios to estimate basic drug tissue partitioning, and clearance of neutral and acidic drugs. Based on these discussions, we believe that current PBPK models are mechanistic but a posteriori and semi-empirical.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The quote by George Box “All models are wrong but some are useful” (1) is often used to remind ourselves that the complexity of any real system or process cannot be captured with simple models. In pharmacokinetics, compartmental models are simple models that can capture most complexities in observed plasma concentration-time (C-t) profiles. Physiologically-based pharmacokinetic (PBPK) models offer the advantages of explicitly modeling tissue-specific blood flows, partition coefficients, and metabolic processes. Since PBPK models are derived using physiologic parameters and interactions of the compound with tissue components, these models are considered to be “bottom up”. For example, tissue partition coefficients are often predicted using “composition-based” models in which interactions with proteins and lipids are either measured experimentally or derived (2–4). Given the usefulness of PBPK models, it is generally believed that the current approach to model parameterization is mechanistic and accurate. This commentary reviews current PBPK approaches and discusses some inconsistencies between some of these approaches and basic physicochemical principles.
Semantics in PBPK Modeling
The difference between “bottom up” versus “top down” approaches is well defined. In PK modeling, compartmental models are primarily “top down”, since observed C-t profiles are used to construct mathematical relationships. PBPK models, on the other hand, are “bottom up” since they are built with basic physiological information and drug-specific characteristics. Modeling approaches can also be characterized as either a posteriori (observational) or a priori (based solely on theory). Furthermore, approaches can be mechanistic (structure and components based on mechanisms) or empirical (based on observations alone). Both “bottom up” and “top down” approaches can incorporate either empirical or mechanistic components. For example, “top down” compartmental models can be semi-empirical, since physical meaning can be assigned to empirically calculated parameters (e.g. biphasic distribution indicates slow equilibration with some tissues). PBPK models, while “bottom up”, can be constructed with empirical, semi-empirical, or mechanistic components. For the most part, PBPK models are mechanistic, since model structure is based on physiological processes. However, there seems to be an aspiration to create PBPK models that are a priori, i.e. based on first principles. A priori models do not require parameterization since a 1:1 relationship (y = mx + c, where m = 1 and c = 0) between model components and physiological processes is assumed. Modeling complex biological systems from first principles is not the norm. Most chemical interactions are modeled with linear free energy relationships, which incorporate mechanistic theories and thermodynamic principles. As discussed below, presumed a priori components in PBPK models include: 1) determining the binding constant for ionizable bases and acidic phospholipids from the blood:plasma ratio (BP), 2) equating neutral phospholipids to 30% n-octanol and 70% water, and 3) predicting drug-adipose partitioning with a vegetable oil:water partition coefficient. Each of these points and a misconception concerning drug clearance predictions is discussed in detail below.
Tissue Partitioning
Tissue partition coefficients are frequently modeled using composition-based models in which different classes of drugs interact with different tissue components. In some current PBPK models, tissue lipids are divided into neutral lipids, neutral phospholipids, and acidic phospholipids (Fig. 1). The primary assumptions of these models are that ionized bases bind only to acidic phospholipids, and uncharged compounds bind to neutral phospholipids and neutral lipids (2). Other than plasma proteins and lipoproteins, nonspecific binding to proteins is usually ignored.

Chemical structures of a neutral phospholipid (phosphatidyl choline), acidic phospholipids (phosphatidyl serine and phosphatidic acid), neutral lipids (triglycerides), and n-octanol.
Binding to acidic phospholipids – The premise that ionized bases bind only to acidic phospholipids is based on a report that the tissue partition coefficients for bases correlate with the tissue phosphatidylserine (PS) content (5). This premise was supported by additional experiments that measured binding affinities of bases to PS in a hexane-water system, essentially an ion pairing experiment. Can we expect that interactions with membranes are well represented by ion pairing in hexane? For a net-neutral phospholipid in hexane, e.g. phosphatidylcholine, the negative phosphates are already paired with the positive choline groups. The net negative charge of PS provides another negative charge to pair with the ionized base and increases the partitioning into hexane. However, membranes are highly ordered lipid bilayers with negatively charged phosphates at the interface between the polar head groups and the hydrophobic core of the membrane. Since a hydrophobic amine can pair with the phosphate group, favorable ionic interactions between ionized bases and all membrane phospholipids are expected. This in fact is observed since artificial immobilized phosphatidylcholine membranes have high affinities for hydrophobic amines (6).
Although the membrane partitioning of some bases is sensitive to PS content, this is not always true. For example, chlorpromazine (7) and propranolol (8) show a 2-fold increase with increasing PS, and amiodarone is insensitive to PS content (9). As reviewed by Balaz (10), the interactions between compounds and the membrane are likely a highly complex function of membrane lipid composition and fluidity, functional groups (H-bond donors, H-bond acceptors, etc.), and the spatial orientation of both the drug molecule and the lipids. Therefore, simple in vitro models (e.g. ion-pairing in hexane) are unlikely to accurately represent drug-membrane interactions in a generalizable manner.
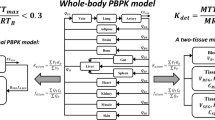
Despite the possible deficiency described above, tissue partition coefficients for bases are well predicted. A possible explanation for these reasonably good predictions is the use of blood-to-plasma partitioning (BP) to calculate the acidic phospholipid binding constant, KaAP. The commonly used equation to calculate tissue partition constants, including erythrocytes, is dominated by the acidic phospholipid binding term (see Fig. 2). This term is itself calculated from BP (essentially unbound partitioning into erythrocytes). It is noteworthy that tissue binding for bases in vivo is highly correlated with erythrocyte partitioning (See Hinderling (11) and Fig. 2). Thus, KaAP is calculated from erythrocyte partitioning, which is itself highly correlated with tissue partitioning, and KaAP is then used to calculate tissue partitioning. This process is circular and there is no mechanistic evidence that this correlation is due to binding to acidic phospholipids. In fact, there are more carboxylate groups due to the sialic acids of the glycocalyx surrounding the erythrocyte than there are acidic phospholipids in the erythrocyte membrane (12). This suggests that although BP can be used to predict the tissue partition coefficients of bases, the approach is empirical since the mechanism is unknown.

Correlation between Log KpuRBC and unbound Log Vss for basic drugs (n = 48), with equations to calculate tissue partitioning of basic drugs (from Rodgers et al. (3)). Data taken from Rodgers and Rowland (26). A similar correlation was reported by Hinderling (11). The acidic phospholipid binding component is assumed to be predominant, and acidic phospholipid tissue partition coefficient is assumed to be equal to as acidic phospholipid erythrocyte partition coefficient. Notations are defined as follows: [AP−]T: acidic phospholipid concentration in tissue, [AP−]BC: acidic phospholipid concentration in red blood cell, BP: blood to plasma ratio, few: fraction of drug in extracellular water, fiw: fraction of drug in intracellular water, fnl: fraction of neutral lipids in tissue, fnp: fraction of neutral phospholipids in tissue, fup: unbound fraction of drug in plasma, H: hematocrit, i: the ith tissue from a total of n tissues representing the whole body, KaBC: acidic phospholipid erythrocyte partition coefficient, KaAP: acidic phospholipid tissue partition coefficient, Kpu: tissue partition coefficient of plasma unbound drug, KpuBC: erythrocyte partition coefficient of plasma unbound drug, pHBC: pH of red blood cell, pHiw: pH of intracellular water, pHp: pH of plasma, Pow: drug octanol to water partition coefficient, Ptp: tissue partition coefficient of total drug (same as Kp); X = 1 + 10pKa-pHiw; Y = 1 + 10pKa-pHp.
There is another unexpected advantage of using BP to calculate tissue KaAP values. Normally, drug volume of distribution (Vss) is very sensitive to the experimental value of the free fraction in plasma (fup). Since fup is also an important determinant of BP, when calculating tissue partitioning (Kp values) from BP, errors in fup will largely cancel (Fig. 2). This has been shown previously using a generic PBPK model to simulate the effect of plasma protein binding errors on Vss prediction (13).
Binding to neutral phospholipids – Current methods assume that only uncharged molecules will bind to neutral phospholipids. This binding is modeled using n-octanol:water partition coefficients (Log P). In the original (14) and subsequent methods to parameterize binding to neutral phospholipids (2–4), it is assumed that neutral phospholipids behave like 70% water and 30% neutral lipids. This ratio is based upon a reported hydrophilic/lipophilic balance (HLB) of 14 for lecithin. The HLB scale for nonionic detergents is 0–20. Therefore, a value of 70% is used (14). In reality, phospholipids are ionic and the HLB scale can be much higher for ionized compounds (15). Use of a different scale would result in a much greater percent of lipid. Also, a wide range of HLB values are reported for lecithin and the most commonly reported values are 3–9.
Irrespective of the HLB analysis, neither the polar head group nor the lipophilic core of the lipid bilayer is well represented by n-octanol or water (16). The reason for the popular use of Log P as a hydrophobicity measure is the presence of both H-bond acceptors and donors in n-octanol. According to Leo et al. (17), “Since many NH and OH groups are present in enzymes and membranes, it is not surprising that alcohol: water systems give better correlations and thus have become more widely used as extrathermodynamic reference systems”. Thus, Log P, while very useful as a general hydrophobicity measure, was never intended to provide a 1:1 relationship with neutral lipid partitioning.
Further, the ordered nature of the phospholipid membrane is important. Hydrophobic molecules with H-acceptors or donors can reside at the interface of the polar head group and hydrophobic core of the membrane (10). Therefore, similar to acidic phospholipids, hydrophobic cations and other amphiphilic molecules can also partition into neutral phospholipids. Predicting these interactions will require more information than simply Log P. Rather than attempting to represent membrane partitioning with Log P alone, QSAR methods, as applied to many biological systems, may be more successful.
Binding to neutral lipids – An important consideration in PBPK modeling is that adipose tissue is significantly different in its lipid content compared to other tissues. Early attempts to calculate adipose Kp values using Log P were unsuccessful (14). Since adipose is predominantly composed of triglycerides, vegetable oil:water partitioning (Log Pvo) was considered instead. In reality, Log Pvo is rarely measured. Instead, a linear relationship between Log P and Log Pvo is used to calculate the Log Pvo value. Linear relationships were originally described by Hansch (18), and were developed using primarily volatile organic compounds. Thus, the Kp,vo could be calculated by combining measurements of vegetable oil:air and air:water partitioning. A single linear relationship between Log P and Log Pvo is unlikely, given that vegetable oil has no H-bond donors and is essentially anhydrous, while n-octanol has an H-bond donor and contains 2 M water. Most of the volatile organic compounds used by Hansch were very small, and could be classified as H-bond donors or acceptors. Two linear equations were therefore derived, one for H-bond acceptors, and one for H-bond donors (18). The two equations had the same slope but the Y-intercepts differed by one log unit. Given the fact that most drug molecules have multiple donor and acceptor functionalities, it is difficult to believe that these equations will accurately predict Log Pvo for all compounds. In fact, Hansch later stated that this model works best in the absence of strong H-bond donors (19). A plot of experimental Log Dvo (Log Dvo is calculated from pKa and Log Pvo) data versus values calculated from Log P (20,21) for n = 32 drugs is shown in Fig. 3. The average fold error for these compounds is 5.1, and the calculated Log Dvo values for several compounds are poorly predicted.

Experimental versus calculated LogDV:O for 32 compounds. Experimental values were obtained from Poulin and Theil (20) and Oldendorf (21). Calculated values were calculated from LogP using Eq. 7 in Poulin and Theil (20) and pKa. Red: acidic drugs, blue: basic drugs, green: neutral drugs. The dashed and dotted lines represent 2-fold and 3-fold error, respectively. The example outliers highlighted are ascorbic acid (6000×), methotrexate (300×), methylphenidate (180×), pentobarbital (37×), and toluene (15×).
Another potential problem with using vegetable oil as a representative solvent is the variability in the oil composition. Others have used pure compounds such as trioleolylglycerol as a solvent (22). Excellent correlations with partition coefficients with other oils are observed, but the intercepts can vary by more than a log unit. Given the importance of adipose partitioning for some drugs and the sensitivity of this component to Dvo, errors in this value can result in inaccurate Vss predictions.
Inaccuracies in Vss predictions are often observed after clinical data becomes available. In order to accurately simulate drug disposition, modifications to the model must be made. Any of the model parameters can be altered to obtain the correct Vss, including Dvo, Log P, tissue volumes etc. However, the modified model will now have a “top-down”, empirical component. Also, since the origin of the errors in tissue Kp values is unknown, tissue specific information is lost.
Clearance Predictions
Clearance and Vss are independent PK parameters. Compared to tissue partitioning and Vss predictions, predicting clearance with PBPK models has been more challenging. Since in vitro clearance data is readily available, PBPK modeling offers an attractive method to incorporate this data for in vivo clearance predictions. Certain processes can be easily predicted, such as renal elimination without active secretion or reabsorption. Other clearance processes such as glucuronidation remain very difficult to model, possibly due to lack of good in vitro assays that mimic in vivo metabolism. In general, many clearances are poorly predicted, and when clinical data becomes available, scaling factors are required to fit the PBPK model to the clinical data (23).
Some of these scaling factors are consistent. For example, hepatic clearance of acidic and neutral drugs is usually under-predicted and scaling factors are required to obtain accurate clearance predictions. Poulin et al. proposed an albumin-mediated transport mechanism that increases the extracellular concentration of drug at the plasma membrane (24), resulting in an increased intracellular concentration and increased clearance. We have recently reported that highly protein bound neutral and acidic drugs require a scaling factor of 12, whereas bases did not require a scaling factor (13). While this is consistent with an albumin-mediated uptake mechanism, in the absence of an active transport or an energy-dependent process, increased concentrations at the membrane cannot increase intracellular concentrations at equilibrium. According to the basic thermodynamic principle of microscopic reversibility, the equilibrium across a membrane can only be altered by energy-dependent processes or a chemical gradient generated by energy dependent processes (e.g. pH).
Reported examples of albumin-mediated transport are usually associated with increased rates of drug uptake and not increased equilibrium intracellular concentrations. For example, several reports of albumin mediated transport into hepatocytes are discussed by Iwatsubo et al. (25). Several mechanisms have been proposed including a conformational change in albumin at the cell surface and increased rates of diffusion through a rate-limiting unstirred water layer. If uptake into the cell is rate limiting, an increase in the rate of uptake will result in an increase in the rate of metabolism. However, rate limiting hepatic uptake will result in an over-prediction in hepatic clearance since intracellular concentrations will be less than unbound extracellular concentrations. Also, most PBPK models today are not permeability-rate limited and instantaneous equilibrium with the blood is assumed. Within this model formalism, only processes that alter the equilibrium intracellular concentration can affect clearance. In the absence of a known active transport mechanism, current scaling factors must be regarded as empirical and not mechanistic.
Balaz describes structure-based subcellular PK models as a posteriori semi-empirical models, because “the modeled system is not known in sufficient detail to allow for the formulation of a priori theoretical models”. To summarize the discussion above, i) drug partitioning into phospholipids and neutral lipids is unlikely to be represented by a single solvent model system, ii) while BP provides a reasonable estimate of basic drug tissue partitioning, the mechanism is unknown, and iii) the mechanism responsible for increased intracellular concentrations of neutral and acidic drugs is unknown. Thus, it is not currently possible to build an a priori mechanistic PBPK model. This is essentially true for all biological systems. It is unreasonable to expect a 1:1 correlation between a physiological process and an artificial in vitro system. Therefore, we believe that current PBPK models are mechanistic but a posteriori and semi-empirical. This point is not just an issue of semantics. Believing that models can be constructed a priori makes a search for more predictive relationships appear to be a step backwards. In reality, a deeper understanding of the mechanisms involved, leading to more predictive relationships, may be necessary to improve PBPK models. With respect to George Box’s quote above, PBPK models are useful but there is ample room for improvement.
References
Box GE. Robustness in the strategy of scientific model building. In: Robustness in statistics. 1979. p. 1201–236.
Rodgers T, Leahy D, Rowland M. Physiologically based pharmacokinetic modeling 1: predicting the tissue distribution of moderate-to-strong bases. J Pharm Sci. 2005;94(6):1259–76.
Rodgers T, Rowland M. Physiologically based pharmacokinetic modelling 2: predicting the tissue distribution of acids, very weak bases, neutrals and zwitterions. J Pharm Sci. 2006;95(6):1238–57.
Peyret T, Poulin P, Krishnan K. A unified algorithm for predicting partition coefficients for PBPK modeling of drugs and environmental chemicals. Toxicol Appl Pharmacol. 2010;249(3):197–207.
Yata N, Toyoda T, Murakami T, Nishiura A, Higashi Y. Phosphatidylserine as a determinant for the tissue distribution of weakly basic drugs in rats. Pharm Res. 1990;7(10):1019–25.
Amato M, Barbato F, Morrica P, Quaglia F, La Rotonda MI. Interactions between amines and phospholipids: a chromatographic study on immobilized artificial membrane (IAM) stationary phases at various pH values. Helv Chim Acta. 2000;83(10):2836–47.
Takegami S, Kitamura K, Kitade T, Takashima M, Ito M, et al. Effects of phosphatidylserine and phosphatidylethanolamine content on partitioning of triflupromazine and chlorpromazine between phosphatidylcholine-aminophospholipid bilayer vesicles and water studied by second-derivative spectrophotometry. Chem Pharm Bull (Tokyo). 2005;53(1):147–50.
Kubo M, Gardner MF, Hostetler KY. Binding of propranolol and gentamicin to small unilamellar phospholipid vesicles. Contribution of ionic and hydrophobic forces. Biochem Pharmacol. 1986;35(21):3761–5.
Chatelain P, Laruel R. Amiodarone partitioning with phospholipid bilayers and erythrocyte membranes. J Pharm Sci. 1985;74(7):783–4.
Balaz S. Modeling kinetics of subcellular disposition of chemicals. Chem Rev. 2009;109(5):1793–899.
Hinderling PH. Red blood cells: a neglected compartment in pharmacokinetics and pharmacodynamics. Pharmacol Rev. 1997;49(3):279–95.
Eylar EH, Madoff MA, Brody OV, Oncley JL. The contribution of sialic acid to the surface charge of the erythrocyte. J Biol Chem. 1962;237:1992–2000.
Ye M, Nagar S, Korzekwa K. A physiologically based pharmacokinetic model to predict the pharmacokinetics of highly protein-bound drugs and the impact of errors in plasma protein binding. Biopharm Drug Dispos. 2016;37(3):123–41.
Poulin P, Krishnan K. A biologically-based algorithm for predicting human tissue: blood partition coefficients of organic chemicals. Hum Exp Toxicol. 1995;14(3):273–80.
Davies JT. A quantitative kinetic theory of emulsion type, I. Physical chemistry of the emulsifying agent. In Gas/Liquid and Liquid/Liquid Interface. Proceedings of the International Congress of Surface Activity. 1957. p 426–438.
Lukacova V, Natesan S, Peng M, Tandlich R, Wang Z, et al. Structural determinants of drug partitioning in surrogates of phosphatidylcholine bilayer strata. Mol Pharm. 2013;10(10):3684–96.
Leo A, Hansch C, Elkins D. Partition coefficients and their uses. Chem Rev. 1971;71(6):525–616.
Leo AJ, Hansch C. Linear free energy relations between partitioning solvent systems. J Org Chem. 1971;36(11):1539–44.
Hansch C, Vittoria A, Silipo C, Jow PY. Partition coefficients and the structure-activity relationship of the anesthetic gases. J Med Chem. 1975;18(6):546–8.
Poulin P, Theil FP. Prediction of pharmacokinetics prior to in vivo studies. 1. Mechanism-based prediction of volume of distribution. J Pharm Sci. 2002;91(1):129–56.
Oldendorf WH. Lipid solubility and drug penetration of the blood brain barrier. Proc Soc Exp Biol Med. 1974;147(3):813–5.
Niimi AJ. Solubility of organic chemicals in octanol, triolein and cod liver oil and relationships between solubility and partition coefficients. Water Res. 1991;25(12):1515–21.
Jones HM, Dickins M, Youdim K, Gosset JR, Attkins NJ, et al. Application of PBPK modelling in drug discovery and development at Pfizer. Xenobiotica. 2012;42(1):94–106.
Poulin P, Haddad S. Albumin and uptake of drugs in cells: additional validation exercises of a recently published equation that quantifies the albumin-facilitated uptake mechanism(s) in physiologically based pharmacokinetic and pharmacodynamic modeling research. J Pharm Sci. 2015;104(12):4448–58.
Iwatsubo T, Hirota N, Ooie T, Suzuki H, Sugiyama Y. Prediction of in vivo drug disposition from in vitro data based on physiological pharmacokinetics. Biopharm Drug Dispos. 1996;17(4):273–310.
Rodgers T, Rowland M. Mechanistic approaches to volume of distribution predictions: understanding the processes. Pharm Res. 2007;24(5):918–33.
ACKNOWLEDGMENTS AND DISCLOSURES
This work was partially funded by NIH/NIGMS grants 1R01GM104178 and 1R01GM114369 to KK and SN.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Korzekwa, K., Nagar, S. On the Nature of Physiologically-Based Pharmacokinetic Models –A Priori or A Posteriori? Mechanistic or Empirical?. Pharm Res 34, 529–534 (2017). https://doi.org/10.1007/s11095-016-2089-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-016-2089-8